
Micronutrient Deficiencies in Patients with Decompensated Liver Cirrhosis

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sampling and Inclusion Criteria
2.3. Sample Size Calculation
2.4. Data Collection and Measurements
2.5. Definition of Deficiencies
2.6. Statistical Methods
2.7. Ethics
3. Results
3.1. Patient Characteristics
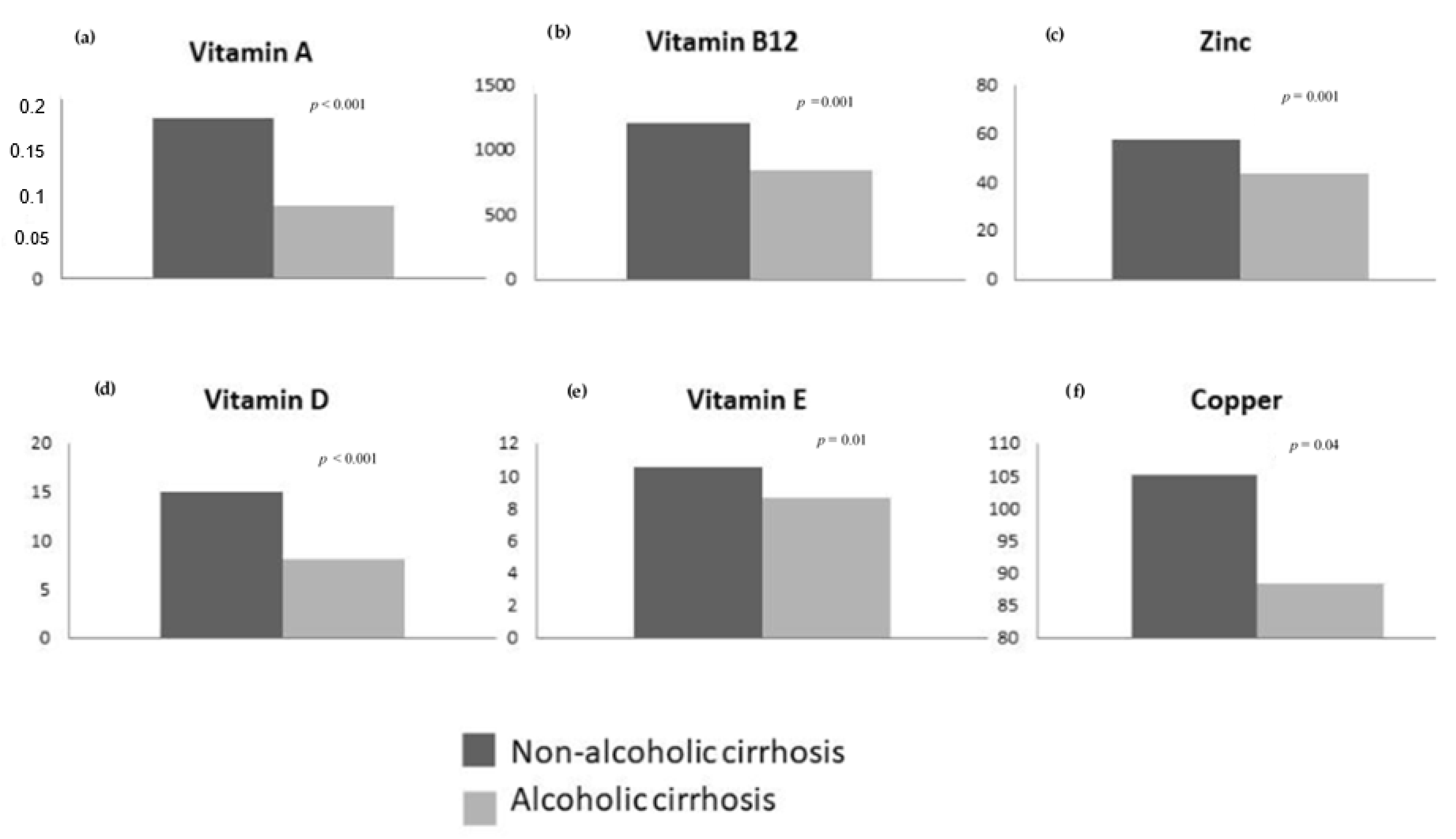
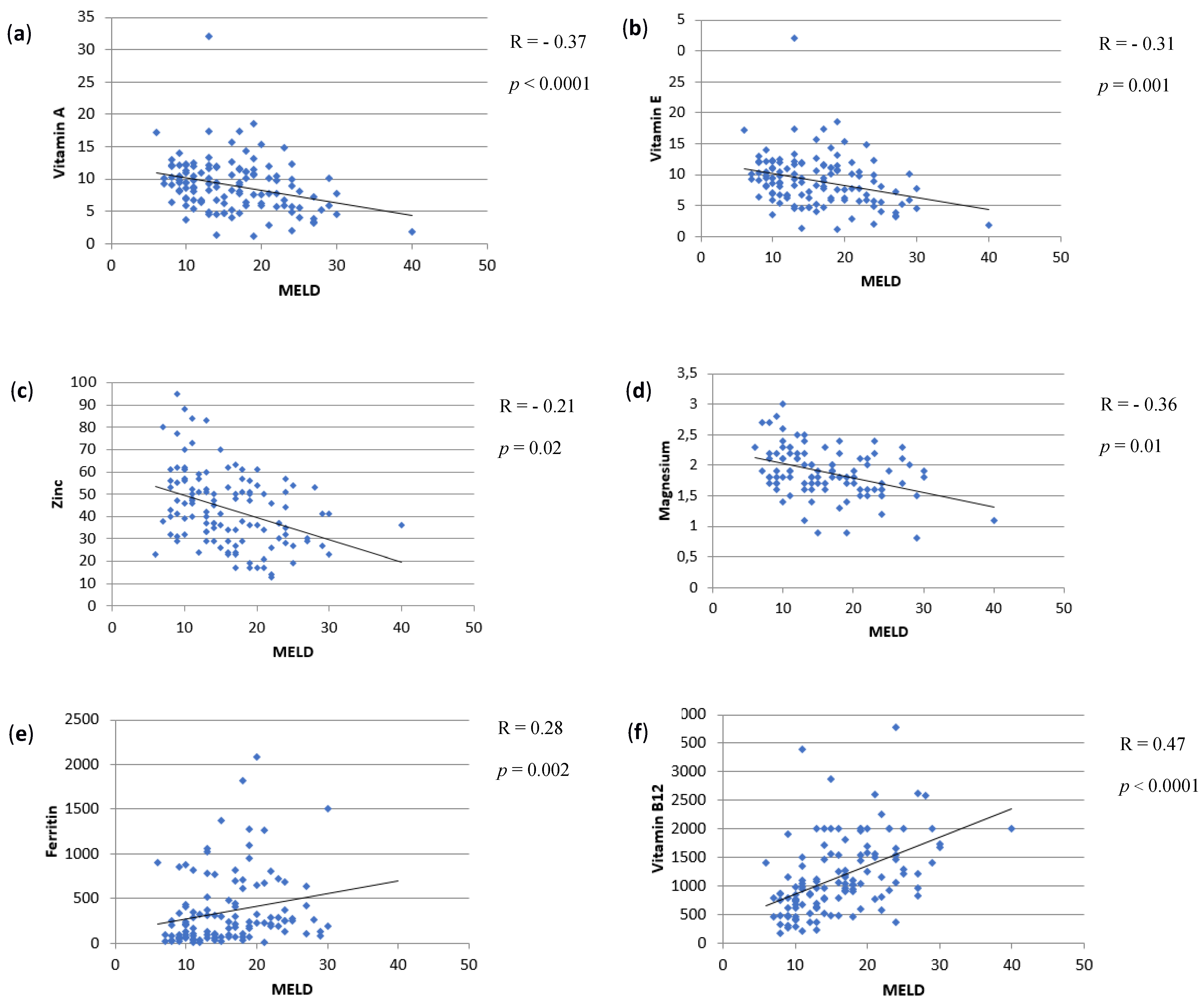
3.2. Micronutrient Deficiencies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kalaitzakis, E.; Simrén, M.; Olsson, R.; Henfridsson, P.; Hugosson, I.; Bengtsson, M.; Björnsson, E. Gastrointestinal symptoms in patients with liver cirrhosis: Associations with nutritional status and health-related quality of life. Clin. Gastroenterol. Hepatol. 2006, 10, 1464–1472. [Google Scholar] [CrossRef]
- Campillo, B.; Richardet, J.P.; Scherman, E.; Bories, P.N. Evaluation of nutritional practice in hospitalized cirrhotic patients: Results of a prospective study. Nutrition 2003, 19, 515–521. [Google Scholar] [CrossRef]
- Englesbe, M.J.; Patel, S.P.; He, K.; Lynch, R.J.; Schaubel, D.E.; Harbaugh, C.; Holcombe, S.A.; Wang, S.C.; Segev, D.L.; Sonnenday, C.J. Sarcopenia and mortality after liver transplantation. J. Am. Coll. Surg. 2010, 211, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, K.; Lee, S.S.; Raman, M. Prevalence and Mechanisms of Malnutrition in Patients with Advanced Liver Disease, and Nutrition Management Strategies. Clin. Gastroenterol. Hepatol. 2012, 10, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Venu, M.; Martin, E.; Saeian, K.; Gawrieh, S. High prevalence of vitamin A deficiency and vitamin D deficiency in patients evaluated for liver transplantation. Liver Transplant. 2013, 19, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Trautwein, C.; Possienke, M.; Schlitt, H.-J.; Boker, K.H.W.; Horn, R.; Raab, R.; Manns, M.P.; Brabant, G. Bone density and metabolism in patients with viral hepatitis and cholestatic liver diseases before and after liver transplantation. Am. J. Gastroenterol. 2000, 95, 2343–2351. [Google Scholar] [CrossRef] [PubMed]
- Stokes, C.S.; Volmer, D.A.; Grünhage, F.; Lammert, F. Vitamin D in chronic liver disease. Liver Int. 2013, 33, 338–352. [Google Scholar] [CrossRef] [PubMed]
- Finkelmeier, F.; Kronenberger, B.; Zeuzem, S.; Piiper, A.; Waidmann, O. Low 25-hydroxyvitamin D levels are associated with infections and mortality in patients with cirrhosis. PLoS ONE 2015, 10. [Google Scholar] [CrossRef]
- Putz-Bankuti, C.; Pilz, S.; Stojakovic, T.; Scharnagl, H.; Pieber, T.R.; Trauner, M.; Obermayer-Pietsch, B.; Stauber, R.E. Association of 25-hydroxyvitamin D levels with liver dysfunction and mortality in chronic liver disease. Liver Int. 2012, 32, 845–851. [Google Scholar] [CrossRef]
- Stokes, C.S.; Krawczyk, M.; Reichel, C.; Lammert, F.; Grünhage, F. Vitamin D deficiency is associated with mortality in patients with advanced liver cirrhosis. Eur. J. Clin. Investig. 2014, 44, 176–183. [Google Scholar] [CrossRef]
- Koop, A.H.; Mousa, O.Y.; Pham, L.E.; Corral-Hurtado, J.E.; Pungpapong, S.; Keaveny, A.P. An argument for vitamin D, A, and zinc monitoring in cirrhosis. Ann. Hepatol. 2018, 17, 920–932. [Google Scholar] [CrossRef]
- Harrison, S.A.; Torgerson, S.; Hayashi, P.; Ward, J.; Schenker, S. Vitamin E and Vitamin C Treatment Improves Fibrosis in Patients with Nonalcoholic Steatohepatitis. Am. J. Gastroenterol. 2003, 98, 2485–2490. [Google Scholar] [CrossRef]
- Bémeur, C.; Butterworth, R.F. Nutrition in the management of cirrhosis and its neurological complications. J. Clin. Exp. Hepatol. 2014, 4, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Gammoh, N.Z.; Rink, L. Zinc in infection and inflammation. Nutrients 2017, 9, 624. [Google Scholar] [CrossRef] [Green Version]
- Himoto, T.; Masaki, T. Associations between zinc deficiency and metabolic abnormalities in patients with chronic liver disease. Nutrients 2018, 10, 88. [Google Scholar] [CrossRef] [Green Version]
- Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [Green Version]
- Angeli, P.; Ginès, P.; Wong, F.; Bernardi, M.; Boyer, T.D.; Gerbes, A.; Moreau, R.; Jalan, R.; Sarin, S.K.; Piano, S.; et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: Revised consensus recommendations of the International Club of Ascites. Gut 2015, 64, 531–537. [Google Scholar] [CrossRef] [Green Version]
- Mangray, S.; Zweit, J.; Puri, P. Zinc Deficiency in Cirrhosis: Micronutrient for Thought? Dig. Dis. Sci. 2015, 60, 2868–2870. [Google Scholar] [CrossRef] [Green Version]
- McClain, C.; Vatsalya, V.; Cave, M. Role of Zinc in the Development/Progression of Alcoholic Liver Disease. Curr. Treat. Options Gastroenterol. 2017, 15, 285–295. [Google Scholar] [CrossRef]
- Tandon, P.; Raman, M.; Mourtzakis, M.; Merli, M. A practical approach to nutritional screening and assessment in cirrhosis. Hepatology 2017, 65, 1044–1057. [Google Scholar] [CrossRef] [Green Version]
- Teriaky, A.; Mosli, M.; Chandok, N.; Al-Judaibi, B.; Marotta, P.; Qumosani, K. Prevalence of fat-soluble vitamin (A, D, and E) and zinc deficiency in patients with cirrhosis being assessed for liver transplantation. Acta Gastroenterol. Belg. 2017, 80, 237–241. [Google Scholar]
- Pescovitz, M.D.; Mehta, P.L.; Jindal, R.M.; Milgrom, M.L.; Leapman, S.B.; Filo, R.S. Zinc deficiency and its repletion following liver transplantation in humans. Clin. Transplant. 1996, 10, 256–260. [Google Scholar]
- Sengupta, S.; Wroblewski, K.; Aronsohn, A.; Reau, N.; Reddy, K.G.; Jensen, D.; Te, H. Screening for Zinc Deficiency in Patients with Cirrhosis: When Should We Start? Dig. Dis. Sci. 2015, 60, 3130–3135. [Google Scholar] [CrossRef]
- Malham, M.; Jørgensen, S.P.; Ott, P.; Agnholt, J.; Vilstrup, H.; Borre, M.; Dahlerup, J.F. Vitamin D deficiency in cirrhosis relates to liver dysfunction rather than aetiology. World J. Gastroenterol. 2011, 17, 922–925. [Google Scholar] [CrossRef]
- Savić, Ž.; Vračarić, V.; Milić, N.; Nićiforović, D.; Damjanov, D.; Pellicano, R.; Medić-Stojanoska, M.; Abenavoli, L. Vitamin D supplementation in patients with alcoholic liver cirrhosis: A prospective study. Minerva Med. 2018, 109, 352–357. [Google Scholar] [CrossRef]
- Jamil, Z.; Arif, S.; Khan, A.; Durrani, A.A.; Yaqoob, N. Vitamin D Deficiency and Its Relationship with Child-Pugh Class in Patients with Chronic Liver Disease. J. Clin. Transl. Hepatol. 2018, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Rode, A.; Fourlanos, S.; Nicoll, A. Oral vitamin D replacement is effective in chronic liver disease. Gastroenterol. Clin. Biol. 2010, 34, 618–620. [Google Scholar] [CrossRef]
- Anty, R.; Tonohouan, M.; Ferrari-Panaia, P.; Piche, T.; Pariente, A.; Anstee, Q.M.; Gual, P.; Tran, A. Low levels of 25-hydroxy vitamin D are independently associated with the risk of bacterial infection in cirrhotic patients. Clin Transl. Gastroenterol. 2014, 5. [Google Scholar] [CrossRef]
- Buonomo, A.R.; Scotto, R.; Zappulo, E.; Nerilli, M.; Pinchera, B.; Perruolo, G.; Formisano, P.; Nappa, S.; Gentile, I. Severe Vitamin D deficiency increases mortality among patients with liver cirrhosis regardless of the presence of HCC. In Vivo 2019, 33, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Leo, M.A.; Lieber, C.S. Alcohol, vitamin A, and beta-carotene: Adverse interactions, including hepatotoxicity and carcinogenicity. Am. J. Clin. Nutr. 1999, 69, 1071–1085. [Google Scholar] [CrossRef] [Green Version]
- Sugihara, T.; Koda, M.; Okamoto, T.; Miyoshi, K.; Matono, T.; Oyama, K.; Hosho, K.; Okano, J.I.; Isomoto, H.; Murawaki, Y. Falsely Elevated Serum Vitamin B12 Levels Were Associated with the Severity and Prognosis of Chronic Viral Liver Disease. Yonago Acta Med. 2017, 60, 31–39. [Google Scholar]
- Halsted, C.H. B-vitamin dependent methionine metabolism and alcoholic liver disease. Clin. Chem. Lab. Med. 2013, 51, 457–465. [Google Scholar] [CrossRef]
- Levy, C.M.; Cardi, L.; Frank, O.; Gellene, R.; Baker, H. Incidence and significance of hypovitaminemia in a randomly selected municipal hospital population. Am. J. Clin. Nutr. 1965, 17, 259–271. [Google Scholar] [CrossRef]
- Cylwik, B.; Czygier, M.; Daniluk, M.; Chrostek, L.; Szmitowski, M. Vitamin B12 concentration in the blood of alcoholics. Pol. Merkur Lek. 2010, 28, 122–125. (In Polish) [Google Scholar]
- Kazimierska, E.; Czestochowska, E. Serum homocysteine, vitamin B12 and folic acid concentrations in patients with alcoholic liver cirrhosis. Pol. Merkur Lek. 2003, 15, 140–143. (In Polish) [Google Scholar]
- Oikonomou, T.; Goulis, I.; Soulaidopoulos, S.; Karasmani, A.; Doumtsis, P.; Tsioni, K. High serum ferritin is associated with worse outcome of patients with decompensated cirrhosis. Ann. Gastroenterol. 2017, 30, 217–224. [Google Scholar] [CrossRef]
- Maras, J.S.; Maiwall, R.; Harsha, H.C.; Das, S.; Hussain, M.S.; Kumar, C.; Bihari, C.; Rastogi, A.; Kumar, M.; Trehanpati, N.; et al. Dysregulated iron homeostasis is strongly associated with multiorgan failure and early mortality in acute-on-chronic liver failure. Hepatology 2015, 61, 1306–1320. [Google Scholar] [CrossRef] [PubMed]
- Walker, N.M.; Stuart, K.A.; Ryan, R.J.; Desai, S.; Saab, S.; Nicol, J.A.; Fletcher, L.M.; Crawford, D.H. Serum ferritin concentration predicts mortality in patients awaiting liver transplantation. Hepatology 2010, 51, 1683–1691. [Google Scholar] [CrossRef]
- Maiwall, R.; Kumar, S.; Chaudhary, A.K.; Maras, J.; Wani, Z.; Kumar, C.; Rastogi, A.; Bihari, C.; Vashisht, C.; Sarin, S.K. Serum ferritin predicts early mortality in patients with decompensated cirrhosis. J. Hepatol. 2014, 61, 43–50. [Google Scholar] [CrossRef]
- Liu, M.; Yang, H.; Mao, Y. Magnesium and liver disease. Ann. Transl. Med. 2019, 7, 578. [Google Scholar] [CrossRef]
- Nangliya, V.; Sharma, A.; Yadav, D.; Sunder, S.; Nijhawan, S.; Mishra, S. Study of Trace Elements in Liver Cirrhosis Patients and Their Role in Prognosis of Disease. Biol. Trace Elem. Res. 2015, 165, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Aigner, E.; Theurl, I.; Haufe, H.; Seifert, M.; Hohla, F.; Scharinger, L.; Stickel, F.; Mourlane, F.; Weiss, G.; Datz, C. Copper Availability Contributes to Iron Perturbations in Human Nonalcoholic Fatty Liver Disease. Gastroenterology 2008, 135, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Mehta, K.J.; Farnaud, S.J.; Sharp, P.A. Iron and liver fibrosis: Mechanistic and clinical aspects. World J. Gastroenterol. 2019, 25, 521–538. [Google Scholar] [CrossRef] [PubMed]
- Antonucci, L.; Porcu, C.; Iannucci, G.; Balsano, C.; Barbaro, B. Non-alcoholic fatty liver disease and nutritional implications: Special focus on copper. Nutrients 2017, 9, 1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakchbandi, I.A. Osteoporosis and fractures in liver disease: Relevance, pathogenesis and therapeutic implications. World J. Gastroenterol. 2014, 20, 9427–9438. [Google Scholar]
- Dirchwolf, M.; Ruf, A.E. Role of systemic inflammation in cirrhosis: From pathogenesis to prognosis. World J. Hepatol. 2015, 7, 1974–1981. [Google Scholar] [CrossRef]
- Namaste, S.M.; Aaron, G.J.; Varadhan, R.; Peerson, J.M.; Suchdev, S.; BRINDA Working Group. Methodologic approach for the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 333–347. [Google Scholar]
- Diana, A.; Haszard, J.J.; Purnamasari, D.M.; Nurulazmi, I.; Luftimas, D.E.; Rahmania, S.; Nugraha, G.I.; Erhardt, J.; Gibson, R.S.; Houghton, L. Iron, zinc, vitamin A and selenium status in a cohort of Indonesian infants after adjusting for inflammation using several different approaches. Br. J. Nutr. 2017, 118, 830–839. [Google Scholar] [CrossRef] [Green Version]
- Namaste, S.M.; Ou, J.; Williams, A.M.; Young, M.F.; Yu, E.X.; Suchdev, S. Adjusting iron and vitamin A status in settings of inflammation: A sensitivity analysis of the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) approach. Am. J. Clin. Nutr. 2019, 112, 458–467. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Age | 62.6 ± 10.3 |
| Sex Male Female | 96 (76.8%) 29 (23.2%) |
| Current smoker | 52 (41.6%) |
| Current alcohol consumption | 70 (57.4%) |
| Diabetes mellitus | 45 (36%) |
| Child-Pugh class A B C | 12 (9.6%) 70 (56%) 43 (34.4%) |
| MELD score | 16.2 ± 6.3 |
| Mid-arm muscle circumference <percentile 5 <percentile 10 ≥percentile 10 BMI categories Underweight (<18.5) Normal weight (18.5–24.9) Overweight (25–26.9) Obese (30–39.9) Extremely obese (>40) | 22 (17.6%) 8 (6.4%) 95 (76%) 2 (1.7%) 32 (27.1%) 47 (39.8%) 29 (24.6%) 8 (6.8%) |
| Etiology of cirrhosis Alcohol Hepatitis C Alcohol + hepatitis C Hepatitis B MAFLD Cryptogenic | 99 (79.2%) 5 (4%) 8 (6.4%) 2 (1.6%) 4 (3.2%) 7 (5.6%) |
| Decompensation of cirrhosis Ascites Encephalopathy Portal hypertensive bleeding Acute kidney injury Alcoholic hepatitis Infection SBP Respiratory infection Urinary infection Cutaneous infection Bacteremia Other | 100 (80%) 31 (24.8%) 19 (15.2%) 21 (16.8%) 18 (14.4%) 47 (37.6%) 8 (6.4%) 11 (8.8%) 11 (8.8%) 7 (5.2%) 5 (4%) 5 (4%) |
| Parameter | Value | Reference Value |
|---|---|---|
| Leucocytes | 6.86 (1.76–27.06) | 4–11 × 10 9/L |
| Hemoglobin | 105.7 ± 26.7 | 130–175 g/L |
| Platelets | 110 (21–466) | 130–400 × 10 9/L |
| INR | 1.47 ± 0.3 | 0.8–1.3 |
| Urea | 45.19 ± 31.7 | 10–50 mg/dL |
| Creatinine | 1.05 ± 0.56 | 0.70–1.20 mg/dL |
| Sodium | 136.8 ± 8.4 | 136–145 mEq/L |
| Bilirubin | 3.4 ± 1.7 | 0.1–1.3 mg/dL |
| Total protein | 62.07 ± 10.7 | 66–87 g/L |
| Albumin | 30.1 ± 5.7 | 34–48 g/L |
| Prealbumin | 8.5 ± 4.2 | 20–40 mg/dL |
| Total cholesterol HDL LDL | 114.3 ± 49.3 34.3 ± 18.2 64.1 ± 40.6 | 150–200 mg/dL 35–100 mg/dL |
| Triglycerides | 87.2 ± 47.2 | 50–200 mg/dL |
| Vitamin A | 0.09 (0.05–0.16) | 0.3–1 mg/L |
| Vitamin B1 | 3.9 (2.9–13.8) | 2–7.2 µg/dL |
| Vitamin B6 | 19 (9.05–33.5) | 23–173 nmol/L |
| Vitamin B12 | 982 (664–1542) | 150–695 pg/mL |
| Vitamin C | 0.4 (0.11–0.81) | 0.4–2 mg/dL |
| Vitamin D | 6.8 (5.2–49) | >30 ng/mL |
| Vitamin E | 8.8 (5.9–11.1) | 5–20 µg/mL |
| Vitamin K | 0.7 (0.2–3.1) | 0.13–1.50 µL/L |
| Folic acid | 5.4 (4–9.4) | 2–14.54 ng/mL |
| Corrected calcium for albumin | 9.3 ± 0.56 | 8.8–10.2 mg/dL |
| Phosphorus | 2.88 ± 0.82 | 2.7–4.5 mg/dL |
| Magnesium | 1.9 ± 0.41 | 1.6–2.6 mg/dL |
| Copper | 91.3 ± 32.1 | 70–140 µg/dL |
| Zinc | 45.9 ± 29.1 | 68–120 µg/dL |
| Iron | 81.4 ± 63.7 | 60–158 µg/dL |
| Ferritin | 211 (75.5–4362.7) | 30–400 ng/mL |
| Micronutrient (n) | Prevalence |
|---|---|
| Vitamins A (n = 123) B1 (n = 81) B6 (n = 120) B9 (folic acid) (n = 97) B12 (n = 123) C (n = 101) D (n = 109) E (n = 123) K (n = 97) | 115 (93.5%) 3 (3.7%) 73 (60.8%) 5 (5.2%) 0 (0%) 51 (50.5%) 103 (94.5%) 19 (15.4%) 3 (3.1%) |
| Trace elements Calcium (n = 87) Phosphorus (n = 125) Magnesium (n = 125) Copper (n = 125) Iron (n = 125) Ferritin (n = 125) Zinc (n = 125) | 4 (4.6%) 43 (34.4%) 16 (12.8%) 21 (16.8%) 48 (38.4%) 6 (5.2%) 107 (85.6%) |
| Child-Pugh A | Child-Pugh B | Child-Pugh C | p-value | |
|---|---|---|---|---|
| Vitamin A | 0.24 (0.09–0.59) | 0.09 (0.01–0.55) | 0.05 (0.02–0.22) | <0.0001 |
| Vitamin B1 | 4.2 (3.4–4.8) | 3.9 (1.2–8.7) | 3.1 (1.2–13.8) | 0.5 |
| Vitamin B6 | 27.4 (11.3–106) | 22.1 (9–97.8) | 12.35 (9–46) | 0.21 |
| Folic acid (B9) | 6.2 (4–14.40) | 5.4 (1.3–20) | 5.3 (1.5–23.30) | 0.5 |
| Vitamin B12 | 416.5 (164–1919) | 872.5 (269–2868) | 1459 (186–3771) | <0.0001 |
| Vitamin C | 0.6 (0.1–1.41) | 0.41 (0.1–2.69) | 0.24 (0.1–9) | 0.82 |
| Vitamin D | 9.8 (5.5–22.9) | 6.6 (5–26.9) | 6.6 (5–49) | 0.25 |
| Vitamin E | 10.6 (4.7–17.4) | 9.4 (1.2–32) | 6.5 (1.3–14.3) | 0.01 |
| Vitamin K | 1.14 (0.18–4.03) | 0.83 (0.09–4.31) | 0.52 (0.05–1.90) | 0.07 |
| Calcium | 9.2 (8–9.8) | 9,4 (8.29–10.8) | 9.5 (8.17–10.6) | 0.26 |
| Phosphorus | 3.2 (2.3–4) | 2.75 (1–4,7) | 2.75 (1–3.5) | 0.27 |
| Magnesium | 2.1 (1.8–2.5) | 1.8 (0.9–2.7) | 1.75 (0.8–2.5) | 0.05 |
| Copper | 86 (67–126) | 96.5 (17–121) | 80.5 (40–155) | 0.44 |
| Zinc | 56 (51–84) | 45.5 (17–95) | 35 (13–57) | <0.0001 |
| Ferritin | 71 (12–774) | 208.5 (10–2083) | 260 (12–4262) | 0.002 |
| Iron | 32 (25–269) | 46.5 (11–205) | 80 (22–178) | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llibre-Nieto, G.; Lira, A.; Vergara, M.; Solé, C.; Casas, M.; Puig-Diví, V.; Solé, G.; Humanes, A.; Grau, L.; Barradas, J.M.; et al. Micronutrient Deficiencies in Patients with Decompensated Liver Cirrhosis. Nutrients 2021, 13, 1249. https://doi.org/10.3390/nu13041249
Llibre-Nieto G, Lira A, Vergara M, Solé C, Casas M, Puig-Diví V, Solé G, Humanes A, Grau L, Barradas JM, et al. Micronutrient Deficiencies in Patients with Decompensated Liver Cirrhosis. Nutrients. 2021; 13(4):1249. https://doi.org/10.3390/nu13041249
Chicago/Turabian StyleLlibre-Nieto, Gemma, Alba Lira, Mercedes Vergara, Cristina Solé, Meritxell Casas, Valentí Puig-Diví, Gemma Solé, Antonia Humanes, Laia Grau, Josep Maria Barradas, and et al. 2021. "Micronutrient Deficiencies in Patients with Decompensated Liver Cirrhosis" Nutrients 13, no. 4: 1249. https://doi.org/10.3390/nu13041249
APA StyleLlibre-Nieto, G., Lira, A., Vergara, M., Solé, C., Casas, M., Puig-Diví, V., Solé, G., Humanes, A., Grau, L., Barradas, J. M., Miquel, M., & Sánchez-Delgado, J. (2021). Micronutrient Deficiencies in Patients with Decompensated Liver Cirrhosis. Nutrients, 13(4), 1249. https://doi.org/10.3390/nu13041249