
Association of Urinary Potassium Excretion with Blood Pressure Variability and Cardiovascular Outcomes in Patients with Pre-Dialysis Chronic Kidney Disease

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
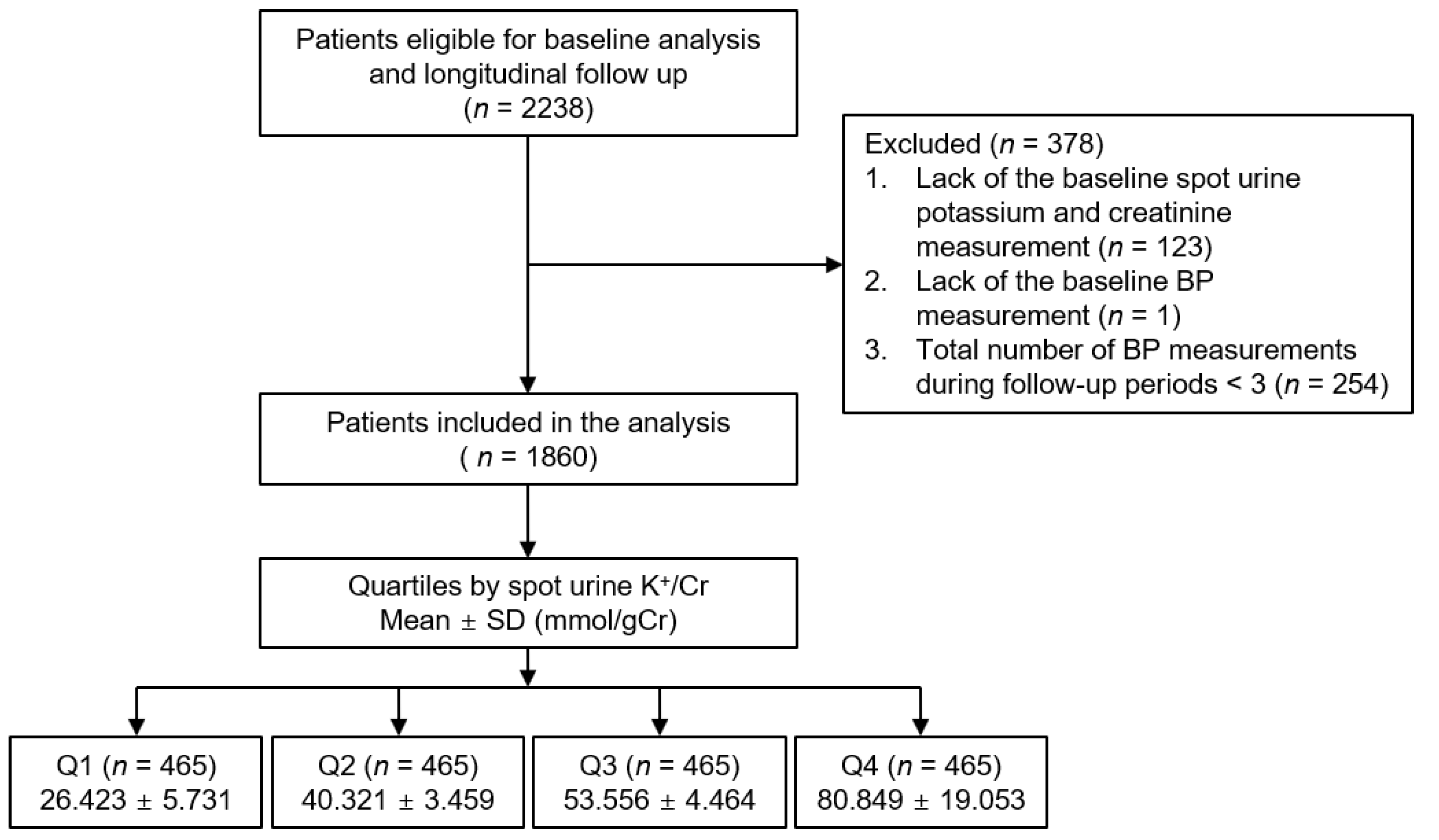
2.1. Study Design and Participants
2.2. Data Collection
2.3. Determination of Visit-to-Visit BPV
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
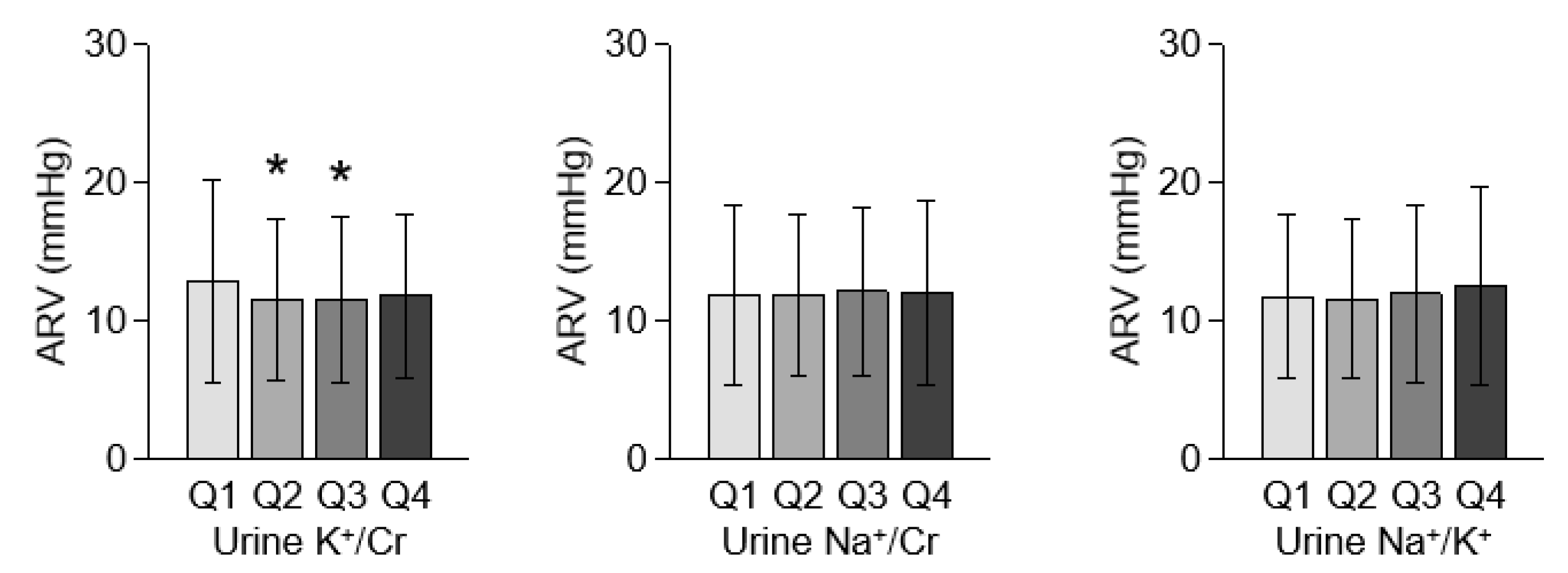
3.2. Association between Spot Urine K+/Cr and BPV in Patients with Pre-Dialysis CKD
3.3. Association of Low Urine Potassium Excretion with Adverse CV Outcomes in Patients with Pre-Dialysis CKD
3.4. Sensitivity Analyses
3.5. Subgroup Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mezue, K.; Goyal, A.; Pressman, G.S.; Matthew, R.; Horrow, J.C.; Rangaswami, J. Blood pressure variability predicts adverse events and cardiovascular outcomes in SPRINT. J. Clin. Hypertens. 2018, 20, 1247–1252. [Google Scholar] [CrossRef] [Green Version]
- Myasoedova, E.; Crowson, C.S.; Green, A.B.; Matteson, E.L.; Gabriel, S.E. Longterm blood pressure variability in patients with rheumatoid arthritis and its effect on cardiovascular events and all-cause mortality in RA: A population-based comparative cohort study. J. Rheumatol. 2014, 41, 1638–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.; Shin, J.; Choi, S.Y.; Sung, K.C.; Ihm, S.H.; Kim, K.I.; Kim, Y.M. Impact of Visit-to-Visit Variability in Systolic Blood Pressure on Cardiovascular Outcomes in Korean National Health Insurance Service-National Sample Cohort. Am. J. Hypertens. 2017, 30, 577–586. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Li, D.; Song, Y.; Gao, L.; Fan, F.; Wang, B.; Liang, M.; Wang, G.; Li, J.; Zhang, Y.; et al. Visit-to-visit variability in blood pressure and the development of chronic kidney disease in treated general hypertensive patients. Nephrol. Dial. Transplant. 2020, 35, 1739–1746. [Google Scholar] [CrossRef]
- Okada, H.; Fukui, M.; Tanaka, M.; Matsumoto, S.; Mineoka, Y.; Nakanishi, N.; Asano, M.; Yamazaki, M.; Hasegawa, G.; Nakamura, N. Visit-to-visit blood pressure variability is a novel risk factor for the development and progression of diabetic nephropathy in patients with type 2 diabetes. Diabetes Care 2013, 36, 1908–1912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noshad, S.; Mousavizadeh, M.; Mozafari, M.; Nakhjavani, M.; Esteghamati, A. Visit-to-visit blood pressure variability is related to albuminuria variability and progression in patients with type 2 diabetes. J. Hum. Hypertens. 2014, 28, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Whittle, J.; Lynch, A.I.; Tanner, R.M.; Simpson, L.M.; Davis, B.R.; Rahman, M.; Whelton, P.K.; Oparil, S.; Muntner, P. Visit-to-Visit Variability of BP and CKD Outcomes: Results from the ALLHAT. Clin. J. Am. Soc. Nephrol. 2016, 11, 471–480. [Google Scholar] [CrossRef] [Green Version]
- Mallamaci, F.; Tripepi, G.; D’Arrigo, G.; Borrelli, S.; Garofalo, C.; Stanzione, G.; Provenzano, M.; De Nicola, L.; Conte, G.; Minutolo, R.; et al. Blood Pressure Variability, Mortality, and Cardiovascular Outcomes in CKD Patients. Clin. J. Am. Soc. Nephrol. 2019, 14, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruddy, M.C.; Arora, A.; Malka, E.S.; Bialy, G.B. Blood pressure variability and urinary electrolyte excretion in normotensive adults. Am. J. Hypertens. 1993, 6, 480–486. [Google Scholar] [CrossRef]
- Ozkayar, N.; Dede, F.; Ates, I.; Akyel, F.; Yildirim, T.; Altun, B. The relationship between dietary salt intake and ambulatory blood pressure variability in non-diabetic hypertensive patients. Nefrologia 2016, 36, 694–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, D.; He, J.; Wu, X.; Duan, X.; Whelton, P.K. Effect of potassium supplementation on blood pressure in Chinese: A randomized, placebo-controlled trial. J. Hypertens. 2001, 19, 1325–1331. [Google Scholar] [CrossRef]
- He, F.J.; Marciniak, M.; Carney, C.; Markandu, N.D.; Anand, V.; Fraser, W.D.; Dalton, R.N.; Kaski, J.C.; MacGregor, G.A. Effects of potassium chloride and potassium bicarbonate on endothelial function, cardiovascular risk factors, and bone turnover in mild hypertensives. Hypertension 2010, 55, 681–688. [Google Scholar] [CrossRef]
- Cupisti, A.; Kovesdy, C.P.; D’Alessandro, C.; Kalantar-Zadeh, K. Dietary Approach to Recurrent or Chronic Hyperkalaemia in Patients with Decreased Kidney Function. Nutrients 2018, 10, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaron, K.J.; Sanders, P.W. Role of dietary salt and potassium intake in cardiovascular health and disease: A review of the evidence. Mayo Clin. Proc. 2013, 88, 987–995. [Google Scholar] [CrossRef] [Green Version]
- Kovesdy, C.P.; Matsushita, K.; Sang, Y.; Brunskill, N.J.; Carrero, J.J.; Chodick, G.; Hasegawa, T.; Heerspink, H.L.; Hirayama, A.; Landman, G.W.D.; et al. Serum potassium and adverse outcomes across the range of kidney function: A CKD Prognosis Consortium meta-analysis. Eur. Heart J. 2018, 39, 1535–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonberg-Yoo, A.K.; Tighiouart, H.; Levey, A.S.; Beck, G.J.; Sarnak, M.J. Urine Potassium Excretion, Kidney Failure, and Mortality in CKD. Am. J. Kidney Dis. 2017, 69, 341–349. [Google Scholar] [CrossRef]
- Kim, H.W.; Park, J.T.; Yoo, T.H.; Lee, J.; Chung, W.; Lee, K.B.; Chae, D.W.; Ahn, C.; Kang, S.W.; Choi, K.H.; et al. Urinary Potassium Excretion and Progression of CKD. Clin. J. Am. Soc. Nephrol. 2019, 14, 330–340. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.J.; Wang, X.; Liu, L.; Yan, H.; Lee, S.F.; Mony, P.; Devanath, A.; et al. Urinary sodium and potassium excretion, mortality, and cardiovascular events. N. Engl. J. Med. 2014, 371, 612–623. [Google Scholar] [CrossRef] [Green Version]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ 2013, 346, f1378. [Google Scholar] [CrossRef] [Green Version]
- Cook, N.R.; Obarzanek, E.; Cutler, J.A.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K.; Trials of Hypertension Prevention Collaborative Research Group. Joint effects of sodium and potassium intake on subsequent cardiovascular disease: The Trials of Hypertension Prevention follow-up study. Arch. Intern. Med. 2009, 169, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelton, P.K.; He, J.; Cutler, J.A.; Brancati, F.L.; Appel, L.J.; Follmann, D.; Klag, M.J. Effects of oral potassium on blood pressure. Meta-analysis of randomized controlled clinical trials. JAMA 1997, 277, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.-H.; Park, S.K.; Park, H.C.; Chin, H.J.; Chae, D.W.; Choi, K.H.; Han, S.H.; Yoo, T.H.; Lee, K.; Kim, Y.-S.; et al. KNOW-CKD (KoreaN cohort study for Outcome in patients With Chronic Kidney Disease): Design and methods. BMC Nephrol. 2014, 15, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Chapter 1: Definition and classification of CKD. Kidney Int. Suppl. (2011) 2013, 3, 19–62. [CrossRef] [PubMed] [Green Version]
- Fujita, T.; Ito, Y. Salt loads attenuate potassium-induced vasodilation of forearm vasculature in humans. Hypertension 1993, 21, 772–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, R.J.; Robinson, B.F. The dilator response to K+ is reduced in the forearm resistance vessels of men with primary hypertension. Clin. Sci. 1984, 66, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Jhee, J.H.; Seo, J.; Lee, C.J.; Park, J.T.; Han, S.H.; Kang, S.W.; Park, S.; Yoo, T.H. Ambulatory blood pressure variability and risk of cardiovascular events, all-cause mortality, and progression of kidney disease. J. Hypertens. 2020, 38, 1712–1721. [Google Scholar] [CrossRef]
- Shimbo, D.; Shea, S.; McClelland, R.L.; Viera, A.J.; Mann, D.; Newman, J.; Lima, J.; Polak, J.F.; Psaty, B.M.; Muntner, P. Associations of aortic distensibility and arterial elasticity with long-term visit-to-visit blood pressure variability: The Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Hypertens. 2013, 26, 896–902. [Google Scholar] [CrossRef] [Green Version]
- Nagai, M.; Hoshide, S.; Nishikawa, M.; Masahisa, S.; Kario, K. Visit-to-visit blood pressure variability in the elderly: Associations with cognitive impairment and carotid artery remodeling. Atherosclerosis 2014, 233, 19–26. [Google Scholar] [CrossRef]
- Diaz, K.M.; Veerabhadrappa, P.; Kashem, M.A.; Feairheller, D.L.; Sturgeon, K.M.; Williamson, S.T.; Crabbe, D.L.; Brown, M.D. Relationship of visit-to-visit and ambulatory blood pressure variability to vascular function in African Americans. Hypertens. Res. 2012, 35, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Tatasciore, A.; Zimarino, M.; Renda, G.; Zurro, M.; Soccio, M.; Prontera, C.; Emdin, M.; Flacco, M.; Schillaci, G.; De Caterina, R. Awake blood pressure variability, inflammatory markers and target organ damage in newly diagnosed hypertension. Hypertens. Res. 2008, 31, 2137–2146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahranavard, T.; Carbone, F.; Montecucco, F.; Xu, S.; Al-Rasadi, K.; Jamialahmadi, T.; Sahebkar, A. The role of potassium in atherosclerosis. Eur. J. Clin. Investig. 2021, 51, e13454. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef] [PubMed]
- Parati, G.; Ochoa, J.E.; Lombardi, C.; Bilo, G. Assessment and management of blood-pressure variability. Nat. Rev. Cardiol. 2013, 10, 143–155. [Google Scholar] [CrossRef]
- Wong, Y.K.; Chan, Y.H.; Hai, J.S.H.; Lau, K.K.; Tse, H.F. Predictive value of visit-to-visit blood pressure variability for cardiovascular events in patients with coronary artery disease with and without diabetes mellitus. Cardiovasc. Diabetol. 2021, 20, 88. [Google Scholar] [CrossRef]
- Eguchi, K.; Hoshide, S.; Schwartz, J.E.; Shimada, K.; Kario, K. Visit-to-visit and ambulatory blood pressure variability as predictors of incident cardiovascular events in patients with hypertension. Am. J. Hypertens. 2012, 25, 962–968. [Google Scholar] [CrossRef] [Green Version]
- Hoshide, S. Clinical implication of visit-to-visit blood pressure variability. Hypertens. Res. 2018, 41, 993–999. [Google Scholar] [CrossRef]
- Mena, L.; Pintos, S.; Queipo, N.V.; Aizpúrua, J.A.; Maestre, G.; Sulbarán, T. A reliable index for the prognostic significance of blood pressure variability. J. Hypertens. 2005, 23, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Rothwell, P.M.; Howard, S.C.; Dolan, E.; O’Brien, E.; Dobson, J.E.; Dahlöf, B.; Sever, P.S.; Poulter, N.R. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet 2010, 375, 895–905. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Spot Urine K+/Cr | p Value | ||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||
| Follow-up duration (year) | 5.150 ± 1.766 | 5.237 ± 1.724 | 5.180 ± 1.715 | 5.180 ± 1.709 | 0.892 |
| Age (year) | 50.785 ± 13.566 | 53.880 ± 11.609 | 54.487 ± 11.157 | 55.282 ± 11.198 | <0.001 |
| Male | 358 (77.0) | 330 (71.0) | 260 (55.8) | 172 (37.1) | <0.001 |
| Charlson comorbidity index | 0.049 | ||||
| 0–3 | 316 (68.0) | 348 (74.8) | 353 (75.9) | 354 (76.3) | |
| 4–5 | 137 (29.5) | 110 (23.7) | 108 (23.2) | 105 (22.6) | |
| ≥6 | 12 (2.6) | 7 (1.5) | 5 (1.1) | 5 (1.1) | |
| Primary renal disease | 0.218 | ||||
| DM | 128 (27.5) | 106 (22.8) | 89 (19.1) | 105 (22.6) | |
| HTN | 95 (20.4) | 102 (21.9) | 89 (19.1) | 92 (19.8) | |
| GN | 154 (33.1) | 144 (31.0) | 164 (35.2) | 152 (32.8) | |
| TID | 3 (0.6) | 4 (0.9) | 3 (0.6) | 4 (0.9) | |
| PKD | 56 (12.0) | 81 (17.4) | 91 (19.5) | 84 (18.1) | |
| Others | 29 (6.2) | 28 (6.0) | 30 (6.4) | 27 (5.8) | |
| History of DM | 164 (35.3) | 144 (31.0) | 126 (27.0) | 156 (33.6) | 0.060 |
| Medication | |||||
| ACEi/ARBs | 399 (89.9) | 382 (89.7) | 415 (94.1) | 395 (90.2) | 0.068 |
| Diuretics | 169 (38.1) | 121 (27.7) | 140 (31.7) | 131 (29.9) | 0.007 |
| Number of antihypertensive drugs ≥ 3 | 165 (35.5) | 144 (31.0) | 135 (29.0) | 121 (26.1) | 0.016 |
| BMI (kg/m2) | 24.635 ± 3.496 | 24.552 ± 3.402 | 24.555 ± 3.196 | 24.517 ± 3.403 | 0.960 |
| WC (cm) | 87.461 ± 9.775 | 88.195 ± 10.083 | 86.987 ± 9.343 | 86.682 ± 9.475 | 0.111 |
| SBP (mmHg) | 127.194 ± 16.501 | 127.860 ± 15.620 | 126.863 ± 14.774 | 126.170 ± 14.620 | 0.407 |
| DBP (mmHg) | 76.428 ± 11.306 | 77.204 ± 11.317 | 77.485 ± 11.010 | 76.069 ± 9.963 | 0.165 |
| Laboratory findings | |||||
| Serum K+ (mEq/L) | 4.594 ± 0.682 | 4.547 ± 0.661 | 4.529 ± 0.631 | 4.555 ± 0.649 | 0.511 |
| 24 h urine K+ (mEq/day) | 42.027 ± 17.588 | 51.258 ± 43.036 | 56.539 ± 19.539 | 63.575 ± 23.118 | <0.001 |
| Hemoglobin (g/dL) | 12.910 ± 2.116 | 13.138 ± 1.995 | 13.027 ± 1.947 | 12.835 ± 1.816 | 0.098 |
| Albumin (g/dL) | 4.192 ± 0.388 | 4.199 ± 0.412 | 4.189 ± 0.370 | 4.245 ± 0.360 | 0.085 |
| Total cholesterol (mg/dL) | 168.254 ± 39.284 | 172.600 ± 38.473 | 177.301 ± 37.889 | 177.711 ± 34.974 | <0.001 |
| HDL-C (mg/dL) | 46.447 ± 15.762 | 48.837 ± 15.353 | 50.428 ± 14.616 | 52.714 ± 15.800 | <0.001 |
| LDL-C (mg/dL) | 93.485 ± 31.973 | 94.838 ± 30.550 | 97.863 ± 28.925 | 99.501 ± 29.626 | 0.011 |
| TG (mg/dL) | 163.899 ± 104.737 | 158.026 ± 96.706 | 155.236 ± 101.332 | 150.296 ± 91.559 | 0.213 |
| Fasting glucose (mg/dL) | 112.513 ± 46.816 | 109.218 ± 36.002 | 107.429 ± 33.016 | 110.770 ± 35.886 | 0.217 |
| 25(OH) Vitamin D (ng/mL) | 17.190 ± 9.218 | 18.653 ± 9.408 | 18.806 ± 9.916 | 19.683 ± 10.427 | 0.017 |
| hsCRP (mg/dL) | 0.600 [0.100, 1.860] | 0.780 [0.100, 1.800] | 0.550 [0.200, 1.400] | 0.500 [0.200, 1.600] | 0.004 |
| Spot urine ACR (mg/gCr) | 349.855 [103.771, 1050.062] | 280.683 [57.545, 856.995] | 318.405 [71.818, 901.375] | 306.642 [48.397, 801.223] | 0.387 |
| eGFR (mL/min/1.73 m2) | 48.048 ± 28.928 | 51.516 ± 27.605 | 56.207 ± 58.677 | 64.745 ± 31.792 | <0.001 |
| CKD stages | <0.001 | ||||
| Stage 1 | 49 (10.5) | 62 (13.3) | 73 (15.7) | 129 (27.8) | |
| Stage 2 | 78 (16.8) | 84 (18.1) | 107 (23.0) | 103 (22.2) | |
| Stage 3a | 73 (15.7) | 87 (18.7) | 85 (18.2) | 77 (16.6) | |
| Stage 3b | 116 (24.9) | 118 (25.4) | 107 (23.0) | 81 (17.5) | |
| Stage 4 | 129 (27.7) | 96 (20.6) | 78 (16.7) | 62 (13.4) | |
| Stage 5 | 20 (4.3) | 18 (3.9) | 16 (3.4) | 12 (2.6) | |
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| Coefficients (95% CIs) | p Value | Coefficients (95% CIs) | p Value | |
| Low urine K+/Cr | ||||
| ARV | 1.260 (0.545, 1.975) | 0.001 | 1.163 (0.424, 1.901) | 0.002 |
| SD | 0.511 (−0.071, 1.094) | 0.085 | 0.431 (−0.176, 1.037) | 0.164 |
| CoV | 0.005 (0.000, 0.009) | 0.057 | 0.004 (−0.001, 0.009) | 0.138 |
| High urine K+/Cr | ||||
| ARV | −0.130 (−0.857, 0.598) | 0.727 | 0.127 (−0.634, 0.887) | 0.744 |
| SD | 0.261 (−0.330, 0.853) | 0.386 | 0.468 (−0.154, 1.091) | 0.140 |
| CoV | 0.002 (−0.002, 0.007) | 0.299 | 0.004 (−0.001, 0.009) | 0.101 |
| Low urine Na+/Cr | ||||
| ARV | −0.139 (−0.871, 0.593) | 0.710 | 0.169 (−0.547, 0.884) | 0.644 |
| SD | −0.257 (−0.851, 0.338) | 0.397 | −0.018 (−0.605, 0.568) | 0.951 |
| CoV | −0.001 (0.006, 0.004) | 0.611 | 0.000 (−0.005, 0.005) | 0.978 |
| High urine Na+/Cr | ||||
| ARV | 0.105 (−0.614, 0.824) | 0.774 | −0.190 (−0.904, 0.524) | 0.602 |
| SD | 0.127 (−0.457, 0.711) | 0.669 | −0.116 (−0.701, 0.469) | 0.698 |
| CoV | 0.000 (−0.005, 0.004) | 0.915 | −0.001 (−0.006, 0.004) | 0.659 |
| Low urine Na+/K+ | ||||
| ARV | −0.176 (−0.906, 0.553) | 0.635 | 0.222 (−0.483, 0.927) | 0.536 |
| SD | 0.060 (−0.533, 0.652) | 0.844 | 0.343 (−0.235, 0.920) | 0.245 |
| CoV | 0.001 (−0.004, 0.006) | 0.654 | 0.003 (−0.002, 0.007) | 0.263 |
| High urine Na+/K+ | ||||
| ARV | 0.873 (0.158, 1.588) | 0.017 | 0.275 (−0.426, 0.976) | 0.442 |
| SD | 0.545 (−0.036, 1.126) | 0.066 | 0.146 (−0.429, 0.720) | 0.618 |
| CoV | 0.003 (−0.002, 0.008) | 0.220 | 0.001 (−0.004, 0.005) | 0.722 |
| Spot Urine K+/Cr | Cases, n (%) | Unadjusted | Adjusted | |||
|---|---|---|---|---|---|---|
| HR (95% CIs) | p Value | HR (95% CIs) | p Value | |||
| eMACE | Q1 | 36 (7.7) | 1.899 (1.114, 3.239) | 0.018 | 2.502 (1.162, 5.387) | 0.019 |
| Q2 | 27 (5.8) | 1.727 (0.992, 3.006) | 0.053 | 1.120 (0.512, 2.451) | 0.777 | |
| Q3 | 29 (6.2) | 1.393 (0.812, 2.389) | 0.228 | 1.590 (0.777, 3.252) | 0.204 | |
| Q4 | 40 (8.6) | Reference | Reference | |||
| All-cause mortality | Q1 | 17 (3.7) | 0.733 (0.321, 1.672) | 0.460 | 0.604 (0.240, 1.519) | 0.284 |
| Q2 | 20 (4.30) | 1.406 (0.694, 2.846) | 0.344 | 1.222 (0.560, 2.668) | 0.615 | |
| Q3 | 17(3.6) | 1.037 (0.487, 2.207) | 0.925 | 0.953 (0.433, 2.099) | 0.905 | |
| Q4 | 17 (3.7) | Reference | Reference | |||
| Spot Urine K+/Cr | Cases, n (%) | Unadjusted | Adjusted | |||
|---|---|---|---|---|---|---|
| HR (95% CIs) | p for Interaction | HR (95% CIs) | p for Interaction | |||
| Age < 60 years | Q1 | 14 (4.3) | 4.162 (1.523, 11.373) | 0.672 | 0.502 (0.202, 12.797) | 0.780 |
| Q2 | 11 (3.5) | 3.800 (1.334, 10.826) | 5.681 (0.378, 85.486) | |||
| Q3 | 16 (5.3) | 4.155 (1.492, 11.570) | 2.271 (0.203, 25.433) | |||
| Q4 | 13 (4.6) | Reference | Reference | |||
| Age ≥ 60 years | Q1 | 22 (15.4) | 1.221 (0.631, 2.365) | 4.737 (1.453, 15.445) | ||
| Q2 | 16 (10.3) | 1.132 (0.557, 2.301) | 2.351 (0.488, 11.334) | |||
| Q3 | 13 (7.9) | 0.707 (0.330, 1.514) | 1.645 (0.511, 5.294) | |||
| Q4 | 27 (14.9) | Reference | Reference | |||
| Diuretics (−) | Q1 | 17 (6.2) | 1.414 (0.684, 2.924) | 0.618 | 1.152 (0.302, 4.386) | 0.896 |
| Q2 | 21 (6.6) | 1.631 (0.830, 3.206) | 1.439 (0.432, 4.797) | |||
| Q3 | 14 (4.7) | 2.015 (0.962, 4.222) | 5.175 (1.726, 15.518) | |||
| Q4 | 22 (7.2) | Reference | Reference | |||
| Diuretics (+) | Q1 | 17 (10.1) | 2.873 (1.264, 6.531) | 2.936 (0.465, 18.526) | ||
| Q2 | 6 (5.0) | 1.933 (0.666, 5.604) | 0.521 (0.066, 4.077) | |||
| Q3 | 13 (9.3) | 0.939 (0.409, 2.158) | 1.445 (0.132, 15.812) | |||
| Q4 | 16 (12.2) | Reference | Reference | |||
| eGFR ≥ 45 mL/min/1.73 m2 | Q1 | 10 (5.0) | 1.627 (0.678, 3.906) | 0.194 | 2.374 (0.245, 23.011) | 0.535 |
| Q2 | 8 (3.4) | 2.030 (0.837, 4.922) | 7.845 (0.368, 167.103) | |||
| Q3 | 18 (6.8) | 1.184 (0.575, 2.436) | 8.476 (1.301, 55.226) | |||
| Q4 | 22 (7.1) | Reference | Reference | |||
| eGFR < 45 mL/min/1.73 m2 | Q1 | 26 (9.8) | 1.958 (0.971, 3.950) | 2.494 (0.841, 7.393) | ||
| Q2 | 18 (8.2) | 1.603 (0.767, 3.352) | 1.201 (0.364, 3.961) | |||
| Q3 | 11 (5.5) | 1.991 (0.819, 4.840) | 2.600 (0.467, 14.478) | |||
| Q4 | 18 (11.6) | Reference | Reference | |||
| Spot urine ACR < 300 mg/gCr | Q1 | 17 (7.9) | 2.416 (1.035, 5.644) | 0.913 | 0.421 (0.067, 2.636) | 0.593 |
| Q2 | 13 (5.4) | 2.378 (1.053, 5.370) | 2.595 (0.112, 59.942) | |||
| Q3 | 10 (4.4) | 1.505 (0.642, 3.531) | 6.738 (1.044, 43.490) | |||
| Q4 | 20 (8.8) | Reference | Reference | |||
| Spot urine ACR ≥ 300 mg/gCr | Q1 | 19 (7.6) | 1.542 (0.769, 3.093) | 3.888 (1.208, 12.512) | ||
| Q2 | 14 (6.2) | 1.339 (0.616, 2.913) | 1.371 (0.313, 6.008) | |||
| Q3 | 19 (7.9) | 1.182 (0.573, 2.437) | 2.936 (0.793, 10.867) | |||
| Q4 | 20 (8.4) | Reference | Reference | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suh, S.H.; Song, S.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Oh, K.-H.; Lee, J.; Han, S.H.; Kim, Y.H.; et al. Association of Urinary Potassium Excretion with Blood Pressure Variability and Cardiovascular Outcomes in Patients with Pre-Dialysis Chronic Kidney Disease. Nutrients 2021, 13, 4443. https://doi.org/10.3390/nu13124443
Suh SH, Song SH, Oh TR, Choi HS, Kim CS, Bae EH, Oh K-H, Lee J, Han SH, Kim YH, et al. Association of Urinary Potassium Excretion with Blood Pressure Variability and Cardiovascular Outcomes in Patients with Pre-Dialysis Chronic Kidney Disease. Nutrients. 2021; 13(12):4443. https://doi.org/10.3390/nu13124443
Chicago/Turabian StyleSuh, Sang Heon, Su Hyun Song, Tae Ryom Oh, Hong Sang Choi, Chang Seong Kim, Eun Hui Bae, Kook-Hwan Oh, Joongyub Lee, Seung Hyeok Han, Yeong Hoon Kim, and et al. 2021. "Association of Urinary Potassium Excretion with Blood Pressure Variability and Cardiovascular Outcomes in Patients with Pre-Dialysis Chronic Kidney Disease" Nutrients 13, no. 12: 4443. https://doi.org/10.3390/nu13124443