
Positive Association between Endothelium–Platelet Microparticles and Urinary Concentration of Lead and Cadmium in Adolescents and Young Adults

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
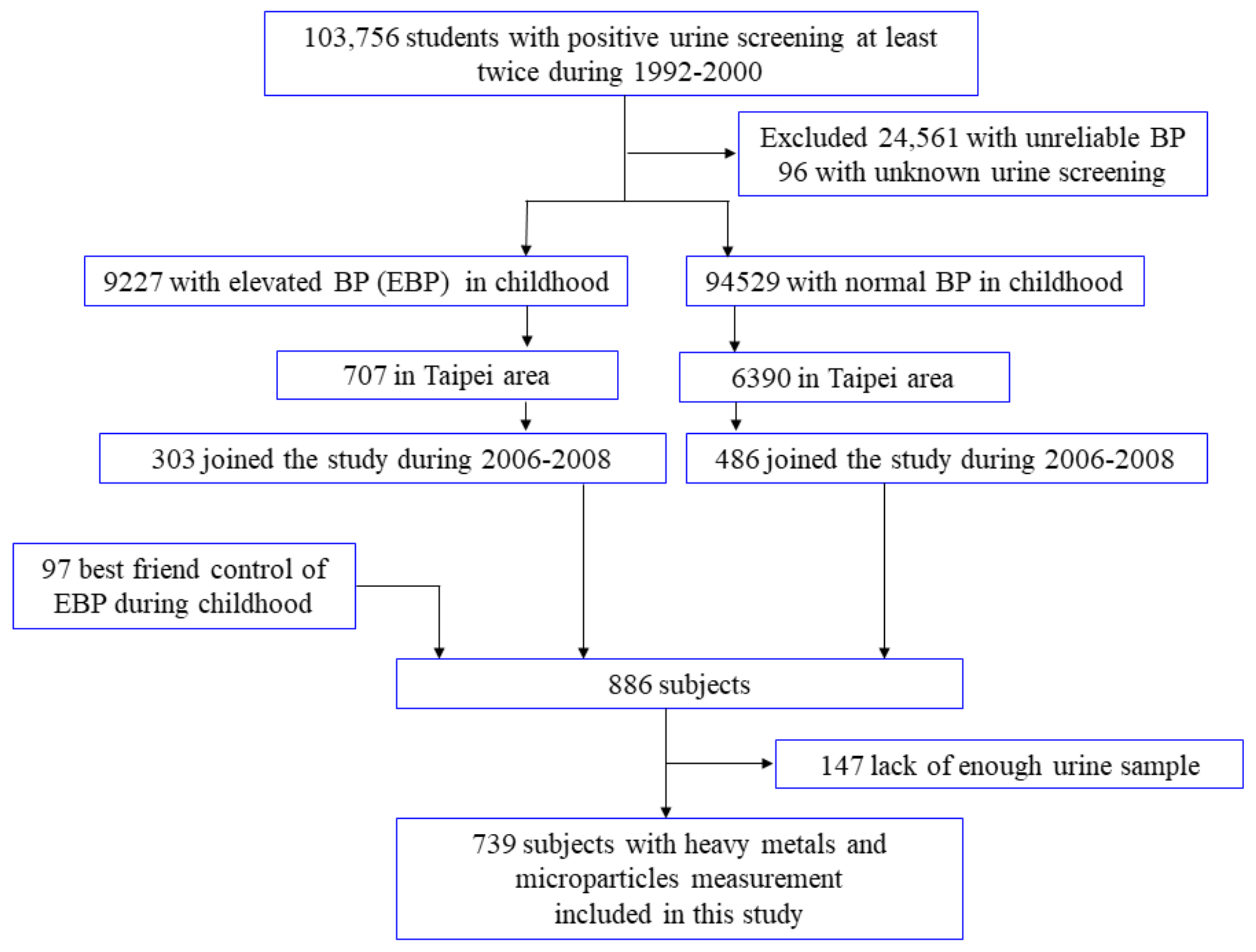
2.1. Study Design, Setting, and Ethics Statement
2.2. Measurement of Urinary Metals and Microparticles
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, U.K.; Kumar, B. Pathways of heavy metals contamination and associated human health risk in Ajay River basin, India. Chemosphere 2017, 174, 183–199. [Google Scholar] [CrossRef] [PubMed]
- Solenkova, N.V.; Newman, J.D.; Berger, J.S.; Thurston, G.; Hochman, J.S.; Lamas, G.A. Metal pollutants and cardiovascular disease: Mechanisms and consequences of exposure. Am. Heart J. 2014, 168, 812–822. [Google Scholar] [CrossRef]
- Jaishankar, M.; Tseten, T.; Anbalagan, N.; Mathew, B.B.; Beeregowda, K.N. Toxicity, mechanism and health effects of some heavy metals. Interdiscip. Toxicol. 2014, 7, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Navas-Acien, A.; Guallar, E.; Silbergeld, E.K.; Rothenberg, S.J. Lead exposure and cardiovascular disease—A systematic review. Environ. Health Perspect. 2007, 115, 472–482. [Google Scholar] [CrossRef]
- Lustberg, M.; Silbergeld, E. Blood lead levels and mortality. Arch. Intern. Med. 2002, 162, 2443–2449. [Google Scholar] [CrossRef]
- Schober, S.E.; Mirel, L.B.; Graubard, B.I.; Brody, D.J.; Flegal, K.M. Blood lead levels and death from all causes, cardiovascular disease, and cancer: Results from the NHANES III mortality study. Environ. Health Perspect. 2006, 114, 1538–1541. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Rauch, S.; Auinger, P.; Allen, R.W.; Hornung, R.W. Low-level lead exposure and mortality in US adults: A population-based cohort study. Lancet Public Health 2018, 3, e177–e184. [Google Scholar] [CrossRef]
- Jarup, L.; Akesson, A. Current status of cadmium as an environmental health problem. Toxicol. Appl. Pharmacol. 2009, 238, 201–208. [Google Scholar] [CrossRef]
- Lee, M.S.; Park, S.K.; Hu, H.; Lee, S. Cadmium exposure and cardiovascular disease in the 2005 Korea National Health and Nutrition Examination Survey. Environ. Res. 2011, 111, 171–176. [Google Scholar] [CrossRef]
- Tellez-Plaza, M.; Navas-Acien, A.; Menke, A.; Crainiceanu, C.M.; Pastor-Barriuso, R.; Guallar, E. Cadmium exposure and all-cause and cardiovascular mortality in the U.S. general population. Environ. Health Perspect. 2012, 120, 1017–1022. [Google Scholar] [CrossRef]
- Messner, B.; Knoflach, M.; Seubert, A.; Ritsch, A.; Pfaller, K.; Henderson, B.; Shen, Y.H.; Zeller, I.; Willeit, J.; Laufer, G.; et al. Cadmium is a novel and independent risk factor for early atherosclerosis mechanisms and in vivo relevance. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 1392–1398. [Google Scholar] [CrossRef]
- Liao, K.W.; Pan, W.H.; Liou, S.H.; Sun, C.W.; Huang, P.C.; Wang, S.L. Levels and temporal variations of urinary lead, cadmium, cobalt, and copper exposure in the general population of Taiwan. Environ. Sci. Pollut. Res. Int. 2019, 26, 6048–6064. [Google Scholar] [CrossRef]
- Lin, C.Y.; Huang, P.C.; Wu, C.; Sung, F.C.; Su, T.C. Association between urine lead levels and cardiovascular disease risk factors, carotid intima-media thickness and metabolic syndrome in adolescents and young adults. Int. J. Hyg. Environ. Health 2020, 223, 248–255. [Google Scholar] [CrossRef]
- Hoefer, I.E.; Steffens, S.; Ala-Korpela, M.; Back, M.; Badimon, L.; Bochaton-Piallat, M.L.; Boulanger, C.M.; Caligiuri, G.; Dimmeler, S.; Egido, J.; et al. Novel methodologies for biomarker discovery in atherosclerosis. Eur. Heart J. 2015, 36, 2635–2642. [Google Scholar] [CrossRef] [PubMed]
- Christersson, C.; Thulin, A.; Siegbahn, A. Microparticles during long-term follow-up after acute myocardial infarction. Association to atherosclerotic burden and risk of cardiovascular events. Thromb. Haemost. 2017, 117, 1571–1581. [Google Scholar] [PubMed]
- Tsai, C.-W.; Kuo, C.-C.; Wu, C.-F.; Chien, K.-L.; Wu, V.-C.; Chen, M.-F.; Sung, F.-C.; Su, T.-C. Associations of renal vascular resistance with albuminuria in adolescents and young adults. Nephrol. Dial. Transplant. 2011, 26, 3943–3949. [Google Scholar] [CrossRef][Green Version]
- Lin, C.Y.; Lin, L.Y.; Wen, T.W.; Lien, G.W.; Chien, K.L.; Hsu, S.H.; Liao, C.C.; Sung, F.C.; Chen, P.C.; Su, T.C. Association between levels of serum perfluorooctane sulfate and carotid artery intima-media thickness in adolescents and young adults. Int. J. Cardiol. 2013, 168, 3309–3316. [Google Scholar] [CrossRef]
- Wei, J.-N.; Sung, F.-C.; Lin, C.-C.; Lin, R.-S.; Chiang, C.-C.; Chuang, L.-M. National Surveillance for Type 2 Diabetes Mellitus in Taiwanese Children. JAMA 2003, 290, 1345–1350. [Google Scholar] [CrossRef]
- Chen, J.W.; Chen, H.Y.; Li, W.F.; Liou, S.H.; Chen, C.J.; Wu, J.H.; Wang, S.L. The association between total urinary arsenic concentration and renal dysfunction in a community-based population from central Taiwan. Chemosphere 2011, 84, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.L.; Kuo, C.C.; Pan, W.H.; Chung, Y.T.; Chen, C.Y.; Wu, T.N.; Wang, S.L. The decline in kidney function with chromium exposure is exacerbated with co-exposure to lead and cadmium. Kidney Int. 2017, 92, 710–720. [Google Scholar] [CrossRef] [PubMed]
- Chirinos, J.A.; Zambrano, J.P.; Virani, S.S.; Jimenez, J.J.; Jy, W.; Ahn, E.; Horstman, L.L.; Castellanos, A.; Myerburg, R.J.; Ahn, Y.S. Correlation between apoptotic endothelial microparticles and serum interleukin-6 and C-reactive protein in healthy men. Am. J. Cardiol. 2005, 95, 1258–1260. [Google Scholar] [CrossRef]
- Stohs, S.J.; Bagchi, D. Oxidative mechanisms in the toxicity of metal ions. Free Radic. Biol. Med. 1995, 18, 321–336. [Google Scholar] [CrossRef]
- Revis, N.W.; Zinsmeister, A.R.; Bull, R. Atherosclerosis and hypertension induction by lead and cadmium ions: An effect prevented by calcium ion. Proc. Natl. Acad. Sci. USA 1981, 78, 6494–6498. [Google Scholar] [CrossRef]
- Voors, A.W.; Shuman, M.S.; Johnson, W.D. Additive statistical effects of cadmium and lead on heart-related disease in a North Carolina autopsy series. Arch. Environ. Health 1982, 37, 98–102. [Google Scholar] [CrossRef]
- Aalbers, T.G.; Houtman, J.P. Relationships between trace elements and atherosclerosis. Sci. Total Environ. 1985, 43, 255–283. [Google Scholar] [CrossRef]
- Heiss, C.; Amabile, N.; Lee, A.C.; Real, W.M.; Schick, S.F.; Lao, D.; Wong, M.L.; Jahn, S.; Angeli, F.S.; Minasi, P.; et al. Brief secondhand smoke exposure depresses endothelial progenitor cells activity and endothelial function: Sustained vascular injury and blunted nitric oxide production. J. Am. Coll. Cardiol. 2008, 51, 1760–1771. [Google Scholar] [CrossRef]
- Amabile, N.; Rautou, P.E.; Tedgui, A.; Boulanger, C.M. Microparticles: Key protagonists in cardiovascular disorders. Semin. Thromb. Hemost. 2010, 36, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Burnier, L.; Fontana, P.; Kwak, B.R.; Angelillo-Scherrer, A. Cell-derived microparticles in haemostasis and vascular medicine. Thromb. Haemost. 2009, 101, 439–451. [Google Scholar] [CrossRef] [PubMed]
- Shantsila, E.; Kamphuisen, P.W.; Lip, G.Y. Circulating microparticles in cardiovascular disease: Implications for atherogenesis and atherothrombosis. J. Thromb. Haemost. 2010, 8, 2358–2368. [Google Scholar] [CrossRef]
- Werner, N.; Wassmann, S.; Ahlers, P.; Kosiol, S.; Nickenig, G. Circulating CD31+/annexin V+ apoptotic microparticles correlate with coronary endothelial function in patients with coronary artery disease. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Koga, H.; Sugiyama, S.; Kugiyama, K.; Watanabe, K.; Fukushima, H.; Tanaka, T.; Sakamoto, T.; Yoshimura, M.; Jinnouchi, H.; Ogawa, H. Elevated levels of VE-cadherin-positive endothelial microparticles in patients with type 2 diabetes mellitus and coronary artery disease. J. Am. Coll. Cardiol. 2005, 45, 1622–1630. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, R.; Robert, S.; Poncelet, P.; Kasthuri, R.S.; Key, N.S.; Dignat-George, F. Standardization of platelet-derived microparticle enumeration by flow cytometry with calibrated beads: Results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop. J. Thromb. Haemost. 2010, 8, 2571–2574. [Google Scholar] [CrossRef]
- Jimenez, J.J.; Jy, W.; Mauro, L.M.; Soderland, C.; Horstman, L.L.; Ahn, Y.S. Endothelial cells release phenotypically and quantitatively distinct microparticles in activation and apoptosis. Thromb. Res. 2003, 109, 175–180. [Google Scholar] [CrossRef]
- Bergdahl, I.A.; Schütz, A.; Gerhardsson, L.; Jensen, A.; Skerfving, S. Lead concentrations in human plasma, urine and whole blood. Scand. J. Work. Environ. Health 1997, 23, 359–363. [Google Scholar] [CrossRef]
- Bergdahl, I.A.; Skerfving, S. Biomonitoring of Lead Exposure—Alternatives to Blood. J. Toxicol. Environ. Health Part A 2008, 71, 1235–1243. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No. | Cd (μg/L) | Pb (μg/L) | Cr (μg/L) | Mn (μg/L) | Fe (μg/L) | Ni (μg/L) | Cu (μg/L) | Zn (μg/L) | |
|---|---|---|---|---|---|---|---|---|---|
| Overall | 739 | 0.22 ± 0.32 | 1.04 ± 2.07 | 0.03 ± 0.08 | 0.08 ± 0.15 | 1.81 ± 4.2 | 0.4 ± 1.42 | 1.36 ± 2.21 | 47.27 ± 33.63 |
| Age (years) | |||||||||
| 12–19 | 235 | 0.3 ± 0.38 | 1.64 ± 2.69 | 0.03 ± 0.03 | 0.08 ± 0.09 | 1.7 ± 2.21 | 0.43 ± 0.37 | 1.42 ± 1.26 | 53.73 ± 36.44 |
| 20–30 | 504 | 0.18 ± 0.27 ‡ | 0.76 ± 1.64 ‡ | 0.03 ± 0.1 | 0.08 ± 0.17 | 1.86 ± 4.86 | 0.39 ± 1.7 | 1.33 ± 2.53 | 44.26 ± 31.83 ‡ |
| Gender | |||||||||
| Male | 294 | 0.25 ± 0.33 | 1.21 ± 2.24 | 0.03 ± 0.06 | 0.1 ± 0.19 | 1.9 ± 3.6 | 0.42 ± 0.37 | 1.36 ± 1.18 | 47.22 ± 33.72 |
| Female | 445 | 0.18 ± 0.29 * | 0.78 ± 1.75 † | 0.03 ± 0.11 | 0.06 ± 0.03 ‡ | 1.67 ± 4.98 | 0.38 ± 2.21 | 1.36 ± 3.19 | 47.35 ± 33.55 |
| Smoking habit | |||||||||
| Never | 619 | 0.23 ± 0.32 | 1.09 ± 2.13 | 0.03 ± 0.05 | 0.08 ± 0.09 | 1.73 ± 3.54 | 0.43 ± 1.55 | 1.39 ± 2.36 | 47.77 ± 33.79 |
| Former | 21 | 0.12 ± 0.15 | 0.6 ± 1.49 | 0.1 ± 0.39 ‡ | 0.06 ± 0.03 | 3.51 ± 10.27 | 0.27 ± 0.16 | 1.19 ± 1.08 | 38.65 ± 20.76 |
| Current | 99 | 0.18 ± 0.29 | 0.85 ± 1.79 | 0.02 ± 0.04 | 0.1 ± 0.34 | 1.94 ± 5.65 | 0.26 ± 0.21 | 1.19 ± 1.12 | 45.98 ± 34.8 |
| Alcohol Consumption | |||||||||
| Never | 656 | 0.22 ± 0.32 | 1.03 ± 2.08 | 0.03 ± 0.05 | 0.08 ± 0.16 | 1.79 ± 4.05 | 0.42 ± 1.5 | 1.29 ± 1.35 | 47.42 ± 33.13 |
| Former | 13 | 0.36 ± 0.57 | 1.4 ± 2.56 | 0.02 ± 0.02 | 0.05 ± 0.03 | 1.4 ± 1.48 | 0.17 ± 0.1 | 1.45 ± 1.42 | 32.75 ± 22.36 |
| Current | 69 | 0.2 ± 0.25 | 1.05 ± 1.89 | 0.05 ± 0.22 | 0.06 ± 0.03 | 2.07 ± 5.72 | 0.3 ± 0.24 | 1.95 ± 5.89 | 49.05 ± 39.45 |
| Body Mass Index (kg/m2) | |||||||||
| <25 | 122 | 0.2 ± 0.28 | 0.91 ± 1.86 | 0.03 ± 0.09 | 0.08 ± 0.16 | 1.88 ± 4.56 | 0.42 ± 1.55 | 1.34 ± 2.34 | 46.62 ± 33.08 |
| ≥25 | 617 | 0.3 ± 0.45 * | 1.7 ± 2.82 † | 0.03 ± 0.04 | 0.08 ± 0.1 | 1.44 ± 1.29 * | 0.33 ± 0.35 | 1.46 ± 1.31 | 50.57 ± 36.26 |
| Hypertension | |||||||||
| Yes | 231 | 0.22 ± 0.3 | 1.02 ± 2 | 0.03 ± 0.08 | 0.08 ± 0.15 | 1.75 ± 3.5 | 0.41 ± 1.45 | 1.37 ± 2.25 | 47.14 ± 33.55 |
| No | 508 | 0.31 ± 0.58 | 1.54 ± 3.25 | 0.02 ± 0.03 | 0.06 ± 0.03 † | 3.03 ± 11.49 | 0.21 ± 0.14 † | 1.12 ± 0.86 | 50.03 ± 35.59 |
| Diabetes Mellitus | |||||||||
| Yes | 12 | 0.22 ± 0.3 | 1.01 ± 1.99 | 0.03 ± 0.08 | 0.08 ± 0.15 | 1.81 ± 4.23 | 0.4 ± 1.43 | 1.35 ± 2.22 | 46.79 ± 33.16 |
| No | 727 | 0.42 ± 0.75 | 2.66 ± 4.86 | 0.02 ± 0.02 | 0.08 ± 0.03 | 1.58 ± 1.5 | 0.36 ± 0.22 | 1.58 ± 1.48 | 76.62 ± 48.39 |
| Hyperlipidemia | |||||||||
| Yes | 150 | 0.22 ± 0.31 | 1.01 ± 2.04 | 0.03 ± 0.09 | 0.08 ± 0.17 | 1.95 ± 4.67 | 0.43 ± 1.59 | 1.38 ± 2.4 | 47.65 ± 33.85 |
| No | 589 | 0.22 ± 0.33 | 1.15 ± 2.18 | 0.02 ± 0.03 * | 0.07 ± 0.04 * | 1.26 ± 1.04 † | 0.31 ± 0.23 | 1.27 ± 1.16 | 45.78 ± 32.79 |
| Metals (µg/L) | Mean ± SD | Max | Min | Median | Q1 | Q3 | IQR |
|---|---|---|---|---|---|---|---|
| Cd | 2.01 ± 2.77 | 20.48 | 0.02 | 0.71 | 0.36 | 3.11 | 2.75 |
| Pb | 9.38 ± 17.82 | 103.18 | 0.05 | 1.35 | 0.66 | 5.61 | 4.95 |
| Cr | 0.26 ± 0.85 | 19.85 | 0.00 | 0.13 | 0.01 | 0.27 | 0.25 |
| Mn | 0.73 ± 1.21 | 27.71 | 0.01 | 0.58 | 0.43 | 0.78 | 0.35 |
| Fe | 16.83 ± 41.26 | 746.78 | 1.49 | 9.58 | 6.55 | 14.88 | 8.33 |
| Ni | 3.69 ± 14.10 | 379.35 | 0.00 | 2.48 | 1.50 | 3.96 | 2.46 |
| Cu | 12.83 ± 23.78 | 539.66 | 1.41 | 9.27 | 6.12 | 13.88 | 7.76 |
| Zn | 440.26 ± 316.00 | 2470.57 | 24.62 | 361.09 | 211.07 | 589.96 | 378.89 |
| Microparticles | |||||||
| CD14 | 124.64 ± 72.59 | 1110 | 0 | 111.43 | 80 | 151.43 | 71.43 |
| CD62E | 263.91 ± 134.99 | 1391.43 | 0 | 235.71 | 172.86 | 326.43 | 153.57 |
| CD62 | 163.47 ± 113.16 | 874.29 | 0 | 134.29 | 82.86 | 211.43 | 128.57 |
| CD31+/CD42a− | 386.42 ± 722.61 | 11,891.43 | 0 | 169.29 | 61.43 | 405 | 343.57 |
| CD31+/CD42a+ | 11,582.5 ± 18,530.6 | 129,938.6 | 0 | 4180.7 | 1190.7 | 12,966.4 | 11,775.7 |
| CD31+/CD42a− Counts, µL | |||||
|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | ||
| ≤61.43 | 61.43–169.29 | 169.29–405 | >405 | p-Trend | |
| Metals (µg/L) | 177 | 191 | 187 | 184 | |
| Cd | 0.86 ± 1.09 | 1.32 ± 2.09 | 2.07 ± 2.73 | 3.78 ± 3.56 | <0.0001 |
| Pb | 1.56 ± 2.24 | 3.86 ± 10.37 | 9.82 ± 17.57 | 22.20 ± 24.36 | <0.0001 |
| Cr | 0.23 ± 0.48 | 0.28 ± 1.46 | 0.25 ± 0.49 | 0.30 ± 0.45 | 0.5932 |
| Mn | 0.96 ± 2.21 | 0.65 ± 0.68 | 0.66 ± 0.72 | 0.65 ± 0.43 | 0.044 |
| Fe | 19.04 ± 40.23 | 15.43 ± 39.57 | 18.84 ± 58.70 | 14.11 ± 12.71 | 0.4811 |
| Ni | 4.99 ± 28.39 | 3.02 ± 2.78 | 3.28 ± 2.92 | 3.56 ± 2.80 | 0.3452 |
| Cu | 10.52 ± 8.77 | 11.26 ± 19.59 | 14.62 ± 39.99 | 14.86 ± 12.95 | 0.1498 |
| Zn | 392.39 ± 270.32 | 413.60 ± 299.47 | 447.54 ± 303.53 | 506.61 ± 371.79 | 0.0003 |
| CD31+/CD42a+ Counts, µL | |||||
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p-Trend | |
| ≤1190.71 | 1190.07–4180.71 | 4180.7–12,966.43 | >12,966.43 | ||
| Metals (µg/L) | 182 | 185 | 191 | 181 | |
| Cd | 1.07 ± 2.06 | 2.01 ± 2.74 | 2.41 ± 2.95 | 2.56 ± 2.98 | <0.0001 |
| Pb | 3.79 ± 12.38 | 9.12 ± 17.67 | 11.23 ± 19.71 | 13.32 ± 19.16 | <0.0001 |
| Cr | 0.23 ± 0.49 | 0.25 ± 0.44 | 0.23 ± 0.41 | 0.35 ± 1.52 | 0.2016 |
| Mn | 0.82 ± 1.02 | 0.82 ± 2.05 | 0.63 ± 0.35 | 0.63 ± 0.75 | 0.1546 |
| Fe | 16.91 ± 24.55 | 17.10 ± 37.67 | 18.16 ± 55.88 | 15.05 ± 40.26 | 0.7724 |
| Ni | 5.14 ± 28.02 | 3.07 ± 2.37 | 3.36 ± 3.02 | 3.22 ± 2.75 | 0.2841 |
| Cu | 15.32 ± 43.89 | 11.32 ± 11.45 | 12.86 ± 11.95 | 11.84 ± 9.34 | 0.2222 |
| Zn | 429.46 ± 284.31 | 429.62 ± 316.57 | 464.24 ± 331.44 | 436.70 ± 329.94 | 0.5894 |
| EMPs | PMPs | ||||
|---|---|---|---|---|---|
| CD62Ecounts | CD31+/CD42a−_countsUL | CD62Pcounts | CD31+/CD42a+_countsUR | CD14counts | |
| Cd, μg/L | 3.03 ± 1.91 | 59.67 ± 7.03 | 6.77 ± 1.62 | 1007.06 ± 259.22 | 3.24 ± 1.05 |
| p | 0.1133 | <0.0001 | <0.0001 | <0.0001 | 0.0022 |
| Pb, μg/L | 0.56 ± 0.30 | 10.04 ± 1.08 | 1.15 ± 0.25 | 176.17 ± 40.13 | 0.71 ± 0.16 |
| p | 0.0618 | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| Active smokers (N = 99) | |||||
| Cd, μg/L | 0.29 ± 4.51 | 108.22 ± 22.22 | 5.79 ± 4.24 | 1732.68 ± 676.46 | 3.34 ± 2.50 |
| p value | 0.949 | <0.001 | 0.175 | 0.012 | 0.185 |
| Pb μg/L | −0.12 ± 0.73 | 15.32 ± 3.70 | 0.32 ± 0.69 | 454.89 ± 102.18 | 0.97 ± 0.39 |
| p value | 0.865 | <0.001 | 0.645 | <0.001 | 0.016 |
| Inactive smokers (N = 638) | |||||
| Cd, μg/L | 3.30 ± 2.12 | 54.50 ± 7.36 | 6.91 ± 1.72 | 1012.36 ± 276.46 | 3.51 ± 1.13 |
| p value | 0.120 | <0.001 | <0.001 | <0.001 | 0.002 |
| Pb, μg/L | 0.67 ± 0.33 | 9.95 ± 1.12 | 1.22 ± 0.27 | 153.08 ± 42.91 | 0.70 ± 0.17 |
| p value | 0.043 | <0.001 | <0.001 | <0.001 | <0.001 |
| Range (ug/L) | N | ≥75th Percentile EMPs or PMPs | |||||
|---|---|---|---|---|---|---|---|
| EMPs | PMPs | ||||||
| CD62E Counts | CD31+/CD42a−_Counts UL | CD62P Counts | CD31+/CD42a+_Counts UR | CD14 Counts | |||
| Pb | |||||||
| Quartile 1 | ≤0.657 | 184 | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) |
| Quartile 2 | 0.657–1.345 | 186 | 0.85 (0.50, 1.45) | 1.36 (0.69, 2.69) | 1.09(0.66, 1.80) | 0.52 (0.29, 0.95) | 1.05 (0.59, 1.87) |
| Quartile 3 | 1.345–5.610 | 185 | 1.05 (0.63, 1.76) | 2.72 (1.45, 5.09) | 0.75 (0.44, 1.27) | 1.56 (0.95, 2.57) | 1.40 (0.80, 2.44) |
| Quartile 4 | >5.610 | 184 | 1.61 (0.97, 2.65) | 13.22 (7.12, 24.55) | 1.68 (1.02, 2.78) | 2.10 (1.28, 3.46) | 3.49 (2.06, 5.91) |
| p-trend | 0.0047 | <0.0001 | 0.0140 | <0.0001 | <0.0001 | ||
| Per doubling change | 1.01 (1.00, 1.02) | 1.05 (1.04, 1.06) | 1.02 (1.01, 1.03) | 1.01(1.00,1.02) | 1.02 (1.01, 1.03) | ||
| Cd | |||||||
| Quartile 1 | ≤0.360 | 184 | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) |
| Quartile 2 | 0.360–0.710 | 186 | 0.75 (0.44, 1.30) | 1.74 (0.85, 3.54) | 1.35 (0.80, 2.29) | 0.53 (0.30, 0.95) | 0.85 (0.47, 1.51) |
| Quartile 3 | 0.710–3.111 | 185 | 1.29 (0.78, 2.13) | 4.76 (2.49, 9.09) | 1.05 (0.61, 1.81) | 1.20 (0.73, 1.99) | 1.76 (1.04, 2.99) |
| Quartile 4 | >3.111 | 184 | 1.14 (0.68, 1.92) | 15.72 (8.18, 30.20) | 2.00 (1.19, 3.38) | 1.72 (1.04, 2.85) | 1.99 (1.17, 3.38) |
| p-trend | 0.0573 | <0.0001 | 0.0013 | 0.0004 | <0.0001 | ||
| Per doubling change | 1.05 (0.99, 1.11) | 1.37 (1.26, 1.49) | 1.12 (1.06, 1.19) | 1.08 (1.02, 1.14) | 1.09 (1.03, 1.16) | ||
| CD31+/CD42a− | CD31+/CD42a+ | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SE | p Value | p for Trend | Mean | SE | p Value | p for Trend | |
| Pb ≤ 50th and Cd ≤ 50th | 218.41 | 40.56 | Reference | <0.001 | 8647.03 | 1448.90 | Reference | <0.001 |
| Pb > 50th and Cd ≤ 50th | 270.09 | 73.79 | 0.697 | 7541.92 | 2605.26 | 1.000 | ||
| Pb ≤ 50th and Cd > 50th | 334.17 | 72.93 | 1.000 | 13,375.92 | 2635.98 | 0.406 | ||
| Pb > 50th and Cd > 50th | 579.29 | 40.79 | <0.001 | 17,363.41 | 1457.19 | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-K.; Wu, C.; Lin, C.-Y.; Huang, P.-C.; Sung, F.-C.; Su, T.-C. Positive Association between Endothelium–Platelet Microparticles and Urinary Concentration of Lead and Cadmium in Adolescents and Young Adults. Nutrients 2021, 13, 2913. https://doi.org/10.3390/nu13092913
Lee C-K, Wu C, Lin C-Y, Huang P-C, Sung F-C, Su T-C. Positive Association between Endothelium–Platelet Microparticles and Urinary Concentration of Lead and Cadmium in Adolescents and Young Adults. Nutrients. 2021; 13(9):2913. https://doi.org/10.3390/nu13092913
Chicago/Turabian StyleLee, Chih-Kuo, Charlene Wu, Chien-Yu Lin, Po-Chin Huang, Fung-Chang Sung, and Ta-Chen Su. 2021. "Positive Association between Endothelium–Platelet Microparticles and Urinary Concentration of Lead and Cadmium in Adolescents and Young Adults" Nutrients 13, no. 9: 2913. https://doi.org/10.3390/nu13092913
APA StyleLee, C.-K., Wu, C., Lin, C.-Y., Huang, P.-C., Sung, F.-C., & Su, T.-C. (2021). Positive Association between Endothelium–Platelet Microparticles and Urinary Concentration of Lead and Cadmium in Adolescents and Young Adults. Nutrients, 13(9), 2913. https://doi.org/10.3390/nu13092913