
Effects of DHA-Rich n-3 Fatty Acid Supplementation and/or Resistance Training on Body Composition and Cardiometabolic Biomarkers in Overweight and Obese Post-Menopausal Women

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Nutritional Intervention
2.4. Supplements Information
2.5. Resistance Training Program
2.6. Evaluation of Weight Loss and Body Composition
2.7. Evaluation of Lipid and Glucose Metabolism and other Biomarkers
2.8. Statistical Analysis
3. Results
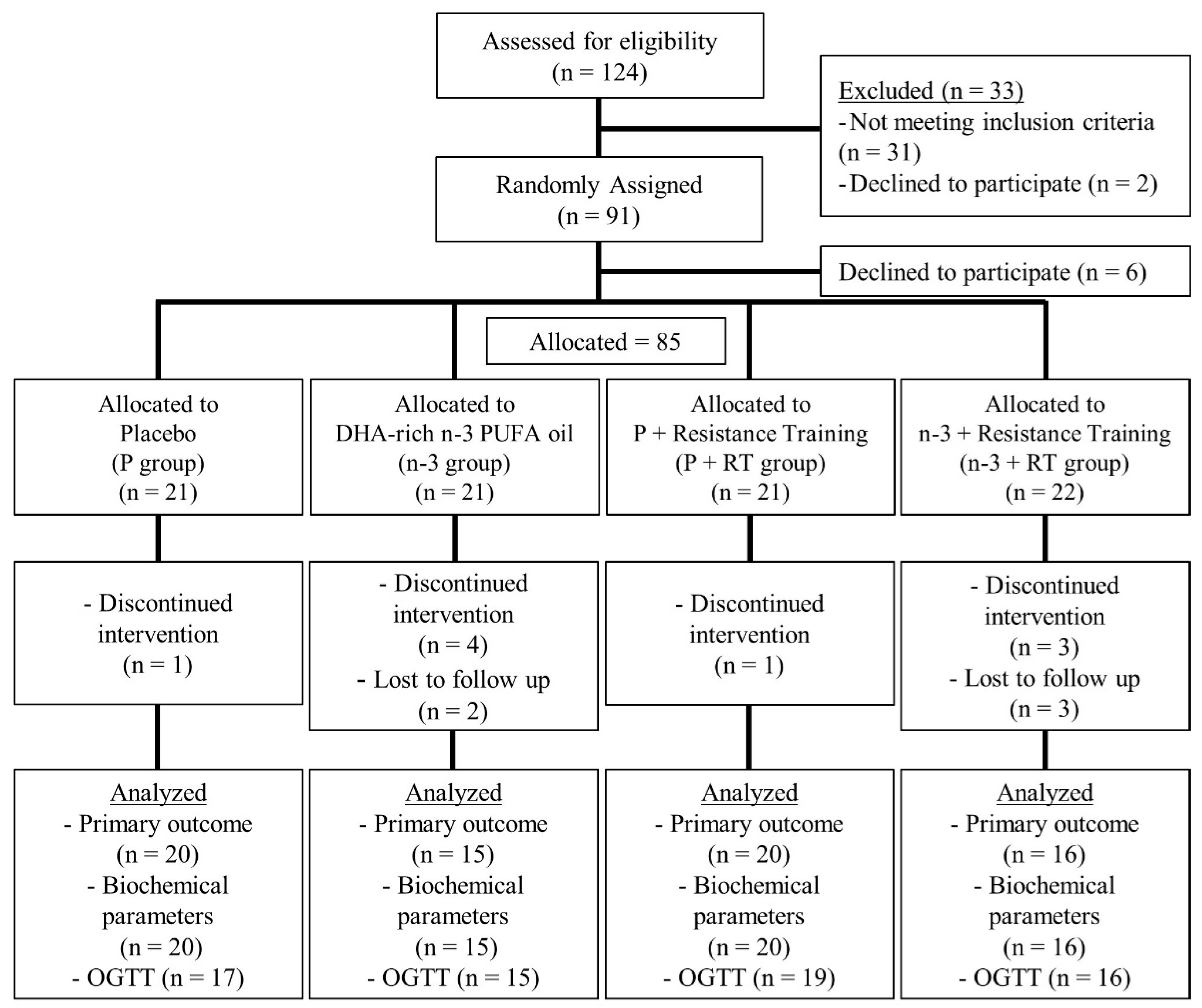
3.1. Basal Characteristics and Flowchart of the Participants
3.2. Effects on Whole Body Composition and Anthropometric Measurements
3.3. Effects on Segmented Body Composition and Anthropometric Measurements
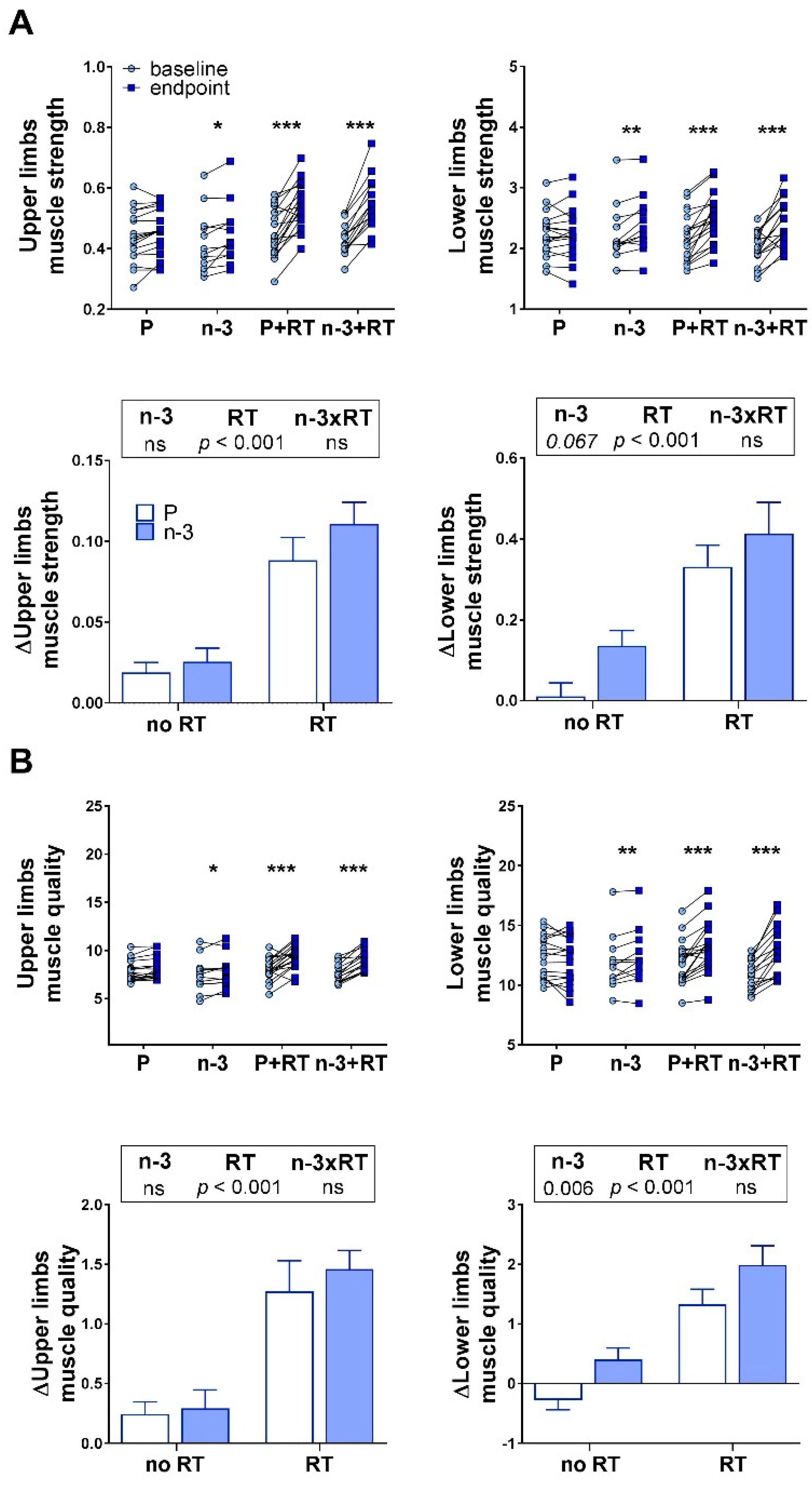
3.4. Effects on Muscle Strength and Quality
3.5. Effects on Blood Pressure and Lipid Metabolism Biomarkers
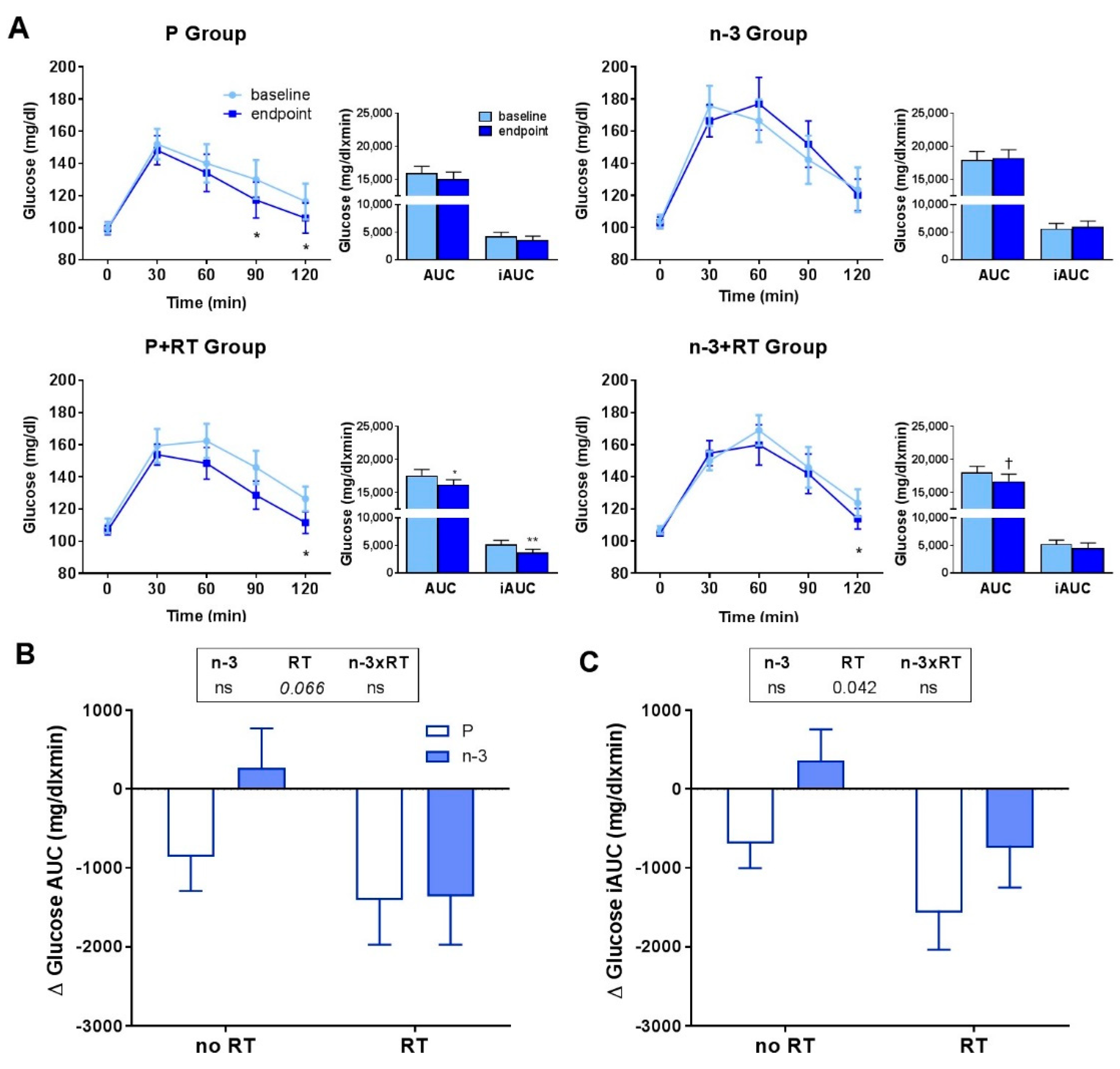
3.6. Effects on Serum Glucose Metabolism Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gold, E.B. The Timing of the Age at Which Natural Menopause Occurs. Obstet. Gynecol. Clin. 2011, 38, 425–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Liu, L.; Song, F.; Song, Y.; Dai, H. Ages at Menarche and Menopause, and Mortality among Postmenopausal Women. Maturitas 2019, 130, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Polotsky, H.N.; Polotsky, A.J. Metabolic Implications of Menopause. Semin. Reprod. Med. 2010, 28, 426–434. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F. Epidemiology of Gender Differences in Diabetes and Obesity. Adv. Exp. Med. Biol. 2017, 1043, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.S.; Islam, S.; Rosengren, A.; Franzosi, M.G.; Steyn, K.; Yusufali, A.H.; Keltai, M.; Diaz, R.; Rangarajan, S.; Yusuf, S. Risk Factors for Myocardial Infarction in Women and Men: Insights from the INTERHEART Study. Eur. Heart J. 2008, 29, 932–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Safi, Z.A.; Polotsky, A.J. Obesity and Menopause. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 548–553. [Google Scholar] [CrossRef]
- Elhakeem, A.; Cooper, R.; Whincup, P.; Brage, S.; Kuh, D.; Hardy, R. Physical Activity, Sedentary Time, and Cardiovascular Disease Biomarkers at Age 60 to 64 Years. J. Am. Heart Assoc. 2018, 7, e007459. [Google Scholar] [CrossRef]
- Peterson, M.D.; Sen, A.; Gordon, P.M. Influence of Resistance Exercise on Lean Body Mass in Aging Adults: A Meta-Analysis. Med. Sci. Sports Exerc. 2011, 43, 249–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caserotti, P.; Aagaard, P.; Buttrup Larsen, J.; Puggaard, L. Explosive Heavy-Resistance Training in Old and Very Old Adults: Changes in Rapid Muscle Force, Strength and Power. Scand. J. Med. Sci. Sports 2008, 18, 773–782. [Google Scholar] [CrossRef]
- Zhao, R.; Zhao, M.; Xu, Z. The Effects of Differing Resistance Training Modes on the Preservation of Bone Mineral Density in Postmenopausal Women: A Meta-Analysis. Osteoporos. Int. 2015, 26, 1605–1618. [Google Scholar] [CrossRef]
- Häkkinen, K.; Pakarinen, A.; Kraemer, W.J.; Newton, R.U.; Alen, M. Basal Concentrations and Acute Responses of Serum Hormones and Strength Development during Heavy Resistance Training in Middle-Aged and Elderly Men and Women. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, B95–B105. [Google Scholar] [CrossRef] [Green Version]
- Hanson, E.D.; Srivatsan, S.R.; Agrawal, S.; Menon, K.S.; Delmonico, M.J.; Wang, M.Q.; Hurley, B.F. Effects of Strength Training on Physical Function: Influence of Power, Strength, and Body Composition. J. Strength Cond. Res. 2010, 23, 2627–2637. [Google Scholar] [CrossRef] [Green Version]
- Ryan, A.S.; Hurlbut, D.E.; Lott, M.E.; Ivey, F.M.; Fleg, J.; Hurley, B.F.; Goldberg, A.P. Insulin Action after Resistive Training in Insulin Resistant Older Men and Women. J. Am. Geriatr. Soc. 2001, 49, 247–253. [Google Scholar] [CrossRef]
- Davidson, L.E.; Hudson, R.; Kilpatrick, K.; Kuk, J.L.; McMillan, K.; Janiszewski, P.M.; Lee, S.; Lam, M.; Ross, R. Effects of Exercise Modality on Insulin Resistance and Functional Limitation in Older Adults: A Randomized Controlled Trial. Arch. Intern. Med. 2009, 169, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Cornelissen, V.A.; Fagard, R.H.; Coeckelberghs, E.; Vanhees, L. Impact of Resistance Training on Blood Pressure and Other Cardiovascular Risk Factors: A Meta-Analysis of Randomized, Controlled Trials. Hypertension 2011, 58, 950–958. [Google Scholar] [CrossRef]
- Da Cunha Nascimento, D.; da Silva, C.R.; Valduga, R.; Saraiva, B.; de Sousa Neto, I.V.; Vieira, A.; Funghetto, S.S.; Silva, A.O.; da Cunha Oliveira, S.; Borges Pereira, G.; et al. Blood Pressure Response to Resistance Training in Hypertensive and Normotensive Older Women. Clin. Interv. Aging 2018, 13, 541–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wooten, J.S.; Phillips, M.D.; Mitchell, J.B.; Patrizi, R.; Pleasant, R.N.; Hein, R.M.; Menzies, R.D.; Barbee, J.J. Resistance Exercise and Lipoproteins in Postmenopausal Women. Int. J. Sports Med. 2011, 32, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, A.S.; Tomeleri, C.M.; Souza, M.F.; Pina, F.L.C.; Schoenfeld, B.J.; Nascimento, M.A.; Venturini, D.; Barbosa, D.S.; Cyrino, E.S. Effect of Resistance Training on C-Reactive Protein, Blood Glucose and Lipid Profile in Older Women with Differing Levels of RT Experience. Age 2015, 37, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahtiainen, J.P.; Sallinen, J.; Häkkinen, K.; Sillanpää, E. Inter-Individual Variation in Response to Resistance Training in Cardiometabolic Health Indicators. Scand. J. Med. Sci. Sports 2020, 30, 1040–1053. [Google Scholar] [CrossRef]
- Botero, J.P.; Shiguemoto, G.E.; Prestes, J.; Marin, C.T.; Do Prado, W.L.; Pontes, C.S.; Guerra, R.L.; Ferreia, F.C.; Baldissera, V.; Perez, S.E. Effects of Long-Term Periodized Resistance Training on Body Composition, Leptin, Resistin and Muscle Strength in Elderly Post-Menopausal Women. J. Sports Med. Phys. Fit. 2013, 53, 1460. [Google Scholar]
- Sillanpää, E.; Laaksonen, D.E.; Häkkinen, A.; Karavirta, L.; Jensen, B.; Kraemer, W.J.; Nyman, K.; Häkkinen, K. Body Composition, Fitness, and Metabolic Health during Strength and Endurance Training and Their Combination in Middle-Aged and Older Women. Eur. J. Appl. Physiol. 2009, 106, 285–296. [Google Scholar] [CrossRef]
- Lalia, A.Z.; Dasari, S.; Robinson, M.M.; Abid, H.; Morse, D.M.; Klaus, K.A.; Lanza, I.R. Influence of Omega-3 Fatty Acids on Skeletal Muscle Protein Metabolism and Mitochondrial Bioenergetics in Older Adults. Aging 2017, 9, 1096–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strandberg, E.; Ponsot, E.; Piehl-Aulin, K.; Falk, G.; Kadi, F. Resistance Training Alone or Combined with N-3 PUFA-Rich Diet in Older Women: Effects on Muscle Fiber Hypertrophy. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Da Boit, M.; Sibson, R.; Sivasubramaniam, S.; Meakin, J.R.; Greig, C.A.; Aspden, R.M.; Thies, F.; Jeromson, S.; Hamilton, D.L.; Speakman, J.R.; et al. Sex Differences in the Effect of Fish-Oil Supplementation on the Adaptive Response to Resistance Exercise Training in Older People: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2017, 105, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Strandberg, E.; Edholm, P.; Ponsot, E.; Wåhlin-Larsson, B.; Hellmén, E.; Nilsson, A.; Engfeldt, P.; Cederholm, T.; Risérus, U.; Kadi, F. Influence of Combined Resistance Training and Healthy Diet on Muscle Mass in Healthy Elderly Women: A Randomized Controlled Trial. J. Appl. Physiol. 2015, 119, 918–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodacki, C.L.N.; Rodacki, A.L.F.; Pereira, G.; Naliwaiko, K.; Coelho, I.; Pequito, D.; Fernandes, L.C. Fish-Oil Supplementation Enhances the Effects of Strength Training in Elderly Women. Am. J. Clin. Nutr. 2012, 95, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Lorente-Cebrián, S.; Costa, A.G.V.; Navas-Carretero, S.; Zabala, M.; Alfredo Martínez, J.; Moreno-Aliaga, M.J. Role of Omega-3 Fatty Acids in Obesity, Metabolic Syndrome, and Cardiovascular Diseases: A Review of the Evidence. J. Physiol. Biochem. 2013, 69, 633–651. [Google Scholar] [CrossRef]
- Zhuang, P.; Lu, Y.; Shou, Q.; Mao, L.; He, L.; Wang, J.; Chen, J.; Zhang, Y.; Jiao, J. Differential Anti-Adipogenic Effects of Eicosapentaenoic and Docosahexaenoic Acids in Obesity. Mol. Nutr. Food Res. 2019, 63, e1801135. [Google Scholar] [CrossRef]
- Erkkilä, A.T.; Matthan, N.R.; Herrington, D.M.; Lichtenstein, A.H. Higher Plasma Docosahexaenoic Acid Is Associated with Reduced Progression of Coronary Atherosclerosis in Women with CAD. J. Lipid Res. 2006, 47, 2814–2819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, Y.; Paik, M.J.; Kim, K.R.; Ko, Y.G.; Kang, E.S.; Cha, B.S.; Lee, H.C.; Lim, S.K. Plasma Free Fatty Acid Level Patterns According to Cardiovascular Risk Status in Postmenopausal Women. Clin. Chim. Acta 2008, 392, 11–16. [Google Scholar] [CrossRef]
- Woodman, R.J.; Mori, T.A.; Burke, V.; Puddey, I.B.; Barden, A.; Watts, G.F.; Beilin, L.J. Effects of Purified Eicosapentaenoic Acid and Docosahexaenoic Acid on Platelet, Fibrinolytic and Vascular Function in Hypertensive Type 2 Diabetic Patients. Atherosclerosis 2003, 166, 85–93. [Google Scholar] [CrossRef]
- Sparkes, C.; Gibson, R.; Sinclair, A.; Else, P.L.; Meyer, B.J. Effect of Low Dose Docosahexaenoic Acid-Rich Fish Oil on Plasma Lipids and Lipoproteins in Pre-Menopausal Women: A Dose-Response Randomized Placebo-Controlled Trial. Nutrients 2018, 10, 1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, M.D.; Sanders, T.A.B.; Davies, I.G.; Morgan, L.M.; Millward, D.J.; Lewis, F.; Slaughter, S.; Cooper, J.A.; Miller, G.J.; Griffin, B.A. Effects of Altering the Ratio of Dietary N-6 to n-3 Fatty Acids on Insulin Sensitivity, Lipoprotein Size, and Postprandial Lipemia in Men and Postmenopausal Women Aged 45–70 y: The OPTILIP Study. Am. J. Clin. Nutr. 2006, 84, 1290–1298. [Google Scholar] [CrossRef] [Green Version]
- AbuMweis, S.; Jew, S.; Tayyem, R.; Agraib, L. Eicosapentaenoic Acid and Docosahexaenoic Acid Containing Supplements Modulate Risk Factors for Cardiovascular Disease: A Meta-Analysis of Randomised Placebo-Control Human Clinical Trials. J. Hum. Nutr. Diet. 2018, 31, 67–84. [Google Scholar] [CrossRef]
- Gao, H.; Geng, T.; Huang, T.; Zhao, Q. Fish Oil Supplementation and Insulin Sensitivity: A Systematic Review and Meta-Analysis. Lipids Health Dis. 2017, 16, 131. [Google Scholar] [CrossRef] [Green Version]
- Akinkuolie, A.O.; Ngwa, J.S.; Meigs, J.B.; Djoussé, L. Omega-3 Polyunsaturated Fatty Acid and Insulin Sensitivity: A Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. 2011, 30, 702–707. [Google Scholar] [CrossRef] [Green Version]
- Bender, N.; Portmann, M.; Heg, Z.; Hofmann, K.; Zwahlen, M.; Egger, M. Fish or N3-PUFA Intake and Body Composition: A Systematic Review and Meta-Analysis. Obes. Rev. 2014, 15, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.J.; Kim, T.H.; Byun, D.W.; Park, Y. Positive correlation between erythrocyte levels of n-3 polyunsaturated fatty acids and bone mass in postmenopausal Korean women with osteoporosis. Ann. Nutr. Metab. 2012, 60, 146–153. [Google Scholar] [CrossRef]
- Cook, R.J.; Dickens, B.M.; Fathalla, M.F. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. In Reproductive Health and Human Rights: Integrating Medicine, Ethics, and Law; Clarendon Press: Oxford, UK, 2003. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Men, Ageing and Health: Achieving Health across the Life Span; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; WHO: Geneva, Switzerland, 2000; pp. 1–253. [Google Scholar]
- Huerta, A.E.; Prieto-Hontoria, P.L.; Fernández-Galilea, M.; Sáinz, N.; Cuervo, M.; Martínez, J.A.; Moreno-Aliaga, M.J. Circulating Irisin and Glucose Metabolism in Overweight/Obese Women: Effects of α-Lipoic Acid and Eicosapentaenoic Acid. J. Physiol. Biochem. 2015, 71, 547–558. [Google Scholar] [CrossRef]
- Aranceta Bartrina, J.; Arija Val, V.V.; Maíz Aldalur, E.; Martínez de Victoria Muñoz, E.; Ortega Anta, R.M.; Pérez-Rodrigo, C.; Quiles Izquierdo, J.; Rodríguez Martín, A.; Román Viñas, B.; Salvador Castell, G.; et al. Dietary Guidelines for the Spanish Population (SENC, Diciembre 2016); the New Graphic Icon of Healthy Food. Nutr. Hosp. 2016, 33, e95581. [Google Scholar] [CrossRef] [Green Version]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De La Fuente-Arrillaga, C.; Vázquez Ruiz, Z.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ Validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish Version of the Physical Activity Questionnaire Used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Munro, I.A.; Garg, M.L. Prior Supplementation with Long Chain Omega-3 Polyunsaturated Fatty Acids Promotes Weight Loss in Obese Adults: A Double-Blinded Randomised Controlled Trial. Food Funct. 2013, 4, 650–658. [Google Scholar] [CrossRef]
- Munro, I.A.; Garg, M.L. Dietary Supplementation with Long Chain Omega-3 Polyunsaturated Fatty Acids and Weight Loss in Obese Adults. Obes. Res. Clin. Pract. 2013, 7, e173–e181. [Google Scholar] [CrossRef]
- Munro, I.A.; Garg, M.L. Dietary Supplementation with N-3 PUFA Does Not Promote Weight Loss When Combined with a Very-Low-Energy Diet. Br. J. Nutr. 2012, 108, 1466–1474. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food and Drug Administration (FDA). Qualified Health Claims: Letters of Enforcement Discretion. Omega-3 Fatty Acids and Reduced Risk of Coronary Heart Disease (Martek Petition). Available online: https://www.fda.gov/food/food-labeling-nutrition/qualified-health-claims-letters-enforcement-discretion (accessed on 23 November 2020).
- Mataix-Verdú, J.; Mañas Almendros, M.; Llopis González, J.; Martínez de Victoria, E. Tablas de Composición de Alimentos; Universidad de Granada: Granada, Spain, 1993. [Google Scholar]
- EFSA Panel on Dietetict Products, Nutrition and Allergies (NDA). Scientific Opinion on the Tolerable Upper Intake Level of Eicosapentaenoic Acid (EPA), Docosahexaenoic Acid (DHA) and Docosapentaenoic Acid (DPA). EFSA J. 2012, 10, 2815. [Google Scholar] [CrossRef]
- Ansorena, D.; Echarte, A.; Ollé, R.; Astiasarán, I. 2012: No Trans Fatty Acids in Spanish Bakery Products. Food Chem. 2013, 138, 422–429. [Google Scholar] [CrossRef]
- Ibañez, J.; Izquierdo, M.; Argüelles, I.; Forga, L.; Larrión, J.L.; García-Unciti, M.; Idoate, F.; Gorostiaga, E.M. Twice-Weekly Progressive Resistance Training Decreases Abdominal Fat and Improves Insulin Sensitivity in Older Men with Type 2 Diabetes. Diabetes Care 2005, 28, 662–667. [Google Scholar] [CrossRef] [Green Version]
- Ibáñez, J.; Gorostiaga, E.M.; Alonso, A.M.; Forga, L.; Argüelles, I.; Larrión, J.L.; Izquierdo, M. Lower Muscle Strength Gains in Older Men with Type 2 Diabetes after Resistance Training. J. Diabetes Complicat. 2008, 22, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Cuff, D.J.; Meneilly, G.S.; Martin, A.; Ignaszewski, A.; Tildesley, H.D.; Frohlich, J.J. Effective Exercise Modality to Reduce Insulin Resistance in Women with Type 2 Diabetes. Diabetes Care 2003, 26, 2977–2982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Sports Medicine. Progression Models in Resistance Training for Healthy Adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef] [PubMed]
- Pina, F.L.C.; Nunes, J.P.; Nascimento, M.A.; Ribeiro, A.S.; Mayhew, J.L.; Cyrino, E.S. Similar Effects of 24 Weeks of Resistance Training Performed with Different Frequencies on Muscle Strength, Muscle Mass, and Muscle Quality in Older Women. Int. J. Exerc. Sci. 2019, 12, 623–635. [Google Scholar]
- Huerta, A.E.; Navas-Carretero, S.; Prieto-Hontoria, P.L.; Martínez, J.A.; Moreno-Aliaga, M.J. Effects of α-Lipoic Acid and Eicosapentaenoic Acid in Overweight and Obese Women during Weight Loss. Obesity 2015, 23, 313–321. [Google Scholar] [CrossRef]
- Abe, T.; Thiebaud, R.S.; Loenneke, J.P.; Young, K.C. Prediction and Validation of DXA-Derived Appendicular Lean Soft Tissue Mass by Ultrasound in Older Adults. Age 2015, 37, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midorikawa, T.; Ohta, M.; Torii, S.; Sakamoto, S. Lean Soft Tissue Mass Measured Using Dual-Energy X-Ray Absorptiometry Is an Effective Index for Assessing Change in Leg Skeletal Muscle Mass Following Exercise Training. J. Clin. Densitom. 2018, 21, 394–398. [Google Scholar] [CrossRef]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; de Ridder, H. International Standards for Anthropometric Assessment; ISAK: Lower Hutt, New Zealand, 2011; ISBN 9780620362078. [Google Scholar]
- Hill, A.M.; Buckley, J.D.; Murphy, K.J.; Howe, P.R.C. Combining Fish-Oil Supplements with Regular Aerobic Exercise Improves Body Composition and Cardiovascular Disease Risk Factors. Am. J. Clin. Nutr. 2007, 85, 1267–1274. [Google Scholar] [CrossRef] [Green Version]
- DeFina, L.F.; Marcoux, L.G.; Devers, S.M.; Cleaver, J.P.; Willis, B.L. Effects of Omega-3 Supplementation in Combination with Diet and Exercise on Weight Loss and Body Composition. Am. J. Clin. Nutr. 2011, 93, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Zamora Zamora, F.; Miguel Martínez Galiano, J.; Juan Gaforio Martínez, J.; Delgado Rodríguez, M. Olive Oil and Body Weight. Systematic Review and Meta-Analysis of Randomized Controlled Trials. Rev. Esp. Salud Pública 2018, 92, e201811083. [Google Scholar]
- Hunter, G.R.; Bryan, D.R.; Wetzstein, C.J.; Zuckerman, P.A.; Bamman, M.M. Resistance Training and Intra-Abdominal Adipose Tissue in Older Men and Women. Med. Sci. Sports Exerc. 2002, 34, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Ihalainen, J.K.; Inglis, A.; Mäkinen, T.; Newton, R.U.; Kainulainen, H.; Kyröläinen, H.; Walker, S. Strength Training Improves Metabolic Health Markers in Older Individual Regardless of Training Frequency. Front. Physiol. 2019, 10, 32. [Google Scholar] [CrossRef] [Green Version]
- Phillips, B.E.; Williams, J.P.; Greenhaff, P.L.; Smith, K.; Atherton, P.J. Physiological Adaptations to Resistance Exercise as a Function of Age. JCI Insight 2017, 2, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomeleri, C.M.; Ribeiro, A.S.; Souza, M.F.; Schiavoni, D.; Schoenfeld, B.J.; Venturini, D.; Barbosa, D.S.; Landucci, K.; Sardinha, L.B.; Cyrino, E.S. Resistance Training Improves Inflammatory Level, Lipid and Glycemic Profiles in Obese Older Women: A Randomized Controlled Trial. Exp. Gerontol. 2016, 84, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.S.; Schoenfeld, B.J.; Souza, M.F.; Tomeleri, C.M.; Venturini, D.; Barbosa, D.S.; Cyrino, E.S. Traditional and Pyramidal Resistance Training Systems Improve Muscle Quality and Metabolic Biomarkers in Older Women: A Randomized Crossover Study. Exp. Gerontol. 2016, 79, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Sardeli, A.V.; Tomeleri, C.M.; Cyrino, E.S.; Fernhall, B.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.T. Effect of Resistance Training on Inflammatory Markers of Older Adults: A Meta-Analysis. Exp. Gerontol. 2018, 111, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.D.; Patrizi, R.M.; Cheek, D.J.; Wooten, J.S.; Barbee, J.J.; Mitchell, J.B. Resistance Training Reduces Subclinical Inflammation in Obese, Postmenopausal Women. Med. Sci. Sports Exerc. 2012, 44, 2099–2110. [Google Scholar] [CrossRef] [Green Version]
- Churchward-Venne, T.A.; Tieland, M.; Verdijk, L.B.; Leenders, M.; Dirks, M.L.; de Groot, L.C.P.G.M.; van Loon, L.J.C. There Are No Nonresponders to Resistance-Type Exercise Training in Older Men and Women. J. Am. Med. Dir. Assoc. 2015, 16, 400–411. [Google Scholar] [CrossRef]
- Howe, T.; Shea, B.; Dawson, L.J.; Downie, F.; Murray, A.; Ross, C.; Harbour, R.; Caldwell, L.; Creed, G. Exercise for Preventing and Treating Osteoporosis in Postmenopausal Women (Review). Cochrane Database Syst. Rev. 2011, 7, CD000333. [Google Scholar] [CrossRef]
- Curtis, E.M.; Harvey, N.C.; D’Angelo, S.; Cooper, C.S.; Ward, K.A.; Taylor, P.; Pearson, G.; Cooper, C. Bone Mineral Content and Areal Density, but Not Bone Area, Predict an Incident Fracture Risk: A Comparative Study in a UK Prospective Cohort. Arch. Osteoporos. 2016, 11, 39. [Google Scholar] [CrossRef] [Green Version]
- Mosti, M.P.; Kaehler, N.; Stunes, A.K.; Hoff, J.; Syversen, U. Maximal Strength Training in Postmenopausal Women with Osteoporosis or Osteopenia. J. Strength Cond. Res. 2013, 27, 2879–2886. [Google Scholar] [CrossRef]
- Watson, S.L.; Weeks, B.K.; Weis, L.J.; Harding, A.T.; Horan, S.A.; Beck, B.R. High-Intensity Resistance and Impact Training Improves Bone Mineral Density and Physical Function in Postmenopausal Women with Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial. J. Bone Miner. Res. 2018, 33, 211–220. [Google Scholar] [CrossRef]
- Holzer, G.; Von Skrbensky, G.; Holzer, L.A.; Pichl, W. Hip Fractures and the Contribution of Cortical versus Trabecular Bone to Femoral Neck Strength. J. Bone Miner. Res. 2009, 24, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.T.; Li, X.D.; Wang, W.Z.; Zhang, J.G.; Yang, D.Z. Efficacy of Weight Adjusted Bone Mineral Content in Osteoporosis Diagnosis in Chinese Female Population. Chin. Med. J. 2019, 132, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. Dietary omega-3 fatty acid supplementation increases the rate of muscle protein synthesis in older adults: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 93, 402–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, G.; Sun, Q.; Hu, F.B.; Ye, X.; Yu, Z.; Zong, G.; Li, H.; Zhou, Y.; Lin, X. Erythrocyte N-3 Fatty Acids and Metabolic Syndrome in Middle-Aged and Older Chinese. J. Clin. Endocrinol. Metab. 2012, 97, E973–E977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howe, P.R.C.; Evans, H.M.; Kuszewski, J.C.; Wong, R.H.X. Effects of Long Chain Omega-3 Polyunsaturated Fatty Acids on Brain Function in Mildly Hypertensive Older Adults. Nutrients 2018, 10, 1413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.Y.; Liu, W.; Zhao, T.Y.; Tian, H.M. Efficacy of Omega-3 Polyunsaturated Fatty Acids Supplementation in Managing Overweight and Obesity: A Meta-Analysis of Randomized Clinical Trials. J. Nutr. Health Aging 2017, 21, 187–192. [Google Scholar] [CrossRef]
- Bassan, R. Cardiovascular Changes and Cardiac Morbidity of Menopause. Effects of Hormone Replacement Therapy. Arq. Bras. Cardiol. 1999, 72, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Costa, R.R.; Buttelli, A.C.K.; Vieira, A.F.; Coconcelli, L.; De Lima Magalhães, R.; Delevatti, R.S.; Kruel, L.F.M. Effect of Strength Training on Lipid and Inflammatory Outcomes: Systematic Review with Meta-Analysis and Meta-Regression. J. Phys. Act. Health 2019, 16, 477–491. [Google Scholar] [CrossRef]
- Marques, E.; Carvalho, J.; Soares, J.M.C.; Marques, F.; Mota, J. Effects of Resistance and Multicomponent Exercise on Lipid Profiles of Older Women. Maturitas 2009, 63, 84–88. [Google Scholar] [CrossRef]
- De Siqueria Mendes Barbalho, M.; Gentil, P.; Izquierdo, M.; Fisher, J.; Steele, J.; de Azevedo Raiol, R. There Are No No-Responders to Low or High Resistance Training Volumes among Older Women. Exp. Gerontol. 2017, 99, 18–26. [Google Scholar] [CrossRef]
- Cunha, P.M.; Tomeleri, C.M.; Nascimento, M.A.; Mayhew, J.L.; Fungari, E.; Trindade, L.; Barbosa, D.S.; Venturini, D.; Cyrino, E.S. Comparision of Low and High Volume of Resistance Training on Body Fat and Blood Biomarkers in Untrained Older Women: A Randomized Clinical Trial. J. Strength Cond. Res. 2019, 35, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, E.S.; Asano, R.Y.; Filho, I.G.; Lopes, N.L.; Panelli, P.; Nascimento, D.d.C.; Collier, S.R.; Prestes, J. Acute and Chronic Cardiovascular Response to 16 Weeks of Combined Eccentric or Traditional Resistance and Aerobic Training in Elderly Hypertensive Women: A Randomized Controlled Trial. J. Strength Cond. Res. 2014, 28, 3073–3084. [Google Scholar] [CrossRef] [PubMed]
- Spolador de Alencar Silva, B.; Santos Lira, F.; Eduardo Rossi, F.; Conrado de Freitas, M.; Paula Coelho Figueira Freire, A.; Ribeiro dos Santos, V.; Alberto Gobbo, L. Elastic Resistance Training Improved Glycemic Homeostasis, Strength, and Functionality in Sarcopenic Older Adults: A Pilot Study. J. Exerc. Rehabil. 2018, 14, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Slentz, C.A.; Bateman, L.A.; Willis, L.H.; Shields, A.T.; Tanner, C.J.; Piner, L.W.; Hawk, V.H.; Muehlbauer, M.J.; Samsa, G.P.; Nelson, R.C.; et al. Effects of Aerobic vs. Resistance Training on Visceral and Liver Fat Stores, Liver Enzymes, and Insulin Resistance by HOMA in Overweight Adults from STRRIDE AT/RT. Am. J. Physiol. Endocrinol. Metab. 2011, 301, 1033–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.C.; Ang, R.P.; Fung, D.S. Something Fishy: The Issue of Omega-3 Blinding in Psychiatric Clinical Trials. Aust. N. Z. J. Psychiatry 2013, 47, 201–205. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| P | n-3 | P+RT | n-3+RT | Two-Way ANOVA c | |||
|---|---|---|---|---|---|---|---|
| N | 20 | 15 | 20 | 16 | n-3 | RT | n-3xRT |
| Age (years) | 58.75 ± 3.39 | 58.00 ± 2.78 | 58.95 ± 3.46 | 58.13 ± 3.14 | |||
| Weight (kg) | |||||||
| Baseline | 76.75 ± 4.99 | 80.34 ± 8.51 | 77.76 ± 7.92 | 80.57 ± 6.60 | |||
| Change | −2.66 ± 2.95 a,*** | −2.65 ± 2.47 a,** | −2.21 ± 2.39 a,*** | −2.70 ± 3.49 a,** | ns | ns | ns |
| BMI (kg/m2) | |||||||
| Baseline | 30.25 ± 2.30 | 30.39 ± 1.94 | 30.79 ± 2.34 | 31.07 ± 1.82 | |||
| Change | −1.07 ± 1.16 b,** | −1.03 ± 0.94 a,*** | −0.90 ± 0.94 a,*** | −1.06 ± 1.34 a,** | ns | ns | ns |
| Fat mass (%) | |||||||
| Baseline | 47.44 ± 3.42 | 45.55 ± 2.38 | 47.05 ± 3.96 | 46.70 ± 2.90 | |||
| Change | −2.27 ± 1.14 a,*** | −1.58 ± 1.34 a,*** | −1.77 ± 1.50 a,*** | −2.12 ± 2.40 a,** | ns | ns | ns |
| Visceral fat (kg) | |||||||
| Baseline | 1.30 ± 0.44 | 1.37 ± 0.44 | 1.27 ± 0.51 | 1.18 ± 0.47 | |||
| Change | −0.20 ± 0.19 a,*** | −0.11 ± 0.14 a,** | −0.11 ± 0.18 b,* | −0.12 ± 0.23 a,† | ns | ns | ns |
| Adjusted change d | −0.20(0.04) a,*** | −0.11(0.02) a,*** | −0.12(0.03) b,** | −0.12(0.03) a,** | ns | ns | ns |
| Lean mass (%) | |||||||
| Baseline | 49.76± 3.20 | 51.52 ± 2.18 | 50.16 ± 3.78 | 50.53 ± 2.76 | |||
| Change | 2.21 ± 1.08 a,*** | 1.49 ± 1.26 a,*** | 1.70 ± 1.43 a,*** | 2.01 ± 2.34 a,** | ns | ns | ns |
| BMC (g) | |||||||
| Baseline | 2152.65 ± 308.05 | 2366.33 ± 332.76 | 2156.10 ± 231.21 | 2240.31 ± 258.36 | |||
| Change | −27.60 ± 17.36 *** | −17.53 ± 20.22 b,** | 1.40 ± 30.33 | −1.38 ± 32.81 | ns | 0.001 | ns |
| Adjusted change d | −25.95(4.19) *** | −17.50(5.08) b,** | −2.08(6.63) | −1.26(7.10) | ns | p < 0.001 | ns |
| Waist circumference (cm) | |||||||
| Baseline | 93.11 ± 4.57 | 95.00 ± 7.63 | 92.67 ± 5.47 | 93.90 ± 7.16 | |||
| Change | −3.45 ± 2.62 a,*** | −3.15 ± 2.94 a,** | −3.01 ± 1.80 a,*** | −4.04 ± 3.73 a,*** | ns | ns | ns |
| Adjusted change d | −3.35(0.26) a,*** | −3.18(0.65) a,*** | −3.08(0.38) b,*** | −4.03(0.62) a,*** | ns | ns | ns |
| Hip circumference (cm) | |||||||
| Baseline | 110.68 ± 7.14 | 112.50 ± 5.78 | 110.65 ± 5.74 | 113.35 ± 6.82 | |||
| Change | −2.40 ± 2.97 a,** | −3.00 ± 3.12 a,** | −3.17 ± 4.99 a,* | −3.06 ± 3.52 a,** | ns | ns | ns |
| Adjusted change d | −2.42(0.37) a,*** | −2.87(0.57) a,*** | −3.33(1.17) a,* | −2.89(0.91) a,** | ns | ns | ns |
| Waist/hip ratio | |||||||
| Baseline | 0.84 ± 0.04 | 0.85 ± 0.06 | 0.84 ± 0.06 | 0.83 ± 0.08 | |||
| Change | −0.01 ± 0.01 a,*** | −0.01 ± 0.01 a,* | −0.00 ± 0.04 | −0.02 ± 0.03 | ns | ns | ns |
| Adjusted change d | −0.01(0.00) a,** | −0.01(0.00) | −0.00(0.01) | −0.02(0.01) a,* | ns | ns | ns |
| P | n-3 | P+RT | n-3+RT | Two-Way ANOVA c | |||
|---|---|---|---|---|---|---|---|
| N | 20 | 15 | 20 | 16 | n-3 | RT | n-3xRT |
| Arms weight (kg) | |||||||
| Baseline | 8.65 ± 0.89 | 8.60 ± 1.17 | 8.73 ± 1.21 | 8.83 ± 1.04 | |||
| Change | −0.37 ± 0.40 a,*** | −0.33 ± 0.42 a,** | −0.13 ± 0.40 | 0.01 ± 0.60 | ns | 0.010 | ns |
| Adjusted change d | −0.38(0.07) a,*** | −0.32(0.11) a,* | −0.15(0.09) | 0.02(0.11) | ns | 0.003 | ns |
| Arms fat mass (kg) | |||||||
| Baseline | 4.36 ± 0.60 | 4.01 ± 0.68 | 4.32 ± 0.68 | 4.24 ± 0.71 | |||
| Change | −0.33 ± 0.27 a,*** | −0.24 ± 0.24 b,** | −0.22 ± 0.28 a,** | −0.11 ± 0.41 | ns | ns | ns |
| Adjusted change d | −0.34(0.04) a,*** | −0.23(0.06) a,** | −0.24(0.05) a,*** | −0.10(0.07) | 0.041 | ns | ns |
| Arms lean mass (kg) | |||||||
| Baseline | 4.02 ± 0.56 | 4.30 ± 0.60 | 4.13 ± 0.66 | 4.29 ± 0.47 | |||
| Change | −0.04 ± 0.18 | −0.09 ± 0.22 | 0.09 ± 0.19 a,† | 0.13 ± 0.30 | ns | 0.002 | ns |
| Adjusted change d | −0.05(0.04) | −0.09(0.06) | 0.09(0.04) a,† | 0.13(0.07) a,† | ns | 0.002 | ns |
| Legs weight (kg) | |||||||
| Baseline | 25.10 ± 3.59 | 27.52 ± 3.28 | 26.55 ± 3.91 | 27.11 ± 3.95 | |||
| Change | −0.60 ± 1.79 b,† | −0.91 ± 0.97 a,** | −0.95 ± 1.12 a,** | −0.98 ± 1.45 a,* | ns | ns | ns |
| Adjusted change d | −0.51(0.22) b,** | −0.86(0.10) a,*** | −1.08(0.22) a,*** | −0.91(0.10) a,*** | ns | ns | ns |
| Legs fat mass (kg) | |||||||
| Baseline | 11.29 ± 2.58 | 12.16 ± 2.38 | 12.36 ± 2.88 | 12.18 ± 2.47 | |||
| Change | −0.62 ± 0.90 b,** | −0.73 ± 0.66 a,*** | −0.96 ± 0.73 a,*** | −0.97 ± 1.02 a,** | ns | ns | ns |
| Adjusted change d | −0.60(0.12) b,** | −0.70(0.08) a,*** | −1.02(0.14) a,*** | −0.92(0.12) a,*** | ns | 0.005 | ns |
| Legs lean mass (kg) | |||||||
| Baseline | 13.03 ± 1.57 | 14.51 ± 1.66 | 13.40 ± 1.64 | 14.11 ± 1.88 | |||
| Change | 0.02 ± 0.98 | −0.16 ± 0.50 | 0.02 ± 0.57 | 0.02 ± 0.63 | ns | ns | ns |
| Adjusted change d | 0.01(0.14) | −0.15(0.10) | −0.05(0.13) | 0.03(0.99) | ns | ns | ns |
| Thigh circumference (cm) | |||||||
| Baseline | 56.42 ± 4.54 | 56.75 ± 3.48 | 59.71 ± 5.21 | 60.42 ± 6.42 | |||
| Change | −1.49 ± 1.75 b,** | −0.84 ± 1.18 a,* | −2.38 ± 3.00 a,** | −1.50 ± 2.52 a,* | ns | ns | ns |
| Adjusted change d | −1.07(0.24) b,** | −0.91(0.40) a,* | −2.71(0.57) a,*** | −1.60(0.56) a,* | ns | ns | ns |
| Calf circumference (cm) | |||||||
| Baseline | 38.05 ± 2.12 | 39.59 ± 2.58 | 40.15 ± 2.41 | 39.30 ± 2.55 | |||
| Change | −0.32 ± 0.54 a,* | −0.39 ± 0.67 a,* | −0.81 ± 0.78 b,*** | −0.68 ± 0.69 a,** | ns | 0.017 | ns |
| Adjusted change d | −0.26(0.09) a,* | −0.38(0.15) b,* | −0.85(0.19) a,*** | −0.68(0.13) a,*** | ns | 0.005 | ns |
| Thigh skinfold (mm) | |||||||
| Baseline | 39.92 ± 4.76 | 41.25 ± 5.49 | 42.67 ± 2.99 | 41.06 ± 5.37 | |||
| Change | 0.43 ± 3.36 | −1.23 ± 2.28 b,* | −3.43 ± 3.15 a,*** | −5.19 ± 7.61 b,** | ns | p< 0.001 | ns |
| Adjusted change d | −0.28(0.61) | −0.70(0.54) b,* | −3.31(0.66) a,*** | −4.64(1.92) b,* | ns | p< 0.001 | ns |
| Calf skinfold (mm) | |||||||
| Baseline | 31.07 ± 5.28 | 32.02 ± 5.60 | 33.26 ± 4.88 | 34.76 ± 5.45 | |||
| Change | −1.26 ± 3.65 | −2.51 ± 3.05 a,** | −5.17 ± 4.63 a,*** | −7.73 ± 7.40 b,** | ns | p< 0.001 | ns |
| Adjusted change d | −1.46(0.70) a,† | −2.25(0.80) a,* | −5.05(1.92) a,*** | −7.44(1.82) b,** | ns | p< 0.001 | ns |
| P | n-3 | P+RT | n-3+RT | Two-Way ANOVA c | |||
|---|---|---|---|---|---|---|---|
| N | 20 | 15 | 20 | 16 | n-3 | RT | n-3xRT |
| SBP (mm Hg) | |||||||
| Baseline | 121.83 ± 19.68 | 119.18 ± 7.98 | 122.73 ± 14.96 | 123.67 ± 9.01 | ns | ns | ns |
| Change | −2.40 ± 10.84 | 0.20 ± 10.96 | −1.22 ± 14.45 | −6.00 ± 11.79 | ns | ns | ns |
| DBP (mm Hg) | |||||||
| Baseline | 80.04 ± 12.38 | 79.71 ± 6.05 | 79.08 ± 7.88 | 81.62 ± 6.67 | ns | ns | ns |
| Change | −1.40 ± 7.13 | −2.09 ± 6.97 | 1.83 ± 7.05 | −4.94 ± 7.70 a,* | 0.035 | ns | ns |
| TG (mg/dL) | |||||||
| Baseline | 92.64 ± 29.47 | 118.20 ± 55.31 | 110.90 ± 51.66 | 101.34 ± 33.26 | |||
| Change | 1.94 ± 26.29 | −28.87 ± 52.97 b,* | −17.10 ± 23.78 b,* | −18.88 ± 28.73 b,* | 0.047 | ns | ns |
| Adjusted change d | 2.99(6.14) | −22.09(7.34) a,** | −13.98(4.02) a,** | −20.75(5.06) a,** | 0.038 | ns | ns |
| Total Chol (mg/dL) | |||||||
| Baseline | 237.40 ± 30.79 | 239.73 ± 46.41 | 254.50 ± 27.83 | 250.31 ± 45.89 | |||
| Change | −8.10 ± 25.20 | −9.00 ± 44.86 | −21.45 ± 24.34 b,** | −14.41 ± 43.32 | ns | ns | ns |
| Adjusted change d | −12.66(4.87) a,* | −12.66(8.06) | −17.42(3.83) a,*** | −10.41(8.62) | ns | ns | ns |
| LDL−Chol (mg/dL) | |||||||
| Baseline | 153.31 ± 32.65 | 154.20 ± 36.89 | 168.40 ± 24.49 | 164.90 ± 44.04 | |||
| Change | −6.98 ± 19.29 | −4.22 ± 35.87 | −14.20 ± 23.09 b,** | −8.14 ± 38.54 | ns | ns | ns |
| Adjusted change d | −10.46(3.65) a,* | −7.79(7.47) | −10.69(3.95) a,* | −5.29(7.60) | ns | ns | ns |
| HDL−Chol (mg/dL) | |||||||
| Baseline | 65.74 ± 16.77 | 61.89 ± 16.38 | 63.92 ± 14.61 | 65.15 ± 11.03 | |||
| Change | −0.55 ± 9.45 | −0.99 ± 13.97 | −3.83 ± 8.32 a,† | −2.50 ± 9.46 | ns | ns | ns |
| Adjusted change d | −0.08(1.70) | −0.07(2.68) | −4.35(1.83) a,* | −1.63(2.08) | ns | ns | ns |
| Glucose (mg/dL) | |||||||
| Baseline | 98.57 ± 13.03 | 103.90 ± 15.72 | 109.14 ± 18.90 | 108.35 ± 11.32 | |||
| Change | −1.83 ± 9.22 | −0.86 ± 11.87 | −3.59 ± 20.78 | −4.73 ± 9.36 a,† | ns | ns | ns |
| Adjusted change d | −3.60(2.82) | −2.53(2.67) | −1.33(1.52) | −3.83(1.52) a,* | ns | ns | ns |
| Insulin (mU/L) | |||||||
| Baseline | 10.02 ± 4.41 | 9.90 ± 5.21 | 9.49 ± 5.00 | 10.54 ± 4.05 | |||
| Change | −2.63 ± 3.91 b,* | −0.84 ± 2.75 | −1.35 ± 4.03 | −1.96 ± 2.76 b,* | ns | ns | ns |
| Adjusted change d | −2.28(0.63) a,** | −1.01(0.75) | −1.83(0.63) a,** | −1.75(0.49) a,* | ns | ns | ns |
| HOMA−IR index | |||||||
| Baseline | 2.51 ± 1.43 | 2.48 ± 1.19 | 2.67 ± 1.86 | 2.82 ± 1.14 | |||
| Change | −0.71 ± 1.05 b,* | −0.23 ± 0.87 | −0.54 ± 1.52 | −0.60 ± 0.74 b,** | ns | ns | ns |
| Adjusted change d | −0.63(0.15) a,*** | −0.40(0.21) a,† | −0.56(0.17) a,** | −0.53(0.13) a,** | ns | ns | ns |
| TyG index | |||||||
| Baseline | 8.45 ± 0.45 | 8.64 ± 0.41 | 8.64 ± 0.47 | 8.59 ± 0.39 | |||
| Change | −0.05 ± 0.31 | −0.15 ± 0.37 | −0.17 ± 0.27 a,* | −0.23 ± 0.33 a,* | ns | ns | ns |
| Adjusted change d | −0.08(0.07) | −0.13(0.09) | −0.16(0.06) a,* | −0.22(0.06) a,** | ns | ns | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Félix-Soriano, E.; Martínez-Gayo, A.; Cobo, M.J.; Pérez-Chávez, A.; Ibáñez-Santos, J.; Palacios Samper, N.; Goikoetxea Galarza, I.; Cuervo, M.; García-Unciti, M.; González-Muniesa, P.; et al. Effects of DHA-Rich n-3 Fatty Acid Supplementation and/or Resistance Training on Body Composition and Cardiometabolic Biomarkers in Overweight and Obese Post-Menopausal Women. Nutrients 2021, 13, 2465. https://doi.org/10.3390/nu13072465
Félix-Soriano E, Martínez-Gayo A, Cobo MJ, Pérez-Chávez A, Ibáñez-Santos J, Palacios Samper N, Goikoetxea Galarza I, Cuervo M, García-Unciti M, González-Muniesa P, et al. Effects of DHA-Rich n-3 Fatty Acid Supplementation and/or Resistance Training on Body Composition and Cardiometabolic Biomarkers in Overweight and Obese Post-Menopausal Women. Nutrients. 2021; 13(7):2465. https://doi.org/10.3390/nu13072465
Chicago/Turabian StyleFélix-Soriano, Elisa, Alejandro Martínez-Gayo, María José Cobo, Adriana Pérez-Chávez, Javier Ibáñez-Santos, Natalia Palacios Samper, Iñaki Goikoetxea Galarza, Marta Cuervo, Marisol García-Unciti, Pedro González-Muniesa, and et al. 2021. "Effects of DHA-Rich n-3 Fatty Acid Supplementation and/or Resistance Training on Body Composition and Cardiometabolic Biomarkers in Overweight and Obese Post-Menopausal Women" Nutrients 13, no. 7: 2465. https://doi.org/10.3390/nu13072465
APA StyleFélix-Soriano, E., Martínez-Gayo, A., Cobo, M. J., Pérez-Chávez, A., Ibáñez-Santos, J., Palacios Samper, N., Goikoetxea Galarza, I., Cuervo, M., García-Unciti, M., González-Muniesa, P., Lorente-Cebrián, S., & Moreno-Aliaga, M. J. (2021). Effects of DHA-Rich n-3 Fatty Acid Supplementation and/or Resistance Training on Body Composition and Cardiometabolic Biomarkers in Overweight and Obese Post-Menopausal Women. Nutrients, 13(7), 2465. https://doi.org/10.3390/nu13072465