1. Introduction
Special needs schools (SNS) for children and young people with major neurological disabilities (ND) and cerebral palsy (CP) have as a main objective the promotion to the highest degree of students’ personal autonomy and social integration by developing their physical, affective, cognitive, communicative, moral, civic, and social insertion abilities. Multidisciplinary teams at SNS in Catalonia (Spain) are composed of educational staff including special education teachers, social educators, SLP teachers and physiotherapists. L’Arboç SNS also has a social worker, a nurse, a neurologist, and a psychologist. SNS educate children with major associated health problems (musculoskeletal disorders, intellectual disability, epilepsy, swallowing disorders, and malnutrition (MN)). In early childhood and adolescence, these populations are more likely to suffer from poor nutrition than during adulthood because of the high nutritional demands needed for growth and development. Providing adequate nutrition and hydration to these students is essential to promote their maximal level of both physical and cognitive development [
1]. Oropharyngeal dysphagia (OD) is an extremely common digestive disorder amongst children with ND and CP, with a reported prevalence in excess of 90% [
2,
3]. The main complications of OD include respiratory infections, aspiration pneumonia, MN, and dehydration (DH) [
4,
5]. Respiratory diseases are the leading cause of death in patients with severe intellectual disability and severe developmental disability [
6,
7,
8].
Feeding and swallowing difficulties in children with ND and CP severely affect nutrient intake, which leads to MN, DH, alterations in linear growth, and micronutrient deficiency [
2,
3,
4,
5]. Poor nutritional status may detrimentally impact health and physical and cognitive development [
5,
6,
7,
8]. CP describes a group of permanent disorders of movement and posture development attributed to nonprogressive disturbances that occurred in the developing fetal or infant brain [
3]. CP can be caused by injury to the brain at birth, during the early stages of development in the womb, or during the first two years of life. Head injuries, infections such as meningitis, and other forms of brain damage occurring in the first months or years of life are the main causes of acquired CP [
1]. Up to four types of CP have been described, determined by timing, site, type, and extent of the brain lesion: (a) spastic, the most common form (70–80%) affecting motor cortex, (b) dyskinetic arising from the basal ganglia and affecting less than 10% of cases, (c) ataxic arising from cerebellum damage, also affecting less than 10% of cases, and (d) mixed types with a combination of damage [
1]. The prevalence of CP in Europe is 2.08 per 1000 live births [
9], and CP is considered a relatively rare disorder there [
1]. Primary neurological impairments might influence not only physical and mental capacities but also neural pathways leading to dysphagia, vomiting, swallowing deficits, gastroesophageal reflux, aspiration, and constipation [
10,
11,
12,
13,
14].
Motor disorders in CP are often accompanied by alterations in sensation, cognition, and communication, as well as by secondary musculoskeletal problems [
15], and they are classified by the GMFCS into five subgroups according to their severity [
16]. The severity of GMFCS also correlates with the severity of swallowing difficulties [
17,
18]. The most severe complication of swallowing disorders is respiratory infection, which occurs when food, liquid, or oropharyngeal secretions, together with microorganisms, are aspirated into the respiratory tract [
19,
20]. OH is closely related to OD because the oropharynx is a constant source and reservoir of microorganisms responsible for respiratory infections in patients with OD [
19,
20]. In general, young people and children with ND present greater oral pathology with poorer OH and gingival health and a higher incidence of dental caries than children without ND [
21]. The severity of neurological impairment correlates with increased risk of developing dental disease [
22]. For these reasons, it is recommended that children with ND are assessed for OD to avoid safety impairments, and they should receive early and regular dental care, in order to minimize the reservoir of oral pathogens [
21].
Regarding MN, studies have shown high prevalence among children and young people with ND compared to the general population [
23,
24]. MN has been observed in 46% and 90% of children with CP [
25,
26] and, in the most severe types, the prevalence increases due to the severity of cognitive and motor impairments, OD, and alterations in orolingual facial motricity leading to eating difficulties [
13,
14,
26,
27,
28,
29]. Higher rates of MN are reported among children with bilateral spasticity, dyskinesia, and spastic quadriplegia [
23,
26,
30,
31]. Poor nutritional status is associated with growth impairment, increased spasticity, and irritability [
14,
30], in addition to further risk of adverse cognitive and health outcomes including respiratory complications and mortality. The etiology of MN in children with neurological impairment is multifactorial, and one of the major contributors is OD and subsequent insufficient caloric and nutrient intake [
32,
33]. When nutritional intake is insufficient to cover nutritional requirements or the oral route is not safe, children need enteral nutrition through percutaneous endoscopic gastrostomy (PEG) to feed. The prevalence of children with CP with a gastrostomy tube is 11% in European countries [
34].
Nutritional assessment and support are an essential part of the care of people with ND and CP who have extremely complex and challenging needs [
24]. Adequate nutritional support may restore linear growth, normalize weight, decrease irritability and spasticity, improve wound healing, reduce the frequency of hospitalization, and increase social participation, thus improving overall health and quality of life [
35]. Early screening and management through nutritional and compensatory strategies of OD and MN in SNS can be an effective strategy to improve physical and intellectual development, clinical outcomes, and quality of life for their students [
36,
37,
38].
L’Arboç is an SNS for children and young people with multiple and major ND, located in the city of Mataró, Catalonia, Spain. The school takes care of 50 students, from 3 to 23 years of age, with CP, severe ND, and psychomotor disabilities that interfere with their development and learning processes [
39]. Awareness and management of OD, MN, and OH in SNS in Spain is scarce and must be improved. As most students have severe neurological impairments, we hypothesized that most of them would have dysfunctional swallowing. We believe the introduction of a program mainly based on the management of OD and MN in children attending these schools and the education of their caregivers in the same will improve students’ hydration and nutritional status, reduce complications associated with OD (respiratory infections and hospital readmissions), and improve the knowledge of parents, caregivers, and professionals at these schools on the management of these relevant conditions.
The aim of this study was to assess the prevalence of swallowing and feeding disorders and oral health impairments in students at L’Arboç SNS and their relation to students’ nutritional and hydration status. This is the first step of a program that includes (a) a transversal descriptive study that will be repeated at the end of each school year, assessing OD, nutritional status, and oral health, (b) the implementation of a nutritional intervention including adaptations in texture, caloric and protein content, and palatability during meals at school and at home, (c) a hydration program including regular services, fluid-thickening agents, and special cups at school and home, and (d) an educational program on the clinical relevance and management of OD and MN in these children for parents, caregivers, and all professionals at L’Arboç school (
Supplementary Material S1).
4. Discussion
The main results of this study showed that children from L’Arboç SNS presented the following characteristics: all of them had swallowing disorders, 90.6% with impaired safety of swallow; 96.9% had eating and drinking disabilities according to EDACS (68.7 with II-III and 31.3% with IV–V); 83.9% had poor or fair OH; 89.3% and 21.4% had chronic and acute MN, respectively; 70% had dehydration. In addition, they had a wide age range and several types and severity levels of comorbidities, polymedication, and physical and intellectual disabilities. They were frail and their clinical outcomes were poor with high rates of emergency room (ER) visits and hospitalizations. Their educational and social outcomes were also poor, with a high level of absenteeism.
The Arboç school students had severe neurological conditions and a very high level of physical impairment according to GMFCS (63.6% level IV–V). Spastic CP was the most frequent neurological condition, and epilepsy and chronic gastrointestinal impairments were the most common comorbidities [
82]. These high levels of health frailty lead to frequent hospital and ER admissions, as well as multiple visits to medical specialists, with respiratory infections being the main cause of ER admissions. Our students were polymedicated, with a high percentage of consumption of benzodiazepines, antiepileptics, and other muscle relaxants. Although the purpose of the school is educational, the care needs of the students require adapting the day-to-day life of school attendance to circumstances such as high absenteeism, which makes school health monitoring even more complex
(Supplementary Material S5).
Regarding swallowing function, we found that OD was extremely prevalent and highly severe in our SNS students according to the oral-motor, EDACS, and swallowing assessments. All study participants had OD with a high prevalence of impaired safety of swallow. Similar results were obtained by Calis in a study of 166 children with neurological impairment (NI), where the prevalence of OD was 99% [
3,
32]. The proportion of students fed by gastrostomy in our study (31.3%, 25% exclusively and 6.3% mixed) was greater than that obtained by other authors. Caramico et al. noted 17.5% (12.5% exclusively and 5% mixed) after assessing 40 children with CP [
83], and Dahlseng described gastrostomies at 11% [
34]. However, when Dahlseng stratified the CP patients according to GMFCS (Level IV–V), the prevalence was 32%, which coincides with the numbers in our study. All these data further confirm the close correlation between GMFCS and OD, which is also well defined in the literature [
84].
Disruption of the oral phase leads to alterations in both the efficacy and the safety of swallowing. High rates of oral phase impairments (66.7% tongue protrusion, 54.2% incomplete lip seal, and 45.8% accumulation of residue in the mouth) were observed in Arboç students, which can lead to feeding difficulties and MN. Other authors described chewing impairment (21%), motor speech articulation (36%), and oral-motor delays (44–47%) [
84]. Cervical hyperextension was described in 41.7% of Arboç students, and Furkim found this characteristic in more than 50% of individuals with CP [
85]. This last condition, together with an ineffective velopharyngeal seal, can lead to aspiration because it favors premature spillage of the bolus into the pharynx while the pharynx is still in a respiratory configuration. Up to 90.6% (29) of the study sample had signs of impaired safety of swallow and aspiration, which have been associated with poor long-term prognosis [
86,
87]. Benfer noted that the most common signs on direct assessment were cough (44.7%), multiple swallows (25.2%), gurgly voice (20.3%), wet breathing (18.7%), and gagging (11.4%). Furkim also found suggestive signs of aspiration during clinical evaluation, especially with liquids [
85]. It should be noted that OD is frequently a neglected condition, and many of these students are not diagnosed in SNS where there may be low awareness of OD. Compensatory strategies to ameliorate these findings, such as increasing bolus viscosity, have been proven to be a valid strategy in several phenotypes of dysphagic patients [
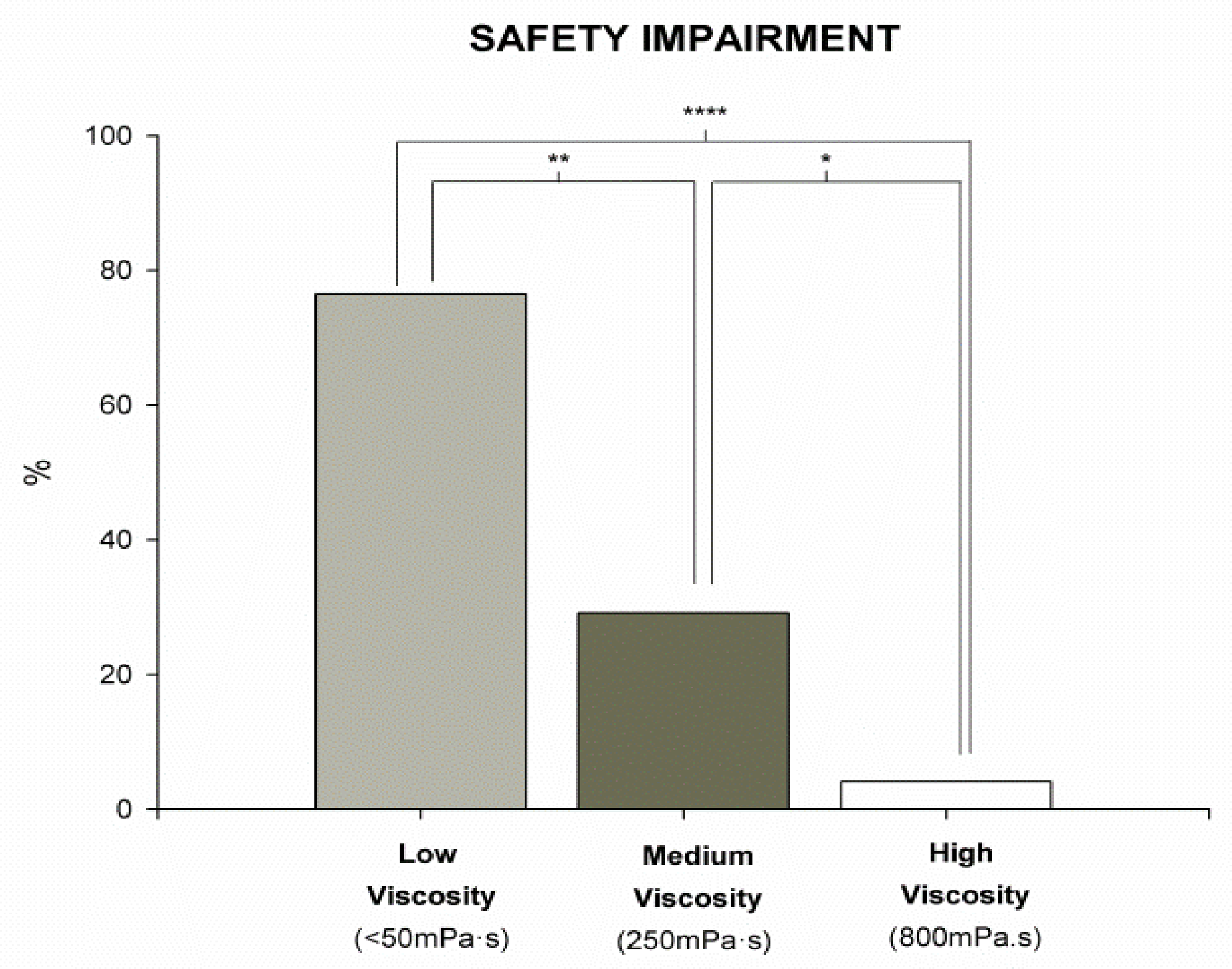
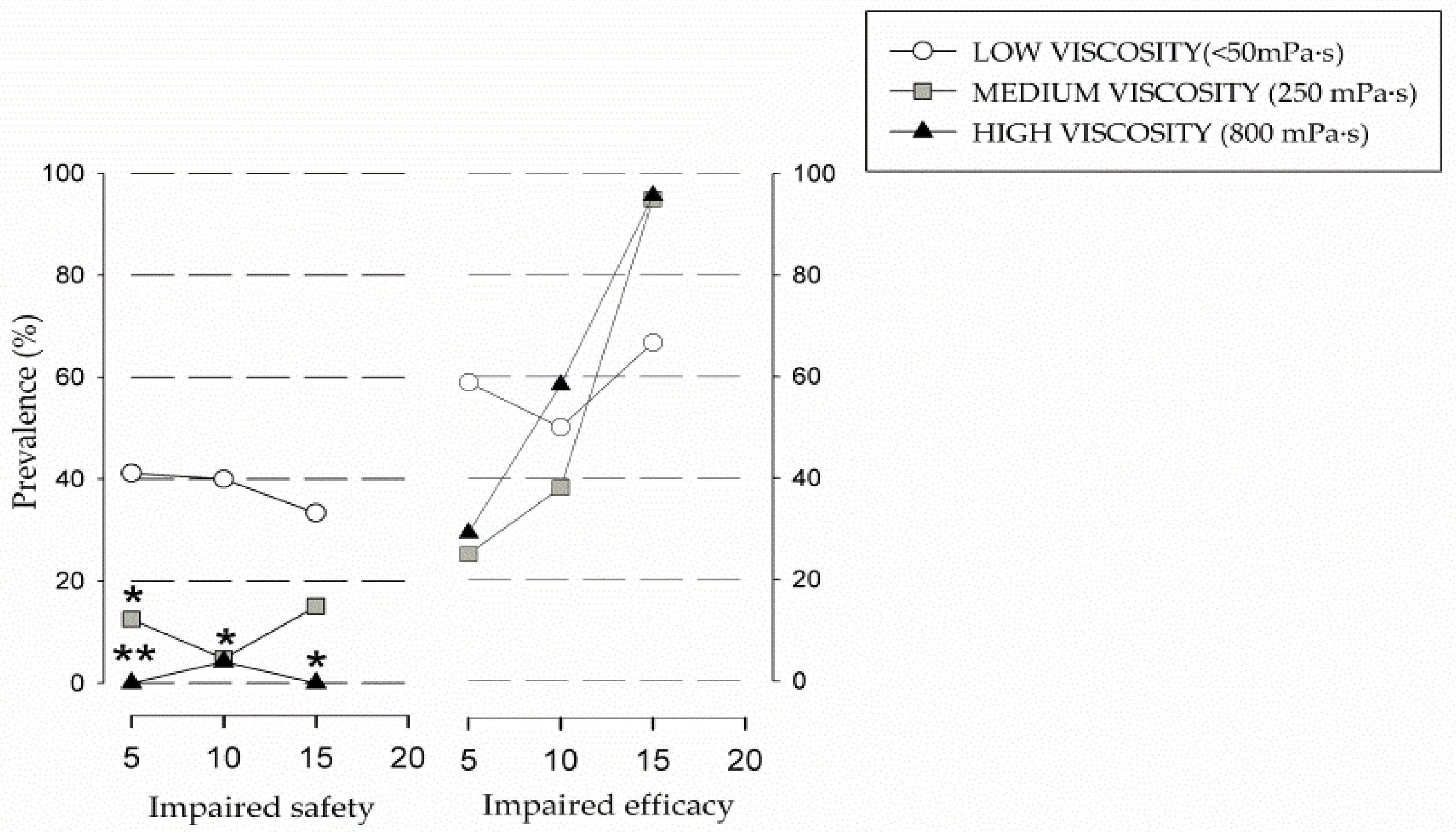
88]. Our results showed that the safest viscosity was the highest (800 mPa·s) and the least safe was liquid (<50 mPa·s). These results are in line with our previous studies which showed the strong therapeutic effect of increasing viscosity up to level of 800 mPa·s [
48]. A similar effect was also described in neurodegenerative diseases and stroke patients [
89]. We also observed that our students presented a high prevalence of efficacy impairment, particularly oral residue (95.8%) and pharyngeal residue (83.3%), which directly correlated with an increment in volume and viscosity. In this specific study, 250 mPa·s and 10 mL were selected as the most effective viscosity and volume for thickened fluids.
One of the main risk factors for the development of respiratory complications in patients with OD is poor oral health and colonization by respiratory pathogens [
20]. In our study, we found similar results to those found by other authors and confirm the low awareness of this condition in this specific phenotype. We observed that 51.6% of students showed malocclusion, 83.9% had gingivitis, and 22.6% had periodontitis. Orellana and collaborators, in a study on CP, reported a higher prevalence of dental malocclusion (84%) and similar results regarding gingivitis and periodontal disease (67% and 14%, respectively) [
90]. Up to 83.9% of our students needed to improve their OH, with 64.5% of them being in fair status and 19.4% in poor status. Orellana also described poor OH since the total of the study group presented more than 60% plaque and 50% calculus on all tooth surfaces. In its 2020 annual report, the Spanish Association of Dentists reported a prevalence of 40.8% in healthy young people (12–15 years) with a healthy periodontium [
91]. Students’ caregivers, usually parents, reported that the main problem was rejection of toothbrushing, which often made it impossible for them to perform the technique correctly, a justification of the situation. It is well known that two of the main complications of OD are respiratory infections and aspiration pneumonia [
92]. We previously found that frail older patients with OD had poor OH, high oral bacterial load, and prevalence of oral colonization by respiratory pathogens, and they presented high risk for respiratory infections [
50,
93]. During the previous year, one-third of Arboç students had a respiratory infection, and three of them were hospitalized with pneumonia. We previously found that OD, poor oral health, and colonization by respiratory pathogens and MN are risk factors associated with respiratory infections, including aspiration pneumonia [
4,
94]. On the other hand, we previously proved that interventions with the aim of treating these main risk factors (dysphagia with fluid adaptation, malnutrition and vulnerability with texture adaptation and nutritional supplementation, and impaired oral health and hygiene to reduce the bacterial load of the oral cavity) are effective in reducing the incidence of respiratory infections and improving nutritional and clinical outcomes in older patients with OD [
51]. Therefore, we aim to apply these strategies in L’Arboç students in future studies.
Nutritional status is also a key factor for the development of complications, and it is associated with OD. Poor nutrition and growth impairments are common findings in children with CP. Studies showed that these individuals are shorter and thinner than similarly aged healthy children [
33,
95,
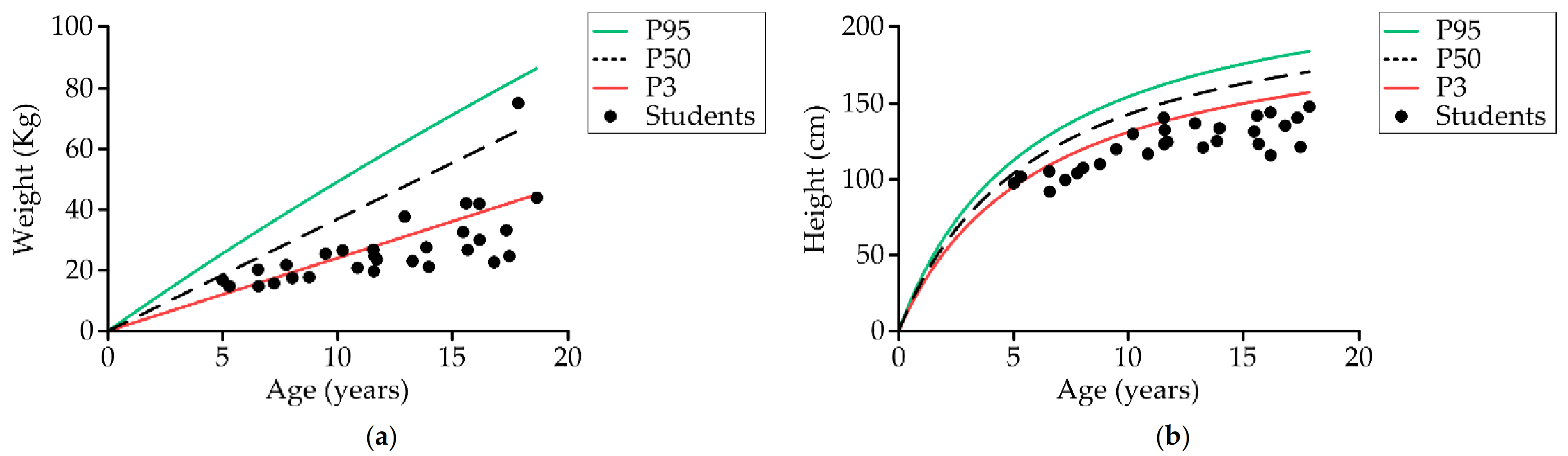
96], and that they have difficulties in growing. This was fully confirmed in our study where, regarding weight, 96.6% of study participants were below the 50th percentile and 69% were below the third percentile; regarding height, 89.7% were below the third percentile, while none of our students were above the 50th percentile. Main factors causing low weight and height in this group are nutritional but also brain damage and the type, distribution, and severity of the motor impairment, as one Spanish study found significantly lower body weight in the group with the highest GMFCS [
32]. CP-specific growth charts describe substandard growth as they include many children with other health conditions that affect growth, particularly malnutrition. ESPGHAN does not recommend using these charts as they do not measure how this group of children should ideally grow [
32]. Our main results were obtained by comparison with standard growth charts validated by ESPGHAN [
32]. Studies have also reported that the intake of energy and nutrients in this group is considerably lower than the recommended daily allowances [
26,
97]. Caramico et al. found that patients with CP and OD received lower daily energy [
83]. However, another study based on preschool children with CP found that energy requirements in ambulant children were similar to healthy children [
13]. Other studies conducted in Norway found that the presence of orofacial dysfunction was associated with reduced daily energy intake [
98]. Difficulty biting (70%), cleaning behaviors (70%), and chewing (65%) were the most common deficiencies in processing solid foods in CP [
99]. In our study, we found high prevalence of impaired chewing and swallowing in students (66.7% tongue protrusion, 54.2% incomplete lip seal, 45.8% accumulation of bolus in the mouth, and 100% of students with efficacy impairments of swallow, the main cause of insufficient nutrient intake). Moreover, the texturization that these children received before the study was suboptimal, which made it even more difficult to meet their caloric and nutritional requirements.
Differences in energy expenditure also play an important role in children with CP. Growth failure in these children also depends on non-nutrition-related factors such as the severity and type of neurological impairment, mobility, and cognitive function [
100]. Increased muscle tone, level of physical activity, and the presence of involuntary movements may also contribute to increased daily energy expenditure in CP [
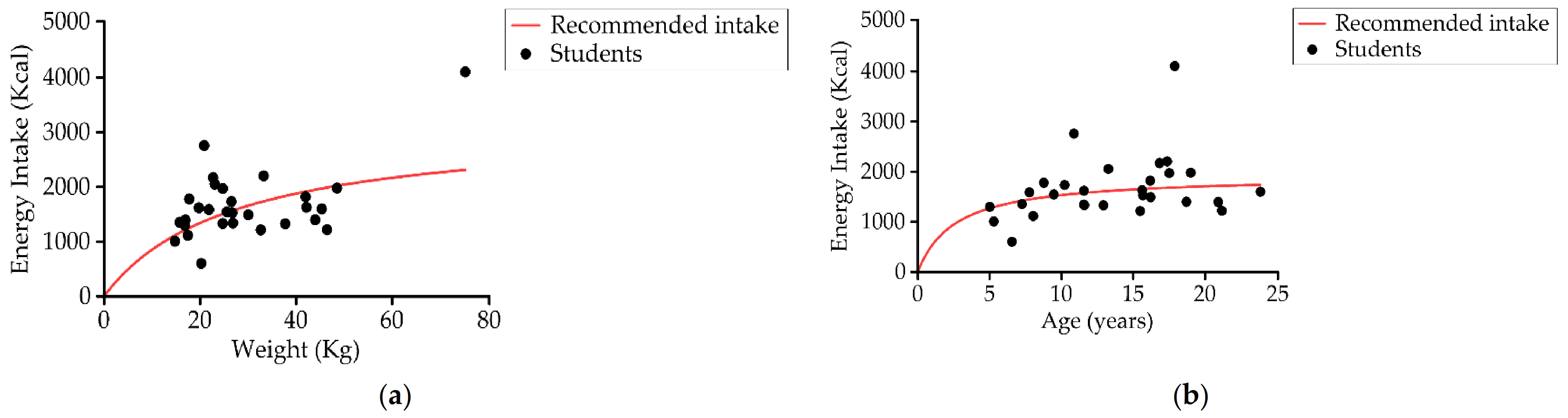
101]. However, several studies have confirmed that the main cause of growth failure and malnutrition in children with neurological dysfunction is insufficient caloric and protein intake [
102,
103,
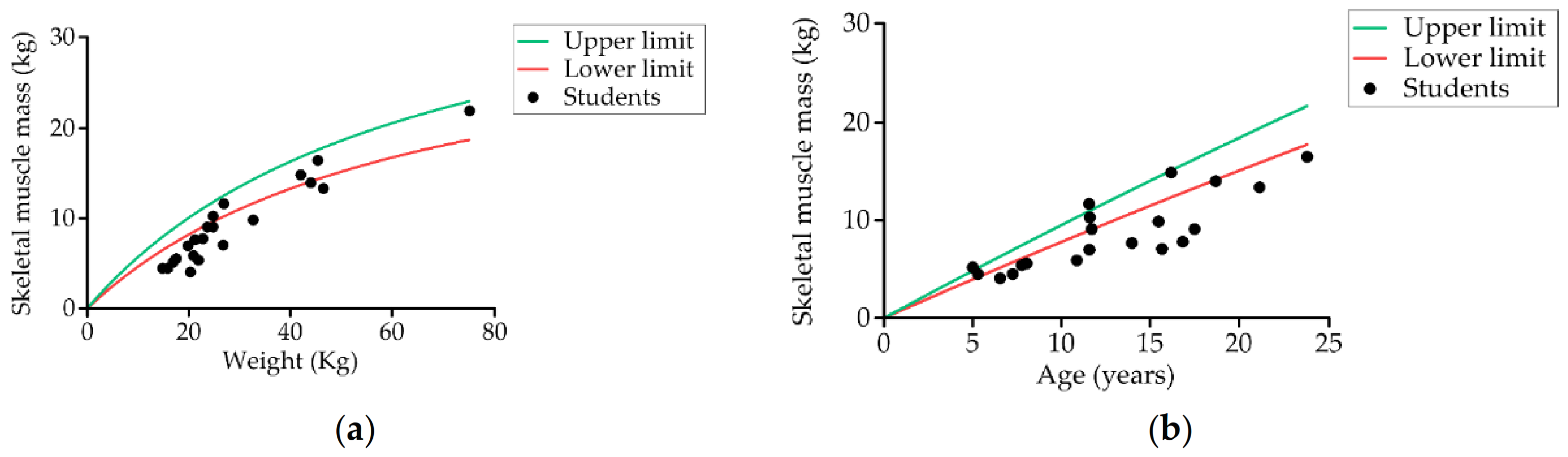
104]. In our scenario, around 50% of students presented an insufficient energy intake according to recommendations for weight and age. As expected, the students at our school had low fat-free mass, low skeletal muscle mass, and low cell mass, results that are consistent with most studies [
96,
104]. However, some students at Arboç had excess fat mass, both in quantity and percentage. This finding is consistent with Romano [
105], who noted that children with marked NI had high fat mass compared with reference children of similar age and sex. Metabolic principles describe that, if nutrient intake is insufficient to meet the needs, resulting in malnutrition, body fat and muscle will be catabolized to provide energy [
106]; thus, it could be expected that fat would also be low in our students. Increased risk of body fat accumulation may be associated with insufficient physical activity in children with NI and with the high consumption of sugar observed in the intake records, which are associated with increased risk for obesity [
107]. Another important finding of our study is the low body cell mass value, which is considered an important indicator of nutritional status in this group and inversely related to the degree of GMFCS [
108].
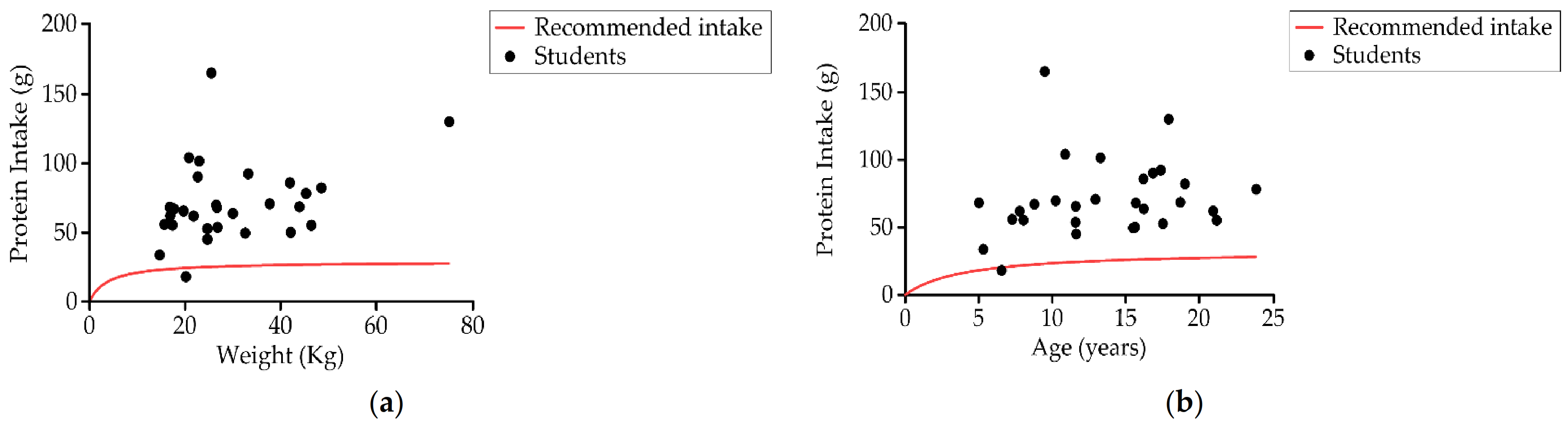
The energy distribution from the daily intake of macronutrients we found in our study (47.5% carbohydrate, 34.6% fat, and 17.4% protein) was similar to that found in another study [
109]. In general, students ate excessive amounts of protein and insufficient complex carbohydrates. Protein intake was very high (≥2.5 times the RDA), especially in the younger group (5–12 years), which also agrees with other authors [
83,
97]. Excess of protein intake could be due to the belief of families and caregivers that protein intake alone can improve muscle mass, but evidence shows that it is necessary to combine nutrition with exercise to maintain muscle function [
110]. Protein requirements of the students differ depending on whether they are established on the basis of the current weight of the children [
79] or the general recommendations for healthy children (30–54 g/day) [
76]. Neither result is compatible with the protein requirements in healthy patients with an optimal weight according to age. Most of them have insufficient current weight, and these optimal amounts are excessive for them. Therefore, it is important to be careful and avoid daily protein excess. The same occurs with energy intake, calculated from the current weight of the students (Group 1: 1460.2 ± 484.4 kcal and Group 2: 1854.6 ± 703.3 kcal), whereby they establish needs that are underestimated in relation to what they theoretically need by age (1700–3000 kcal) [
79]. Taking this into account, we observed that the intake of Group 1 coincided with that estimated according to weight, but not with that estimated by age. Group 2, however, exceeded the caloric intake according to weight, but would not cover the needs according to age. In order to improve the food offered in the school canteen, our group established guidelines on calorie and protein recommendations for the two school groups. Regarding carbohydrates (CH), the students met the recommended minimum of 130 g/day; however, they did not meet the percentage of the total recommended daily caloric intake (50%), which does not favor muscle synthesis or weight gain of the students. Caramico et al. also noted that patients with OD received lower amounts of CH (median: 170.9 g vs. 234.5 g,
p = 0.023). One possible reason for the low intake of complex CH could be the difficulty in providing complex CH in blended diets for people with OD and CP [
83]. On the other hand, consumption of free sugar exceeded the recommended 5% of the total daily caloric intake in both groups [
74] (15% in Group 1 and 22.6% in Group 2), which could lead to an increased presence of caries [
111] and possible alterations in body composition, thereby increasing body fat deposits, as we observed in our results.
We also observed an imbalance in the lipid profile of the diet, with a low contribution of unsaturated vs. saturated fats, resulting from the high consumption of meat and processed meat. Poor intake of fiber (16.2 vs. 25–30 g/day) was observed in both age groups of our students, as also found by some authors [
112,
113]. Low dietary fiber intake combined with low fluid intake may also contribute to the development of constipation. In general, both groups presented a low intake of most minerals and water-soluble and fat-soluble vitamins, possibly due to an unbalanced diet. The nutritional results correlate with the qualitative evaluation of the diet: a low intake of fiber and folic acid possibly explained by the insufficient intake of fruits, vegetables, legumes, and nuts, as well as an insufficient intake of calcium and vitamin D, both with an important role in bone formation/growth, due to an insufficient intake of dairy products, legumes, and nuts. The high consumption of meat products allows them to cover their iron and vitamin B12 requirements; however, it does not cover the recommended intake of zinc due to the low consumption of seafood, legumes, whole grains, and nuts. This qualitative and quantitative relationship indicates that, beyond digestive problems that may reduce nutrient absorption or drug–food interactions, a balanced diet can help improve nutritional intakes in these SNS students. The students had inappropriate dietary patterns. The Mediterranean food pattern is characterized by grains and vegetable bases with meat or similar as a “garnish” and type of fat (olive oil, fish, and nuts), rich in micronutrients provided by seasonal vegetables, herbs, and spices [
114]. The students’ diet was highly unbalanced, due to the low content of vegetables and excessive content of meat and sweetened products. Low intake of fruits and vegetables (sources of dietary fiber) was previously seen in another study developed in children with CP [
115]. Furthermore, low consumption of fish and no consumption of nuts was also observed. To conclude, the three main objectives for intake improvement are (1) to increase caloric intake by increasing the consumption of complex carbohydrates, (2) to improve the lipid profile of the diet, increasing the consumption of monounsaturated and polyunsaturated fats, and promoting the consumption of vegetable versus animal protein, and (3) to ensure the requirements of micronutrients by consuming fresh, whole-grain, and vegetable products.
Nutritional evaluation, according to WHO Growth Standards [
116], also showed that stunting (chronic MN) was the most common form of MN (89.3%) in our students, followed by underweight (overall MN, 55.5%) and thinness (acute MN, 21.4%). We can highlight two important aspects of our results. First, the prevalence of MN in the older group was higher than in the younger (87.4 vs 80%,
p = 0.002); second, the prevalence and severity of chronic MN were higher in our study than observed by other authors [
23,
117,
118,
119,
120]. Two possible reasons can justify this higher severity: the higher age and high degree of disability of our study group population. Previous studies suggested that prevalence of MN in CP increases with age. Karim et al. found a prevalence of MN of 29% in children aged 5.6 years, and Almunet et al. determined a prevalence of 50% for MN [
117] in children aged 7 years [
14,
23]. The fact that our study group population included students between the ages of 4 and 23 may have been one of the reasons for our higher prevalence of MN. The second reason could have been the higher degree of disability in our study group population. It is known that a greater degree of disability results in a worse nutritional status [
121]. In our study, 63.6% of students had GMFCS IV–V, and 75% of the stunted group population was severe, whereas Jahan found this degree of disability in less than 50% and severe stunting in 52.4% [
23]. The prevalence of acute MN we found in our study coincides with that found by Bell et al. (23%) (6 years,
n = 89) [
118]. Furthermore, the prevalence of overweight and obesity we found (21.4%) is in complete agreement with that found by Martinez de Zabarte [
122]. Another tool we used to measure MN was the Waterlow Index, a method widely used in clinical practice, obtaining prevalence values similar to those obtained using the
z-score: 17.8% vs. 21.4% in acute MN and 96.4 vs 89.3% in chronic MN. We, therefore, consider the WI a good tool for classifying MN in SNS. In addition, all the above information was obtained by comparing with standard growth charts validated by ESPGHAN for children with CP [
32]. However, it should be noted that their growth patterns are often notably different from healthy children. Nevertheless, CP-specific growth charts describe growth which is not necessarily ideal, as they also consider many children with health issues affecting growth, especially MN; for this reason, they are not recommended by ESPGHAN [
32].
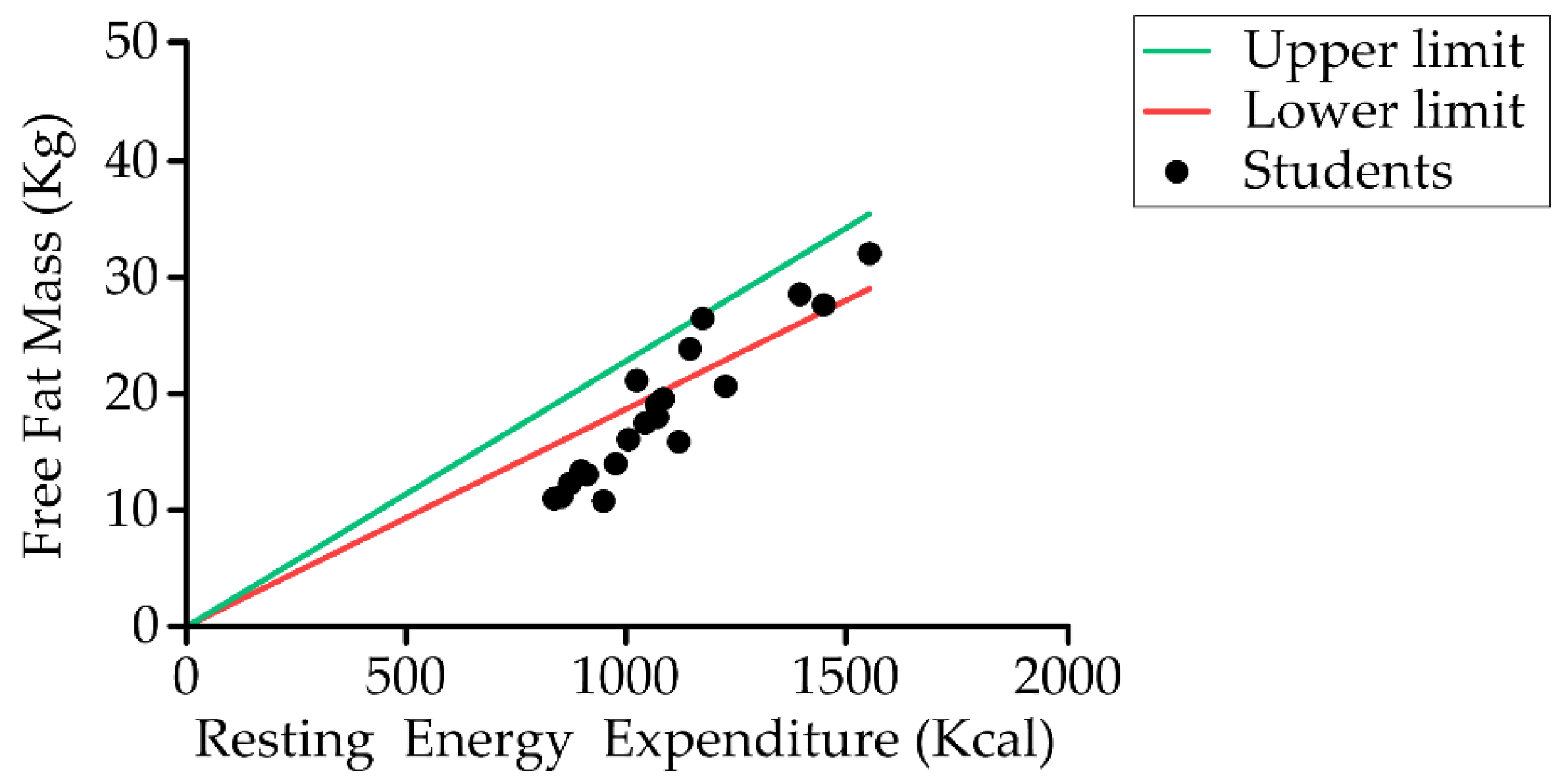
Estimation of energy requirements in children with CP is the first step toward a personalized nutritional intervention. In our study, resting energy expenditure (REE) of students was similar to data reported by Bell et al. in children with bilateral spastic CP aged 5–12 years who found a resting energy expenditure of 1074 ± 168 kcal/day and total energy expenditure of 1674 ± kcal/day [
118]. Other authors reported lower resting energy expenditure (between 760 and 876 kcal/day) [
123] and total energy expenditure of 1367 ± 329.17 kcal [
95], both in younger populations. Several publications have suggested that children with bilateral spastic CP have the highest resting energy expenditure and total energy expenditure (due to the hypertonicity of the muscles), whereas children with spastic quadriplegic CP have the lowest [
26,
95,
123,
124,
125,
126,
127]. Studies of Walker and Rieken showed a decline in the total energy expenditure with increasing GMFCS level [
95,
128]. Similar results were observed when considering the number of limbs involved [
95]. A trend toward lower energy requirements was observed when the number of limbs involved increased. Further research is needed in order to determine the influence of motor type on energy requirements. Moreover, other factors which influence energy requirements that need to be taken into account are level of physical activity, altered body composition, and MN [
105]. For future studies, we could include the assessment of muscle tone (described by the Ashworth Scale) in assessing the nutritional status of children with CP to better adjust for the energy needs of children [
129].
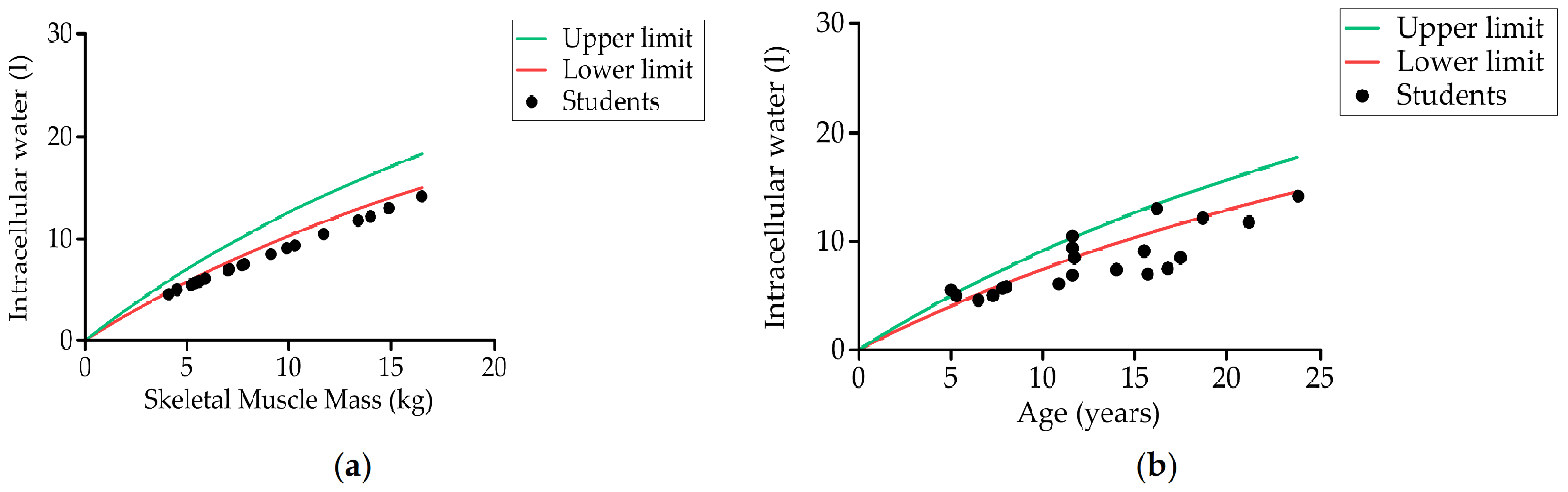
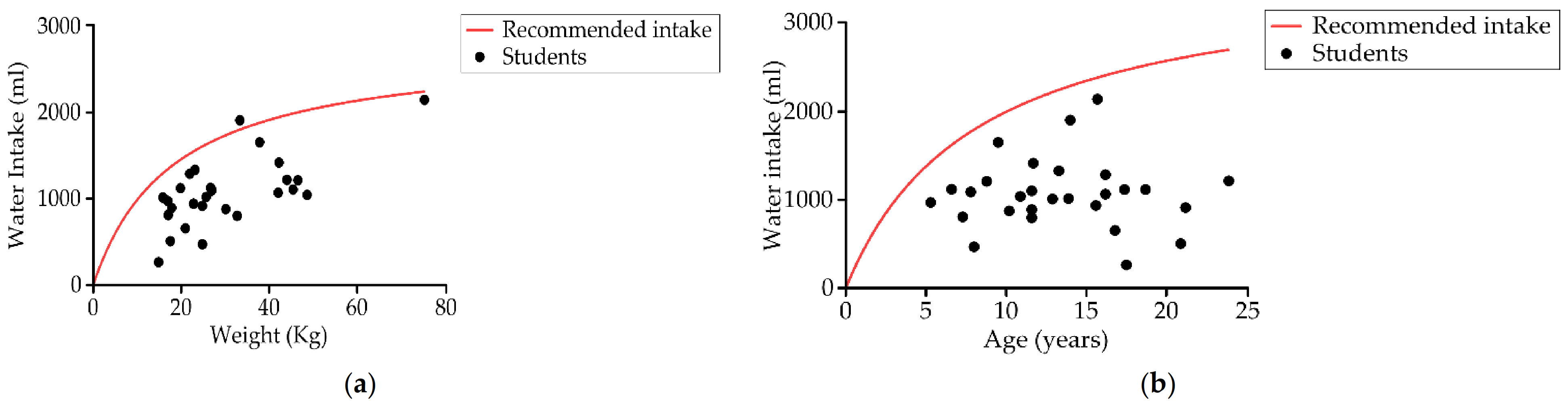
Lastly, we found a high percentage of dehydration among Arboç school students. The high prevalence of OD in our study led up to 96.4% of our students to consume below the daily basal recommendations of fluids, causing dehydration in the intracellular compartment water in 70% (14). Other studies have also reported that people with NI are at a higher risk for dehydration [
130,
131]. Deficiency of body water due to OD and low intake causes dehydration, which might also contribute to impaired cognitive function [
132,
133]. Dehydration in children and young people is associated with reduced cognitive response, while correct hydration has a positive effect on cognitive function [
133]. In our study, the prevalence of dehydration was very high (70%) and mainly hypertonic. The swallowing disorders of these individuals caused low water intake, which was also associated with the difficulties encountered by caregivers to ensure safe intake. Studies also found a relationship between the state of hydropenia and oral-motor impairment of individuals [
134], as well as greater dehydration in subjects with ND compared to a typical development child [
130,
131].
Regarding bolus viscosity descriptors, we did not use the IDDSI descriptors. Firstly, for texture-modified foods, we used the levels proposed by the British Dietetic Association (BDA) descriptors [
45]: (a) thick purée (C) and (b) fork-mashable (E), due to the fact that this classification of texture modified foods is well implemented in our institution and easy to implement in the school. Secondly, for thickened fluids, we expressed the viscosity in SI units (mPa·s) as recommended in a recent paper endorsed by 11 scientific societies [
135].
Our study presents many limitations. The main one was the relatively small sample size (
n = 33) and the diverse levels of disability and socioeconomic status of our study group. Nevertheless, the sample is representative of the population of an SNS, and our results were statistically significant. It would be interesting to expand the scope of this investigation to additional studies with other SNS and a larger group of children with CP, as well as to perform the same assessment on these same students after a period of treatment in terms of OD, MN, and OH. Another limitation is that we used some evaluation tools such as EDACS and GMFCS that are only validated for CP; although this pathology was the most prevalent in our study, we had students with nine different types of neurological disorders. We used these tools as there are no specific classification systems validated for the other neurological diseases and because these tools are the ones recommended in SNS in Spain. However, we recognize that different pediatric diseases or conditions might show different types of dysphagia. A further limitation of our study is the method we used to assess mastication. Due to the severity of the impairment of the participants, it was not possible to use a validated and quantitative method such as TOMASS on all students, as most of the participants were not able to manage a biscuit. Likewise, the evaluation of drooling was assessed in a dichotomic way (presence/absence); the use of more complete indices such as the Blasco index is proposed for future studies [
136,
137]. Lastly, we used the V-VST to clinically assess swallowing impairments on safety and efficacy of swallow, as done in other groups with children; despite its good psychometric properties, the fact that we developed the test, and the fact that we have wide experience with it, we acknowledge that the V-VST has not yet been appropriately validated for children and, hence, its results should be interpreted with caution. We plan to develop specific studies to validate the test in this specific population.
To sum up, our results suggest that (1) a high prevalence of OD for fluids is associated with dehydration, (2) OD for fluids and solids and poor OH could be related to respiratory infections and MN, and (3) MN could be related to poor physical and intellectual development in these children. Due to the presence of OD, impaired OH, chronic MN, and intracellular DH, these children with severe conditions such as CP and ND require complex nutritional and health management. Thus, these students must be specifically managed through nutritional and educational strategies, and the multidisciplinary team at SNS should include healthcare professionals specifically trained in these conditions. Optimal management of these SNS students may improve clinical outcomes and quality of life and reduce their needs for medical care. In accordance, we are currently introducing a personalized intervention at school and at home (
Supplementary Material S6). The optimal intervention consists of four steps: (a) measuring the nutritional, hydration, and OH status of all the students at the end of each school year; (b) establishing an educational program for families and informal caregivers and school staff on the management of OD, MN, DH, and OH of students (already started) (
Supplementary Material S7–S9); (c) developing and implementing an hydration program using homogeneous (xanthan gum) fluid thickeners for all students and specific cups to guarantee the appropriate and safe fluid provision at the appropriate bolus volume and viscosity according to the V-VST (250 vs. 800 mPa·s) and with specific support staff for hydration (
Supplementary Material 10); (d) introducing the triple adaptation of solid foods with a design (parameterization and industrialization) of fifth range dishes that meet the triple adaptation of the diet (already started)—two levels of texture (fork-mashable and purée), four levels of caloric and protein intake according to age and GMFS (1600 kcal and 30–40 g protein for 5–12 years and GMFCS II–IV; 1400 kcal and 20–25 g of protein for 5–12 years and GMFCS V; 2000 kcal and 50 g of protein for 13–23 years and GMFCS II–IV; 1700 kcal and 30–40 g of protein for 13–23 years and GMFCS V). These guidelines of textures and calories and proteins can serve as a basis for the catering companies to produce meals adapted to the special needs of these students. The final goal is to measure the effectiveness of the interventions at the end of each school year.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}