
Long-Term Outcomes of in Utero Ramadan Exposure: A Systematic Literature Review

 , , , ,
, , , ,  , , , and
, , , and 
Abstract
:1. Introduction
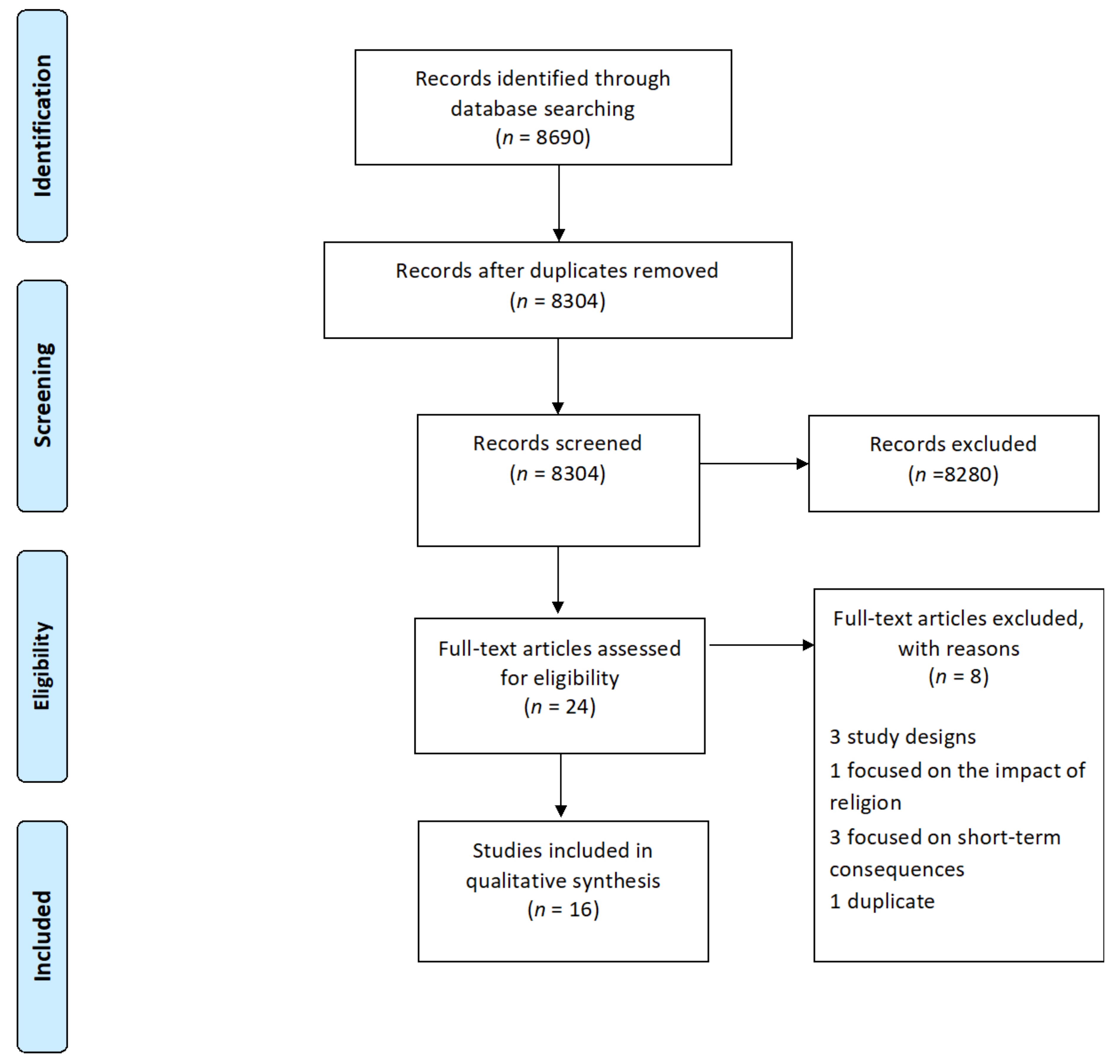
2. Materials and Methods
3. Results
3.1. Study Characteristics
3.2. Study Results According to Outcome Measures
3.3. Health Outcomes
3.4. Economic Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leiper, J.B.; Molla, A.M.; Molla, A.M. Effects on health of fluid restriction during fasting in Ramadan. Eur. J. Clin. Nutr. 2003, 57, S30–S38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seiermann, A.U.; Al-Mufti, H.; Waid, J.L.; Wendt, A.S.; Sobhan, S.; Gabrysch, S. Women’s fasting habits and dietary diversity during Ramadan in rural Bangladesh. Matern. Child Nutr. 2021, 17, e13135. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Rezaie, P.; Chaudhri, O.; Karimi, E.; Nematy, M. The effect of Ramadan fasting on cardiometabolic risk factors and anthropometrics parameters: A systematic review. Pak. J. Med. Sci. 2015, 31, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Kul, S.; Savaş, E.; Öztürk, Z.A.; Karadağ, G. Does Ramadan Fasting Alter Body Weight and Blood Lipids and Fasting Blood Glucose in a Healthy Population? A Meta-analysis. J. Relig. Health 2014, 53, 929–942. [Google Scholar] [CrossRef]
- Kadri, N.; Tilane, A.; El Batal, M.; Taltit, Y.; Tahiri, S.M.; Moussaoui, D. Irritability during the month of Ramadan. Psychosom. Med. 2000, 62, 280–285. [Google Scholar] [CrossRef] [Green Version]
- Rouhani, M.H.; Azadbakht, L. Is Ramadan fasting related to health outcomes? A review on the related evidence. J. Res. Med. Sci. 2014, 19, 987–992. [Google Scholar]
- Ghazal, K.; Khazaal, J.; Chahine, R.; Hajjar, C.; El Hasan, J.; Naser, L.; Koulaymi, E.; Yared, G. Ramadan fasting during pregnancy: Characteristics and outcomes. Int. J. Reprod. Contracept. Obstet. Gynecol. 2020, 9, 3936–3943. [Google Scholar] [CrossRef]
- Joosoph, J.; Abu, J.; Yu, S.L. A survey of fasting during pregnancy. Singap. Med. J. 2004, 45, 583–586. [Google Scholar]
- Baynouna Al Ketbi, L.M.; Niglekerke, N.J.; Zein Al Deen, S.M.; Mirghani, H. Diet restriction in Ramadan and the effect of fasting on glucose levels in pregnancy. BMC Res. Notes 2014, 7, 392. [Google Scholar] [CrossRef] [Green Version]
- Hayward, A.R. The human fetus and newborn: Development of the immune response. Birth Defects Orig. Artic. Ser. 1983, 19, 289–294. [Google Scholar]
- Palmer, A.C. Nutritionally mediated programming of the developing immune system. Adv. Nutr. Bethesda Md. 2011, 2, 377–395. [Google Scholar] [CrossRef] [Green Version]
- Schoeps, A.; van Ewijk, R.; Kynast-Wolf, G.; Nebié, E.; Zabré, P.; Sié, A.; Gabrysch, S. Ramadan exposure in utero and child mortality in Burkina Faso: Analysis of a population-based cohort including 41,025 children. Am. J. Epidemiol. 2018, 187, 2085–2092. [Google Scholar] [CrossRef]
- Glazier, J.D.; Hayes, D.J.L.; Hussain, S.; D’Souza, S.W.; Whitcombe, J.; Heazell, A.E.P.; Ashton, N. The effect of Ramadan fasting during pregnancy on perinatal outcomes: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2018, 18, 421. [Google Scholar] [CrossRef] [Green Version]
- Oosterwijk, V.N.L.; Molenaar, J.M.; van Bilsen, L.A.; Kiefte-de Jong, J.C. Ramadan Fasting during Pregnancy and Health Outcomes in Offspring: A Systematic Review. Nutrients 2021, 13, 3450. [Google Scholar] [CrossRef]
- Roseboom, T.; de Rooij, S.; Painter, R. The Dutch famine and its long-term consequences for adult health. Early Hum. Dev. 2006, 82, 485–491. [Google Scholar] [CrossRef]
- Painter, R.C.; de Rooij, S.R.; Bossuyt, P.M.; Simmers, T.A.; Osmond, C.; Barker, D.J.; Bleker, O.P.; Roseboom, T.J. Early onset of coronary artery disease after prenatal exposure to the Dutch famine. Am. J. Clin. Nutr. 2006, 84, 322–327. [Google Scholar] [CrossRef]
- De Rooij, S.R.; Wouters, H.; Yonker, J.E.; Painter, R.C.; Roseboom, T.J. Prenatal undernutrition and cognitive function in late adulthood. Proc. Natl. Acad. Sci. USA 2010, 107, 16881–16886. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- CPH’s Data Extraction and Assessment Template. Available online: https://ph.cochrane.org/review-authors (accessed on 21 November 2021).
- Specialist Unit for Review Evidence (SURE). Available online: https://www.cardiff.ac.uk/__data/assets/pdf_file/0006/1142997/SURE-CA-form-for-Cohort_2018.pdf (accessed on 23 November 2021).
- Pradella, F.; van Ewijk, R. As Long as the Breath Lasts: In Utero Exposure to Ramadan and the Occurrence of Wheezing in Adulthood. Am. J. Epidemiol. 2018, 187, 2100–2108. [Google Scholar] [CrossRef]
- Van Ewijk, R.J.; Painter, R.C.; Roseboom, T.J. Associations of prenatal exposure to Ramadan with small stature and thinness in adulthood: Results from a large Indonesian population-based study. Am. J. Epidemiol. 2013, 177, 729–736. [Google Scholar] [CrossRef] [Green Version]
- Van Ewijk, R. Long-term health effects on the next generation of Ramadan fasting during pregnancy. J. Health Econ. 2011, 30, 1246–1260. [Google Scholar] [CrossRef] [Green Version]
- Majid, F.; Behrman, J.; Mani, S. Short-term and long-term distributional consequences of prenatal malnutrition and stress: Using Ramadan as a natural experiment. BMJ Glob. Health 2019, 4, e001185. [Google Scholar] [CrossRef] [Green Version]
- Majid, M.F. The persistent effects of in utero nutrition shocks over the life cycle: Evidence from Ramadan fasting. J. Dev. Econ. 2015, 117, 48–57. [Google Scholar] [CrossRef]
- Kunto, Y.S.; Mandemakers, J.J. The effects of prenatal exposure to Ramadan on stature during childhood and adolescence: Evidence from the Indonesian Family Life Survey. J. Econ. Hum. Biol. 2019, 33, 29–39. [Google Scholar] [CrossRef]
- Chaudhry, T.T.; Mir, A. The Impact of Prenatal Exposure to Ramadan on Child Anthropomorphic Outcomes in Pakistan. Matern. Child Health J. 2021, 25, 1136–1146. [Google Scholar] [CrossRef]
- Azizi, F.; Sadeghipour, H.; Siahkolah, B.; Rezaei-Ghaleh, N. Intellectual development of children born of mothers who fasted in Ramadan during pregnancy. Int. J. Vitam. Nutr. Res. 2004, 74, 374–380. [Google Scholar] [CrossRef]
- Karimi, S.M.; Little, B.B.; Mokhtari, M. Short-term fetal nutritional stress and long-term health: Child height. Am. J. Hum. Biol. 2021, 33, e23531. [Google Scholar] [CrossRef]
- Lee, S.; Nam, M.; Jeong, D.; Lee, W. Does Ramadan Harm Infant Health? Evidence from Ethiopia. Int. Econ. J. 2020, 34, 613–633. [Google Scholar] [CrossRef]
- Almond, D.; Mazumder, B.; Van Ewijk, R. Fasting during Pregnancy and Children’s Academic Performance; 0898-2937; National Bureau of Economic Research: Cambridge, MA, USA, 2011. [Google Scholar]
- Greve, J.; Schultz-Nielsen, M.L.; Tekin, E. Fetal malnutrition and academic success: Evidence from Muslim immigrants in Denmark. J. Econ. Educ. Rev. 2017, 60, 20–35. [Google Scholar] [CrossRef] [Green Version]
- Schultz-Nielsen, M.L.; Tekin, E.; Greve, J. Labor market effects of intrauterine exposure to nutritional deficiency: Evidence from administrative data on Muslim immigrants in Denmark. Econ. Hum. Biol. 2016, 21, 196–209. [Google Scholar] [CrossRef] [Green Version]
- Almond, D.; Mazumder, B. Health capital and the prenatal environment: The effect of Ramadan observance during pregnancy. Am. Econ. J. Appl. Econ. 2011, 3, 56–85. [Google Scholar] [CrossRef] [Green Version]
- Karimi, S.M.; Basu, A. The effect of prenatal exposure to Ramadan on children’s height. Econ. Hum. Biol. 2018, 30, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Van Bilsen, L.A.; Savitri, A.I.; Amelia, D.; Baharuddin, M.; Grobbee, D.E.; Uiterwaal, C.S.P.M. Predictors of Ramadan fasting during pregnancy. J. Epidemiol. Glob. Health 2016, 6, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziaee, V.; Kihanidoost, Z.; Younesian, M.; Akhavirad, M.-B.; Bateni, F.; Kazemianfar, Z.; Hantoushzadeh, S. The effect of ramadan fasting on outcome of pregnancy. Iran. J. Pediatr. 2010, 20, 181–186. [Google Scholar] [PubMed]
- BIMA. Ramadan Compendium. Available online: https://britishima.org/ramadan/compendium/ (accessed on 22 November 2021).
- Seiermann, A.U.; Gabrysch, S. Ramadan Is Not the Same As Ramadan Fasting. J. Nutr. 2020, 150, 968. [Google Scholar] [CrossRef] [PubMed]
- Quaresima, P.; Visconti, F.; Interlandi, F.; Puccio, L.; Caroleo, P.; Amendola, G.; Morelli, M.; Venturella, R.; Di Carlo, C. Awareness of gestational diabetes mellitus foetal-maternal risks: An Italian cohort study on pregnant women. BMC Pregnancy Childbirth 2021, 21, 692. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Country | Author, Year of Publication | Year of Data Collection | Age | Sample | Exposure Estimation (in Utero Ramadan Exposure) Based on | Outcome Measures Including Results | Quality Assessment Score (Max. 13) |
|---|---|---|---|---|---|---|---|
| Indonesia | Pradella and van Ewijk, 2018 [21] | 1997–2008 | ≥15 | 28,489 | date of birth | wheezing ↔, breathing difficulty ↓ | 11 |
| Indonesia | van Ewijk et al., 2013 [22] | 2000 | ≥18 | 43,649 | date of birth | height ↓, weight ↓, BMI ↓ | 11 |
| Indonesia | Van Ewijk, 2011 [23] | 2000 | ≥18 | 29,695 | date of birth | measurements of physical condition (nine-point general health scale) ↓, blood pressure ↔, pulse ↓, hemoglobin level ↔, risk of slow-healing wounds ↓, chest pain ↓ | 8 |
| Indonesia | Majid et al., 2019 [24] | 1993 and 2007 | 8–15, 18–65 | Raven’s CPM: 3514, score: 3521, hours worked: 7780, earnings: 6438 | date of birth | Raven’s Colored Progressive Matrices (CPM) ↓ and mathematics score ↓ (age 8–15); mean hours worked ↓ and earnings ↔ (age 18–65) | 12 |
| Indonesia | Kunto and Mandemakers, 2019 [26] | 1993/1994, 1997/1998, 2000, 2007/2008, and 2014/2015. | 0–19 | 45,246 | date of birth | height-for-age Z-scores T ↓, weight-for-age Z-scores ↔, body-mass-index-for-age Z-scores T ↔ | 11 |
| Indonesia | Majid, 2015 [25] | 1993, 1997, 2000, 2007 | 6–14, 21–29 | 19,038 | date of birth | Raven’s CPM ↓ and mathematics score ↓ (age 6–14); mean hours worked ↓ and employment ↓ (age 21–29); child labor ↓ | 9 |
| Pakistan | Chaudhry and Mir, 2021 [27] | 2007–2008, 2010–2011, 2013–2014, 2017–2018 | 0–5 | 179,943 | date of birth | height-for-age Z-scores T ↓ | 12 |
| Iran | Azizi et al., 2004 [28] | 2001 | 4–13 | 191 | mothers who fasted during Ramadan (questionnaire) | IQ score ↔ | 8 |
| Iran | Karimi et al., 2021 [29] | 2011 | 0–18 | 96,114 | date of birth | height-for-age Z-scores T ↔ | 10 |
| England | Almond et al., 2011 [31] | 2002 | 7 | NA | date of birth | test score on mathematicsT ↓, reading T ↓, writing T ↓ | 9 |
| Denmark | Greve et al., 2017 [32] | 1985–1995 | 16 | NA | mothers and children immigrated from a Muslim country (≥90% Muslims) | test score on Danish T ↔, English T ↔, mathematics T ↔, science T ↔ | 9 |
| Denmark | Schultz-Nielsen et al., 2016 [33] | 2008 | 24–55 | 38,637 | date of birth | employment T ↓, annual salary T ↔, hourly wage rate T ↔, hours of work T ↔ | 9 |
| Burkina Faso | Schoeps et al., 2018 [12] | 1993–2012 | 0–5 | 41,025 | date of birth | under-five mortality rateT ↓ | 12 |
| Ethiopia | Lee et al., 2020 [30] | 2000, 2005, 2011 | 0–4, 7–11, 15–20 | 21,425 | month of birth | mortality rate under three months T ↓, mortality rate under one year T ↓, underweight T ↔, anemia T ↔ (age 0–4); currently enrolled in a school T ↔ (age 7–11); graduated primary school T ↔ (age 15–20) | 11 |
| USA, Iraq, Uganda | Almond and Mazumder, 2011 [34] | 1989–2006 | Iraq: 20–39, Uganda: 20–80 | Iraq: 250,000+, Uganda: 80,000 | date of birth | disability T ↓, home ownership T ↓, employment T ↔ | 9 |
| International | Karimi and Basu, 2018 [35] | Varied across countries | 3–4 | 308,879 | date of birth | height-for-age Z-scores ↓ | 9 |
| Outcome Measures among Exposed Group | Study Results |
|---|---|
| Health outcomes | |
| Body mass index (BMI) | Age-adjusted BMI difference (Δ): −0.32, 95% CI: −0.57, −0.06 [22] BMI Δ: −0.094 SD, p < 0.10 T3 [26] |
| Height | Age-adjusted height Δ: −0.80 cm, 95% CI: −1.33, −0.26 [22] Height-for-age Z-score Δ: −0.105 SD, p < 0.05 T1 [26] Height-for-age Z-score Odds ratio: 1.225, p < 0.001 T2 [27] Height-for-age Z-score Δ: −0.091 SD, p < 0.01 T2 [29] Height-for-age Z-score Δ: girls: 0.019, p = 0.613; boys: −0.073, p = 0.001 [35] |
| Weight | Age-adjusted weight Δ: −0.85 kg, 95% CI: −1.54, −0.17 [22] Weight-for-age Z-score Δ: −0.387 SD, p < 0.05 [26] Age-adjusted weight Δ: −0.014, p > 0.10 T1 [30] |
| Disability | General disability: DID coefficient: 0.819, p < 0.05 T0 [34] Vision: DID coefficient: 0.349, p < 0.10 T0 [34] Hearing: DID coefficient: 0.243, p < 0.05 T0 [34] Learning: DID coefficient: 0.250, p < 0.001 T0 [34] |
| IQ scores | Mean crude full-scale IQ scores: exposed 111 ± 10, unexposed 112 ± 10 [28] |
| Test scores | Mathematics Δ: girls: −0.086, 95% CI: −0.158, −0.013 [24] Mathematics Δ: boys: −0.085, 95% CI: −0.151, −0.019 [24] Mathematics Δ: −0.084, p < 0.01 [25] DID coefficient −0.054, p < 0.05 T1 [31] DID coefficient −0.022, p > 0.10 T0 [32] Reading: DID coefficient −0.049, p < 0.05 T0 [31] Writing: DID coefficient −0.051, p < 0.05 T0 [31] English: DID coefficient −0.021, p > 0.10 T0 [32] Raven’s CPM tests: girls: −0.092, 95% CI: −0.150, −0.03 [24] Raven’s CPM tests: boys: −0.056, 95% CI: −0.109, −0.004 [24] Raven’s CPM tests: −7.4%, p < 0.01 [25] Danish: DID coefficient −0.008, p > 0.10 T0 [32] Science: DID coefficient −0.096, p > 0.10 T0 [32] |
| Wheezing | Odds ratio: 1.26, p = 0.087 [21] among 45+ years odds ratio: 1.41, 95% CI: 0.39, 5.13 [21] |
| Any breathing difficulty | Odds ratio: 1.17, p = 0.022 [21] |
| General health | Age-adjusted mean Δ: −0.061, p < 0.01 [23] |
| Blood pressure | Age-adjusted mean Δ: −0.030, p > 0.10 [23] |
| Pulse pressure | Age-adjusted mean Δ: 0.939, p < 0.01 [23] |
| Hemoglobin level | Age-adjusted mean Δ: −0.054, p < 0.10 [23] Age-adjusted mean Δ: −0.050, p > 0.10 T1 [30] |
| Risk of slow-healing wounds | Age-adjusted mean Δ: 0.047, p < 0.01 [23] |
| Chest pain | Age-adjusted mean Δ: 0.088, p < 0.05 [23] |
| Under-five mortality rate | Hazard ratio: 1.37, p = 0.03 T0 [12] |
| Hazard ratio: 1.33, p = 0.01 T1 [12] | |
| Hazard ratio: 1.25, p = 0.05 T2 [12] | |
| Mortality under one day | Age-adjusted mean Δ: 0.005, p > 0.10 T1 [30] |
| Mortality under three months | Age-adjusted mean Δ: 0.021, p < 0.05 T1 [30] |
| Mortality under one year | Age-adjusted mean Δ: 0.027, p < 0.05 T1 [30] |
| Economic outcomes | |
| Earnings | Δ: −0.042, 95% CI: −0.180, 0.097 [24] DID coefficient: −0.017, p > 0.10 T0 [33] |
| Annual salary | DID coefficient: −0.012, p > 0.10 T0 [33] |
| Home ownership | DID coefficient: −0.026 p = 0.027 T0 [34] |
| Employment | Regression coefficient: −0.026, p < 0.05 T3 [33] Regression coefficient: 0.000, p > 0.10 T0 [34] |
| Hours worked | Δ: −0.075, 95% CI: −0.145, −0.016 [24] Δ: −4.7%, p < 0.05 [25] DID coefficient: 0.007, p > 0.10 T0 [33] |
| Self-employed | Δ: 0.032, p < 0.05 [25] |
| Child labor | Δ: 0.039, p < 0.05 [25] |
| Currently enrolled in a school | Age-adjusted mean Δ: 0.024, p > 0.10 T1 [30] |
| Graduated primary school | Age-adjusted mean Δ: 0.048, p > 0.10 T1 [30] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahanani, M.R.; Abderbwih, E.; Wendt, A.S.; Deckert, A.; Antia, K.; Horstick, O.; Dambach, P.; Kohler, S.; Winkler, V. Long-Term Outcomes of in Utero Ramadan Exposure: A Systematic Literature Review. Nutrients 2021, 13, 4511. https://doi.org/10.3390/nu13124511
Mahanani MR, Abderbwih E, Wendt AS, Deckert A, Antia K, Horstick O, Dambach P, Kohler S, Winkler V. Long-Term Outcomes of in Utero Ramadan Exposure: A Systematic Literature Review. Nutrients. 2021; 13(12):4511. https://doi.org/10.3390/nu13124511
Chicago/Turabian StyleMahanani, Melani R., Eman Abderbwih, Amanda S. Wendt, Andreas Deckert, Khatia Antia, Olaf Horstick, Peter Dambach, Stefan Kohler, and Volker Winkler. 2021. "Long-Term Outcomes of in Utero Ramadan Exposure: A Systematic Literature Review" Nutrients 13, no. 12: 4511. https://doi.org/10.3390/nu13124511
APA StyleMahanani, M. R., Abderbwih, E., Wendt, A. S., Deckert, A., Antia, K., Horstick, O., Dambach, P., Kohler, S., & Winkler, V. (2021). Long-Term Outcomes of in Utero Ramadan Exposure: A Systematic Literature Review. Nutrients, 13(12), 4511. https://doi.org/10.3390/nu13124511