
Eating Behaviors of Children with Autism—Pilot Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
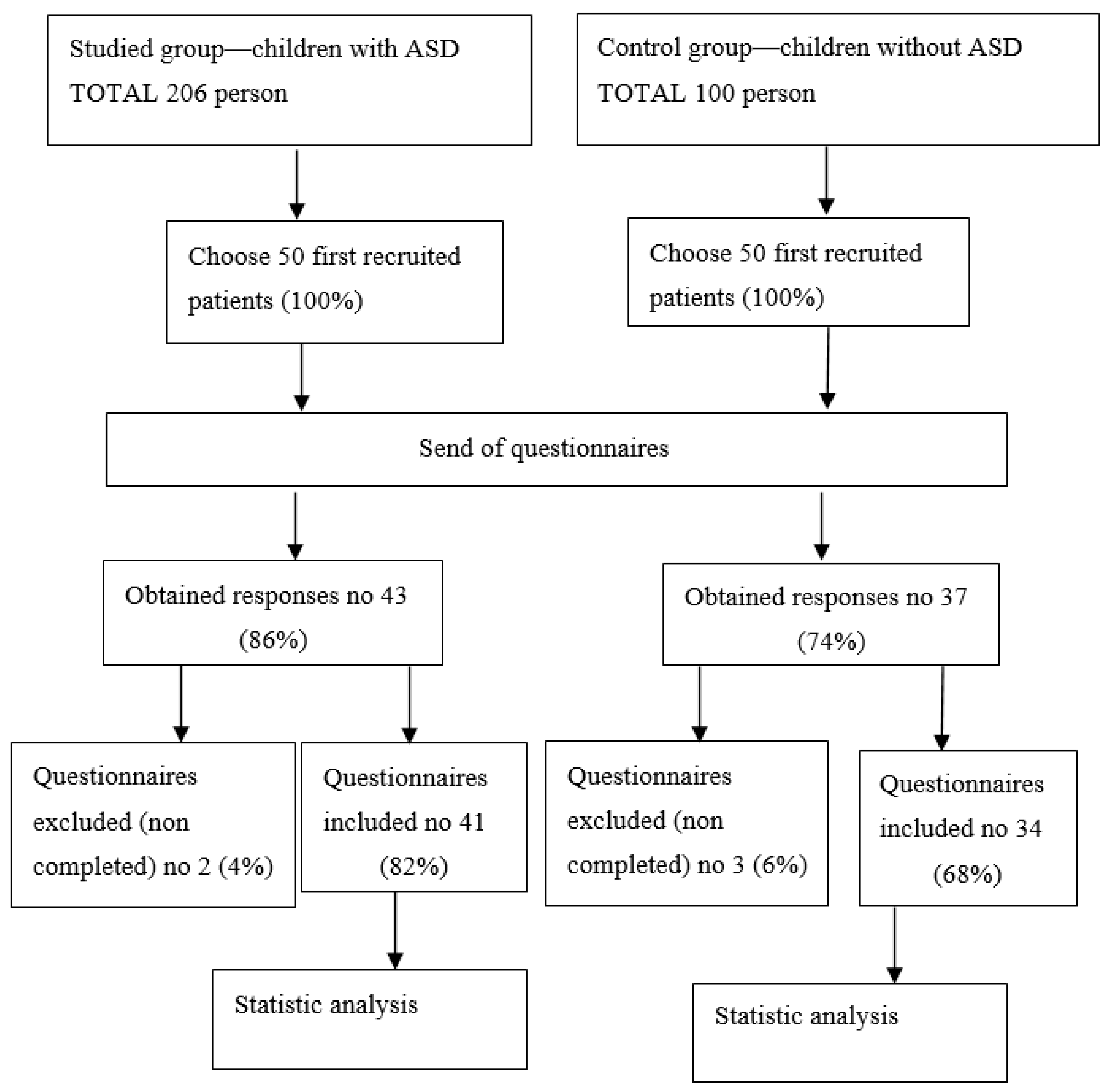
2.1. The Characteristic of the Studied Group
- Informed and voluntary consent of the child’s parent/legal guardian to participate in the study
- Children aged between 2 and 12 years
- Diagnosis made by an ASD psychiatrist (using gold diagnostic test—ADOS-2)
- Syndromic autism (additionally diagnosed mental disorder, epilepsy, congenital disorder, genetic disorder).
- Mental retardation
2.2. The Characteristic of the Control Group
- Informed and voluntary consent of the child’s parent/legal guardian to participate in the study
- Children aged between 2 and 12 years
- Absence of pervasive developmental disorder (as confirmed by a child and adolescent psychiatrist, child neurologist, psychologist and educational research scientist)
- Absence of any diagnosis of chronic conditions with the potential of affecting the nutritional status (the digestive tract diseases previously diagnosed)
- Children younger than 2 years and older than 12 years
- Mental retardation
2.3. Study Method
2.4. Statistical Methods
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| ICD-10 | International Classification of Disease-10, |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders-5, |
| ADOS-2 | Autism Diagnostic Observation Schedule, Second Edition, |
| CDCP | Centers for Disease Control and Prevention, |
| ASD | Autism Spectrum Disorder. |
References
- Onaolapo, A.Y.; Onaolapo, O.J. Global Data on Autism Spectrum Disorders Prevalence: A Review of Facts, Fallacies and Limitations. Univers. J. Clin. Med. 2017, 5, 14–23. [Google Scholar] [CrossRef]
- CDC Data and Statistics on Autism Spectrum Disorder|CDC. Available online: https://www.cdc.gov/ncbddd/autism/data.html (accessed on 20 June 2021).
- Lyall, K.; Croen, L.; Daniels, J.; Fallin, M.D.; Ladd-Acosta, C.; Lee, B.K.; Park, B.Y.; Snyder, N.W.; Schendel, D.; Volk, H.; et al. The Changing Epidemiology of Autism Spectrum Disorders. Annu. Rev. Public Health 2017, 38, 81–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivanov, H.Y.; Stoyanova, V.K.; Popov, N.T.; Vachev, T.I. Autism Spectrum Disorder—A Complex Genetic Disorder. Folia Med. 2015, 57, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Ristori, M.V.; Quagliariello, A.; Reddel, S.; Ianiro, G.; Vicari, S.; Gasbarrini, A.; Putignani, L. Autism, Gastrointestinal Symptoms and Modulation of Gut Microbiota by Nutritional Interventions. Nutrients 2019, 11, 2812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buie, T.; Campbell, D.B.; Fuchs, G.J.; Furuta, G.T.; Levy, J.; Vandewater, J.; Whitaker, A.H.; Atkins, D.; Bauman, M.L.; Beaudet, A.L.; et al. Evaluation, diagnosis, and treatment of gastrointestinal disorders in individuals with ASDs: A consensus report. Pediatrics 2010, 125, S1–S18. [Google Scholar] [CrossRef] [Green Version]
- Leader, G.; Tuohy, E.; Chen, J.L.; Mannion, A.; Gilroy, S.P. Feeding Problems, Gastrointestinal Symptoms, Challenging Behavior and Sensory Issues in Children and Adolescents with Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 1401–1410. [Google Scholar] [CrossRef]
- van’t Hof, M.; Ester, W.A.; van Berckelaer-Onnes, I.; Hillegers, M.H.J.; Hoek, H.W.; Jansen, P.W. Do early-life eating habits predict later autistic traits? Results from a population-based study. Appetite 2021, 156, 104976. [Google Scholar] [CrossRef]
- Scarpato, E.; Kolacek, S.; Jojkic-Pavkov, D.; Konjik, V.; Živković, N.; Roman, E.; Kostovski, A.; Zdraveska, N.; Altamimi, E.; Papadopoulou, A.; et al. Prevalence of Functional Gastrointestinal Disorders in Children and Adolescents in the Mediterranean Region of Europe. Clin. Gastroenterol. Hepatol. 2018, 16, 870–876. [Google Scholar] [CrossRef] [Green Version]
- Saps, M.; Nichols-Vinueza, D.X.; Rosen, J.M.; Velasco-Benítez, C.A. Prevalence of functional gastrointestinal disorders in Colombian school children. J. Pediatr. 2014, 164, 542–545. [Google Scholar] [CrossRef]
- Fabian, M.; Widera, E.; Kazek, B.; Kaniewska, A.; Paprocka, J. The Prenatal and Perinatal Risk Variables of the Sensory Processing Disorder. Clin. Mother Child. Health 2018, 15, 1. [Google Scholar] [CrossRef]
- Gomez, I.N.B.; Calsa, A.P.; Esguerra, J.T.; Penetrante, P.J.H.; Porlucas, K.; Santos, M.E.; Umali, C.B.; Lai, C.Y.Y. Psychometric Properties of the Sensory Processing and Self-Regulation Checklist: English Version. Occup. Ther. Int. 2021, 2021, 6658786. [Google Scholar] [CrossRef] [PubMed]
- Valicenti-McDermott, M.; McVicar, K.; Rapin, I.; Wershil, B.K.; Cohen, H.; Shinnar, S. Frequency of gastrointestinal symptoms in children with autistic spectrum disorders and association with family history of autoimmune disease. J. Dev. Behav. Pediatr. 2006, 27, S128–S136. [Google Scholar] [CrossRef] [PubMed]
- Cermak, S.A.; Curtin, C.; Bandini, L.G. Food selectivity and sensory sensitivity in children with autism spectrum disorders. J. Am. Diet. Assoc. 2010, 110, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Marco, E.J.; Hinkley, L.B.N.; Hill, S.S.; Nagarajan, S.S. Sensory processing in autism: A review of neurophysiologic findings. Pediatr. Res. 2011, 69, 48R–54R. [Google Scholar] [CrossRef]
- Volkert, V.M.; Vaz, P.C.M. Recent Studies on Feeding Problems in Children with Autism. J. Appl. Behav. Anal. 2010, 43, 155–159. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, L.; Heiss, C.; Campbell, E. A Comparison of Nutrient Intake and Eating Behaviors of Boys with and without Autism. Top. Clin. Nutr. 2008, 23, 23–31. [Google Scholar] [CrossRef]
- Viviers, M.; Jongh, M.; Dickonson, L.; Malan, R.; Pike, T. Parent-reported feeding and swallowing difficulties of children with Autism Spectrum Disorders (aged 3 to 5 years) compared to typically developing peers: A South African study. Afr. Health Sci. 2020, 20, 524–532. [Google Scholar] [CrossRef]
- Darling, J.C.; Bamidis, P.D.; Burberry, J.; Rudolf, M.C.J. The First Thousand Days: Early, integrated and evidence-based approaches to improving child health: Coming to a population near you? Arch. Dis. Child. 2020, 105, 837–841. [Google Scholar] [CrossRef]
- Rogers, S.L.; Blissett, J. Infant temperament, maternal feeding behaviours and the timing of solid food introduction. Matern. Child. Nutr. 2019, 15, e12771. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- Mosca, F.; Giannì, M.L. Human milk: Composition and health benefits. Pediatr. Med. Chir. 2017, 39, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Academies of Sciences, E. Feeding Infants and Children from Birth to 24 Months: Summarizing Existing Guidance; Mathematica Policy Research: Princeton, NJ, USA, 2020; ISBN 978-0-309-67538-3. [Google Scholar]
- Smith, H.A.; Becker, G.E. Early additional food and fluids for healthy breastfed full-term infants. Cochrane Database Syst. Rev. 2016, 96, 14651858. [Google Scholar] [CrossRef] [PubMed]
- Spill, M.K.; Johns, K.; Callahan, E.H.; Shapiro, M.J.; Wong, Y.P.; Benjamin-Neelon, S.E.; Birch, L.; Black, M.M.; Cook, J.T.; Faith, M.S.; et al. Repeated exposure to food and food acceptability in infants and toddlers: A systematic review. Am. J. Clin. Nutr. 2019, 109, 978S–989S. [Google Scholar] [CrossRef]
- Bzikowska, A.; Czerwonogrodzka-Senczyna, A.; Wesołowska, A.; Weker, H. Nutrition during breastfeeding—Impact on human milk composition. Pol. Merkur. Lek. 2017, 43, 276–280. [Google Scholar]
- Beckerman, J.P.; Slade, E.; Ventura, A.K. Maternal diet during lactation and breast-feeding practices have synergistic association with child diet at 6 years. Public Health Nutr. 2020, 23, 286–294. [Google Scholar] [CrossRef]
- Keen, D.V. Childhood autism, feeding problems and failure to thrive in early infancy. Seven case studies. Eur. Child. Adolesc. Psychiatry 2008, 17, 209–216. [Google Scholar] [CrossRef] [PubMed]
- De Cosmi, V.; Scaglioni, S.; Agostoni, C. Early Taste Experiences and Later Food Choices. Nutrients 2017, 9, 107. [Google Scholar] [CrossRef] [Green Version]
- Pearson, N.; Biddle, S.J.H.; Griffiths, P.; Johnston, J.P.; Haycraft, E. Clustering and correlates of screen-time and eating behaviours among young children. BMC Public Health 2018, 18, 753. [Google Scholar] [CrossRef]
- Tseng, P.-T.; Chen, Y.-W.; Stubbs, B.; Carvalho, A.F.; Whiteley, P.; Tang, C.-H.; Yang, W.-C.; Chen, T.-Y.; Li, D.-J.; Chu, C.-S.; et al. Maternal breastfeeding and autism spectrum disorder in children: A systematic review and meta-analysis. Nutr. Neurosci. 2019, 22, 354–362. [Google Scholar] [CrossRef]
- Mizuno, K.; Ueda, A. The maturation and coordination of sucking, swallowing, and respiration in preterm infants. J. Pediatrics 2003, 142, 36–40. [Google Scholar] [CrossRef]
- da Costa, S.P.; van den Engel-Hoek, L.; Bos, A.F. Sucking and swallowing in infants and diagnostic tools. J. Perinatol. 2008, 28, 247–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoyre, S.M.; Shaker, C.S.; Pridham, K.F. The early feeding skills assessment for preterm infants. Neonatal. Netw. 2005, 24, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Mennella, J.A.; Nicklaus, S.; Jagolino, A.L.; Yourshaw, L.M. Variety is the spice of life: Strategies for promoting fruit and vegetable acceptance during infancy. Physiol. Behav. 2008, 94, 29–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forestell, C.A.; Mennella, J.A. Early determinants of fruit and vegetable acceptance. Pediatrics 2007, 120, 1247–1254. [Google Scholar] [CrossRef] [Green Version]
- Benton, D. Role of parents in the determination of the food preferences of children and the development of obesity. Int. J. Obes. 2004, 28, 858–869. [Google Scholar] [CrossRef] [Green Version]
- Gerrish, C.J.; Mennella, J.A. Flavor variety enhances food acceptance in formula-fed infants. Am. J. Clin. Nutr. 2001, 73, 1080–1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinello, A.; Di Gangi, V.; Valenza, E. Persistent primary reflexes affect motor acts: Potential implications for autism spectrum disorder. Res. Dev. Disabil. 2018, 83, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.G.; Russell, A. “Food” and “non-food” self-regulation in childhood: A review and reciprocal analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Gisel, E.G. Effect of food texture on the development of chewing of children between six months and two years of age. Dev. Med. Child. Neurol. 1991, 33, 69–79. [Google Scholar] [CrossRef]
- Lewis, L.; Povey, R.; Rose, S.; Cowap, L.; Semper, H.; Carey, A.; Bishop, J.; Clark-Carter, D. What behavior change techniques are associated with effective interventions to reduce screen time in 0–5 year olds? A narrative systematic review. Prev. Med. Rep. 2021, 23, 101429. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sex | Study Group (n = 41; 100%) | Control Group (n = 34; 100%) | Fisher Exact Probability Test |
|---|---|---|---|
| Female | 13 (31.7%) | 8 (23.5%) | NS (p = 0.30) |
| Male | 28 (68.3%) | 26 (76.5%) |
| Age [in Years] | Study Group (n = 41; 100%) | Control Group (n = 34; 100%) | Chi-Square Test for Association with Yates Continuity Correction |
|---|---|---|---|
| From 3 to 7 | 18 (43.9%) | 16 (47.1%) | NS (p = 0.73) |
| From 7 to 10 | 13 (31.7%) | 8 (23.5%) | |
| Above 10 | 10 (24.4%) | 10 (29.4%) |
| Problem | Study Group (n = 37; 100%) | Control Group (n = 33; 100%) | Fisher Exact Probability Test |
|---|---|---|---|
| Child’s difficulty to hold on to the breast | 5 (13.5%) | 5 (15.2%) | NS (p = 0.56) |
| Week sucking reflex | 4 (10.8%) | 1 (3.0%) | NS (p = 0.22) |
| Chaotic sucking (child’s crying, anxiety) | 3 (8.1%) | 1 (3.0%) | NS (p = 0.35) |
| Child getting tired during breastfeeding | 3 (8.1%) | 1 (3.0%) | NS (p = 0.35) |
| Short sucking time (child falls asleep) | 5 (13.5%) | 0 | p = 0.04 |
| Insufficient/absence of breast milk | 7 (18.9%) | 6 (18.2%) | NS (p = 0.59) |
| Poor weight gain | 3 (8.7%) | 2 (6.1%) | NS (p = 0.56) |
| Short lingual frenulum | 2 (5.4%) | 0 | NS (p = 0.28) |
| Regurgitation | 6 (16.2%) | 2 (6.1%) | NS (p = 0.17) |
| Problem with breast nipples (pain, infection) | 4 (10.8%) | 4 (12.1%) | NS (p = 0.58) |
| Problem with the mammary gland (infection, abscess) | 2 (5.4%) | 2 (6.1%) | NS (p = 0.65) |
| Mother’s illness | 0 | 2 (6.1%) | NS (p = 0.22) |
| Child’s illness | 1 (2.7%) | 2 (6.1%) | NS (p = 0.46) |
| Emotional problem of the mother | 0 | 2 (6.1%) | NS (p = 0.22) |
| Food | Study Group (n = 41) | Control Group (n = 34) | Mann-Whitney U Test |
|---|---|---|---|
| Vegetables | 1.6; 1.2; 1 | 1.3; 0.5w; 1 | NS (p = 0.10) |
| Fruit | 2.0; 1.0; 2 | 2.1; 1.2; 2 | NS (p = 0.58) |
| Meat | 3.8; 1.2; 3 | 3.6; 1.0; 3 | NS (p = 0.74) |
| Fish | 5.9; 1.6; 6 | 5.2; 1.6; 5 | NS (p = 0.14) |
| Wheat products | 4.4; 1.7; 5 | 4.3; 1.5; 4 | NS (p = 0.56) |
| Chicken egg yolk | 5.1; 1.7; 6 | 5.1; 1.1; 5 | NS (p = 0.64) |
| Whole chicken egg | 6.9; 1.2; 7 | 7.0; 0.7; 7 | NS (p = 0.61) |
| Dairy products—yogurt, Buttermilk | 6.3; 1.5; 6 | 7.4; 1.0; 8 | p = 0.001 |
| Necessity of Multiple Trials | Study Group (n = 41; 100%) | Control Group (n = 34; 100%) | Fisher Exact Probability Test |
|---|---|---|---|
| Yes | 19 (47.5%) | 6 (17.7%) | p = 0.006 |
| No | 21 (52.5%) | 28 (82.3%) |
| Food Type | Study Group (n = 41; 100%) | Control Group (n = 34; 100%) | Fisher Exact Probability Test |
|---|---|---|---|
| Ready, store-bought jarred baby food | 37 (90.2%) | 11 (70.6%) | p = 0.03 |
| Food prepared at home and designated solely for the child | 37 (90.2%) | 29 (85.3%) | NS (p = 0.38) |
| Food at the family table | 10 (24.4%) | 10 (29.4%) | NS (p = 0.41) |
| Child drinks only milk (breast milk/infant formula) | 0 | 0 | --- |
| Food Texture | Study Group (n = 41) | Control Group (n = 34) | Mann-Whitney U Test |
|---|---|---|---|
| Fluid, mushy | 6.2; 5.1; 6.0 | 5.6; 1.4; 5.5 | NS (p = 0.78) |
| Lumpy | 9.6; 6.5; 8.0 | 8.4; 4.2; 7.0 | p = 0.02 |
| Solid | 12.9; 10.1; 9.0 | 10.5; 4.3; 8.0 | p = 0.02 |
| Child’s Preferred Food Texture | Study Group (n = 41; 100%) | Control Group (n = 34; 100%) | Fisher Exact Probability Test |
|---|---|---|---|
| Fluid | 15 (36.6%) | 9 (26.5%) | NS (p = 0.25) |
| Lumpy | 4 (9.8%) | 13 (38.2%) | p = 0.004 |
| Solid | 2 (4.9%) | 3 (8.8%) | NS (p = 0.41) |
| Absence of any preference of food texture | 24 (58.5%) | 15 (44.1%) | NS (p = 0.16) |
| Accessory | Study Group (n = 41; 100%) | Control Group (n = 34; 100%) | Fisher Exact Probability Test |
|---|---|---|---|
| bottle with a nipple | 29 (70.7%) | 13 (38.2%) | p = 0.005 |
| tea spoon | 41 (100%) | 33 (97.1%) | NS (p = 0.45) |
| child’s hands | 23 (56.1%) | 29 (85.3%) | p = 0.006 |
| sippy cup | 28 (68.3%) | 28 (82.4%) | NS (p = 0.13) |
| regular cup | 16 (39.0%) | 16 (47.1%) | NS (p = 0.32) |
| Additional Involvement | Study Group (n = 41; 100%) | Control Group (n = 34; 100%) | Fisher Exact Probability Test |
|---|---|---|---|
| Yes | 17 (41.5%) | 7 (20.6%) | p = 0.05 |
| No | 24 (58.5%) | 27 (79.4%) |
| Child Watched a Cartoon | Study Group (n = 41; 100%) | Control Group (n = 34; 100%) | Fisher Exact Probability Test |
|---|---|---|---|
| Yes | 13 (31.7%) | 5 (14.7%) | NS (p = 0.07) |
| No | 28 (68.3%) | 29 (85.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brzóska, A.; Kazek, B.; Kozioł, K.; Kapinos-Gorczyca, A.; Ferlewicz, M.; Babraj, A.; Makosz-Raczek, A.; Likus, W.; Paprocka, J.; Matusik, P.; et al. Eating Behaviors of Children with Autism—Pilot Study. Nutrients 2021, 13, 2687. https://doi.org/10.3390/nu13082687
Brzóska A, Kazek B, Kozioł K, Kapinos-Gorczyca A, Ferlewicz M, Babraj A, Makosz-Raczek A, Likus W, Paprocka J, Matusik P, et al. Eating Behaviors of Children with Autism—Pilot Study. Nutrients. 2021; 13(8):2687. https://doi.org/10.3390/nu13082687
Chicago/Turabian StyleBrzóska, Anna, Beata Kazek, Karolina Kozioł, Agnieszka Kapinos-Gorczyca, Małgorzata Ferlewicz, Agnieszka Babraj, Anna Makosz-Raczek, Wirginia Likus, Justyna Paprocka, Paweł Matusik, and et al. 2021. "Eating Behaviors of Children with Autism—Pilot Study" Nutrients 13, no. 8: 2687. https://doi.org/10.3390/nu13082687
APA StyleBrzóska, A., Kazek, B., Kozioł, K., Kapinos-Gorczyca, A., Ferlewicz, M., Babraj, A., Makosz-Raczek, A., Likus, W., Paprocka, J., Matusik, P., & Emich-Widera, E. (2021). Eating Behaviors of Children with Autism—Pilot Study. Nutrients, 13(8), 2687. https://doi.org/10.3390/nu13082687