
Oral Hyaluronan Relieves Wrinkles and Improves Dry Skin: A 12-Week Double-Blinded, Placebo-Controlled Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Samples
2.2. Study Design and Ethical Aspects
2.3. Study Participants
- (1)
- Taiwanese male and female subjects aged 30–65 years;
- (2)
- Not currently taking any HA or any other health, nutritional, herbal supplement for skin;
- (3)
- Not currently under-going any medical treatment (including laser treatment, face-lift, or skin-peel);
- (4)
- Not using any topical application cream for skin treatment prescribed by doctors or dermatologists (commonly used facial cleanser, toner, and moisturizer were acceptable).
2.4. Study Schedule
2.5. Skin Hydration and Barrier Function
2.6. Skin Elasticity
2.7. Skin Structure
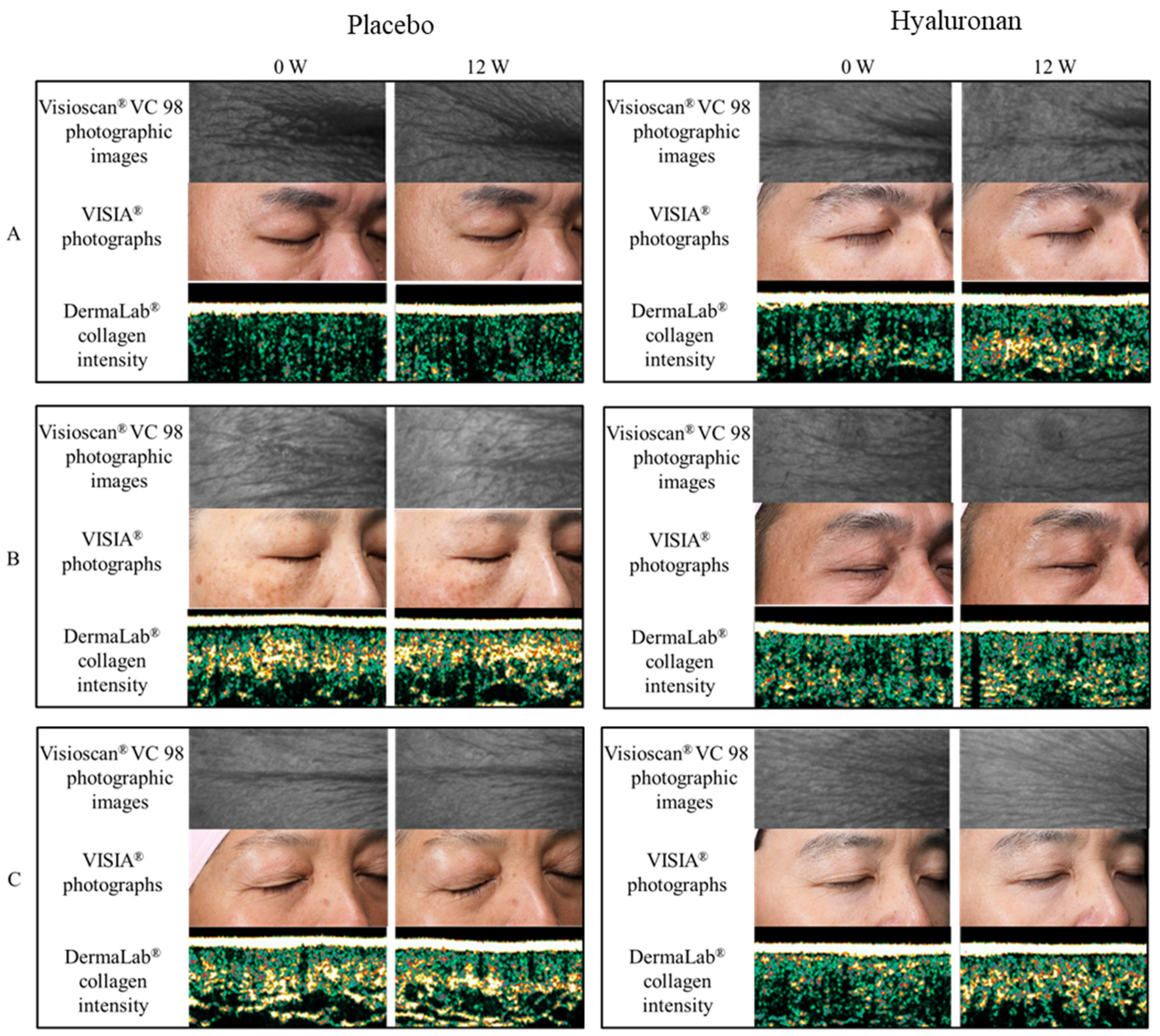
2.8. Facial Photography
2.9. Statistical Analysis
3. Results
3.1. Skin Hydration
3.2. Skin Elasticity
3.3. Skin Structure
3.4. Facial Photography
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laurent, T.C.; Fraser, J.R. Hyaluronan. FASEB J. 1992, 6, 2397–2404. [Google Scholar] [CrossRef]
- Fisher, G.J.; Wang, Z.Q.; Datta, S.C.; Varani, J.; Kang, S.; Voorhees, J.J. Pathophysiology of premature skin aging induced by ultraviolet light. N. Engl. J. Med. 1997, 337, 1419–1428. [Google Scholar] [CrossRef]
- Dai, G.; Freudenberger, T.; Zipper, P.; Melchior, A.; Grether-Beck, S.; Rabausch, B.; de Groot, J.; Twarock, S.; Hanenberg, H.; Homey, B.; et al. Chronic ultraviolet B irradiation causes loss of hyaluronic acid from mouse dermis because of down-regulation of hyaluronic acid synthases. Am. J. Pathol. 2007, 171, 1451–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longas, M.O.; Russell, C.S.; He, X.Y. Evidence for structural changes in dermatan sulfate and hyaluronic acid with aging. Carbohydr Res. 1987, 159, 127–136. [Google Scholar] [CrossRef]
- Haneke, E. Adverse effects of fillers and their histopathology. Facial Plast. Surg. 2014, 30, 599–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannarozzo, G.; Fazia, G.; Bennardo, L.; Tamburi, F.; Amoruso, G.F.; Del Duca, E.; Nisticò, S.P. A new 675 nm laser device in the treatment of facial aging: A prospective observational study. Photobiomodul. Photomed. Laser Surg. 2021, 39, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Nistico, S.P.; Silvestri, M.; Zingoni, T.; Tamburi, F.; Bennardo, L.; Cannarozzo, G. Combination of fractional CO2 laser and rhodamine-intense pulsed light in facial rejuvenation: A randomized controlled trial. Photobiomodul. Photomed. Laser Surg. 2021, 39, 113–117. [Google Scholar] [CrossRef]
- Draelos, Z.D. Facial skin care products and cosmetics. Clin. Dermatol. 2014, 32, 809–812. [Google Scholar] [CrossRef] [PubMed]
- Asserin, J.; Lati, E.; Shioya, T.; Prawitt, J. The effect of oral collagen peptide supplementation on skin moisture and the dermal collagen network: Evidence from an ex vivo model and randomized, placebo-controlled clinical trials. J. Cosmet. Dermatol. 2015, 14, 291–301. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.; Sung, J.; Lee, H.; Ono, T.; Yonei, Y. Effect of a dietary supplement containing porcine placenta extract on skin hydration-A placebo controlled, randomized, double blind, clinical study. Jpn. Pharmacol. Ther. 2018, 46, 1023–1034. [Google Scholar]
- Sugihara, F.; Inoue, N. Clinical effects of collagen hydrolysates ingestion on UV-induced pigmented spots of human skin: A preliminary study. Health Sci. 2012, 28, 153–156. [Google Scholar]
- Sato, T.; Yoshida, T.; Kanemitsu, T.; Yoshida, K.; Hasegawa, M.; Urushibata, O. Clinical effects of hyaluronic acid diet for moisture content of dry skin. Aesthetic Dermatol. 2007, 17, 33–39. (In Japanese) [Google Scholar]
- Oe, M.; Sakai, S.; Yoshida, H.; Okado, N.; Kaneda, H.; Masuda, Y.; Urushibata, O. Oral hyaluronan relieves wrinkles: A double-blinded, placebo-controlled study over a 12-week period. Clin. Cosmet. Investig. Dermatol. 2017, 10, 267–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. ICH Harmonised Guideline: Integrated Addendum to ICH E6 (R1): Guideline for Good Clinical Practice E6 (R2); European Medicines Agency: London, UK, 2016. [Google Scholar]
- Halprin, K.M. Epidermal “turnover time”—A re-examination. Br. J. Dermatol. 1972, 86, 14–19. [Google Scholar] [CrossRef]
- Greco, R.M.; Iocono, J.A.; Ehrlich, H.P. Hyaluronic acid stimulates human fibroblast proliferation within a collagen matrix. J. Cell. Physiol. 1998, 177, 465–473. [Google Scholar] [CrossRef]
- Lüke, H.J.; Prehm, P. Synthesis and shedding of hyaluronan from plasma membranes of human fibroblasts and metastatic and non-metastatic melanoma cells. Biochem. J. 1999, 343, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Rogiers, V.; Derde, M.; Verleye, G.; Roseeuw, D. Standardized conditions needed for skin surface hydration measurements. Cosmet. Toilet. 1990, 105, 73–82. [Google Scholar]
- Jacobi, U.; Gautier, J.; Sterry, W.; Lademann, J. Gender-related differences in the physiology of the stratum corneum. Dermatology 2005, 211, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, K.P.; Cua, A.B.; Maibach, H.I. Skin aging. Effect on transepidermal water loss, stratum corneum hydration, skin surface pH, and casual sebum content. Arch. Dermatol. 1991, 127, 1806–1809. [Google Scholar] [CrossRef] [PubMed]
- Close, T.; Ezure, E.; Yagi, N.; Kunizawa, T.; Hirao, S. Amano. comparison of sagging at the cheek and lower eyelid between male and female faces. Ski. Res. Technol. 2011, 17, 510–515. [Google Scholar]
- Ishikawa, T.; Ishikawa, O.; Miyachi, Y. Measurement of skin elastic properties with a new suction device (I): Relationship to age, sex and the degree of obesity in normal individuals. J. Dermatol. 1995, 22, 713–717. [Google Scholar] [CrossRef]
- Berardesca, E.; Pirot, F.; Singh, M. Differences in stratum corneum pH gradient when comparing white Caucasian and Black African American skin. Br. J. Dermatol. 1988, 139, 855–857. [Google Scholar] [CrossRef]
- Berardesca, E.; Maibach, H.I. Sodium lauryl sulphate induced cutaneous irritation: Comparison of White and Hispanic subjects. Contact Derm. 1988, 18, 136–140. [Google Scholar] [CrossRef]
- Berardesca, E.; Maibach, H.I. Racial differences in sodium lauryl sulphate induced cutaneous irritation: Black and white. Contact Derm. 1988, 18, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Manuskiatti, W.; Schwindt, D.A.; Maibach, H.I. Influence of age, anatomic site and race on skin roughness and scaliness. Dermatology 1998, 196, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Berardesca, E.; Rigal, J.; Leveque, J.L. In vivo biophysical characterization of skin physiological differences in races. Dermatologica 1991, 182, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Aramaki, J.; Kawana, S.; Effendy, I.; Happle, R.; Loffler, H. Differences of skin irritation between Japanese and European women. Br. J. Dermatol. 2002, 146, 1052–1056. [Google Scholar] [CrossRef]
- Meldrum, H.; Harding, C.R.; Rogers, J.S. The characteristic decrease in scalp stratum corneum lipids in dandruff is reversed by the use of a Zince Pyrithione containing shampoo. IFSCC Mag. 2003, 6, 3–6. [Google Scholar]
- Corcuff, P.; Lotte, C.; Rougier, A.; Maibach, H.I. Racial differences in corneocytes. Acta Derm. Venereol. 1991, 71, 146–148. [Google Scholar]
- Göllner, I.; Voss, W.; von Hehn, U.; Kammerer, S. Ingestion of an oral hyaluronan solution improves skin hydration, wrinkle reduction, elasticity, and skin roughness: Results of a clinical study. J. Evid. Based Complement. Altern. Med. 2017, 22, 816–823. [Google Scholar] [CrossRef]
- Kimura, M.; Maeshima, T.; Kubota, T.; Kurihara, H.; Masuda, Y.; Nomura, Y. Absorption of orally administered hyaluronan. J. Med. Food 2016, 19, 1172–1179. [Google Scholar] [CrossRef]
- Karlsson, F.H.; Nookaew, I.; Nielsen, J. Metagenomic data utilization and analysis (MEDUSA) and construction of a global gut microbial gene catalogue. PLoS Comput. Biol. 2014, 10, e1003706. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Kamochi, R.; Oiki, S.; Murata, K.; Hashimoto, W. Probiotics in human gut microbiota can degrade host glycosaminoglycans. Sci. Rep. 2018, 8, 10674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, T.; Kamaguchi, A.; Nakazawa, F. Purification and characterization of hemolysin from Prevotella oris. J. Oral. Biosci. 2012, 54, 11–118. [Google Scholar] [CrossRef] [Green Version]
- Tammi, R.; Ripellino, J.A.; Margolis, R.U.; Maibach, H.I.; Tammi, M. Localization of epidermal hyaluronic acid using the hyaluronate binding region of cartilage proteoglycan as a specific probe. J. Investig. Dermatol. 1988, 90, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Sakai, S.; Yasuda, R.; Sayo, T.; Ishikawa, O.; Inoue, S. Hyaluronan exists in the normal stratum corneum. J. Investig. Dermatol. 2000, 14, 1184–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourguignon, L.Y. Matrix hyaluronan-activated CD44 signaling promotes keratinocyte activities and improves abnormal epidermal functions. Am. J. Pathol. 2014, 184, 1912–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comper, W.D.; Laurent, T.C. Physiological function of connective tissue polysaccharides. Physiol. Rev. 1978, 58, 255–315. [Google Scholar] [CrossRef]


{kind=link}
| Placebo | HA | Total | ||||
|---|---|---|---|---|---|---|
| Males | Females | Males | Females | Males | Females | |
| Number | 5 | 15 | 6 | 14 | 11 | 29 |
| Age (years) mean ± SD | 44.2 ± 3.6 | 44.3 ± 6.5 | 40.5 ± 4.0 | 43.5 ± 6.8 | 43.0 ± 4.1 | 44.5 ± 6.6 |
| Number | 20 | 20 | 40 | |||
| Evaluation Parameter | Group | Measurement Sites | Week 0 | Week 4 | Week 8 | Week 12 |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Corneometer | HA | Face | 49.5 ± 8.53 | 51.5 ± 6.55 | 52.8 ± 7.18 ** | 54.9 ± 7.06 ***† |
| (AU) 1 | Placebo | Face | 49.1 ± 8.13 | 49.4 ± 8.79 | 48.9 ± 9.36 | 48.8 ± 8.99 |
| HA | Arm | 33.9 ± 8.41 | 36.8 ± 6.90 | 36.1 ± 6.38 | 38.6 ± 7.99 ** | |
| Placebo | Arm | 35.4 ± 4.91 | 36.4 ± 5.78 | 35.1 ± 4.99 | 35.6 ± 4.38 | |
| HA | Waist | 29.7 ± 7.85 | 31.9 ± 7.60 | 30.4 ± 7.20 | 32.5 ± 7.14 * | |
| Placebo | Waist | 29.7 ± 5.26 | 31.0 ± 6.57 | 29.9 ± 6.38 | 30.2 ± 5.87 | |
| Tewameter | HA | Face | 12.8 ± 2.39 | 12.1 ± 1.85 | 12.0 ± 2.65 | 10.8 ± 2.49 ***†† |
| (g/h/m2) 2 | Placebo | Face | 12.6 ± 3.23 | 12.9 ± 2.67 | 13.0 ± 3.45 | 13.3 ± 3.09 |
| HA | Arm | 5.79 ± 1.86 | 5.45 ± 1.89 | 5.39 ± 2.10 | 5.40 ± 2.07 | |
| Placebo | Arm | 5.89 ± 2.43 | 5.94 ±3.06 | 5.31 ± 2.10 | 5.57 ± 1.90 | |
| HA | Waist | 3.47 ± 2.18 | 4.27 ± 1.53 | 3.60 ± 1.88 | 4.30 ± 1.88 | |
| Placebo | Waist | 3.74 ± 2.03 | 3.41 ± 1.32 | 3.72 ± 2.68 | 3.83 ± 1.91 |
| Group | Measurement Sites | Evaluation Parameter | Week 0 | Week 4 | Week 8 | Week 12 |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| HA | Forehead | R0 | 0.09 ± 0.04 | 0.09 ± 0.04 | 0.10 ± 0.05 | 0.11 ± 0.05 **† |
| Placebo | 0.08 ± 0.03 | 0.08 ± 0.03 | 0.08 ± 0.02 | 0.08 ± 0.02 | ||
| HA | Forehead | R1 | 0.04 ± 0.02 | 0.04 ± 0.02 | 0.04 ± 0.01 | 0.04 ± 0.02 |
| Placebo | 0.04 ± 0.02 | 0.04 ± 0.01 | 0.04 ± 0.02 | 0.04 ± 0.01 | ||
| HA | Forehead | R2 | 0.62 ± 0.17 | 0.54 ± 0.14 * | 0.52 ± 0.18 ** | 0.59 ± 0.11 |
| Placebo | 0.61 ± 0.14 | 0.59 ± 0.17 | 0.55 ± 0.14 | 0.56 ± 0.15 | ||
| HA | Forehead | R7 | 0.44 ± 0.09 | 0.39 ± 0.09 | 0.37 ± 0.07 * | 0.41 ± 0.12 |
| Placebo | 0.43 ± 0.11 | 0.44 ± 0.16 | 0.42 ± 0.14 | 0.42 ± 0.11 | ||
| HA | Arm | R0 | 0.24 ± 0.04 | 0.24 ± 0.04 | 0.25 ± 0.05 | 0.26 ± 0.04 *† |
| Placebo | 0.23 ± 0.05 | 0.23 ± 0.06 | 0.23 ± 0.05 | 0.22 ± 0.04 | ||
| HA | Arm | R1 | 0.03 ± 0.01 | 0.03 ± 0.01 | 0.03 ± 0.01 | 0.03 ± 0.01 |
| Placebo | 0.04 ± 0.01 | 0.03 ± 0.01 | 0.03 ± 0.01 | 0.04 ± 0.01 | ||
| HA | Arm | R2 | 0.85 ± 0.05 | 0.86 ± 0.04 | 0.86 ± 0.04 | 0.88 ± 0.05 |
| Placebo | 0.84 ± 0.05 | 0.87 ± 0.05 | 0.86 ± 0.04 | 0.85 ± 0.05 | ||
| HA | Arm | R7 | 0.73±0.09 | 0.70 ± 0.05 | 0.72 ± 0.08 | 0.78 ± 0.06 |
| Placebo | 0.74 ± 0.07 | 0.72 ± 0.08 | 0.71 ± 0.08 | 0.75 ± 0.09 | ||
| HA | Waist | R0 | 0.32 ± 0.06 | 0.33 ± 0.07 | 0.34 ± 0.06 | 0.38 ± 0.08 ***†† |
| Placebo | 0.33 ± 0.05 | 0.31 ± 0.05 ** | 0.32 ± 0.05 | 0.32 ± 0.05 | ||
| HA | Waist | R1 | 0.04 ± 0.01 | 0.04 ± 0.01 | 0.03 ± 0.01 *** | 0.04 ± 0.01 |
| Placebo | 0.04 ± 0.01 | 0.04 ± 0.01 | 0.04 ± 0.01 | 0.04 ± 0.02 | ||
| HA | Waist | R2 | 0.87 ± 0.03 | 0.88 ± 0.04 | 0.90 ± 0.04 ** | 0.89 ± 0.04 * |
| Placebo | 0.87 ± 0.03 | 0.88 ± 0.03 | 0.89 ± 0.03 | 0.88 ± 0.04 | ||
| HA | Waist | R7 | 0.77 ± 0.05 | 0.73 ± 0.07 | 0.74 ± 0.06 | 0.78 ± 0.08 |
| Placebo | 0.79 ± 0.05 | 0.75 ± 0.06 | 0.73 ± 0.07 * | 0.77 ± 0.08 |
| Group | Week 0 | Week 4 | Week 8 | Week 12 |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| HA | 269 ± 9.64 | 267 ± 9.85 | 269 ± 9.33 | 269 ± 11.6 |
| Placebo | 269 ± 12.19 | 269 ± 12.5 | 270 ± 11.7 | 269 ± 11.1 |
| Group | Measurement Sites | Evaluation Parameter | Week 0 | Week 4 | Week 8 | Week 12 |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| HA | Temple | Thickness | 1152 ± 195 | 1151 ± 205 | 1177 ± 204 | 1207 ± 217 * |
| Placebo | Temple | Thickness | 1152 ± 229 | 1152 ± 225 | 1151 ± 210 | 1150 ± 212 |
| HA | Waist | Thickness | 1537 ± 302 | 1544 ± 280 | 1566 ± 313 | 1614 ± 303 ** |
| Placebo | Waist | Thickness | 1513 ± 259 | 1501 ± 254 | 1509 ± 275 | 1517 ± 257 |
| HA | Temple | Intensity | 46.6 ± 9.96 | 47.9 ± 11.9 | 49.6 ± 13.6 | 52.0 ± 12.3 ** |
| Placebo | Temple | Intensity | 47.8 ± 11.9 | 47.0 ± 10.8 | 47.3 ± 11.4 | 48.7 ± 11.4 |
| HA | Waist | Intensity | 38.4 ± 13.4 | 37.6 ± 13.0 | 38.8 ± 13.8 | 41.8 ± 13.5 ** |
| Placebo | Waist | Intensity | 37.8 ± 12.8 | 39.8 ± 12.8 | 38.1 ± 12.6 | 39.3 ± 12.7 |
| Group | Evaluation Parameter | Week 0 | Week 4 | Week 8 | Week 12 |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| HA | Surface | 408 ± 54.0 | 429 ± 54.0 | 423 ± 58.5 | 432 ± 47.8 |
| Placebo | 422 ± 38.0 | 430 ± 43.4 | 421 ± 44.2 | 427 ± 45.2 | |
| HA | Volume | 69.2 ± 22.7 | 64.7 ± 26.5 | 59.6 ± 20.2 | 52.1 ± 9.29 **† |
| Placebo | 60.5 ± 19.0 | 61.1 ± 15.7 | 58.7 ± 13.2 | 59.8 ± 14.1 | |
| HA | SEw | 115 ± 23.1 | 110 ± 26.6 | 103 ± 33.9 | 97.8 ± 31.0 ** |
| Placebo | 115 ± 36.9 | 116 ± 34.7 | 113 ± 30.8 | 116 ± 28.7 | |
| HA | SEsc | 0.52 ± 0.13 | 0.49 ± 0.12 | 0.45 ± 0.09 | 0.43 ± 0.11 ** |
| Placebo | 0.47 ± 0.13 | 0.45 ± 0.13 | 0.44 ± 0.07 | 0.42 ± 0.11 | |
| HA | SEsm | 255 ± 48.9 | 254 ± 45.5 | 266 ± 48.2 | 287 ± 43.4 *† |
| Placebo | 252 ± 62.4 | 241 ± 64.5 | 252 ± 59.6 | 245 ± 60.7 | |
| HA | SEr | 3.63 ± 1.42 | 3.59 ± 1.43 | 3.51 ± 1.56 | 3.25 ± 1.39 |
| Placebo | 3.65 ± 1.44 | 3.62 ± 1.43 | 3.56 ± 1.40 | 3.66 ± 1.29 | |
| HA | NRJ | 0.03 ± 0.007 | 0.03 ± 0.008 | 0.03 ± 0.008 | 0.03 ± 0.007 |
| Placebo | 0.02 ± 0.005 | 0.02 ± 0.004 | 0.03 ± 0.005 | 0.03 ± 0.003 | |
| HA | ENT | 1.52 ± 0.04 | 1.52 ± 0.04 | 1.52 ± 0.04 | 1.52 ± 0.04 |
| Placebo | 1.51 ± 0.03 | 1.51 ± 0.02 | 1.51 ± 0.03 | 1.51 ± 0.02 | |
| HA | HOM | 1.40 ± 0.06 | 1.40 ± 0.08 | 1.42 ± 0.07 | 1.42 ± 0.08 |
| Placebo | 1.39 ± 0.05 | 1.40 ± 0.05 | 1.40 ± 0.05 | 1.40 ± 0.05 | |
| HA | CONT | 1.03 ± 0.28 | 1.00 ± 0.32 | 0.99 ± 0.30 | 0.95 ± 0.32 * |
| Placebo | 0.99 ± 0.24 | 0.90 ± 0.13 | 0.90 ± 0.20 * | 0.95 ± 0.17 | |
| HA | VAR | 3.83 ± 0.79 | 3.75 ± 0.80 | 3.59 ± 0.73 | 3.34 ± 0.63 **† |
| Placebo | 3.74 ± 0.47 | 3.67 ± 0.49 | 3.48 ± 0.51 * | 3.70 ± 0.46 |
| Group | Evaluation Parameter | Week 0 | Week 4 | Week 8 | Week 12 |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| HA | Wrinkle | 192 ± 38.0 | 187 ± 38.8 | 188 ± 38.7 | 184 ± 39.2 ** |
| Placebo | Wrinkle | 197 ± 42.6 | 202 ± 41.2 | 206 ± 37.4 | 204 ± 41.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, T.-F.; Su, Z.-R.; Hsieh, Y.-H.; Wang, M.-F.; Oe, M.; Matsuoka, R.; Masuda, Y. Oral Hyaluronan Relieves Wrinkles and Improves Dry Skin: A 12-Week Double-Blinded, Placebo-Controlled Study. Nutrients 2021, 13, 2220. https://doi.org/10.3390/nu13072220
Hsu T-F, Su Z-R, Hsieh Y-H, Wang M-F, Oe M, Matsuoka R, Masuda Y. Oral Hyaluronan Relieves Wrinkles and Improves Dry Skin: A 12-Week Double-Blinded, Placebo-Controlled Study. Nutrients. 2021; 13(7):2220. https://doi.org/10.3390/nu13072220
Chicago/Turabian StyleHsu, Tzu-Fang, Zi-Rong Su, Yao-Hao Hsieh, Ming-Fu Wang, Mariko Oe, Ryosuke Matsuoka, and Yasunobu Masuda. 2021. "Oral Hyaluronan Relieves Wrinkles and Improves Dry Skin: A 12-Week Double-Blinded, Placebo-Controlled Study" Nutrients 13, no. 7: 2220. https://doi.org/10.3390/nu13072220
APA StyleHsu, T.-F., Su, Z.-R., Hsieh, Y.-H., Wang, M.-F., Oe, M., Matsuoka, R., & Masuda, Y. (2021). Oral Hyaluronan Relieves Wrinkles and Improves Dry Skin: A 12-Week Double-Blinded, Placebo-Controlled Study. Nutrients, 13(7), 2220. https://doi.org/10.3390/nu13072220