
Association of Walnut Consumption with Total and Cause-Specific Mortality and Life Expectancy in U.S. Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Assessment Using FFQ
2.3. Ascertainment of Total and Cause-Specific Deaths
2.4. Statistics
2.5. Estimation of Total Life Expectancy
3. Results
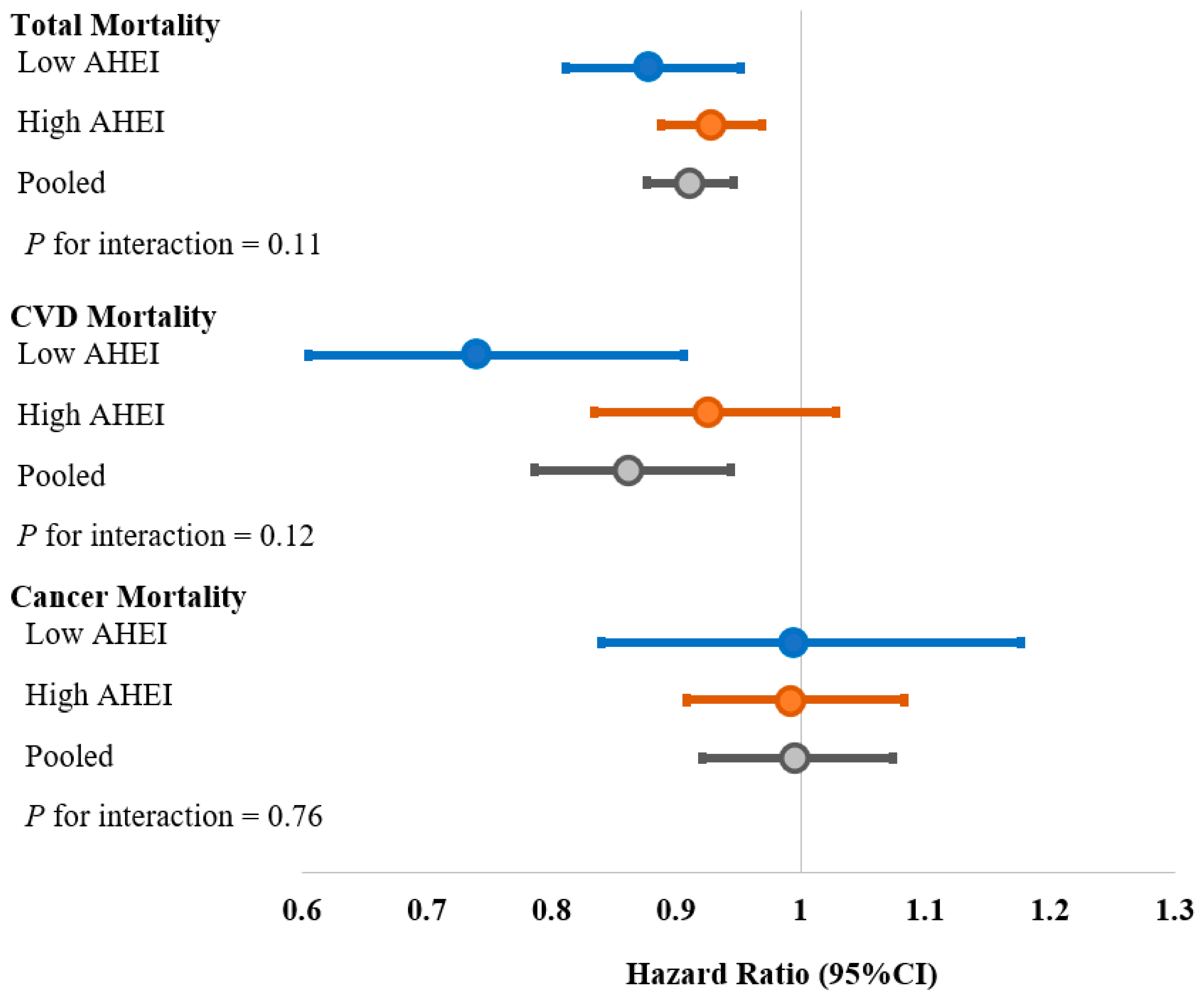
3.1. Walnut Consumption and Total Mortality
3.2. Walnut Consumption and Cause-Specific Mortality
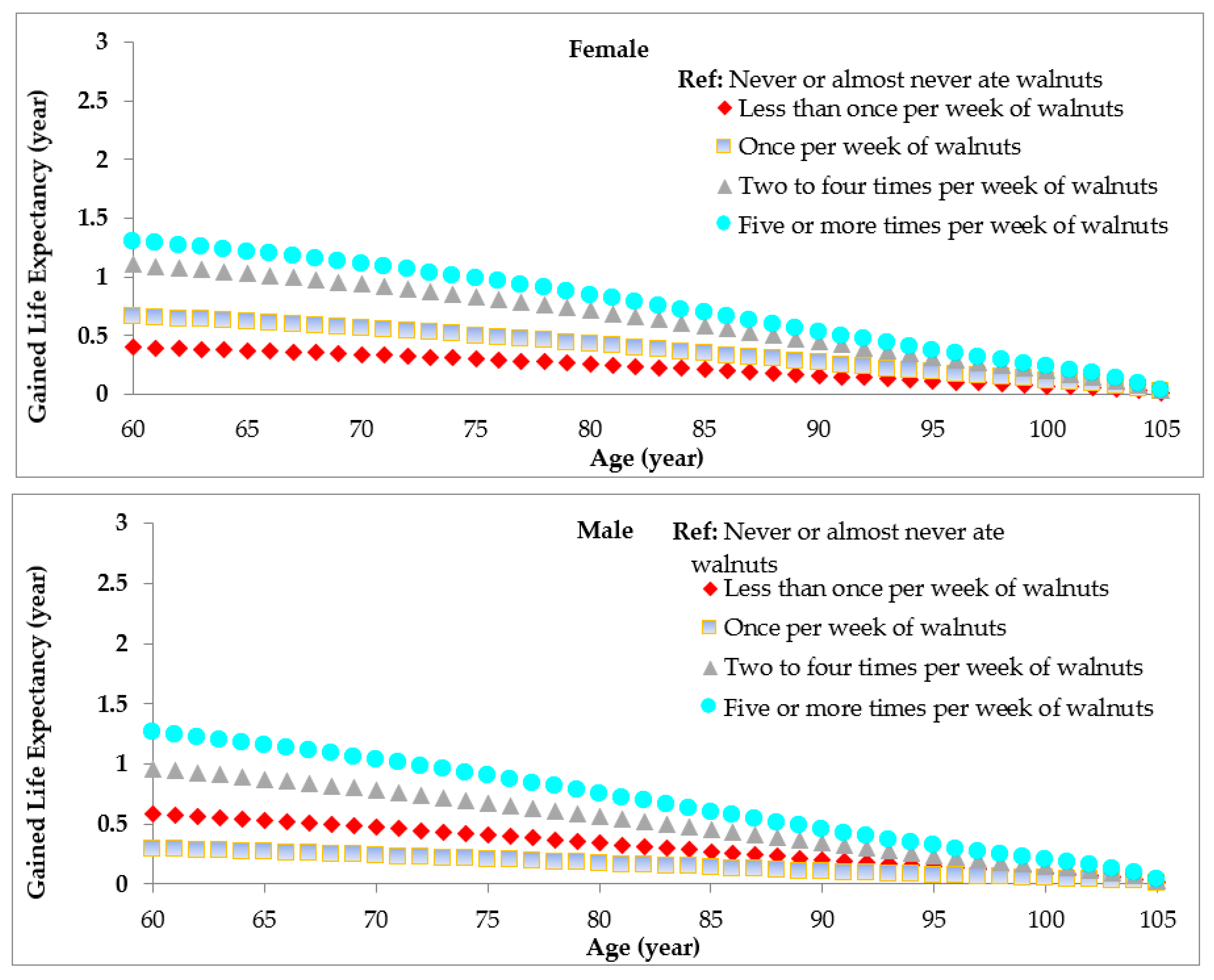
3.3. Walnut Consumption and Life Expectance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rehm, C.D.; Penalvo, J.L.; Afshin, A.; Mozaffarian, D. Dietary Intake among US Adults, 1999–2012. JAMA 2016, 315, 2542–2553. [Google Scholar] [CrossRef]
- Ros, E. Nuts and CVD. Br. J. Nutr. 2015, 113 (Suppl. 2), S111–S120. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferre, M.; Liu, X.; Malik, V.S.; Sun, Q.; Willett, W.C.; Manson, J.E.; Rexrode, K.M.; Li, Y.; Hu, F.B.; Bhupathiraju, S.N. Nut Consumption and Risk of Cardiovascular Disease. J. Am. Coll. Cardiol. 2017, 70, 2519–2532. [Google Scholar] [CrossRef]
- Afshin, A.; Micha, R.; Khatibzadeh, S.; Mozaffarian, D. Consumption of nuts and legumes and risk of incident ischemic heart disease, stroke, and diabetes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 278–288. [Google Scholar] [CrossRef]
- Liu, X.; Guasch-Ferré, M.; Drouin-Chartier, J.P.; Tobias, D.K.; Bhupathiraju, S.N.; Rexrode, K.M.; Willett, W.C.; Sun, Q.; Li, Y. Changes in Nut Consumption and Subsequent Cardiovascular Disease Risk Among US Men and Women: 3 Large Prospective Cohort Studies. J. Am. Heart Assoc. 2020, 9, e013877. [Google Scholar] [CrossRef]
- Bes-Rastrollo, M.; Wedick, N.M.; Martinez-Gonzalez, M.A.; Li, T.Y.; Sampson, L.; Hu, F.B. Prospective study of nut consumption, long-term weight change, and obesity risk in women. Am. J. Clin. Nutr. 2009, 89, 1913–1919. [Google Scholar] [CrossRef]
- Freisling, H.; Noh, H.; Slimani, N.; Chajes, V.; May, A.M.; Peeters, P.H.; Weiderpass, E.; Cross, A.J.; Skeie, G.; Jenab, M.; et al. Nut intake and 5-year changes in body weight and obesity risk in adults: Results from the EPIC-PANACEA study. Eur. J. Nutr. 2018, 57, 2399–2408. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Li, Y.; Tobias, D.K.; Wang, D.D.; Manson, J.E.; Willett, W.C.; Hu, F.B. Changes in Types of Dietary Fats Influence Long-term Weight Change in US Women and Men. J. Nutr. 2018, 148, 1821–1829. [Google Scholar] [CrossRef] [Green Version]
- Rehm, C.D.; Drewnowski, A. Replacing American snacks with tree nuts increases consumption of key nutrients among US children and adults: Results of an NHANES modeling study. Nutr. J. 2017, 16, 17. [Google Scholar] [CrossRef] [Green Version]
- Hepburn, F.N.; Exler, J.; Weihrauch, J.L. Provisional tables on the content of omega-3 fatty acids and other fat components of selected foods. J. Am. Diet. Assoc. 1986, 86, 788–793. [Google Scholar]
- Simopoulos, A.P. Essential fatty acids in health and chronic disease. Am. J. Clin. Nutr. 1999, 70, 560s–569s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guasch-Ferre, M.; Li, J.; Hu, F.B.; Salas-Salvado, J.; Tobias, D.K. Effects of walnut consumption on blood lipids and other cardiovascular risk factors: An updated meta-analysis and systematic review of controlled trials. Am. J. Clin. Nutr. 2018, 108, 174–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almario, R.U.; Vonghavaravat, V.; Wong, R.; Kasim-Karakas, S.E. Effects of walnut consumption on plasma fatty acids and lipoproteins in combined hyperlipidemia. Am. J. Clin. Nutr. 2001, 74, 72–79. [Google Scholar] [CrossRef]
- Xiao, Y.; Huang, W.; Peng, C.; Zhang, J.; Wong, C.; Kim, J.H.; Yeoh, E.K.; Su, X. Effect of nut consumption on vascular endothelial function: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2018, 37, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Njike, V.Y.; Millet, J.; Dutta, S.; Doughty, K.; Treu, J.A.; Katz, D.L. Effects of walnut consumption on endothelial function in type 2 diabetic subjects: A randomized controlled crossover trial. Diabetes Care 2010, 33, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Bulló, M.; Martínez-González, M.Á.; Ros, E.; Corella, D.; Estruch, R.; Fitó, M.; Arós, F.; Wärnberg, J.; Fiol, M.; et al. Frequency of nut consumption and mortality risk in the PREDIMED nutrition intervention trial. BMC Med. 2013, 11, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, Y.; Han, J.; Hu, F.B.; Giovannucci, E.L.; Stampfer, M.J.; Willett, W.C.; Fuchs, C.S. Association of nut consumption with total and cause-specific mortality. N. Engl. J. Med. 2013, 369, 2001–2011. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Nut consumption and risk of cardiovascular disease, total cancer, all-cause and cause-specific mortality: A systematic review and dose-response meta-analysis of prospective studies. BMC Med. 2016, 14, 207. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.C.; Zhang, R.; Martinez-Gonzalez, M.A.; Zhang, Z.L.; Bonaccio, M.; van Dam, R.M.; Qin, L.Q. Nut consumption in relation to all-cause and cause-specific mortality: A meta-analysis 18 prospective studies. Food Funct. 2017, 8, 3893–3905. [Google Scholar] [CrossRef]
- Fraser, G.E.; Sabatẽ, J.; Beeson, W.L. Nuts, Nuts Good for Your Heart…?-Reply. Arch. Intern. Med. 1992, 152, 2507–2511. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Wu, L.; Wang, Z.; Zhu, J.; Murad, A.L.; Prokop, L.J.; Murad, M.H. Nut consumption and risk of cancer and type 2 diabetes: A systematic review and meta-analysis. Nutr. Rev. 2015, 73, 409–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardman, W.E.; Primerano, D.A.; Legenza, M.T.; Morgan, J.; Fan, J.; Denvir, J. Dietary walnut altered gene expressions related to tumor growth, survival, and metastasis in breast cancer patients: A pilot clinical trial. Nutr. Res. 2019, 66, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Toledo, E.; Salas-Salvadó, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fitó, M.; Hu, F.B.; Arós, F.; et al. Mediterranean Diet and Invasive Breast Cancer Risk Among Women at High Cardiovascular Risk in the PREDIMED Trial: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef]
- Bes-Rastrollo, M.; Sabaté, J.; Gómez-Gracia, E.; Alonso, A.; Martínez, J.A.; Martínez-González, M.A. Nut consumption and weight gain in a Mediterranean cohort: The SUN study. Obesity 2007, 15, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Berryman, C.E.; Grieger, J.A.; West, S.G.; Chen, C.Y.; Blumberg, J.B.; Rothblat, G.H.; Sankaranarayanan, S.; Kris-Etherton, P.M. Acute consumption of walnuts and walnut components differentially affect postprandial lipemia, endothelial function, oxidative stress, and cholesterol efflux in humans with mild hypercholesterolemia. J. Nutr. 2013, 143, 788–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, E.H.; Gaban-Chong, N.; Oda, K.; Sabaté, J. Effect of a walnut meal on postprandial oxidative stress and antioxidants in healthy individuals. Nutr. J. 2014, 13, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ros, E.; Núñez, I.; Pérez-Heras, A.; Serra, M.; Gilabert, R.; Casals, E.; Deulofeu, R. A Walnut Diet Improves Endothelial Function in Hypercholesterolemic Subjects. Circulation 2004, 109, 1609–1614. [Google Scholar] [CrossRef] [Green Version]
- Lorgeril, M.D.; Salen, P.; Martin, J.-L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean Diet, Traditional Risk Factors, and the Rate of Cardiovascular Complications After Myocardial Infarction. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Pan, A.; Wang, D.D.; Liu, X.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C.; et al. Impact of Healthy Lifestyle Factors on Life Expectancies in the US Population. Circulation 2018, 138, 345–355. [Google Scholar] [CrossRef]
- Li, Y.; Schoufour, J.; Wang, D.D.; Dhana, K.; Pan, A.; Liu, X.; Song, M.; Liu, G.; Shin, H.J.; Sun, Q.; et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: Prospective cohort study. BMJ 2020, 368, l6669. [Google Scholar] [CrossRef] [Green Version]
- Bellavia, A.; Tektonidis, T.G.; Orsini, N.; Wolk, A.; Larsson, S.C. Quantifying the benefits of Mediterranean diet in terms of survival. Eur. J. Epidemiol. 2016, 31, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Menotti, A.; Puddu, P.E.; Maiani, G.; Catasta, G. Cardiovascular and other causes of death as a function of lifestyle habits in a quasi extinct middle-aged male population. A 50-year follow-up study. Int. J. Cardiol. 2016, 210, 173–178. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Never or Almost Never | Less Than Once per Week | Once per Week | Two to Four Times per Week | Five or More Times per Week | |
|---|---|---|---|---|---|
| Nurses’ Health Study | (n = 51,013) | (n = 12,398) | (n = 2525) | (n = 806) | (n = 272) |
| Age, years | 63.8 (7.1) | 62.9 (6.7) | 63.6 (6.9) | 65.0 (6.8) | 64.8 (6.7) |
| BMI | 26.7 (5.3) | 26.5 (5.2) | 26.2 (4.9) | 25.9 (5.2) | 25.0 (5.1) |
| AHEI score | 46.0 (9.1) | 47.7 (8.8) | 49.8 (8.9) | 53.5 (9.7) | 57.4 (9.6) |
| Physical activity, MET h/wk | 16.9 (21.3) | 19.1 (21.6) | 20.5 (22.9) | 22.7 (25.5) | 23.1 (24.4) |
| Alcohol intake, g | 5.0 (9.2) | 5.1 (8.8) | 5.1 (8.2) | 4.4 (7.8) | 4.7 (9.1) |
| Smoking status | |||||
| Past smoker,% | 45.0 | 43.0 | 43.4 | 38.8 | 46.8 |
| Current smoker, % | 11.2 | 8.3 | 6.6 | 6.7 | 2.6 |
| White, % | 97.5 | 97.9 | 98.0 | 95.4 | 97.7 |
| Multivitamin use, % | 60.4 | 62.3 | 63.7 | 67.2 | 74.6 |
| Aspirin use, % | 50.2 | 52.8 | 53.1 | 51.2 | 50.4 |
| Family history of diabetes, % | 28.5 | 28.4 | 29.1 | 27.8 | 31.4 |
| Family history of cancer, % | 12.8 | 12.8 | 14.0 | 11.0 | 13.7 |
| Family history of myocardial infarction, % | 24.9 | 24.7 | 23.5 | 23.1 | 23.2 |
| Family history of Hypercholesterolemia, % | 34.1 | 33.3 | 34.9 | 34.3 | 36.7 |
| Family history of Diabetes, % | 6.8 | 5.7 | 5.4 | 5.5 | 8.0 |
| Family history of Hypertension, % | 31.6 | 30.4 | 27.6 | 27.0 | 23.0 |
| Health Professionals Follow-Up Study | (n = 20,000) | (n = 4657) | (n = 1068) | (n = 387) | (n = 214) |
| Age, years | 63.2 (8.9) | 63.6 (8.8) | 64.0 (8.5) | 65.0 (8.9) | 65.7 (8.4) |
| BMI | 26.1 (3.6) | 26.1 (3.6) | 25.8 (3.3) | 25.3 (3.2) | 25.4 (3.2) |
| AHEI score | 45.1 (9.7) | 47.2 (9.3) | 48.9 (9.4) | 53.5 (10) | 56.4 (10.4) |
| Physical activity | 31.4 (30.3) | 36.2 (33.1) | 36.6 (33.8) | 39.5 (33.7) | 47.4 (43.1) |
| Alcohol intake, g | 11.2 (14.3) | 10.9 (13.2) | 10.9 (14.8) | 9.7 (12.6) | 9.7 (12.1) |
| Smoking status | |||||
| Past smoker,% | 51.1 | 48.4 | 47.3 | 46.4 | 47.0 |
| Current smoker, % | 4.9 | 3.8 | 4.0 | 5.0 | 4.1 |
| White, % | 91.7 | 92.1 | 92.4 | 90.9 | 89.6 |
| Multivitamin use, % | 48.2 | 50.2 | 52.6 | 55.1 | 54.3 |
| Aspirin use, % | 65.0 | 66.0 | 63.8 | 64.3 | 60.3 |
| Family history of diabetes, % | 22.6 | 21.9 | 22.8 | 20.9 | 24.6 |
| Family history of cancer, % | 37.5 | 38.8 | 39.2 | 37.5 | 33.8 |
| Family history of myocardial infarction, % | 32.4 | 30.9 | 31.1 | 30.7 | 29.3 |
| Family history of hypercholesterolemia, % | 28.7 | 27.0 | 27.5 | 30.5 | 27.5 |
| Family history of diabetes, % | 6.0 | 5.3 | 6.8 | 6.1 | 4.5 |
| Family history of hypertension, % | 26.6 | 24.6 | 24.7 | 25.4 | 22.9 |
| Never or Almost Never | <1 per Week | 1 per Week | 2–4 Times per Week | ≥5 Times per Week | Per 0.5 Serving Increase | p for Trend | |
|---|---|---|---|---|---|---|---|
| Total mortality | |||||||
| Women | |||||||
| No. of person-years | 763,683 | 245,165 | 82,129 | 55,752 | 31,969 | ||
| No. of deaths | 15,469 | 3110 | 966 | 701 | 409 | ||
| Age-adjusted model | 1.00 | 0.64 (0.62,0.67) | 0.57 (0.53,0.60) | 0.49 (0.45,0.53) | 0.47 (0.42,0.52) | 0.56 (0.53,0.59) | <0.0001 |
| Multivariate-adjusted Model 1 | 1.00 | 0.92 (0.89,0.96) | 0.87 (0.81,0.92) | 0.80 (0.74,0.86) | 0.79 (0.71,0.87) | 0.85 (0.81,0.89) | <0.0001 |
| Multivariate-adjusted Model 2 | 1.00 | 0.94 (0.90,0.98) | 0.87 (0.82,0.93) | 0.80 (0.74,0.87) | 0.78 (0.71,0.86) | 0.85 (0.81,0.89) | <0.0001 |
| Multivariate-adjusted Model 3 | 1.00 | 0.96 (0.92,1.00) | 0.93 (0.87,0.99) | 0.87 (0.80,0.94) | 0.85 (0.77,0.94) | 0.90 (0.86,0.95) | <0.0001 |
| Multivariate-adjusted Model 4 | 1.00 | 0.95 (0.91,0.99) | 0.92 (0.86,0.99) | 0.87 (0.81,0.95) | 0.85 (0.77,0.94) | 0.90 (0.86,0.95) | <0.0001 |
| Men | |||||||
| No. of person-years | 292,832 | 90,907 | 31,655 | 19,193 | 15,274 | ||
| No. of deaths | 6809 | 1605 | 573 | 347 | 274 | ||
| Age-adjusted model | 1.00 | 0.75 (0.71,0.79) | 0.73 (0.67,0.79) | 0.62 (0.55,0.69) | 0.59 (0.52,0.66) | 0.71 (0.67,0.75) | <0.0001 |
| Multivariate-adjusted Model 1 | 1.00 | 0.93 (0.88,0.98) | 0.94 (0.86,1.03) | 0.87 (0.78,0.96) | 0.82 (0.73,0.93) | 0.89 (0.84,0.95) | 0.0001 |
| Multivariate-adjusted Model 2 | 1.00 | 0.94 (0.89,0.99) | 0.95 (0.87,1.03) | 0.86 (0.77,0.96) | 0.82 (0.72,0.92) | 0.89 (0.84,0.94) | <0.0001 |
| Multivariate-adjusted Model 3 | 1.00 | 0.95 (0.89,1.00) | 0.98 (0.89,1.07) | 0.90 (0.80,1.01) | 0.86 (0.76,0.98) | 0.92 (0.87,0.98) | 0.007 |
| Multivariate-adjusted Model 4 | 1.00 | 0.93 (0.88,0.99) | 0.97 (0.88,1.06) | 0.89 (0.80,1.00) | 0.86 (0.76,0.98) | 0.92 (0.87,0.98) | 0.008 |
| Pooled | |||||||
| Age-adjusted model | 1.00 | 0.68 (0.65,0.70) | 0.62 (0.59,0.65) | 0.53 (0.49,0.56) | 0.51 (0.47,0.55) | 0.61 (0.59,0.64) | <0.0001 |
| Multivariate-adjusted Model 1 | 1.00 | 0.93 (0.90,0.95) | 0.89 (0.85,0.94) | 0.82 (0.77,0.87) | 0.80 (0.74,0.86) | 0.87 (0.83,0.90) | <0.0001 |
| Multivariate-adjusted Model 2 | 1.00 | 0.94 (0.91,0.97) | 0.90 (0.85,0.94) | 0.82 (0.77,0.87) | 0.79 (0.74,0.86) | 0.86 (0.83,0.89) | <0.0001 |
| Multivariate-adjusted Model 3 | 1.00 | 0.96 (0.92,0.99) | 0.94 (0.89,0.99) | 0.87 (0.81,0.93) | 0.85 (0.79,0.92) | 0.91 (0.87,0.94) | <0.0001 |
| Multivariate-adjusted Model 4 | 1.00 | 0.95 (0.91,0.98) | 0.94 (0.89,0.99) | 0.87 (0.82,0.93) | 0.86 (0.79,0.93) | 0.91 (0.88,0.95) | <0.0001 |
| CVD mortality | |||||||
| Women | |||||||
| No. of CVD deaths | 2468 | 475 | 139 | 96 | 41 | ||
| Age-adjusted model | 1.00 | 0.72 (0.65,0.79) | 0.60 (0.51,0.72) | 0.51 (0.42,0.63) | 0.39 (0.29,0.54) | 0.52 (0.45,0.60) | <0.0001 |
| Multivariate-adjusted Model 1 | 1.00 | 0.97 (0.88,1.07) | 0.87 (0.73,1.03) | 0.80 (0.65,0.99) | 0.62 (0.45,0.84) | 0.78 (0.68,0.89) | 0.0002 |
| Multivariate-adjusted Model 2 | 1.00 | 0.99 (0.89,1.09) | 0.87 (0.73,1.04) | 0.82 (0.67,1.01) | 0.63 (0.46,0.86) | 0.79 (0.69,0.90) | 0.0004 |
| Multivariate-adjusted Model 3 | 1.00 | 1.01 (0.91,1.12) | 0.93 (0.78,1.11) | 0.89 (0.72,1.10) | 0.69 (0.50,0.95) | 0.84 (0.73,0.96) | 0.02 |
| Multivariate-adjusted Model 4 | 1.00 | 1.00 (0.89,1.11) | 0.92 (0.77,1.11) | 0.90 (0.72,1.11) | 0.69 (0.50,0.95) | 0.84 (0.73,0.96) | 0.01 |
| Men | |||||||
| No. of CVD deaths | 1915 | 437 | 162 | 83 | 66 | ||
| Age-adjusted model | 1.00 | 0.76 (0.69,0.85) | 0.79 (0.67,0.93) | 0.57 (0.46,0.71) | 0.55 (0.43,0.70) | 0.67 (0.60,0.76) | <0.0001 |
| Multivariate-adjusted Model 1 | 1.00 | 0.93 (0.83,1.03) | 1.01 (0.85,1.18) | 0.79 (0.63,0.99) | 0.73 (0.57,0.93) | 0.84 (0.75,0.94) | 0.003 |
| Multivariate-adjusted Model 2 | 1.00 | 0.95 (0.85,1.05) | 1.02 (0.87,1.20) | 0.79 (0.63,0.99) | 0.73 (0.57,0.94) | 0.84 (0.75,0.94) | 0.003 |
| Multivariate-adjusted Model 3 | 1.00 | 0.94 (0.84,1.05) | 1.05 (0.89,1.25) | 0.85 (0.68,1.07) | 0.82 (0.63,1.06) | 0.90 (0.80,1.01) | 0.07 |
| Multivariate-adjusted Model 4 | 1.00 | 0.93 (0.83,1.04) | 1.03 (0.87,1.22) | 0.83 (0.66,1.05) | 0.80 (0.62,1.03) | 0.88 (0.78,0.99) | 0.04 |
| Pooled | |||||||
| Age-adjusted model | 1.00 | 0.74 (0.69,0.79) | 0.69 (0.61,0.78) | 0.54 (0.46,0.62) | 0.48 (0.39,0.58) | 0.60 (0.55,0.66) | <0.0001 |
| Multivariate-adjusted Model 1 | 1.00 | 0.95 (0.88,1.02) | 0.94 (0.84,1.06) | 0.80 (0.69,0.93) | 0.68 (0.56,0.83) | 0.81 (0.74,0.89) | <0.0001 |
| Multivariate-adjusted Model 2 | 1.00 | 0.97 (0.90,1.04) | 0.95 (0.84,1.07) | 0.80 (0.69,0.93) | 0.69 (0.57,0.84) | 0.82 (0.75,0.89) | <0.0001 |
| Multivariate-adjusted Model 3 | 1.00 | 0.98 (0.90,1.05) | 0.99 (0.87,1.12) | 0.86 (0.74,1.01) | 0.76 (0.62,0.93) | 0.87 (0.79,0.95) | 0.002 |
| Multivariate-adjusted Model 4 | 1.00 | 0.97 (0.89,1.04) | 0.98 (0.86,1.11) | 0.86 (0.73,1.00) | 0.75 (0.62,0.92) | 0.86 (0.79,0.94) | 0.001 |
| Cancer mortality | |||||||
| Women | |||||||
| No. of cancer deaths | 3225 | 768 | 254 | 154 | 95 | ||
| Age-adjusted model | 1.00 | 0.83 (0.77,0.90) | 0.79 (0.69,0.89) | 0.65 (0.55,0.77) | 0.74 (0.60,0.91) | 0.77 (0.70,0.85) | <0.0001 |
| Multivariate-adjusted Model 1 | 1.00 | 1.05 (0.96,1.13) | 1.05 (0.92,1.20) | 0.92 (0.78,1.08) | 1.06 (0.86,1.30) | 1.01 (0.92,1.10) | 0.91 |
| Multivariate-adjusted Model 2 | 1.00 | 1.05 (0.97,1.14) | 1.06 (0.93,1.20) | 0.92 (0.78,1.09) | 1.05 (0.85,1.29) | 1.00 (0.91,1.10) | 0.95 |
| Multivariate-adjusted Model 3 | 1.00 | 1.04 (0.95,1.13) | 1.07 (0.93,1.22) | 0.94 (0.79,1.11) | 1.09 (0.88,1.35) | 1.03 (0.93,1.13) | 0.60 |
| Multivariate-adjusted Model 4 | 1.00 | 1.02 (0.94,1.12) | 1.06 (0.92,1.21) | 0.94 (0.80,1.12) | 1.10 (0.89,1.36) | 1.03 (0.93,1.13) | 0.61 |
| Men | |||||||
| No. of cancer deaths | 1476 | 431 | 151 | 86 | 66 | ||
| Age-adjusted model | 1.00 | 0.93 (0.84,1.04) | 0.90 (0.76,1.07) | 0.77 (0.62,0.96) | 0.72 (0.56,0.92) | 0.82 (0.73,0.92) | 0.0009 |
| Multivariate-adjusted Model 1 | 1.00 | 1.07 (0.96,1.19) | 1.07 (0.90,1.27) | 0.97 (0.78,1.21) | 0.93 (0.73,1.19) | 0.97 (0.86,1.08) | 0.57 |
| Multivariate-adjusted Model 2 | 1.00 | 1.08 (0.97,1.20) | 1.07 (0.91,1.27) | 0.96 (0.77,1.19) | 0.91 (0.71,1.17) | 0.96 (0.85,1.07) | 0.43 |
| Multivariate-adjusted Model 3 | 1.00 | 1.06 (0.95,1.19) | 1.04 (0.87,1.24) | 0.92 (0.73,1.15) | 0.87 (0.67,1.13) | 0.93 (0.82,1.05) | 0.22 |
| Multivariate-adjusted Model 4 | 1.00 | 1.07 (0.95,1.20) | 1.05 (0.88,1.25) | 0.93 (0.74,1.17) | 0.91 (0.70,1.18) | 0.95 (0.84,1.07) | 0.37 |
| Pooled | |||||||
| Age-adjusted model | 1.00 | 0.86 (0.81,0.92) | 0.82 (0.74,0.91) | 0.69 (0.60,0.78) | 0.73 (0.62,0.85) | 0.79 (0.73,0.85) | <0.0001 |
| Multivariate-adjusted Model 1 | 1.00 | 1.06 (0.99,1.13) | 1.06 (0.96,1.18) | 0.94 (0.82,1.07) | 1.01 (0.86,1.18) | 0.99 (0.92,1.07) | 0.85 |
| Multivariate-adjusted Model 2 | 1.00 | 1.06 (0.99,1.13) | 1.06 (0.96,1.18) | 0.94 (0.82,1.07) | 1.00 (0.85,1.17) | 0.99 (0.92,1.06) | 0.76 |
| Multivariate-adjusted Model 3 | 1.00 | 1.05 (0.98,1.12) | 1.06 (0.95,1.18) | 0.93 (0.81,1.07) | 1.00 (0.85,1.18) | 0.99 (0.92,1.06) | 0.73 |
| Multivariate-adjusted Model 4 | 1.00 | 1.04 (0.97,1.12) | 1.05 (0.94,1.17) | 0.94 (0.82,1.08) | 1.02 (0.86,1.20) | 1.00 (0.92,1.07) | 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Guasch-Ferré, M.; Tobias, D.K.; Li, Y. Association of Walnut Consumption with Total and Cause-Specific Mortality and Life Expectancy in U.S. Adults. Nutrients 2021, 13, 2699. https://doi.org/10.3390/nu13082699
Liu X, Guasch-Ferré M, Tobias DK, Li Y. Association of Walnut Consumption with Total and Cause-Specific Mortality and Life Expectancy in U.S. Adults. Nutrients. 2021; 13(8):2699. https://doi.org/10.3390/nu13082699
Chicago/Turabian StyleLiu, Xiaoran, Marta Guasch-Ferré, Deirdre K. Tobias, and Yanping Li. 2021. "Association of Walnut Consumption with Total and Cause-Specific Mortality and Life Expectancy in U.S. Adults" Nutrients 13, no. 8: 2699. https://doi.org/10.3390/nu13082699
APA StyleLiu, X., Guasch-Ferré, M., Tobias, D. K., & Li, Y. (2021). Association of Walnut Consumption with Total and Cause-Specific Mortality and Life Expectancy in U.S. Adults. Nutrients, 13(8), 2699. https://doi.org/10.3390/nu13082699