
TIMER: A Clinical Study of Energy Restriction in Women with Gestational Diabetes Mellitus

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
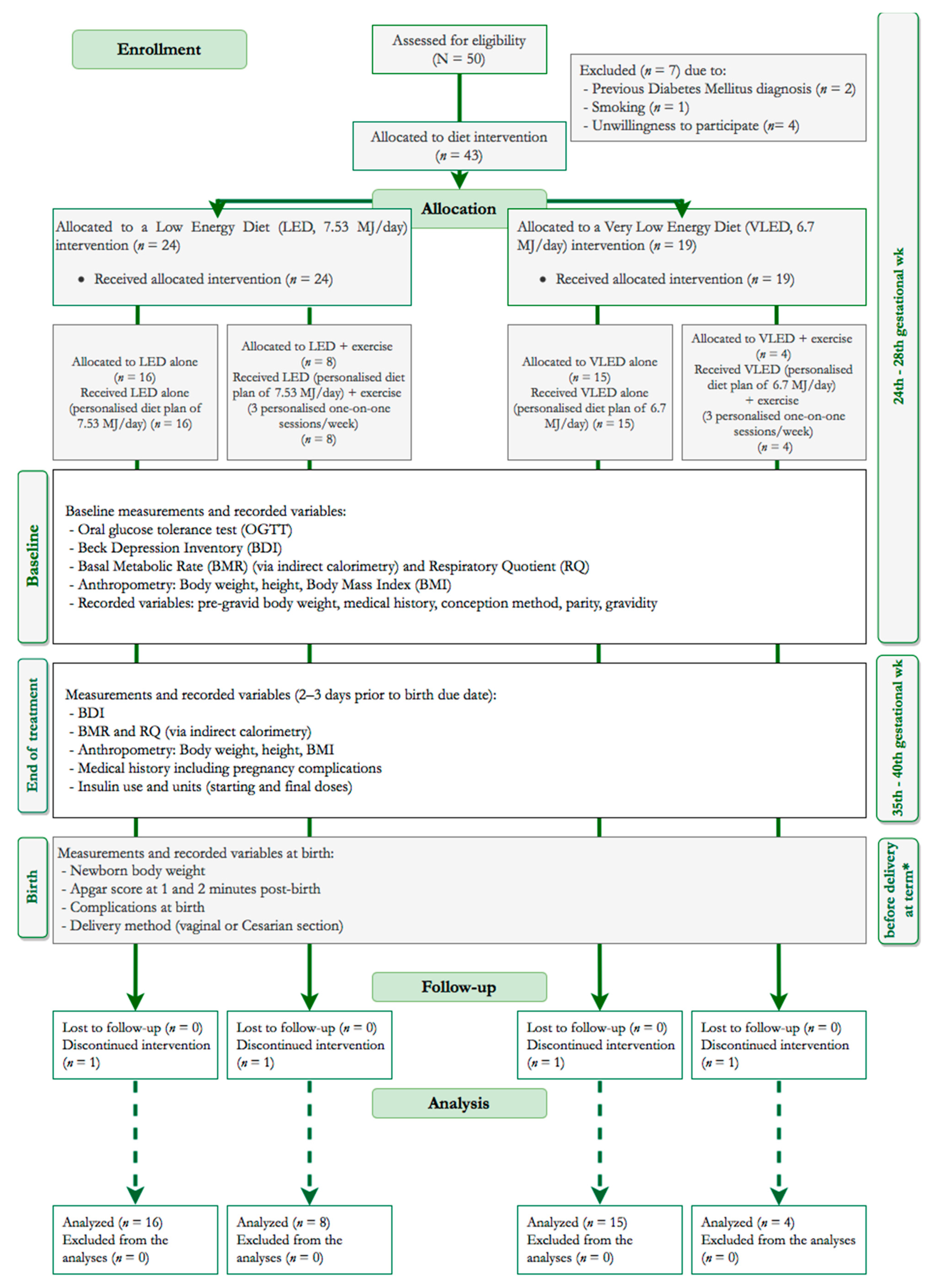
2.1. Recruitment, Allocation and Blinding
2.2. Inclusion and Exclusion Criteria
2.3. Dietary Intervention Characteristics
2.4. Exercise and Physical Activity Advice Interventions
2.5. Anthropometrics and Energy Requirements
2.6. Blood Glucose and Ketone Levels Measurements
2.7. Dietary Treatment Adherence
2.8. Maternal Characteristics and Additional Measurements
2.9. Fetal Outcomes
2.10. Composite Outcome Score
2.11. Primary Outcome Measures
2.12. Secondary Outcome Measures
2.13. Adverse Events
2.14. Ethical Approval and Informed Consent
2.15. Missing Data and Analysis Plan
2.16. Statistical Analyses
3. Results
3.1. Baseline Characteristics and Drop-Outs
3.2. Maternal and Fetal Outcomes
3.3. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheng, J.; Li, J.; Tang, X. Analysis of perinatal risk factors for small-for-gestational-age and appropriate-for-gestational-age late-term infants. Exp. Ther. Med. 2020, 19, 1719–1724. [Google Scholar] [CrossRef] [Green Version]
- Manerkar, K.; Harding, J.; Conlon, C.; McKinlay, C. Maternal gestational diabetes and infant feeding, nutrition and growth: A systematic review and meta-analysis. Br. J. Nutr. 2020, 123, 1201–1215. [Google Scholar] [CrossRef] [PubMed]
- Mitanchez, D.; Ciangura, C.; Jacqueminet, S. How Can Maternal Lifestyle Interventions Modify the Effects of Gestational Diabetes in the Neonate and the Offspring? A Systematic Review of Meta-Analyses. Nutrients 2020, 12, 353. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Yan, P.; Tao, F.; Yuan, J.; Yang, G.; Liu, Y.; Zhang, Z.-J. The association between gestational diabetes mellitus and cancer in women: A systematic review and meta-analysis of observational studies. Diabetes Metab. 2020, 46, 461–471. [Google Scholar] [CrossRef]
- Pathirana, M.M.; Lassi, Z.S.; Roberts, C.T.; Andraweera, P.H. Cardiovascular risk factors in offspring exposed to gestational diabetes mellitus in utero: Systematic review and meta-analysis. J. Dev. Orig. Health Dis. 2020, 11, 599–616. [Google Scholar] [CrossRef] [PubMed]
- Pantzartzis, K.A.; Manolopoulos, P.P.; Paschou, S.A.; Kazakos, K.; Kotsa, K.; Goulis, D.G. Gestational diabetes mellitus and quality of life during the third trimester of pregnancy. Qual. Life Res. 2019, 28, 1349–1354. [Google Scholar] [CrossRef]
- Paschou, S.A.; Sydney, G.I.; Ioakim, K.J.; Kotsa, K.; Goulis, D.G. Comment on the systematic review and meta-analysis titled “Gestational diabetes and the risk of cardiovascular disease in women”. Hormones (Athens) 2020, 19, 447–448. [Google Scholar] [CrossRef]
- Tsirou, E.; Grammatikopoulou, M.G.; Theodoridis, X.; Gkiouras, K.; Petalidou, A.; Taousani, E.; Savvaki, D.; Tsapas, A.; Goulis, D.G. Guidelines for Medical Nutrition Therapy in Gestational Diabetes Mellitus: Systematic Review and Critical Appraisal. J. Acad. Nutr. Diet. 2019, 119, 1320–1339. [Google Scholar] [CrossRef] [PubMed]
- Kintiraki, E.; Goulis, D.G. Gestational diabetes mellitus: Multi-disciplinary treatment approaches. Metabolism 2018, 86, 91–101. [Google Scholar] [CrossRef]
- Anastasiou, E.; Farmakidis, G.; Gerede, A.; Goulis, D.G.; Koukkou, E.; Kourtis, A.; Mamopoulos, A.; Papadimitriou, K.; Papadopoulos, V.; Stefos, T. Clinical practice guidelines on diabetes mellitus and pregnancy: ΙI. Gestational diabetes mellitus. Hormones (Athens) 2020, 19, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Viana, L.V.; Gross, J.L.; Azevedo, M.J. Dietary Intervention in Patients with Gestational Diabetes Mellitus: A Systematic Review and Meta-analysis of Randomized Clinical Trials on Maternal and Newborn Outcomes. Diabetes Care 2014, 37, 3345–3355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.; Middleton, P.; Shepherd, E.; Van Ryswyk, E.; Crowther, C.A. Different types of dietary advice for women with gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 2, CD009275. [Google Scholar] [CrossRef]
- Ojo, O.; Ojo, O.O.; Wang, X.-H.; Adegboye, A.R.A. The Effects of a Low GI Diet on Cardiometabolic and Inflammatory Parameters in Patients with Type 2 and Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2019, 11, 1584. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Heng, W.; Gao, J. Effects of Low Glycemic Index Diets on Gestational Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Clinical Trials. Medicine (Baltimore) 2016, 95, e3792. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-C.; Tung, Y.-T.; Chang, H.-C.; Lin, C.-H.; Chen, Y.-C. Effect of Probiotic Supplementation on Newborn Birth Weight for Mother with Gestational Diabetes Mellitus or Overweight/Obesity: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3477. [Google Scholar] [CrossRef]
- New Zealand Ministry of Health (NZMoH). Screening, Diagnosis and Management of Gestational Diabetes in New Zealand A Clinical Practice Guideline; New Zealand Ministry of Health: Wellington, New Zealand, 2014.
- Scottish Intercollegiate Guidelines Network (SIGN). Management of Diabetes. A national Clinical Guideline; Scottish Intercollegiate Guidelines Network (SIGN): Edinburgh, UK, 2017. [Google Scholar]
- Irish Health Service Executive (IHSE). Guidelines for the Management of Pre-Gestational and Gestational Diabetes Mellitus from Pre-Conception to the Postnatal Period: Changing Practice to Support Service Delivery; Irish Health Service Executive (IHSE): Dublin, Ireland, 2010.
- Malaysia Health Technology Assessment Section (MaHTAS). Clinical Practice Guidelines: Management of Diabetes in Pregnancy; Malaysia Health Technology Assessment Section (MaHTAS): Putrajaya, Malaysia, 2017. [Google Scholar]
- International Diabetes Federation (IDF). Pregnancy and Diabetes: Global Guideline; International Diabetes Federation (IDF): Brussels, Belgium, 2009. [Google Scholar]
- Grammatikopoulou, M.G.; Theodoridis, X.; Gkiouras, K.; Lampropoulou, M.; Petalidou, A.; Patelida, M.; Tsirou, E.; Papoutsakis, C.; Goulis, D.G. Methodological quality of clinical practice guidelines for nutrition and weight gain during pregnancy: A systematic review. Nutr. Rev. 2020, 78, 546–562. [Google Scholar] [CrossRef]
- Italian Association of Diabetologists-Diabete Italia and Italian Society of Diabetology (IAD/DI/ISD). Italian Standards for Diabetes Mellitus; Italian Association of Diabetologists-Diabete Italia and Italian Society of Diabetology (IAD/DI/ISD): Torino, Italian, 2007. [Google Scholar]
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; Di Renzo, G.C.; Roura, L.C.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care#. Int. J. Gynecol. Obstet. 2015, 131, S173. [Google Scholar] [CrossRef]
- Kleinwechter, H.; Schäfer-Graf, U.; Bührer, C.; Hoesli, I.; Kainer, F.; Kautzky-Willer, A.; Pawlowski, B.; Schunck, K.; Somville, T.; Sorger, M. Gestational Diabetes Mellitus (GDM) Diagnosis, Therapy and Follow-Up Care. Exp. Clin. Endocrinol. Diabetes 2014, 122, 395–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Nimr, R.I.; Hakeem, R.; Moreschi, J.M.; Gallo, S.; McDermid, J.M.; Pari-Keener, M.; Stahnke, B.; Papoutsakis, C.; Handu, D.; Cheng, F.W. Effects of Bariatric Surgery on Maternal and Infant Outcomes of Pregnancy-An Evidence Analysis Center Systematic Review. J. Acad. Nutr. Diet. 2019, 119, 1921–1943. [Google Scholar] [CrossRef]
- Duarte-Gardea, M.O.; Gonzales-Pacheco, D.M.; Reader, D.M.; Thomas, A.M.; Wang, S.R.; Gregory, R.P.; Piemonte, T.A.; Thompson, K.L.; Moloney, L. Academy of Nutrition and Dietetics Gestational Diabetes Evidence-Based Nutrition Practice Guideline. J. Acad. Nutr. Diet. 2018, 118, 1719–1742. [Google Scholar] [CrossRef] [PubMed]
- Hodson, K.; Dalla Man, C.; Smith, F.E.; Barnes, A.; McParlin, C.; Cobelli, C.; Robson, S.C.; Araújo-Soares, V.; Taylor, R. Liver triacylglycerol content and gestational diabetes: Effects of moderate energy restriction. Diabetologia 2017, 60, 306–313. [Google Scholar] [CrossRef] [Green Version]
- Magee, M.S.; Knopp, R.H.; Benedetti, T.J. Metabolic effects of 1200-kcal diet in obese pregnant women with gestational diabetes. Diabetes 1990, 39, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Gillmer, M.D.; Maresh, M.; Beard, R.W.; Elkeles, R.S.; Alderson, C.; Bloxham, B. Low energy diets in the treatment of gestational diabetes. Acta Endocrinol. Suppl. (Copenh) 1986, 277, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Knopp, R.H.; Magee, M.S.; Raisys, V.; Benedetti, T.; Bonet, B. Hypocaloric diets and ketogenesis in the management of obese gestational diabetic women. J. Am. Coll. Nutr. 1991, 10, 649–667. [Google Scholar] [CrossRef]
- Feng, Y.; Zhao, Z.; Fu, D.; Gao, W.; Zhang, F. Maternal and neonatal outcomes after energy-restricted diet for women with gestational diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore) 2021, 100, e25279. [Google Scholar] [CrossRef] [PubMed]
- Garner, P.; Okun, N.; Keely, E.; Wells, G.; Perkins, S.; Sylvain, J.; Belcher, J. A randomized controlled trial of strict glycemic control and tertiary level obstetric care versus routine obstetric care in the management of gestational diabetes: A pilot study. Am. J. Obstet. Gynecol. 1997, 177, 190–195. [Google Scholar] [CrossRef]
- Rae, A.; Bond, D.; Evans, S.; North, F.; Roberman, B.; Walters, B. A randomised controlled trial of dietary energy restriction in the management of obese women with gestational diabetes. Aust. N. Z. J. Obstet. Gynaecol. 2000, 40, 416–422. [Google Scholar] [CrossRef]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; de Leiva, A.; Hod, M.; et al. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, Y.M.; Yan, J.; Yang, H.X. Identification of severe gestational diabetes mellitus after new criteria used in China. J. Perinatol. 2016, 36, 90–94. [Google Scholar] [CrossRef]
- Black, M.H.; Sacks, D.A.; Xiang, A.H.; Lawrence, J.M. Clinical outcomes of pregnancies complicated by mild gestational diabetes mellitus differ by combinations of abnormal oral glucose tolerance test values. Diabetes Care 2010, 33, 2524–2530. [Google Scholar] [CrossRef] [Green Version]
- Pari-Keener, M.; Gallo, S.; Stahnke, B.; McDermid, J.M.; Al-Nimr, R.I.; Moreschi, J.M.; Hakeem, R.; Handu, D.; Cheng, F.W. Maternal and Infant Health Outcomes Associated with Medical Nutrition Therapy by Registered Dietitian Nutritionists in Pregnant Women with Malnutrition: An Evidence Analysis Center Systematic Review. J. Acad. Nutr. Diet. 2020, 120, 1730–1744. [Google Scholar] [CrossRef]
- Geil, P.B. Choose Your Foods: Exchange Lists for Diabetes: The 2008 Revision of Exchange Lists for Meal Planning. Diabetes Spectr. 2008, 21, 281–283. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association 14. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S183–S192. [Google Scholar] [CrossRef] [Green Version]
- Feig, D.S.; Berger, H.; Donovan, L.; Godbout, A.; Kader, T.; Keely, E.; Sanghera, R.; Sanghera, R. Diabetes and Pregnancy. Can. J. Diabetes 2018, 42, S255–S282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diabetes Care Program of Nova Scotia (DCPoNS). Pregnancy and Diabetes Guidelines: Approaches to Practice; Diabetes Care Program of Nova Scotia (DCPoNS): Halifax, NS, Canada, 2014. [Google Scholar]
- Savvaki, D.; Taousani, E.; Goulis, D.G.; Tsirou, E.; Voziki, E.; Douda, H.; Nikolettos, N.; Tokmakidis, S.P. Guidelines for exercise during normal pregnancy and gestational diabetes: A review of international recommendations. Hormones (Athens) 2018, 17, 521–529. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012; ISBN 9780199754038. [Google Scholar]
- Ye, C.; Ruan, Y.; Zou, L.; Li, G.; Li, C.; Chen, Y.; Jia, C.; Megson, I.L.; Wei, J.; Zhang, W. The 2011 Survey on Hypertensive Disorders of Pregnancy (HDP) in China: Prevalence, Risk Factors, Complications, Pregnancy and Perinatal Outcomes. PLoS ONE 2014, 9, e100180. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.; Steer, R.; Brown, G. Beck Depression Inventory, 2nd ed.; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Fountoulakis, K.N.; Iacovides, A.; Kleanthous, S.; Samolis, S.; Gougoulias, K.; St Kaprinis, G.; Bech, P. The Greek translation of the symptoms rating scale for depression and anxiety: Preliminary results of the validation study. BMC Psychiatry 2003, 3, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spong, C.Y. Defining “term” pregnancy: Recommendations from the defining “term” pregnancy workgroup. JAMA-J. Am. Med. Assoc. 2013, 309, 2445–2446. [Google Scholar] [CrossRef]
- Engle, W.A.; Tomashek, K.M.; Wallman, C.; Stark, A.R.; Adamkin, D.H.; Batton, D.G.; Bell, E.F.; Bhutani, V.K.; Denson, S.E.; Martin, G.I.; et al. “Late-preterm” infants: A population at risk. Pediatrics 2007, 120, 1390–1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Recommendations on Newborn Health: Guidelines Approved by the WHO Guidelines Review Committee; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Villar, J.; Ismail, L.C.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy of Pediatrics Committee on Fetus and Newborn. American College of Obstetricians and Gynecologists Committee on Obstetric Practice The Apgar Score. Pediatrics 2015, 136, 819–822. [Google Scholar] [CrossRef] [Green Version]
- Executive Summary: Neonatal Encephalopathy and Neurologic Outcome, Second Edition. Report of the American College of Obstetricians and Gynecologists’ Task Force on Neonatal Encephalopathy. Obstet. Gynecol. 2014, 123, 896–901. [CrossRef] [PubMed]
- Novicoff, W.M.; Wagner, D.P.; Knaus, W.A.; Kane, E.K.; Cecere, F.; Draper, E.; Ferguson, J.E. Initial development of a system-wide maternal-fetal outcomes assessment program. Am. J. Obstet. Gynecol. 2000, 183, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.-Y.; Zhang, L.-F.; He, J.-R.; Lu, J.-H.; Chen, N.-N.; Xiao, W.-Q.; Yuan, M.-Y.; Xia, H.-M.; Lam, K.B.H.; Qiu, X. Association Between Maternal Hyperglycemia and Composite Maternal-Birth Outcomes. Front. Endocrinol. (Lausanne) 2018, 9, 755. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Gillespie, B.M. Intention-to-treat in randomized controlled trials: Recommendations for a total trial strategy. Res. Nurs. Health 2010, 33, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Del Re, A.C.; Maisel, N.C.; Blodgett, J.C.; Finney, J.W. Intention-to-treat analyses and missing data approaches in pharmacotherapy trials for alcohol use disorders. BMJ Open 2013, 3, e003464. [Google Scholar] [CrossRef] [PubMed]
- The Jamovi Project (2021). Jamovi (Version 1.6) [Computer Software]. Available online: https://www.jamovi.org2020 (accessed on 17 July 2021).
- Chen, L.; Stralovich-Romani, A. Nutrition in Critically Ill Patients. In Critical Care Secrets; Parsons, P.E., Wiener-Kronish, J.P., Eds.; Mosby: Philadelphia, PA, USA, 2007; pp. 39–46. ISBN 978-1-4160-3206-9. [Google Scholar]
- Reader, D.; Splett, P.; Gunderson, E.P.; Diabetes Care and Education Dietetic Practice Group. Impact of gestational diabetes mellitus nutrition practice guidelines implemented by registered dietitians on pregnancy outcomes. J. Am. Diet. Assoc. 2006, 106, 1426–1433. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; Monk, A.; Barry, B.; McCllain, K.; Weaver, T.; Cooper, N.; Upham, P.; Bergerstall, R.; Mazze, R.S. Effectiveness of Medical Nutrition Therapy Provided by Dietitians in the Management of Non-Insulin-Dependent Diabetes Mellitus. A Randomized, Controlled Clinical Trial. J. Am. Diet. Assoc. 1995, 95, 1009–1017. [Google Scholar] [CrossRef]
- Renault, K.M.; Carlsen, E.M.; Hædersdal, S.; Nilas, L.; Secher, N.J.; Eugen-Olsen, J.; Cortes, D.; Olsen, S.F.; Halldorsson, T.I.; Nørgaard, K. Impact of lifestyle intervention for obese women during pregnancy on maternal metabolic and inflammatory markers. Int. J. Obes. (Lond) 2017, 41, 598–605. [Google Scholar] [CrossRef]
- Vounzoulaki, E.; Dipla, K.; Kintiraki, E.; Triantafyllou, A.; Grigoriadou, I.; Koletsos, N.; Zafeiridis, A.; Goulis, D.G.; Douma, S. Pregnancy and post-partum muscle and cerebral oxygenation during intermittent exercise in gestational diabetes: A pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 232, 54–59. [Google Scholar] [CrossRef]
- Wexler, D.J.; Powe, C.E.; Barbour, L.A.; Buchanan, T.; Coustan, D.R.; Corcoy, R.; Damm, P.; Dunne, F.; Feig, D.S.; Ferrara, A.; et al. Research Gaps in Gestational Diabetes Mellitus. Obstet. Gynecol. 2018, 132, 496–505. [Google Scholar] [CrossRef]
- Reader, D.M. Medical Nutrition Therapy and Lifestyle Interventions. Diabetes Care 2007, 30, S188–S193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusinski, L.C.; Murphy, H.R.; De Lucia Rolfe, E.; Rennie, K.L.; Oude Griep, L.M.; Hughes, D.; Taylor, R.; Meek, C.L. Dietary Intervention in Pregnant Women with Gestational Diabetes; Protocol for the DiGest Randomised Controlled Trial. Nutrients 2020, 12, 1165. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, T.L.; Brand-Miller, J.C. Nutrition Therapy in Gestational Diabetes Mellitus: Time to Move Forward. Diabetes Care 2018, 41, 1343–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mijatovic, J.; Louie, J.C.Y.; Buso, M.E.C.; Atkinson, F.S.; Ross, G.P.; Markovic, T.P.; Brand-Miller, J.C. Effects of a modestly lower carbohydrate diet in gestational diabetes: A randomized controlled trial. Am. J. Clin. Nutr. 2020, 112, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Castilla, C.; Hernandez, M.; Bergua, M.; Alvarez, M.C.; Arce, M.A.; Rodriguez, K.; Martinez-Alonso, M.; Iglesias, M.; Mateu, M.; Santos, M.D.; et al. Low-Carbohydrate Diet for the Treatment of Gestational Diabetes Mellitus. Diabetes Care 2013, 36, 2233–2238. [Google Scholar] [CrossRef] [Green Version]
- Kintiraki, E.; Goulis, D.G.; Mameletzi, S.; Kasmas, S.; Athanasiadis, A.; Assimakopoulos, E.; Tsapas, A.; Dinas, K.; Tarlatzis, B.C. Large- and small-for-gestational-age neonates born by women with gestational diabetes mellitus diagnosed by the new IADPSG criteria: A case-control study of 289 patients and 1 108 controls. Exp. Clin. Endocrinol. Diabetes 2013, 121, 262–265. [Google Scholar] [CrossRef]
- Snyder, J.; Gray-Donald, K.; Koski, K.G. Predictors of infant birth weight in gestational diabetes. Am. J. Clin. Nutr. 1994, 59, 1409–1414. [Google Scholar] [CrossRef]
- Barnes, R.A.; Edghill, N.; Mackenzie, J.; Holters, G.; Ross, G.P.; Jalaludin, B.B.; Flack, J.R. Predictors of large and small for gestational age birthweight in offspring of women with gestational diabetes mellitus. Diabet. Med. 2013, 30, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Shook, R.P.; Hand, G.A.; Paluch, A.E.; Wang, X.; Moran, R.; Hébert, J.R.; Jakicic, J.M.; Blair, S.N. High respiratory quotient is associated with increases in body weight and fat mass in young adults. Eur. J. Clin. Nutr. 2016, 70, 1197–1202. [Google Scholar] [CrossRef]
- Butte, N.F. Carbohydrate and lipid metabolism in pregnancy: Normal compared with gestational diabetes mellitus. Am. J. Clin. Nutr. 2000, 71, 1256S–1261S. [Google Scholar] [CrossRef] [PubMed]
- Assel, B.; Rossi, K.; Kalhan, S. Glucose metabolism during fasting through human pregnancy: Comparison of tracer method with respiratory calorimetry. Am. J. Physiol. Endocrinol. Metab. 1993, 265, E351–E356. [Google Scholar] [CrossRef]
- Melzer, K.; Kayser, B.; Schutz, Y. Respiratory quotient evolution during normal pregnancy: What nutritional or clinical information can we get out of it? Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 176, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Liu, F.; Li, S. Metabolic Adaptations in Pregnancy: A Review. Ann. Nutr. Metab. 2017, 70, 59–65. [Google Scholar] [CrossRef]
- López, L.B.; Calvo, E.B.; Poy, M.S.; del Valle Balmaceda, Y.; Cámera, K. Changes in skinfolds and mid-upper arm circumference during pregnancy in Argentine women. Matern. Child Nutr. 2011, 7, 253–262. [Google Scholar] [CrossRef]
- Mwanri, A.W.; Kinabo, J.; Ramaiya, K.; Feskens, E.J.M. Prevalence of gestational diabetes mellitus in urban and rural Tanzania. Diabetes Res. Clin. Pract. 2014, 103, 71–78. [Google Scholar] [CrossRef]
- Msollo, S.S.; Martin, H.D.; Mwanri, A.W.; Petrucka, P. Prevalence of hyperglycemia in pregnancy and influence of body fat on development of hyperglycemia in pregnancy among pregnant women in urban areas of Arusha region, Tanzania. BMC Pregnancy Childbirth 2019, 19, 315. [Google Scholar] [CrossRef] [Green Version]
- Allehdan, S.S.; Basha, A.S.; Asali, F.F.; Tayyem, R.F. Dietary and exercise interventions and glycemic control and maternal and newborn outcomes in women diagnosed with gestational diabetes: Systematic review. Diabetes Metab. Syndr. 2019, 13, 2775–2784. [Google Scholar] [CrossRef]
- Hayes, L.; McParlin, C.; Azevedo, L.B.; Jones, D.; Newham, J.; Olajide, J.; McCleman, L.; Heslehurst, N. The Effectiveness of Smoking Cessation, Alcohol Reduction, Diet and Physical Activity Interventions in Improving Maternal and Infant Health Outcomes: A Systematic Review of Meta-Analyses. Nutrients 2021, 13, 1036. [Google Scholar] [CrossRef]
- Hinkle, S.N.; Li, M.; Grewal, J.; Yisahak, S.F.; Grobman, W.A.; Newman, R.B.; Wing, D.A.; Grantz, K.L.; Zhang, C. Changes in Diet and Exercise in Pregnant Women after Diagnosis with Gestational Diabetes: Findings from a Longitudinal Prospective Cohort Study. J. Acad. Nutr. Diet. 2021. [Google Scholar] [CrossRef]
- Galliano, L.M.; Del Vecchio, A.H.M.; Silvani, J.; Façanha, C.; Del Vecchio, F.B. Physical activity level in women with gestational diabetes mellitus: Lifestyle INtervention for Diabetes prevention after pregnancy (LINDA-Brasil) study. J. Diabetes 2019, 11, 457–465. [Google Scholar] [CrossRef]
- Wang, R.; Yang, Q.; Sun, T.; Qiang, Y.; Li, X.; Li, H.; Tang, Y.; Yang, L.; Sun, J.; Li, B. Physical Exercise is Associated with Glycemic Control among Women with Gestational Diabetes Mellitus: Findings from a Prospective Cohort in Shanghai, China. Diabetes Metab. Syndr. Obes. 2021, 14, 1949–1961. [Google Scholar] [CrossRef]
- Onaade, O.; Maples, J.M.; Rand, B.; Fortner, K.B.; Zite, N.B.; Ehrlich, S.F. Physical activity for blood glucose control in gestational diabetes mellitus: Rationale and recommendations for translational behavioral interventions. Clin. Diabetes Endocrinol. 2021, 7, 7. [Google Scholar] [CrossRef]
- Dipla, K.; Zafeiridis, A.; Mintziori, G.; Boutou, A.K.; Goulis, D.G.; Hackney, A.C. Exercise as a Therapeutic Intervention in Gestational Diabetes Mellitus. Endocrines 2021, 2, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Chatzakis, C.; Goulis, D.G.; Mareti, E.; Eleftheriades, M.; Zavlanos, A.; Dinas, K.; Sotiriadis, A. Prevention of gestational diabetes mellitus in overweight or obese pregnant women: A network meta-analysis. Diabetes Res. Clin. Pract. 2019, 158, 107924. [Google Scholar] [CrossRef]
- Szatko, A.; Kacperczyk-Bartnik, J.; Bartnik, P.; Mabiala, E.; Goryszewska, M.; Dobrowolska-Redo, A.; Romejko-Wolniewicz, E. Physical activity during pregnancy—the state of Polish women’s knowledge. Ginekol. Pol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Pratilas, G.C.; Sotiriadis, A.; Dinas, K. Is high use of caesarean section sometimes justified? Lancet 2019, 394, 25–26. [Google Scholar] [CrossRef] [Green Version]
- Mossialos, E.; Allin, S.; Karras, K.; Davaki, K. An investigation of Caesarean sections in three Greek hospitals: The impact of financial incentives and convenience. Eur. J. Public Health 2005, 15, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Profit, J.; Typpo, K.V.; Hysong, S.J.; Woodard, L.D.; Kallen, M.A.; Petersen, L.A. Improving benchmarking by using an explicit framework for the development of composite indicators: An example using pediatric quality of care. Implement. Sci. 2010, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assaf-Balut, C.; García de la Torre, N.; Fuentes, M.; Durán, A.; Bordiú, E.; del Valle, L.; Valerio, J.; Jiménez, I.; Herraiz, M.; Izquierdo, N.; et al. A High Adherence to Six Food Targets of the Mediterranean Diet in the Late First Trimester is Associated with a Reduction in the Risk of Materno-Foetal Outcomes: The St. Carlos Gestational Diabetes Mellitus Prevention Study. Nutrients 2018, 11, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepherd, E.; Gomersall, J.C.; Tieu, J.; Han, S.; Crowther, C.A.; Middleton, P. Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 11, CD010443. [Google Scholar] [CrossRef] [PubMed]
- Dabelea, D.; Mayer-Davis, E.J.; Lamichhane, A.P.; D’Agostino, R.B.; Liese, A.D.; Vehik, K.S.; Narayan, K.M.V.; Zeitler, P.; Hamman, R.F. Association of Intrauterine Exposure to Maternal Diabetes and Obesity with Type 2 Diabetes in Youth: The SEARCH Case-Control Study. Diabetes Care 2008, 31, 1422–1426. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, T.L. Carbohydrate Content in the GDM Diet: Two Views: View 1: Nutrition Therapy in Gestational Diabetes: The Case for Complex Carbohydrates. Diabetes Spectr. 2016, 29, 82–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Parameters | LED (n = 16) | LED + Exercise (n = 8) | VLED (n = 15) | VLED + Exercise (n = 4) | p Value (4 arms) | p Value (LED vs. VLED) |
|---|---|---|---|---|---|---|
| Age (years) | 34.4 ± 4.99 | 32.6 ± 4.24 | 33.9 ± 3.78 | 36.8 ± 2.99 | 0.45 1 | 0.75 3 |
| Pre-gravid body weight (kg) | 76.3 ± 17.3 | 70.8 ± 11.9 | 86.2 ± 17.0 | 69.0 ± 13.5 | 0.10 1 | 0.11 3 |
| Height (cm) | 167 (162–174) | 168 (165–169) | 167 (161–170) | 160 (160–163) | 0.48 1 | 0.42 3 |
| Pre-gravid BMI (kg/m2) | 25.3 (23.1–31.5) | 26.3 (23.1–28.1) | 32.1 (26.8–35.0) | 23.8 (23.2–26.9) | 0.08 1 | 0.05 4 |
| MUAC (cm) | 28.3 ± 3.92 | 28.7 ± 2.85 | 31.5 ± 3.18 | 28.8 ± 2.53 | 0.04 1 | 0.02 3 |
| Method of conception Spontaneous/IUI/IVF (n) | 16/0/0 | 6/1/1 | 14/1/0 | 4/0/0 | 0.23 2 | 0.48 2 |
| Gravidity 1st/2nd/3rd/4th/5th/6th (n) | 5/7/1/1/1/1 | 5/3/0/0/0/0 | 3/10/1/1/0/0 | 1/2/0/1/0/0 | 0.75 2 | 0.84 2 |
| Parity 0/1/2/3 (n) | 8/6/1/1 | 6/2/0/0 | 4/11/0/0 | 2/1/1/0 | 0.11 2 | 0.14 2 |
| RMR (kcal/day) | 1781 (1662–1851) | 1689 (1581–1945) | 1842 (1604–2150) | 1811 (1613–1909) | 0.82 1 | 0.47 4 |
| RQ | 0.790 (0.760–0.843) | 0.805 (0.800–0.833) | 0.810 (0.775–0.855) | 0.820 (0.808–0.837) | 0.66 1 | 0.67 3 |
| BDI | 10.0 (7.75–15.0) | 8.50 (7.25–13.5) | 10.0 (6.00–11.0) | 8.00 (7.50–8.50) | 0.61 1 | 0.36 4 |
| LED (n = 16) | LED + Exercise (n = 8) | VLED (n = 15) | VLED + Exercise (n = 4) | p Value | ||
|---|---|---|---|---|---|---|
| Total gestational weight gain (kg) | 12.0 (9.8–14.3) | 10.3 (8.9–11.5) | 6.0 (2.6–9.3) | 9.0 (6.7–12.5) | 0.03 1 | |
| Insulin use: | Initiation week | 24 (21–28) | 30 (29–30) | 22 (15–28) | 25 (24–25) | 0.15 1 |
| Units at labor (IU) | 16 (9–33) | 14 (11–21) | 26 (19–30) | 13 (11–16) | 0.44 1 | |
| Insulin users (n) | 8 (50.0%) | 4 (50.0%) | 8 (53.3%) | 2 (50.0%) | 1.00 2 | |
| Infant birth weight (g) | 3120 (2815–3283) | 2980 (2948–3255) | 2950 (2750–3245) | 3275 (3115–3485) | 0.47 1 | |
| Type of delivery: | Vaginal (n) | 8 (50.0%) | 5 (62.5%) | 5 (33.3%) | 1 (25.0%) | 0.48 2 |
| C-section (n) | 8 (50.0%) | 3 (37.5%) | 10 (66.7%) | 3 (75.0%) | ||
| Prematurity (n) | 0 (0.0%) | 0 (0.0%) | 1 (6.7%) | 1 (25.0%) | 0.14 2 | |
| Infant birth weight categorization: | AGA (n) | 13 (81.3%) | 8 (100.0%) | 14 (93.3%) | 3 (75.0%) | 0.52 2 |
| SGA (n) | 1 (6.3%) | 0 (0.0%) | 1 (6.7%) | 0 (0.0%) | ||
| LGA (n) | 2 (12.5%) | 0 (0.0%) | 0 (0.0%) | 1 (25.0%) | ||
| Infant sex: | Female/Male (n, %) | 10/6 (62.5%/37.5%) | 4/4 (50.0%/50.0%) | 8/7 (53.3%/46.7%) | 3/1 (75.0%/25.0%) | 0.86 2 |
| Apgar score: | at 1 min post-birth | 8.0 (8.0–8.0) | 9.0 (8.0–9.0) | 8.0 (8.0–8.0) | 8.0 (8.0–8.0) | 0.12 1 |
| at 5 min post-birth | 9.0 (9.0–9.0) | 9.0 (9.0–9.0) | 9.0 (9.0–9.0) | 9.0 (9.0–9.0) | 0.23 1 | |
| Complications at delivery (n) | 1 (6.3%) | 0 (0%) | 1 (6.7%) | 2 (50.0%) | 0.07 2 | |
| Composite outcome score components: | Stillbirth (n) | 0 | 0 | 0 | 0 | - |
| Preeclampsia (n) | 0 | 0 | 0 | 0 | - | |
| C-section delivery (n) | 8 (50.0%) | 3 (37.5%) | 10 (66.7%) | 3 (75.0%) | 0.48 2 | |
| Gestational age 24–34 wk (n) | 0 | 0 | 0 | 0 | ||
| Gestational age 34–36 wk (n) | 0 | 0 | 1 (6.7%) | 1 (25.0%) | 0.14 2 | |
| Gestational age ≥ 37 wk, <42 wk (n) | 16 (100%) | 8 (100%) | 14 (93.3%) | 3 (75.0%) | ||
| Gestational age > 42 wk (n) | 0 | 0 | 0 | 0 | ||
| Birth weight < 750 g (n) | 0 | 0 | 0 | 0 | ||
| Birth weight 750–1500 g (n) | 0 | 0 | 0 | 0 | ||
| Birth weight 1500–2500 g (n) | 1 (6.3%) | 0 | 1 (6.7%) | 0 | 1.00 2 | |
| Birth weight 2500–4000 g (n) | 15 (93.8%) | 8 (100%) | 14 (93.3%) | 4 (100%) | ||
| Birth weight > 4000 g (n) | 0 | 0 | 0 | 0 | ||
| Composite maternal-fetal score | 1.3 (0.0–2.5) | 0.0 (0.0–2.5) | 2.5 (0.0–2.5) | 2.5 (2.4–2.5) | 0.36 1 | |
| Parameters | LED (n = 16) | VLED (n = 15) | p Value | |
|---|---|---|---|---|
| Total gestational weight gain (kg) | 11.4 ± 5.0 | 6.8 ± 7.6 | 0.05 1 | |
| Insulin use | Initiation week | 25 ± 7 | 22 ± 8 | 0.36 1 |
| Units at labor (IU) | 18.9 ± 13.7 | 26.8 ± 13.6 | 0.27 1 | |
| Insulin users (n) | 8 (50.0%) | 8 (53.3%) | 0.85 2 | |
| Infant birth weight (g) | 3114 ± 400 | 3011 ± 333 | 0.44 1 | |
| Type of delivery | Vaginal (n) | 8 (50.0%) | 5 (33.3%) | 0.35 2 |
| C-section (n) | 8 (50.0%) | 10 (66.7%) | ||
| Prematurity (n) | 0 (0.0%) | 1 (6.7%) | 0.48 3 | |
| Infant birth weight categorization | AGA (n) | 13 (81.3%) | 14 (93.3%) | 0.73 3 |
| SGA (n) | 1 (6.3%) | 1 (6.7%) | ||
| LGA (n) | 2 (12.5%) | 0 (0.0%) | ||
| Infant sex: Female/Male (n) | 10/6 (62.5%/37.5%) | 8/7 (53.3%/46.7%) | 0.61 2 | |
| Apgar score: | at 1 min post-birth | 8.0 (8.0–8.0) | 8.0 (8.0–8.0) | 0.55 4 |
| at 5 min post-birth | 9.0 (9.0–9.0) | 9.0 (9.0–9.0) | 1.00 4 | |
| Complications at delivery (n) | 1 (6.3%) | 1 (6.7%) | 1.00 3 | |
| Composite outcome score components | Stillbirth (n) | 0 | 0 | |
| Preeclampsia (n) | 0 | 0 | ||
| C-section delivery (n) | 8 (50.0%) | 10 (66.7%) | 0.35 2 | |
| Gestational age 24–34 wk (n) | 0 | 0 | ||
| Gestational age 34–36 wk (n) | 0 | 1 (6.7%) | ||
| Gestational age ≥ 37 wk, <42 wk (n) | 16 (100%) | 14 (93.3%) | 0.48 3 | |
| Gestational age > 42 wk (n) | 0 | 0 | ||
| Birth weight < 750 g (n) | 0 | 0 | ||
| Birth weight 750–1500 g (n) | 0 | 0 | ||
| Birth weight 1500–2500 g (n) | 1 (6.3%) | 1 (6.7%) | ||
| Birth weight 2500–4000 g (n) | 15 (93.8%) | 14 (93.3%) | 1.00 3 | |
| Birth weight > 4000 g (n) | 0 | 0 | ||
| Composite maternal-fetal score | 1.3 (0.0–2.5) | 2.5 (0.0–2.5) | 0.41 4 | |
| LED (n = 16) | LED + Exercise (n = 8) | VLED (n = 15) | VLED + Exercise (n = 4) | p Value 1 | |
|---|---|---|---|---|---|
| RMR (kcal/day) | 177.0 (37.3 to 265.0) | 279.0 (184.0 to 318.0) | 121.0 (−51.0, to 339.0) | 231.0 (147.0 to 360.0) | 0.56 |
| RQ | 0.025 (−0.003 to 0.060) | 0.00 (−0.013 to 0.03) | 0.010 (−0.005 to 0.050) | −0.025 (−0.053 to −0.018) | 0.12 |
| MUAC (cm) | 1.0 (−0.50 to 1.50) | −0.10 (−1.00 to 0.50) | −1.20 (−1.50 to 0.150) | −0.85 (−1.50 to −0.15) | 0.11 |
| BDI score | 0.00 (−1.00 to 2.00) | −0.50 (−1.00 to 2.00) | 0.00 (−1.00 to 1.00) | 1.00 (0.50 to 2.50) | 0.85 |
| LED (n = 16) | VLED (n = 15) | p Value 1 | |
|---|---|---|---|
| RMR (kcal/day) | 170.0 (37.3 to 265.0) | 121.0 (−58.0 to 339.0) | 0.92 |
| RQ | 0.025 (−0.003 to 0.060) | 0.010 (−0.005 to 0.050) | 0.61 |
| MUAC (cm) | 1.00 (−0.50 to 1.50) | −1.20 (−1.50 to 0.35) | 0.07 |
| BDI score | 0.00 (−1.00 to 2.00) | 0.00 (−1.00 to 1.00) | 0.75 |
| Ketone Urine Value | LED (n = 16) | LED + Exercise (n = 8) | VLED (n = 15) | VLED + Exercise (n = 4) | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| 0 (negative) | 142 | 98.60% | 72 | 100% | 132 | 97.80% | 36 | 100% | 382 | 98.70% |
| +1 (mild) | 2 | 1.40% | 0 | 0% | 1 | 0.70% | 0 | 0% | 3 | 0.80% |
| +2 (moderate) | 0 | 0% | 0 | 0% | 1 | 0.70% | 0 | 0% | 1 | 0.26% |
| +3 (ketonuria) | 0 | 0% | 0 | 0% | 1 | 0.70% | 0 | 0% | 1 | 0.26% |
| Total | 144 | 72 | 135 | 36 | 387 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsirou, E.; Grammatikopoulou, M.G.; Nigdelis, M.P.; Taousani, E.; Savvaki, D.; Assimakopoulos, E.; Tsapas, A.; Goulis, D.G. TIMER: A Clinical Study of Energy Restriction in Women with Gestational Diabetes Mellitus. Nutrients 2021, 13, 2457. https://doi.org/10.3390/nu13072457
Tsirou E, Grammatikopoulou MG, Nigdelis MP, Taousani E, Savvaki D, Assimakopoulos E, Tsapas A, Goulis DG. TIMER: A Clinical Study of Energy Restriction in Women with Gestational Diabetes Mellitus. Nutrients. 2021; 13(7):2457. https://doi.org/10.3390/nu13072457
Chicago/Turabian StyleTsirou, Efrosini, Maria G. Grammatikopoulou, Meletios P. Nigdelis, Eleftheria Taousani, Dimitra Savvaki, Efstratios Assimakopoulos, Apostolos Tsapas, and Dimitrios G. Goulis. 2021. "TIMER: A Clinical Study of Energy Restriction in Women with Gestational Diabetes Mellitus" Nutrients 13, no. 7: 2457. https://doi.org/10.3390/nu13072457
APA StyleTsirou, E., Grammatikopoulou, M. G., Nigdelis, M. P., Taousani, E., Savvaki, D., Assimakopoulos, E., Tsapas, A., & Goulis, D. G. (2021). TIMER: A Clinical Study of Energy Restriction in Women with Gestational Diabetes Mellitus. Nutrients, 13(7), 2457. https://doi.org/10.3390/nu13072457