Effect of Calcium Fortified Foods on Health Outcomes: A Systematic Review and Meta-Analysis

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Type of Studies
2.1.2. Type of Participants
2.1.3. Type of Fortification (Interventions)
2.1.4. Type of Outcomes
2.2. Search Strategy for Identification of Studies and Data Sources
2.3. Data Collection and Analysis
2.3.1. Risk of Bias Assessment
2.3.2. Statistical Analyses
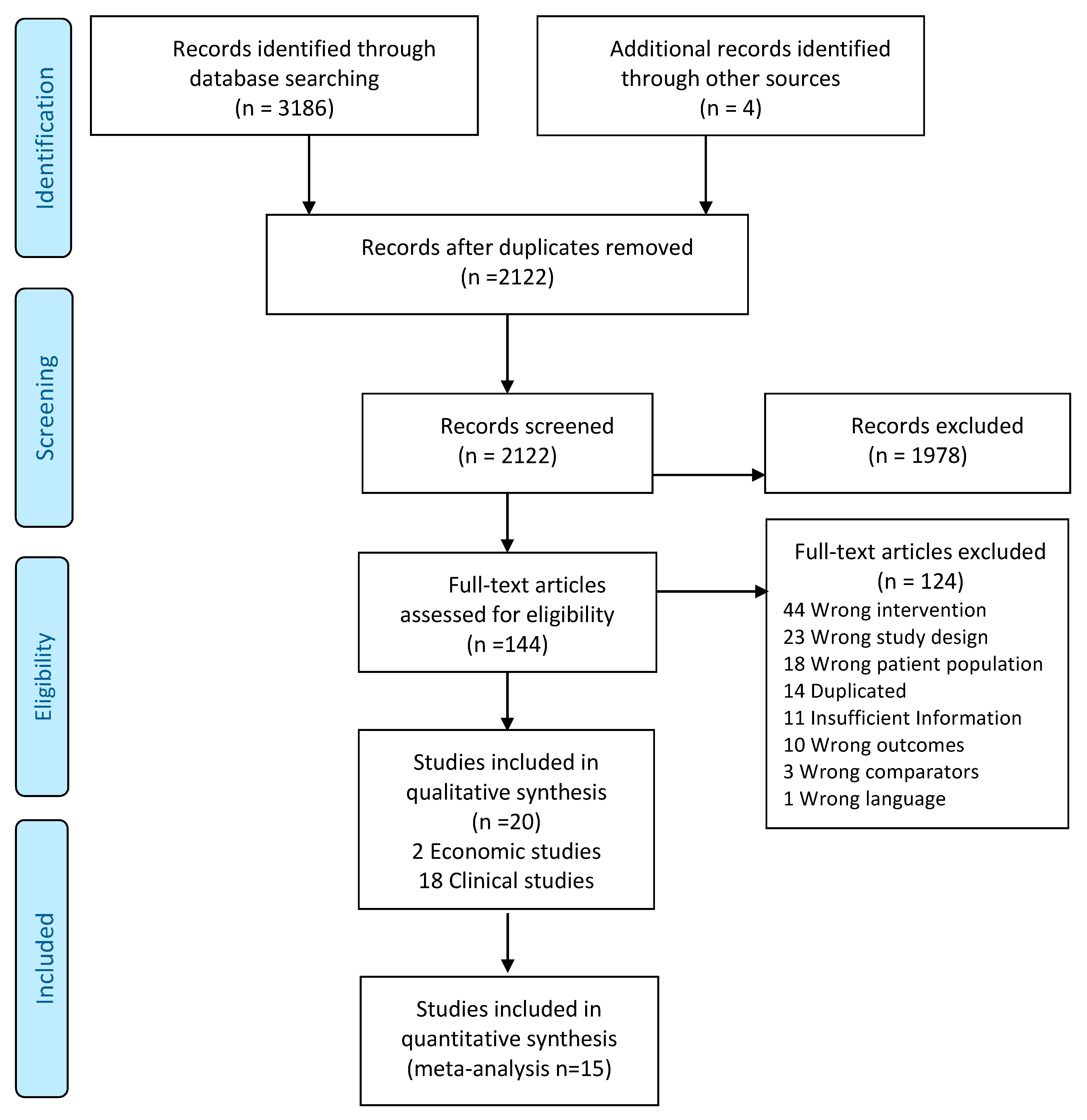
3. Results
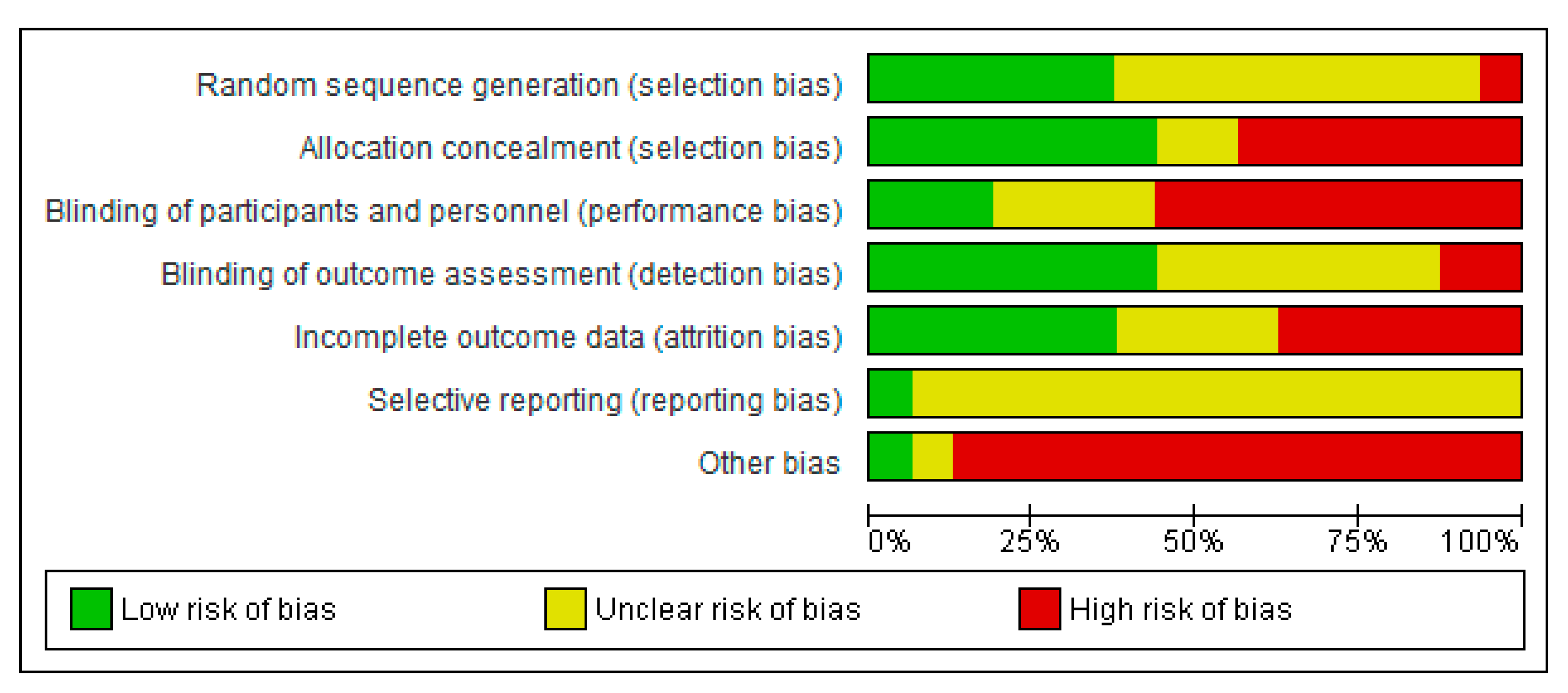
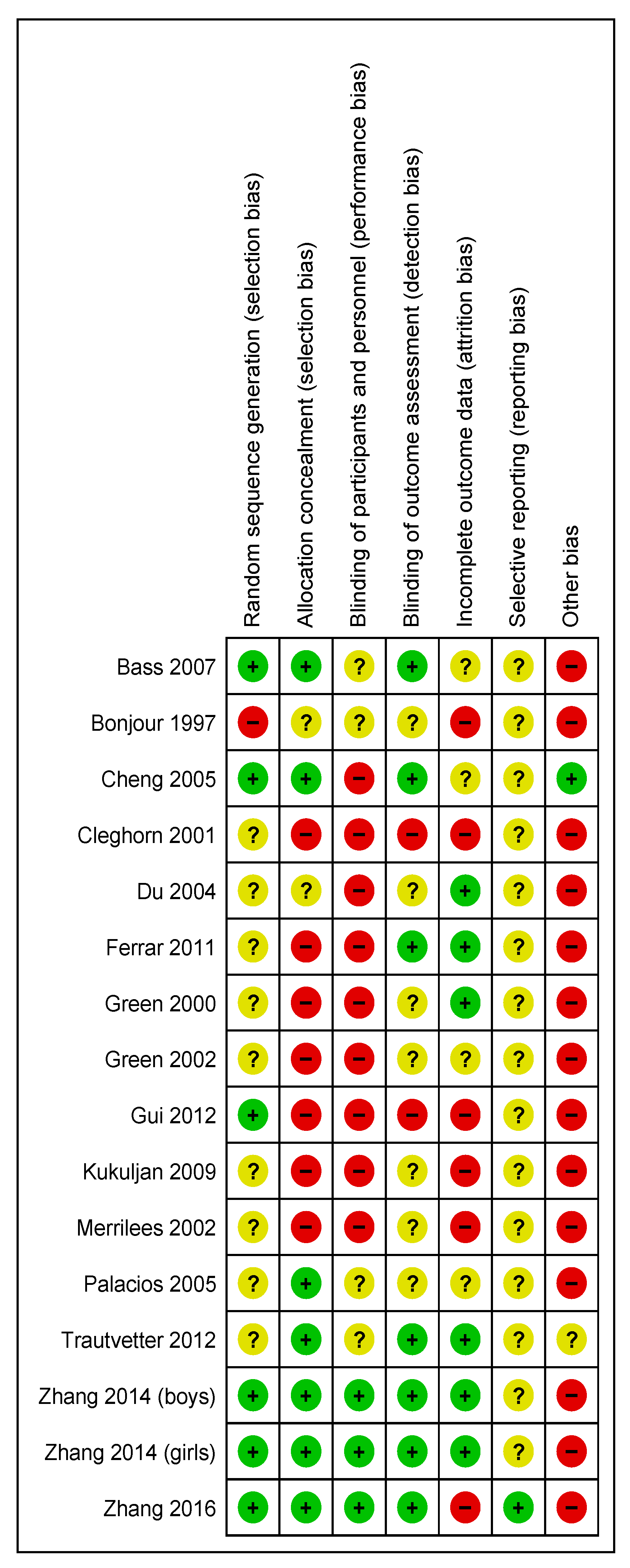
3.1. Risk of Bias of Included RCTs
3.2. Descriptive Synthesis of Clinical Studies
3.3. Synthesis of Economic Studies
3.4. Effect of Interventions
3.5. Calcium Intake
3.6. Anthropometric Outcomes
3.7. Outcomes Related to Calcium Metabolism
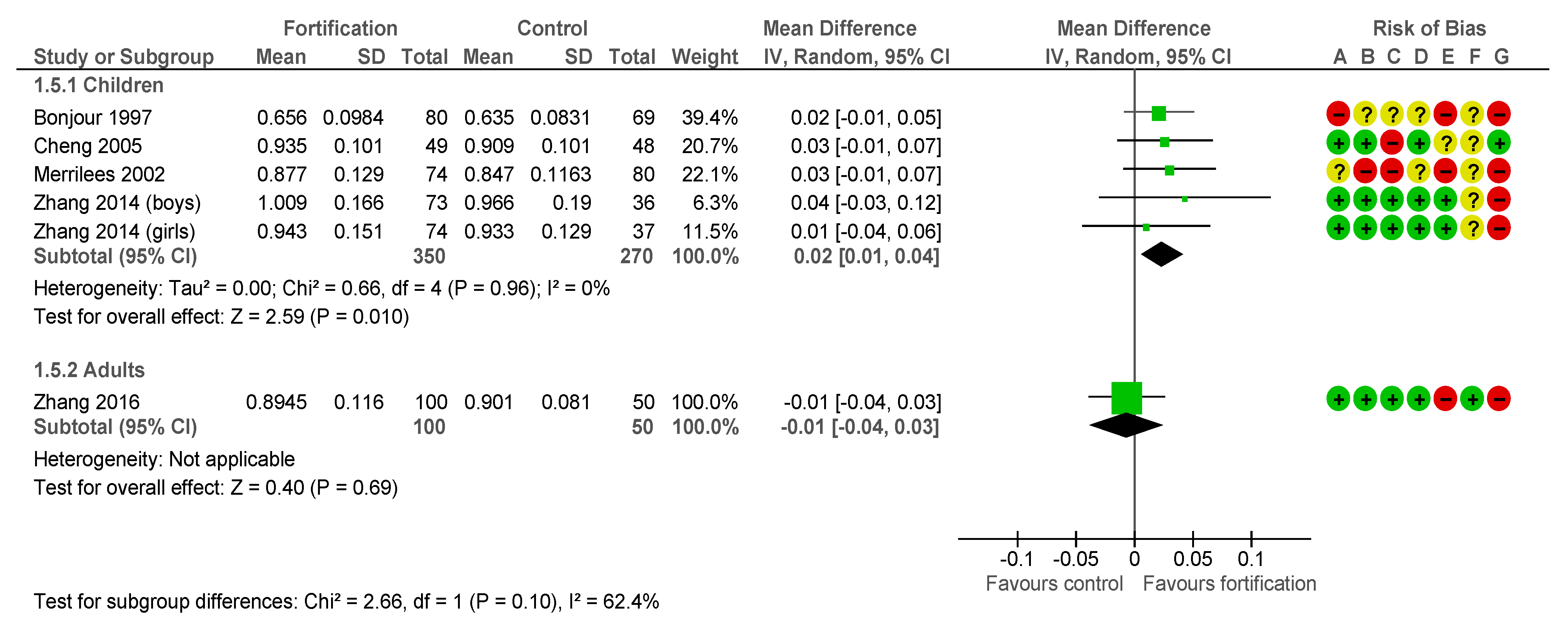
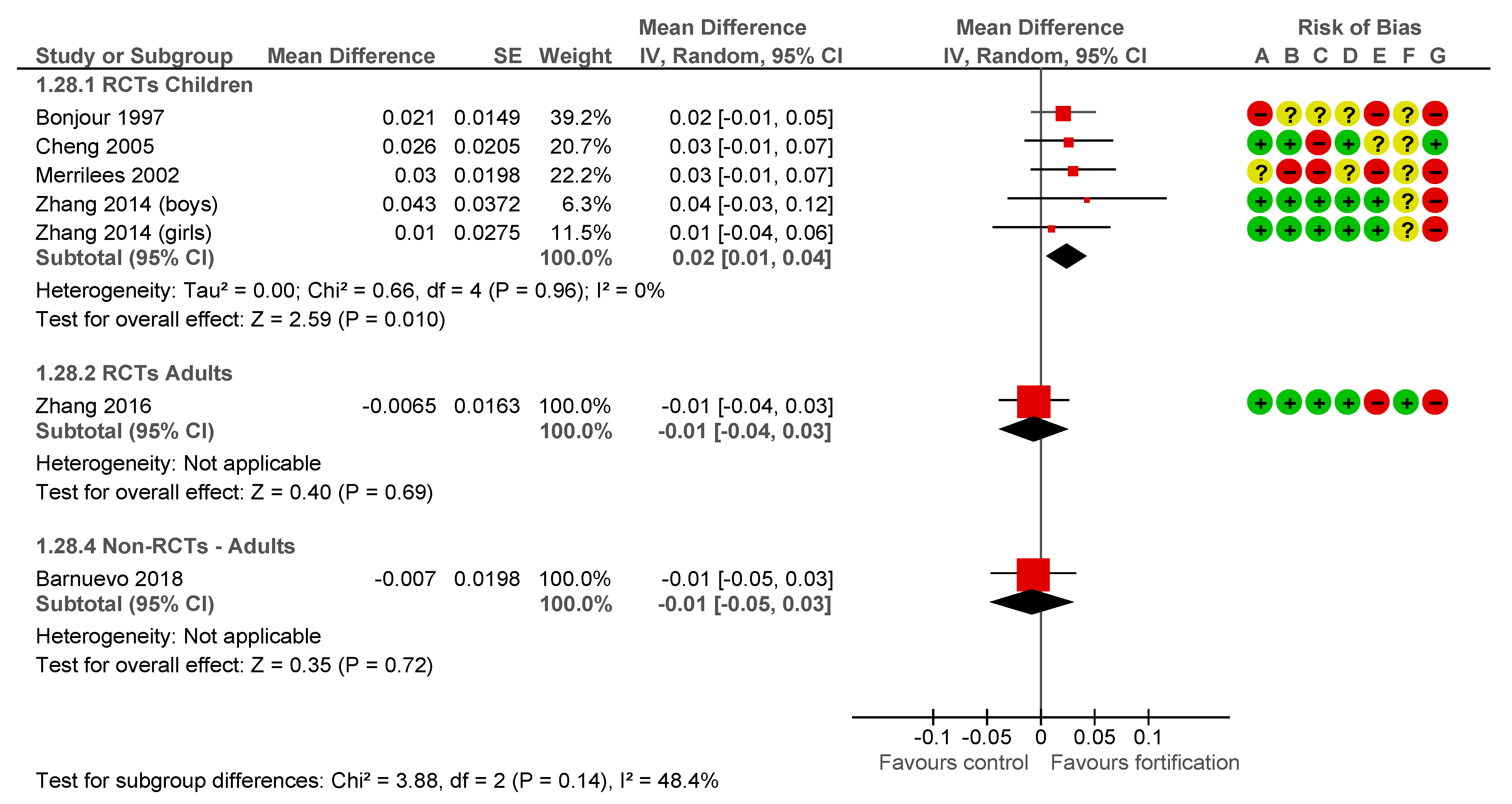
3.8. Outcomes Related to Bone Structure
3.9. Other Outcomes
3.10. Sensitivity and Subgroup Analysis
3.11. Economic Studies
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Query Results |
|---|---|
| #41. | #31 AND #35 AND #40 |
| #40. | #36 OR #37 OR #38 OR #39 |
| #39. | ca:ti,ab |
| #38. | calcium:ti,ab |
| #37. | ‘calcium intake’/exp |
| #36. | ‘calcium’/exp |
| #35. | #32 OR #33 OR #34 |
| #34. | enriched*:ti,ab |
| #33. | fortificat*:ti,ab |
| #32. | biofortificat*:ti,ab |
| #31. | #31. #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 |
| #30. | tortilla*:ti,ab |
| #29. | biscuit*:ti,ab |
| #28. | bread:ti,ab |
| #27. | ‘bread’/exp |
| #26. | flour:ti,ab |
| #25. | ‘flour’/exp |
| #24. | cheese:ti,ab |
| #23. | ‘cheese’/exp |
| #22. | eggs:ti,ab |
| #21. | egg:ti,ab |
| #20. | milk:ti,ab |
| #19. | meat:ti,ab |
| #18. | yam:ti,ab |
| #17. | ‘yam’/exp |
| #16. | cassava:ti,ab |
| #15. | ‘cassava’/exp |
| #14. | potato:ti,ab |
| #13. | ‘potato’/exp |
| #12. | millet*:ti,ab |
| #11. | ‘millet’/exp |
| #10. | corn:ti,ab |
| #9. | maize:ti,ab |
| #8. | maize’/exp |
| #7. | rice:ti,ab |
| #6. | ‘rice’/exp |
| #5. | ‘basic meal’:ti,ab |
| #4. | ‘essential meal’:ti,ab |
| #3. | ‘basic food’:ti,ab |
| #2. | ‘essential food’:ti,ab |
| #1. | staple*:ti,ab |
| Search | Query |
| #36 | (#26 AND #30 AND #35) |
| #35 | (#31 OR #32 OR #33 OR #34) |
| #34 | Ca[tiab] |
| #33 | Calcium[tiab] |
| #32 | Calcium, Dietary [Mesh] |
| #31 | Calcium [Mesh] |
| #30 | (#27 OR #28 OR #29) |
| #29 | Enriched*[tiab] |
| #28 | Fortifi*[tiab] |
| #27 | Biofortificat*[tiab] |
| #26 | (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25) |
| #25 | Tortilla*[tiab] |
| #24 | Biscuit*[tiab] |
| #23 | Bread[tiab] |
| #22 | Bread [Mesh] |
| #21 | Flour [tiab] |
| #20 | Flour [Mesh] |
| #19 | Cheese*[tiab] |
| #18 | Cheese [Mesh] |
| #17 | Eggs[tiab] |
| #16 | Egg[tiab] |
| #15 | Milk[tiab] |
| #14 | Meat[tiab] |
| #13 | Yam[tiab] |
| #12 | Cassava[tiab] |
| #11 | Potato*[tiab] |
| #10 | Solanum Tuberosum [Mesh] |
| #9 | Millet*[tiab] |
| #8 | Millets [Mesh] |
| #7 | Corn[tiab] |
| #6 | Rice[tiab] |
| #5 | Basic Meal*[tiab] |
| #4 | Essential Meal*[tiab] |
| #3 | Basic Food*[tiab] |
| #2 | Essential Food*[tiab] |
| #1 | Staple*[tiab] |
| # | Query |
| S29 | S21 AND S25 AND S28 |
| S28 | S26 OR S27 |
| S27 | TI Ca OR AB Ca |
| S26 | TI Calcium OR AB Calcium |
| S25 | S22 OR S23 OR S24 |
| S24 | TI Enriched* OR AB Enriched* |
| S23 | TI Fortifi* OR AB Fortifi* |
| S22 | TI Biofortificat* OR AB Biofortificat* |
| S21 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 |
| S20 | TI Tortilla* OR AB Tortilla* |
| S19 | TI Biscuit* OR AB Biscuit* |
| S18 | TI Bread OR AB Bread |
| S17 | TI Flour OR AB Flour |
| S16 | TI Cheese* OR AB Cheese* |
| S15 | TI(Egg OR Eggs) OR AB (Egg OR Eggs) |
| S14 | TI Milk OR AB Milk |
| S13 | TI Meat OR AB Meat |
| S12 | TI Yam OR AB Yam |
| S11 | TI Cassava OR AB Cassava |
| S10 | TI Potato* OR AB Potato* |
| S9 | TI Millet* OR AB Millet* |
| S8 | TI Corn OR AB Corn |
| S7 | TI Maize OR AB Maize |
| S6 | TI Rice OR AB Rice |
| S5 | TI “Basic Meal” OR AB “Basic Meal” |
| S4 | TI “Essential Meal” OR AB “Essential Meal” |
| S3 | TI “Basic Food” OR AB “Basic Food” |
| S2 | TI “Essential Food” OR AB “Essential Food” |
| S1 | TI Staple* OR AB Staple* |
| # | Query |
| S36 | S25 AND S30 AND S35 |
| S35 | S31 OR S32 OR S33 OR S34 |
| S34 | TI Ca OR AB Ca |
| S33 | TI Calcium OR AB Calcium |
| S32 | (MH “Calcium, Dietary”) |
| S31 | (MH “Calcium”) |
| S30 | S26 OR S27 OR S28 OR S29 |
| S29 | (MH “Food, Fortified”) |
| S28 | TI Enriched* OR AB Enriched* |
| S27 | TI Fortifi* OR AB Fortifi* |
| S26 | TI Biofortificat* OR AB Biofortificat* |
| S25 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 |
| S24 | TI Tortilla* OR AB Tortilla* |
| S23 | TI Biscuit* OR AB Biscuit* |
| S22 | TI Flour OR AB Flour |
| S21 | TI Bread OR AB Bread |
| S20 | (MH “Bread”) |
| S19 | TI Cheese* OR AB Cheese* |
| S18 | (MH “Cheese”) |
| S17 | TI (Egg OR Eggs) OR AB (Egg OR Eggs) |
| S16 | TI Milk OR AB Milk |
| S15 | TI Yam OR AB Yam |
| S14 | TI Cassava OR AB Cassava |
| S13 | TI Potato* OR AB Potato* |
| S12 | (MH “Potato”) |
| S11 | TI Millet* OR AB Millet* |
| S10 | TI Corn OR AB Corn |
| S9 | TI Maize OR AB Maize |
| S8 | (MH “Corn”) |
| S7 | TI Rice OR AB Rice |
| S6 | (MH “Rice”) |
| S5 | TI “Basic Meal” OR AB “Basic Meal” |
| S4 | TI “Essential Meal” OR AB “Essential Meal” |
| S3 | TI “Basic Food” OR AB “Basic Food” |
| S2 | TI “Essential Food” OR AB “Essential Food” |
| S1 | TI Staple* OR AB Staple* |
| # ▲ | es |
| 1 | Staple*.ti,ab. |
| 2 | Essential Food*.ti,ab. |
| 3 | Basic Food*.ti,ab. |
| 4 | Essential Meal*.ti,ab. |
| 5 | Basic Meal*.ti,ab. |
| 6 | Rice.ti,ab. |
| 7 | Corn.ti,ab. |
| 8 | Maize.ti,ab. |
| 9 | Millet*.ti,ab. |
| 10 | Potato*.ti,ab. |
| 11 | Cassava.ti,ab. |
| 12 | Yam.ti,ab. |
| 13 | Meat.ti,ab. |
| 14 | Milk.ti,ab. |
| 15 | (Egg or Eggs).ti,ab. |
| 16 | Cheese*.ti,ab. |
| 17 | Flour.ti,ab. |
| 18 | Bread.ti,ab. |
| 19 | Biscuit*.ti,ab. |
| 20 | Tortilla*.ti,ab. |
| 21 | or/1-20 |
| 22 | Biofortificat*.ti,ab. |
| 23 | Fortificat*.ti,ab. |
| 24 | Enriched*.ti,ab. |
| 25 | or/22-24 |
| 26 | Calcium.ti,ab. |
| 27 | Ca.ti,ab. |
| 28 | 26 or 27 |
| 29 | 21 and 25 and 28 |
| ID | Hits |
| #1 | Staple*:ti,ab,kw |
| #2 | (Essential NEAR/2 Food*):ti,ab,kw |
| #3 | (Basic NEAR/2 Food*):ti,ab,kw |
| #4 | (Essential NEAR/2 Meal*):ti,ab,kw |
| #5 | (Basic NEAR/2 Meal*):ti,ab,kw |
| #6 | MeSH descriptor: [Oryza] explode all trees |
| #7 | Rice:ti,ab,kw |
| #8 | MeSH descriptor: [Zea mays] explode all trees |
| #9 | Corn:ti,ab,kw |
| #10 | Maize:ti,ab,kw |
| #11 | MeSH descriptor: [Millets] explode all trees |
| #12 | Millet*:ti,ab,kw |
| #13 | MeSH descriptor: [Solanum tuberosum] explode all trees |
| #14 | Potato*:ti,ab,kw |
| #15 | Cassava:ti,ab,kw |
| #16 | Yam:ti,ab,kw |
| #17 | Meat:ti,ab,kw |
| #18 | Milk:ti,ab,kw |
| #19 | Egg:ti,ab,kw OR Eggs:ti,ab,kw |
| #20 | MeSH descriptor: [Cheese] explode all trees |
| #21 | Cheese*:ti,ab,kw |
| #22 | MeSH descriptor: [Flour] explode all trees |
| #23 | Flour:ti,ab,kw |
| #24 | MeSH descriptor: [Bread] explode all trees |
| #25 | Bread:ti,ab,kw |
| #26 | Biscuit*:ti,ab,kw |
| #27 | Tortilla*:ti,ab,kw |
| #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28; (*): truncation. |
| Author | Reason for Exclusion | Comments |
|---|---|---|
| ADOLPHI 2009 [63] | Wrong study design | Duration less than 1 month |
| DITSCHEID 2009 [64] | Wrong study design | Cross-over trial without washout |
| FONOLLA-JOYA 2016 [65] | Wrong intervention | Only the intervention arm contained Vit D and other micronutrients |
| HO 2005 [66] | Wrong intervention | Only the intervention arm contained Vit D |
| KRUGER 2006 [67] | Wrong comparator | The comparison has phylloquinone |
| LEE 2015 [68] | Wrong study design | Duration less than 1 month |
| LUTWAK 1964 [69] | Wrong study design | Non-randomised study, no basal information |
References
- Balk, E.M.; Adam, G.P.; Langberg, V.N.; Earley, A.; Clark, P.; Ebeling, P.R.; Mithal, A.; Rizzoli, R.; Zerbini, C.A.F.F.; Pierroz, D.D.; et al. Global dietary calcium intake among adults: A systematic review. Osteoporos. Int. 2017, 28, 3315–3324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cormick, G.; Betrán, A.P.; Romero, I.B.; Lombardo, C.F.; Gülmezoglu, A.M.; Ciapponi, A.; Belizán, J.M. Global inequities in dietary calcium intake during pregnancy: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraví, F.D. WHO scientific group on the assessment of osteoporosis at primary care level, summary meeting report: Brussels, Belgium, 5–7 May 2004, World Health Organization, Geneva, Switzerland, 2007. J. Osteoporos. 2013, 2013. [Google Scholar] [CrossRef] [Green Version]
- Nazarko, L. Osteoporosis: Assessing the risk of fragility. Nurs. Resid. Care 2012, 14, 505. [Google Scholar] [CrossRef]
- Wiseman, M. The COMA report: Dietary reference values for food energy and nutrients for the United Kingdom. Br. Food J. 1992, 94, 7–9. [Google Scholar] [CrossRef]
- Ross, A.C.; Manson, J.A.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the institute of medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M.; Gordon, C.M.; Janz, K.F.; Kalkwarf, H.J.; Lappe, J.M.; Lewis, R.; O’Karma, M.; Wallace, T.C.; Zemel, B.S. The national osteoporosis foundation’s position statement on peak bone mass development and lifestyle factors: A systematic review and implementation recommendations. Osteoporos. Int. 2016, 27, 1281–1386. [Google Scholar] [CrossRef] [Green Version]
- Newberry, S.J.; Chung, M.; Shekelle, P.G.; Booth, M.S.; Liu, J.L.; Maher, A.R.; Motala, A.; Cui, M.; Perry, T.; Shanman, R.; et al. Vitamin D and calcium: A systematic review of health outcomes (Update). Evid. Rep. Technol. Assess. (Full. Rep.) 2014, 1–929. [Google Scholar] [CrossRef] [Green Version]
- Whiting, S.J.; Kohrt, W.M.; Warren, M.P.; Kraenzlin, M.I.; Bonjour, J.P. Food fortification for bone health in adulthood: A scoping review. Eur. J. Clin. Nutr. 2016, 70, 1099–1105. [Google Scholar] [CrossRef] [Green Version]
- McNellis, R.; Barnes, K.R. Vitamin D and calcium supplementation to prevent fractures in adults. Am. Fam. Physician 2014, 89, 897–898. [Google Scholar] [CrossRef] [PubMed]
- Reid, I.R.; Bolland, M.J. Controversies in medicine: The role of calcium and vitamin D supplements in adults. Med. J. Aust. 2019, 211, 468–473. [Google Scholar] [CrossRef]
- Cormick, G.; Belizán, J.M. Calcium intake and health. Nutrients 2019, 11, 1606. [Google Scholar] [CrossRef] [Green Version]
- Bonovas, S.; Fiorino, G.; Lytras, T.; Malesci, A.; Danese, S. Calcium supplementation for the prevention of colorectal adenomas: A systematic review and meta-analysis of randomized controlled trials. World J. Gastroenterol. 2016, 22, 4594–4603. [Google Scholar] [CrossRef] [PubMed]
- Cormick, G.; Ciapponi, A.; Cafferata, M.L.M.L.; Belizán, J.M.J.M. Calcium supplementation for prevention of primary hypertension. Cochrane Database Syst. Rev. 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Ge, S.; Li, S.; Wu, L.; Liu, T.; Li, C. The effects of dietary calcium supplements alone or with vitamin D on cholesterol metabolism. J. Cardiovasc. Nurs. 2017, 32, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyr, G.J.; Lawrie, T.A.; Atallah, A.N.; Duley, L.; Gj, H.; Ta, L.; Án, A.; Duley, L. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems (Review). Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Jamshidi, F.; Kelishadi, R. A systematic review on the effects of maternal calcium supplementation on offspring’s blood pressure. J. Res. Med. Sci. 2015, 20, 994–999. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Betrán, A.P.; Singata-Madliki, M.; Cormick, G.; Munjanja, S.P.; Fawcus, S.; Mose, S.; Hall, D.; Ciganda, A.; Seuc, A.H.; et al. Prepregnancy and early pregnancy calcium supplementation among women at high risk of pre-eclampsia: A multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2019, 393, 330–339. [Google Scholar] [CrossRef]
- WHO. WHO Recommendation on Calcium Supplementation before Pregnancy for the Prevention of Pre-Eclampsia and Its Complications; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Omotayo, M.O.; Martin, S.L.; Stoltzfus, R.J.; Ortolano, S.E.; Mwanga, E.; Dickin, K.L. With adaptation, the WHO guidelines on calcium supplementation for prevention of pre-eclampsia are adopted by pregnant women. Matern. Child. Nutr. 2018, 14, e12521. [Google Scholar] [CrossRef] [Green Version]
- Lewis, J.R.; Zhu, K.; Prince, R.L. Adverse events from calcium supplementation: Relationship to errors in myocardial infarction self-reporting in randomized controlled trials of calcium supplementation. J. Bone Min. Res. 2012, 27, 719–722. [Google Scholar] [CrossRef]
- Martin, S.L.; Omotayo, M.O.; Pelto, G.H.; Chapleau, G.M.; Stoltzfus, R.J.; Dickin, K.L. Adherence-specific social support enhances adherence to calcium supplementation regimens among pregnant women. J. Nutr. 2017, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imdad, A.; Jabeen, A.; Bhutta, Z.A. Role of calcium supplementation during pregnancy in reducing risk of developing gestational hypertensive disorders: A meta-analysis of studies from developing countries. BMC Public Health 2011, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, S.L.; Wawire, V.; Ombunda, H.; Li, T.; Sklar, K.; Tzehaie, H.; Wong, A.; Pelto, G.H.; Omotayo, M.O.; Chapleau, G.M.; et al. Integrating calcium supplementation into facility-based antenatal care services in western Kenya: A qualitative process evaluation to identify implementation barriers and facilitators. Curr. Dev. Nutr. 2018, 2. [Google Scholar] [CrossRef] [PubMed]
- Osendarp, S.J.M.; Martinez, H.; Garrett, G.S.; Neufeld, L.M.; De-Regil, L.M.; Vossenaar, M.; Darnton-Hill, I. Large-scale food fortification and biofortification in low- and middle-income countries: A review of programs, trends, challenges, and evidence gaps. Food Nutr. Bull. 2018, 39, 315–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; ISBN 9780470699515. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Proc. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E. Consolidated health economic evaluation reporting standards (CHEERS)-explanation and elaboration: A report of the ISPOR health economic evaluation publication guidelines good reporting practices task force. Value Health 2013. [Google Scholar] [CrossRef] [Green Version]
- Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia; Available online: www.covidence.org (accessed on 20 January 2021).
- Review Manager (RevMan) [Computer Program] Version 5.4 Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration. 2020. Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman (accessed on 20 January 2021).
- Bass, S.L.; Naughton, G.; Saxon, L.; Iuliano-Burns, S.; Daly, R.; Briganti, E.M.; Hume, C.; Nowson, C. Exercise and calcium combined results in a greater osteogenic effect than either factor alone: A blinded randomized placebo-controlled trial in boys. J. Bone Miner. Res. 2007. [Google Scholar] [CrossRef] [Green Version]
- Bonjour, J.P.; Carrie, A.L.; Ferrari, S.; Clavien, H.; Slosman, D.; Theintz, G.; Rizzoli, R. Calcium-enriched foods and bone mass growth in prepubertal girls: A randomized, double-blind, placebo-controlled trial. J. Clin. Investig. 1997. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.; Lyytikäinen, A.; Kröger, H.; Lamberg-Allardt, C.; Alén, M.; Koistinen, A.; Wang, Q.J.; Suuriniemi, M.; Suominen, H.; Mahonen, A.; et al. Effects of calcium, dairy product, and vitamin D supplementation on bone mass accrual and body composition in 10-12-y-old girls: A 2-y randomized trial. Am. J. Clin. Nutr. 2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleghorn, D.B.; O’Loughlin, P.D.; Schroeder, B.J.; Nordin, B.E.C. An open, crossover trial of calcium-fortified milk in prevention of early postmenopausal bone loss. Med. J. Aust. 2001, 175. [Google Scholar] [CrossRef]
- Du, X.; Zhu, K.; Trube, A.; Zhang, Q.; Ma, G.; Hu, X.; Fraser, D.R.; Greenfield, H. School-milk intervention trial enhances growth and bone mineral accretion in Chinese girls aged 10–12 years in Beijing. Br. J. Nutr. 2004, 92, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Ferrar, L.; Van Der Hee, R.M.; Berry, M.; Watson, C.; Miret, S.; Wilkinson, J.; Bradburn, M.; Eastell, R. Effects of calcium-fortified ice cream on markers of bone health. Osteoporos. Int. 2011. [Google Scholar] [CrossRef]
- Green, J.H.; Richards, J.K.; Bunning, R.L.W. Blood pressure responses to high-calcium skim milk and potassium-enriched high-calcium skim milk. J. Hypertens. 2000, 18, 1331–1339. [Google Scholar] [CrossRef]
- Green, J.H.; Booth, C.; Bunning, R. Impact of supplementary high calcium milk with additional magnesium on parathyroid hormone and biochemical markers of bone turnover in postmenopausal women. Asia Pac. J. Clin. Nutr. 2002. [Google Scholar] [CrossRef] [Green Version]
- Gui, J.C.; Brašié, J.R.; Liu, X.D.; Gong, G.Y.; Zhang, G.M.; Liu, C.J.; Gao, G.Q. Bone mineral density in postmenopausal Chinese women treated with calcium fortification in soymilk and cow’s milk. Osteoporos. Int. 2012. [Google Scholar] [CrossRef]
- Kukuljan, S.; Nowson, C.A.; Sanders, K.; Daly, R.M. Effects of resistance exercise and fortified milk on skeletal muscle mass, muscle size, and functional performance in middle-aged and older men: An 18-mo randomized controlled trial. J. Appl. Physiol. 2009. [Google Scholar] [CrossRef]
- Gibbons, M.J.; Gilchrist, N.L.; Frampton, C.; Maguire, P.; Reilly, P.H.; March, R.L.; Wall, C.R. The effects of a high calcium dairy food on bone health in pre-pubertal children in New Zealand. Asia Pac. J. Clin. Nutr. 2004, 13, 341–347. [Google Scholar]
- Palacios, S.; Castelo-Branco, C.; Cifuentes, I.; Von Helde, S.; Baró, L.; Tapia-Ruano, C.; Menéndez, C.; Rueda, C. Changes in bone turnover markers after calcium-enriched milk supplementation in healthy postmenopausal women: A randomized, double-blind, prospective clinical trial. Menopause 2005. [Google Scholar] [CrossRef]
- Trautvetter, U.; Ditscheid, B.; Kiehntopf, M.; Jahreis, G. A combination of calcium phosphate and probiotics beneficially influences intestinal lactobacilli and cholesterol metabolism in humans. Clin. Nutr. 2012. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Q.; Ma, X.M.; Huang, Z.W.; Yang, X.G.; Chen, Y.M.; Su, Y.X. Effects of milk salt supplementation on bone mineral gain in pubertal Chinese adolescents: A 2-year randomized, double-blind, controlled, dose-response trial. Bone 2014. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Q.; Chen, Y.M.; Wang, R.Q.; Huang, Z.W.; Yang, X.G.; Su, Y.X. The effects of different levels of calcium supplementation on the bone mineral status of postpartum lactating Chinese women: A 12-month randomised, double-blinded, controlled trial. Br. J. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnuevo, M.D.; Marhuenda, J.; Aldeguer, M.; Abellán, M.S.; Zafrilla Rentero, P.; Contreras, C.J.; Guillén, I.; Hernández, M.; López, F.J. In vivo randomized trial of three marketed milk preparations enriched with calcium and vitamins (D and K) on bone mass and bone turnover markers from biological fluids in premenopausal caucasian women. Nutr. Hosp. 2018. [Google Scholar] [CrossRef]
- González Sánchez, M.E.; Rivera Torres, A.; Morán Fagúndez, L.J. Estudio nutricional para evaluar el aporte de calcio sobre la dieta de una leche fermentada enriquecida en calcio y vitamina D (densia®) en mujeres postmenopáusicas. Nutr. Hosp. 2012. [Google Scholar] [CrossRef]
- Osler, M.; Heitmann, B.L. Food patterns, flour fortification, and intakes of calcium and vitamin D: A longitudinal study of Danish adults. J. Epidemiol. Community Health 1998. [Google Scholar] [CrossRef] [Green Version]
- Keller, J.L.; Lanou, A.J.; Barnard, N.D. The consumer cost of calcium from food and supplements. J. Am. Diet. Assoc. 2002, 102, 1669–1671. [Google Scholar] [CrossRef]
- Sandmann, A.; Amling, M.; Barvencik, F.; König, H.H.; Bleibler, F. Economic evaluation of vitamin D and calcium food fortification for fracture prevention in Germany. Public Health Nutr. 2017, 20, 1874–1883. [Google Scholar] [CrossRef] [Green Version]
- Villa-Etchegoyen, C.; Lombarte, M.; Matamoros, N.; Belizán, J.M.; Cormick, G. Mechanisms involved in the relationship between low calcium intake and high blood pressure. Nutrients 2019, 11, 1112. [Google Scholar] [CrossRef] [Green Version]
- Kumssa, D.B.; Joy, E.J.M.; Ander, E.L.; Watts, M.J.; Young, S.D.; Walker, S.; Broadley, M.R. Dietary calcium and zinc deficiency risks are decreasing but remain prevalent. Sci. Rep. 2015. [Google Scholar] [CrossRef] [Green Version]
- Rajwar, E.; Parsekar, S.S.; Venkatesh, B.T.; Sharma, Z. Effect of vitamin A, calcium and vitamin D fortification and supplementation on nutritional status of women: An overview of systematic reviews. Syst. Rev. 2020, 9, 248. [Google Scholar] [CrossRef] [PubMed]
- De Lourdes Samaniego-Vaesken, M.; Alonso-Aperte, E.; Varela-Moreiras, G. Vitamin food fortification today. Food Nutr. Res. 2012, 56, 5459. [Google Scholar] [CrossRef] [PubMed]
- Government of UK. The Bread and Flour Regulations 1998; Government of UK: London, UK, 1998; Volume 141, pp. 1–10.
- Department for Environment, Food and Rural Affairs. Bread and Flour Regulations. A Summary of Responses to the Consultation and Government Reply. 1998. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/226553/bread-flour-sum-resp-130805.pdf (accessed on 10 December 2020).
- Cormick, G.; Betrán, A.P.; Metz, F.; Palacios, C.; Beltrán-Velazquez, F.; De Las Nieves García-Casal, M.; Peña-Rosas, J.P.; Hofmeyr, G.J.; Belizán, J.M. Regulatory and policy-related aspects of calcium fortification of foods. Implications for implementing national strategies of calcium fortification. Nutrients 2020, 12, 1022. [Google Scholar] [CrossRef] [Green Version]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Baron, J.A.; Burckhardt, P.; Li, R.; Spiegelman, D.; Specker, B.; Orav, J.E.; Wong, J.B.; Staehelin, H.B.; et al. Calcium intake and hip fracture risk in men and women: A meta-analysis of prospective cohort studies and randomized controlled trials. Am. J. Clin. Nutr. 2007, 86. [Google Scholar] [CrossRef]
- Kahwati, L.C.; Weber, R.P.; Pan, H.; Gourlay, M.; LeBlanc, E.; Coker-Schwimmer, M.; Viswanathan, M. Vitamin D, Calcium, or Combined Supplementation for the Primary Prevention of Fractures in Community-Dwelling Adults. JAMA 2018, 319. [Google Scholar] [CrossRef] [PubMed]
- Reid, I.R.; Bolland, M.J. Calcium and/or Vitamin D Supplementation for the Prevention of Fragility Fractures: Who Needs It? Nutrients 2020, 12, 1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, I.R.; Bristow, S.M. Calcium and Bone. Handb. Exp. Pharmacol. 2020, 262, 259–280. [Google Scholar] [PubMed]
- Adolphi, B.; Scholz-Ahrens, K.E.; De Vrese, M.; Açil, Y.; Laue, C.; Schrezenmeir, J. Short-term effect of bedtime consumption of fermented milk supplemented with calcium, inulin-type fructans and caseinphosphopeptides on bone metabolism in healthy, postmenopausal women. Eur. J. Nutr. 2009, 48, 45–53. [Google Scholar] [CrossRef]
- Ditscheid, B. Faecal steroid excretion in humans is affected by calcium supplementation and shows gender-specific differences. Eur. J. Nutr. 2009, 22–30. [Google Scholar] [CrossRef]
- Fonolla-joya, J.; Reyes-garcía, R.; García-, A.; Reyes-garcía, R.; García, A.; Fonolla-joya, J.; Reyes-garc, R. Daily intake of milk enriched with n-3 fatty acids, oleic acid, and calcium improves metabolic and bone biomarkers in postmenopausal women. J. Am. Coll. Nutr. 2016, 5724. [Google Scholar] [CrossRef]
- Ho, S.C.; Guldan, G.S.; Woo, J.; Yu, R.; Tse, M.M.; Sham, A.; Cheng, J. A prospective study of the effects of 1-year calcium-fortified soy milk supplementation on dietary calcium intake and bone health in Chinese adolescent girls aged 14 to 16. Osteoporos. Int. 2005, 1907–1916. [Google Scholar] [CrossRef] [PubMed]
- Kruger, M.C.; Booth, C.L.; Coad, J.; Schollum, L.M.; Kuhn-Sherlock, B.; Shearer, M.J. Effect of calcium fortified milk supplementation with or without vitamin K on biochemical markers of bone turnover in premenopausal women. Nutrition 2006, 22, 1120–1128. [Google Scholar] [CrossRef]
- Lee, J.T.; Moore, C.E.; Radcliffe, J.D. Consumption of Calcium-Fortified Cereal Bars to Improve Dietary Calcium Intake of Healthy Women: Randomized Controlled Feasibility Study. PLoS ONE 2015, 10, e0125207. [Google Scholar] [CrossRef] [PubMed]
- Lutwak, L.; Laster, L.; Gitelman, H.; Fox, M.; Donald, G.; Wolfe, E.; Woodson, L. Effects of High Dietary Calcium and Phosphorus on Calcium, Phosphorus, Nitrogen and Fat Metabolism in Children. Am. J. Clin. Nutr. 1964, 14, 76–82. [Google Scholar] [CrossRef] [PubMed]





| Author | Region | Country | Population Characteristics | N | Study Design | Fortified Food | Baseline Calcium Intake mg/day | Intervention and Control Group Used for this Analysis | Food Fortification Level < 0.5; 0.5–1; >1 g/assigned Daily Portion | Calcium Intake Difference between Intervention and Control Group (mg/day) | Duration of Fortification (Months) | Main Outcome | Outcomes Assessed Included in This Review |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bass 2007 [32] | Western Pacific Region | Australia | Healthy boys between 7–11 years old | 88 | RCT | Cakes/cookies | I: 931 P:934 | Intervention: one out of 10 varieties of muffins and cookies a day. Muffins and cookies were fortified with 4 g of milk minerals powder, which provided participants with an additional 800 mg of elemental calcium per day. Placebo: one out of 10 varieties of muffins and cookies without added calcium. | 0.5–1 | 800 | 8.5 | Bone health | Calcium Intake, Weight, Height, BMC (total body, lumbar spine, leg (Femur + Tibia-Fibula), arm (Humerus + Ulna-Radius) |
| Bonjour 1997 [33] | Europe | Switzerland | Healthy prepubertal Caucasian girls. Mean age 7.93 years old | 149 | RCT | Cakes | NA | Intervention: Two food products every day in place of similar foods taken for breakfast or snacks fortified with calcium from milk extract. The calcium contents (mg/serving) of calcium-enriched food products was as follows: chocolate cakes, 516; caramel cakes, 512; biscuits, 548; fruit juices, 383; powdered drinking chocolate, 530; chocolate bars, 429; yogurts, 478. Calcium from milk extract was used to fortify food products. Placebo: Two food products every day in place of similar foods taken for breakfast or snacks without added calcium. The calcium contents (mg/serving) of placebo food products was as follows: chocolate cakes, 33; caramel cakes, 41; biscuits, 8; fruit juices, 11; powdered drinking chocolate, 4; chocolate bars, 80; yogurts, 174. | 0.5–1/>1 | -Chocolate cakes, 483 -Caramel cakes, 471 -Biscuits, 540 -Fruit juices, 372 -Powdered drinking chocolate, 526 -Chocolate bars, 349 -Yogurts, 304 | 11 | Bone health | Weight, Height, BMI, BMD (lumbar spine, femoral neck) |
| Cheng 2005 [34] | Europe | Finland | Girls aged 10–12 years old | 195 | RCT | Cheese | I: 706 P: 664 | Intervention: dairy products such as natural low-fat cheese (110 g Edam with 17% fat and 100 g Turunmaa with 15% fat) which provided a quantity equivalent to 1000 mg of elemental calcium a day. Placebo: calcium plus vitamin D supplements placebo. | 0.5–1 | 1000 | 24 | Bone health | Weight, Height, aBMD (lumbar spine, femoral neck, total femur), BMC total body. |
| Cleghorn 2001 [35] | Western Pacific Region | Australia | Women who were less than five years postmenopausal. | 142 | RCT-c | Milk | I: 967 C: 918 | Intervention: one litre of calcium-fortified milk thrice weekly (428 mL/d). Milk was fortified by adding to reduced-fat milk the retentate from ultrafiltration of low-fat milk. It contains 1600 mg of elemental calcium and 1200 mg phosphorus per litre providing an average of 685 mg of elemental calcium a day. Control: Usual diet | 0.5–1 | 686 | 24 | Bone health | Weight, BMD (Forearm, Lumbar spine L2–L4) |
| Du 2004 [36] | Western Pacific Region | China | Healthy girls aged 10 years old | 757 | RCT | Milk | I: 418.2 C: 455.3 | Intervention: 330 mL ultra-heat-treated (UHT) milk 5 days a week, which had been fortified to contain 560 mg of elemental calcium. It provided 245 mg of elemental calcium a day. Control: Usual diet | <0.5 | 245 | 24 | Bone health | Calcium Intake, Height, PTH, Plasma 25(OH)D, Plasma Ca, BMD Total body, BMI, Urine Ca/creatinine. |
| Ferrar 2011 [37] | Europe | UK | Young women ages 20 to 39 years old | 76 | RCT | Ice cream | I 1: 735 I 2: 663 I 3: 754 P: 714 | One per day Ice cream low in fat—Calcium, magnesium, phosphorus and zinc. Milk minerals (Arla Foods Ingredients, Redhill, Surrey, UK) Intervention Group 1: 60 g ice cream containing 244 mg of elemental Calcium fortified with milk minerals. Intervention Group 2: 60 g ice cream containing 459 mg of elemental Calcium fortified with milk minerals. Intervention Group 3: 60 g ice cream containing 676 mg of elemental Calcium fortified with milk minerals. Placebo: consumed 60 g of ice cream containing 96 mg calcium per unit. | <0.5/0.5–1 | I 1: 148 I 2: 363 I 3: 580 | 1 | Bone health | Calcium Intake, PTH, Serum 1,25D. |
| Green 2000 [38] | Western Pacific Region | New Zealand | Healthy volunteers aged over 40 years, 19 men and 19 women. | 38 | RCT-c | Milk | 1120 | A 4-week washout period separated consecutive milk interventions. Each volunteer consumed each of the milks in randomized order. Intervention: 50 g of high Calcium skim milk powder diluted in tap water to provide 480 mL of milk per day containing 1075 mg of elemental Calcium. Control: 50 g of skim milk powder diluted in tap water to provide 480 mL of milk per day containing 720 mg of Calcium. | >1 | 355 | 1 | Blood Pressure | Office sitting SBP (mmHg), office sitting DBP (mmHg), office standing SBP (mmHg), office standing DBP (mmHg). |
| Green 2002 [39] | Western Pacific Region | New Zealand | Healthy postmenopausal women (at least 5 years postmenopausal) | 50 | RCT | Milk | I: 850 C: 900 | Intervention: 400 mL of high-calcium skim milk powder containing 1200 mg of calcium supplemented with 172 mg magnesium per 50 g milk powder a day. Control: 400 mL of apple drink containing no more than 25% apple juice a day. | >1 | 1200 | 1 | Bone Health | Calcium Intake, Serum PTH (pmol/L), Serum Calcium. |
| Gui 2012 [40] | Western Pacific Region | China | Postmenopausal women without osteoporosis, aged 45–65, and postmenopausal for more than 2 years. | 141 | RCT | Soymilk | NA | Intervention: 250 mL calcium-fortified soymilk daily. Calcium-fortified soymilk contained 6.5 g soy protein, 2.5 g fat, 2.5 g lactose, 250 mg calcium, and 3.75 to 4.5 mg soy isoflavones. Control: Usual diet. They abstain from any other dietary supplementation, including other milk, other soymilk, vitamin D, vitamin K, complex vitamins, and calcium tablets. | <0.5 | 250 | 18 | Bone Health | BMD (spine, femoral neck, hip). |
| Kukuljan 2009 [41] | Western Pacific Region | Australia | Healthy community- dwelling Caucasian men aged 50–79 years | 180 | RCT- 2 by 2factorial design | Milk | I: 1039 C: 996 | Intervention: 400 mL milk per day of reduced-fat (1%) ultrahigh temperature (UHT) milk. Milk was fortified with milk salts containing 1000 mg calcium and 800 IU vitamin D3 and 500 mg phosphorous/day Control: Usual Diet. | 0.5–1 | 1000 | 18 | Bone Health | Calcium intake |
| Gibbons 2004 [42] | Western Pacific Region | New Zealand | Children, aged 8–10 years | 154 | RCT | Milk | I: 934 P: 985 | Intervention: 8O g of chocolate milk drink per day. The high calcium milk provided 1200 mg of elemental calcium and 776 mg phosphorus per day. Placebo: 8O g of chocolate milk drink per day. The milk provided 400 mg of elemental calcium and 320 mg of phosphorus per day. | >1 | 800 | 18 | Bone Health | Weight, Height, BMD (Lumbar spine, femoral Neck, total hip, trochanter, total body) and BMC (total body, trochanter, hip, femoral neck and spine) |
| Palacios 2005 [43] | Europe | Spain | Healthy white women, postmenopausal for 10 years or more, between 49 and 71 years old and with a dietary calcium intake lower than 750 mg/day | 79 | RCT | Milk | I: 508 P: 502 | Intervention: 750 mL of skimmed milk enriched with calcium 1200 mg, phosphorus 945 mg, lactose, and vitamin D3 5.7 mg per day. Placebo: 750 mL skimmed milk enriched with vitamin D3 (5.7 mg/750 mL) of identical appearance, taste, and composition to that of intervention group except for the amount of calcium (900 mg/750 mL) and this milk was not fortified with phosphorus or lactose. | >1 | 300 | 6 | Bone Health | Weight, 250H vitamin D3, Calcemia (mg/dL), calcium urine (mg/dL), calcium/creatinine (mg/mg) |
| Trautvetter 2012 [44] | Europe | Germany | Men and women omnivorous, moderately hypercholesterolemic subjects; aged 25.5 y and had a BMI of 22.3 kg/m2. | 32 | RCT-c | Bread | 873 | All subjects consumed 100 mL of the probiotic drink daily. Intervention: 135 g of bread a day fortified with 1000 mg of elemental calcium as pentacalcium hydroxy- triphosphate Control: 135 g of bread a day without added calcium. | 0.5–1 | 1000 | 3 | Cholesterol | Calcium Intake, Total cholesterol [mmol/L], LDL-cholesterol [mmol/L], HDL-cholesterol [mmol/L], LDL/HDL ratio, triacylglycerol [mmol/L] |
| Zhang 2014 [45] | Western Pacific Region | China | Healthy adolescents aged 12–14 years (111 girls and 109 boys) | 220 | RCT | Milk | Girls: I 1: 651 I 2: 707 C: 701 Boys: I 1: 758 I 2: 704 C: 680 | The subjects were assigned to receive 40 g of milk powder daily. Each daily dose was administered in two packages (approximately 20 g/package). Intervention 1: 40 g of milk powder containing 900 mg of calcium and 200 IU of vitamin D. For this fortification daily dose of 2g of isolated milk salt (containing 29.2% calcium and 15% phosphorus) was added to 40 g of milk. Intervention 2: 40 g of milk powder containing 600 mg of calcium and 200 IU of vitamin D. For this fortification daily dose of 1g of isolated milk salt (containing 29.2% calcium and 15% phosphorus) was added to 40 g of milk. Control: 40 g of milk powder containing 300 mg of calcium and 200 IU of vitamin D. | <0.5/0.5–1 | I 1: 600 I 2: 300 | 24 | Bone Health | Calcium Intake, Weight, Height, BMD and BMC (spine, femoral neck, left hip, total body, femoral shaft) |
| Zhang 2016 [46] | Western Pacific Region | China | Postpartum women aged 20–35 years. All were primipara who had delivered a normal single infant at full term and intended to be breast-feeding | 150 | RCT | Milk | I 1: 822 I 2: 811 C: 807 | The subjects were assigned to receive 40 g of milk powder daily for 12 months. Each daily dose was administered in two packages (approximately 20 g/package). Intervention 1: 40 g of milk powder containing 900 mg of calcium and 5 μg of vitamin D. For this fortification daily dose of 2g of isolated milk salt (containing 29.2% calcium and 15% phosphorus) was added to 40 g of milk. Intervention 2: 40 g of milk powder containing 600 mg of calcium and 5 μg of vitamin D. For this fortification daily dose of 1g of isolated milk salt (containing 29.2% calcium and 15% phosphorus) was added to 40 g of milk. Control: 40 g of milk powder containing 300 mg of calcium and 5 μg of vitamin D. | <0.5/0.5–1 | I 1: 600 I 2: 300 | 12 | Bone Health | Calcium Intake, Weight, BMD (spine, femoral neck, left hip, trochanter, total body) |
| Barnuevo 2018 [47] | Europe | Spain | Healthy female young volunteers. Mean age 39.2 ± 4.6 years old | 181 | RCT analyzed as UBAS | Milk | NA | Intervention: 250 mL a day of partly skimmed milk with 240 mg calcium and 105 mg of phosphorus. | <0.5 | NA | 18 | Bone health | BMD (lumbar spine, femoral neck, total hip, throcanteric region) |
| Gonzalez Sanchez 2012 [48] | Europe | Spain | Postmenopausal women, aged between 36 and 84 years, and who had low intake of calcium and vitamin D. | 261 | UBAS | Fermented Milk | 747.9 | Intervention: 125 g of Fermented milk (Densia®) per day, fortified with 400 mg of elemental calcium and 200 UI of Vit D. | <0.5 | 400 | 1 | Dietary Intake | Calcium intake |
| Osler 1998 [49] | Europe | Denmark | Men and women, aged 35–65 years at first examination in 1987, 1988 | 329 | UBAS | Flour | 1215 | Intervention: Flour fortified with calcium, 200 mg of elemental calcium per 100 g wheat flour and 400 mg of calcium per 100 g rye flour, since 1954, and until 1987 when the mandatory fortification was stopped. | <0.5 | NA | 72 | Dietary Intake | Calcium intake |
| Outcomes | Mean Difference (MD) of Fortified Versus Control Group * (95% CI) | No. of Participants (Studies) | Certainty of the Evidence (GRADE) |
|---|---|---|---|
| Calcium Intake (mg/day)—Children | MD 306.17 higher 198.97 higher to 413.38 higher) | 764 (4 RCTs) | ⨁⨁⨁◯ MODERATE a |
| Calcium Intake (mg/day)—Adults | MD 471.47 higher (266.51 higher to 676.42 higher) | 315 (3 RCTs) | ⨁⨁◯◯ LOW a,b |
| Calcium Intake (mg/day)—Postmenopausal Women | MD 1210 higher (1162.8 higher to 1257.2 higher) | 50 (1 RCT) | ⨁⨁◯◯ LOW c |
| Weight (kg)—Children | MD 0.22 higher (0.95 lower to 1.38 higher) | 667 (6 RCTs) | ⨁⨁⨁◯ MODERATE d |
| Weight (kg)—Adults | MD 1.85 higher (0.94 lower to 4.64 higher) | 150 (1 RCT) | ⨁⨁⨁◯ MODERATE e |
| Weight (kg)—Postmenopausal Women (Vit D cointervention in both groups) | MD 0.03 lower (4.11 lower to 4.05 higher) | 79 (1 RCT) | ⨁⨁⨁◯ MODERATE e |
| Height (cm)—Children | MD 0.83 higher (0 to 1.65 higher) | 1164 (7 RCTs) | ⨁⨁⨁◯ MODERATE f |
| BMD Femoral neck (g/cm2)—Children | MD 0.02 higher (0.01 higher to 0.04 higher) | 620 (5 RCTs) | ⨁⨁⨁◯ MODERATE f |
| BMD Femoral neck (g/cm2)—Adults | MD 0.01 lower (0.04 lower to 0.03 higher) | 150 (1 RCT) | ⨁⨁⨁◯ MODERATE g |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cormick, G.; Betran, A.P.; Romero, I.B.; Cormick, M.S.; Belizán, J.M.; Bardach, A.; Ciapponi, A. Effect of Calcium Fortified Foods on Health Outcomes: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 316. https://doi.org/10.3390/nu13020316
Cormick G, Betran AP, Romero IB, Cormick MS, Belizán JM, Bardach A, Ciapponi A. Effect of Calcium Fortified Foods on Health Outcomes: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(2):316. https://doi.org/10.3390/nu13020316
Chicago/Turabian StyleCormick, Gabriela, Ana Pilar Betran, Iris Beatriz Romero, Maria Sol Cormick, José M. Belizán, Ariel Bardach, and Agustín Ciapponi. 2021. "Effect of Calcium Fortified Foods on Health Outcomes: A Systematic Review and Meta-Analysis" Nutrients 13, no. 2: 316. https://doi.org/10.3390/nu13020316
APA StyleCormick, G., Betran, A. P., Romero, I. B., Cormick, M. S., Belizán, J. M., Bardach, A., & Ciapponi, A. (2021). Effect of Calcium Fortified Foods on Health Outcomes: A Systematic Review and Meta-Analysis. Nutrients, 13(2), 316. https://doi.org/10.3390/nu13020316