Independent Dose–Response Associations between Fetuin-A and Lean Nonalcoholic Fatty Liver Disease

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Ultrasonography Assessment
2.3. Blood Analysis
2.4. Statistical Analysis
3. Results
3.1. General Characteristics
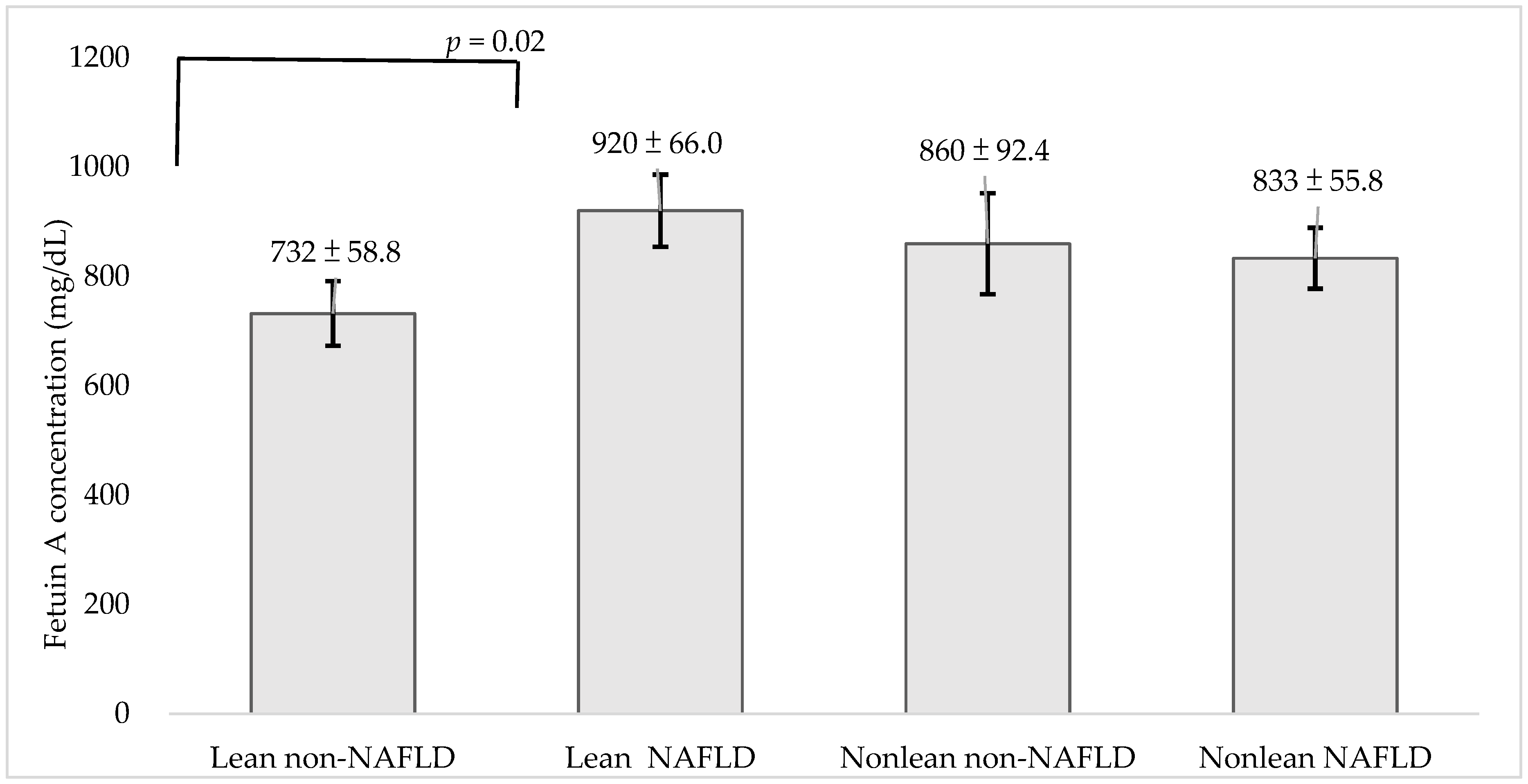
3.2. Association of Fetuin-A and NAFLD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Rinella, M.E.; Sanyal, A.J.; Harrison, S.A.; Brunt, E.M.; Goodman, Z.; Cohen, D.E.; Loomba, R. From NAFLD to MAFLD: Implications of a Premature Change in Terminology. Hepatology 2021, 73, 1194–1198. [Google Scholar] [CrossRef] [PubMed]
- Loomis, A.K.; Kabadi, S.; Preiss, D.; Hyde, C.; Bonato, V.; Louis, M.S.; Desai, J.; Gill, J.M.R.; Welsh, P.; Waterworth, D.; et al. Body Mass Index and Risk of Nonalcoholic Fatty Liver Disease: Two Electronic Health Record Prospective Studies. J. Clin. Endocr. Metab. 2016, 101, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Akyuz, U.; Yesil, A.; Yilmaz, Y. Characterization of lean patients with nonalcoholic fatty liver disease: Potential role of high hemoglobin levels. Scand. J. Gastroenterol. 2015, 50, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Margariti, E.; Deutsch, M.; Manolakopoulos, S.; Papatheodoridis, G.V. Non-alcoholic fatty liver disease may develop in individuals with normal body mass index. Ann. Gastroenterol. 2012, 25, 45–51. [Google Scholar]
- Wang, A.Y.; Dhaliwal, J.; Mouzaki, M. Lean non-alcoholic fatty liver disease. Clin. Nutr. 2019, 38, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Das, K.; Das, K.; Mukherjee, P.S.; Ghosh, A.; Ghosh, S.; Mridha, A.R.; Dhibar, T.; Bhattacharya, B.; Bhattacharya, D.; Manna, B.; et al. Nonobese population in a developing country has a high prevalence of nonalcoholic fatty liver and significant liver disease. Hepatology 2010, 51, 1593–1602. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, H.J.; Lee, K.E.; Kim, D.J.; Kim, S.K.; Ahn, C.W.; Lim, S.-K.; Kim, K.R.; Lee, H.C.; Huh, K.B.; et al. Metabolic significance of nonalcoholic fatty liver disease in nonobese, nondiabetic adults. Arch. Intern. Med. 2004, 164, 2169–2175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, J.C.; Loong, T.C.; Wei, J.L.; Wong, G.L.-H.; Chan, A.; Choi, P.C.; Shu, S.S.; Chim, A.M.; Chan, H.L.; Wong, V.W. Histological severity and clinical outcomes of nonalcoholic fatty liver disease in nonobese patients. Hepatology 2017, 65, 54–64. [Google Scholar] [CrossRef]
- Margariti, A.; Deutsch, M.; Manolakopoulos, S.; Tiniakos, D.; Papatheodoridis, G.V. The severity of histologic liver lesions is independent of body mass index in patients with nonalcoholic fatty liver disease. J. Clin. Gastronterol. 2013, 47, 280–286. [Google Scholar] [CrossRef]
- Jirak, P.; Stechemesser, L.; Moré, E.; Franzen, M.; Topf, A.; Mirna, M.; Paar, V.; Pistulli, R.; Kretzschmar, D.; Wernly, B.; et al. Clinical implications of fetuin-A. Adv. Clin. Chem. 2019, 89, 79–130. [Google Scholar] [PubMed]
- Auberger, P.; Falquerho, L.; Contreres, J.O.; Pages, G.; Le Cam, G.; Rossi, B.; Le Cam, A. Characterization of a natural inhibitor of the insulin receptor tyrosine kinase: cDNA cloning, purification, and anti-mitogenic activity. Cell 1989, 58, 631–640. [Google Scholar] [CrossRef]
- Sujana, C.; Huth, C.; Zierer, A.; Meesters, S.; Sudduth-Klinger, J.; Koenig, W.; Herder, C.; Peters, A.; Thorand, B. Association of fetuin-A with incident type 2 diabetes: Results from the MONICA/KORA Augsburg study and a systematic meta-analysis. Eur. J. Endocrinol. 2018, 178, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Roshanzamir, F.; Miraghajani, M.; Rouhani, M.H.; Mansourian, M.; Ghiasvand, R.; Safavi, S.M. The association between circulating fetuin-A levels and type 2 diabetes mellitus risk: Systematic review and meta-analysis of observational studies. J. Rndocrinol. Investig. 2018, 41, 33–47. [Google Scholar] [CrossRef]
- Pal, D.; Dasgupta, S.; Kundu, R.; Maitra, S.; Das, G.; Mukhopadhyay, S.; Ray, S.; Majumdar, S.S.; Bhattacharya, S. Fetuin-A acts as an endogenous ligand of TLR4 to promote lipid-induced insulin resistance. Nat. Med. 2012, 18, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Fritsche, A.; Weikert, C.; Boeing, H.; Joost, H.-G.; Häring, H.-U.; Schulze, M.B. Plasma fetuin-A levels and the risk of type 2 diabetes. Diabetes 2008, 57, 2762–2767. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Xiao, J.; Zhao, Z.; Wang, M.; Wang, Y.; Xin, Y. Systematic Review and Meta-analysis of Circulating Fetuin-A Levels in Nonalcoholic Fatty Liver Disease. J. Clin. Transl. Hepatol. 2021, 9, 3–14. [Google Scholar]
- Kalinowski, A.; Humphreys, K. Governmental standard drink definitions and low-risk alcohol consumption guidelines in 37 countries. Addiction 2016, 111, 1293–1298. [Google Scholar] [CrossRef] [Green Version]
- Brick, J. Standardization of alcohol calculations in research. Alcohol. Clin. Exp. Res. 2006, 30, 1276–1287. [Google Scholar] [CrossRef]
- Savva, S.; Tornaritis, M.; Savva, M.; Kourides, Y.; Panagi, A.; Silikiotou, N.; Georgiou, C.; Kafatos, A. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1453–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballestri, S.; Lonardo, A.; Romagnoli, D.; Carulli, L.; Losi, L.; Day, C.P.; Loria, P. Ultrasonographic fatty liver indicator, a novel score which rules out NASH and is correlated with metabolic parameters in NAFLD. Liver Int. 2012, 32, 1242–1252. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, K.O. Fetuin, a new globulin isolated from serum. Nature 1944, 154, 575. [Google Scholar] [CrossRef]
- Osawa, M.; Umetsu, K.; Sato, M.; Ohki, T.; Yukawa, N.; Suzuki, T.; Takeichi, S. Structure of the gene encoding human alpha 2-HS glycoprotein (AHSG). Gene 1997, 196, 121–125. [Google Scholar] [CrossRef]
- Stefan, N.; Hennige, A.M.; Staiger, H.; Machann, J.; Schick, F.; Kröber, S.M.; Machicao, F.; Fritsche, A.; Häring, H.-U. Alpha2-Heremans-Schmid glycoprotein/fetuin-A is associated with insulin resistance and fat accumulation in the liver in humans. Diabetes Care 2006, 29, 853–857. [Google Scholar] [CrossRef] [Green Version]
- Mathews, S.T.; Singh, G.P.; Ranalletta, M.; Cintron, V.J.; Qiang, X.; Goustin, A.-S.; Jen, K.-L.C.; Charron, M.J.; Jahnen-Dechent, W.; Grunberger, G. Improved insulin sensitivity and resistance to weight gain in mice null for the Ahsg gene. Diabetes 2002, 51, 2450–2458. [Google Scholar] [CrossRef] [Green Version]
- Orr, J.S.; Puglisi, M.J.; Ellacott, K.L.; Lumeng, C.N.; Wasserman, D.H.; Hasty, A.H. Toll-like receptor 4 deficiency promotes the alternative activation of adipose tissue macrophages. Diabetes 2012, 61, 2718–2727. [Google Scholar] [CrossRef] [Green Version]
- Haukeland, J.W.; Dahl, T.B.; Yndestad, A.; Gladhaug, I.P.; Løberg, E.M.; Haaland, T.; Konopski, Z.; Wium, C.; Aasheim, E.T.; Johansen, O.E. Fetuin A in nonalcoholic fatty liver disease: In vivo and in vitro studies. Eur. J. Endocrinol. 2012, 166, 503–510. [Google Scholar] [CrossRef]
- Dasgupta, S.; Bhattacharya, S.; Biswas, A.; Majumdar, S.S.; Mukhopadhyay, S.; Ray, S.; Bhattacharya, S. NF-kappaB mediates lipid-induced fetuin-A expression in hepatocytes that impairs adipocyte function effecting insulin resistance. Biochem. J. 2010, 429, 451–462. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, P.; Seal, S.; Mukherjee, S.; Kundu, R.; Mukherjee, S.; Ray, S.; Mukhopadhyay, S.; Majumdar, S.S.; Bhattacharya, S. Adipocyte fetuin-A contributes to macrophage migration into adipose tissue and polarization of macrophages. J. Biol. Chem. 2013, 288, 28324–28330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinella, M.E. Nonalcoholic fatty liver disease: A systematic review. JAMA 2015, 313, 2263–2273. [Google Scholar] [CrossRef]
- Sookoian, S.; Pirola, C.J. Systematic review with meta-analysis: The significance of histological disease severity in lean patients with nonalcoholic fatty liver disease. Aliment. Pharm. Ther. 2018, 47, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younes, R.; Govaere, O.; Petta, S.; Miele, L.; Tiniakos, D.; Burt, A.; David, E.; Vecchio, F.M.; Maggioni, M.; Cabibi, D.; et al. Caucasian lean subjects with non-alcoholic fatty liver disease share long-term prognosis of non-lean: Time for reappraisal of BMI-driven approach? Gut 2021. [Google Scholar] [CrossRef] [PubMed]
- Garg, A. Acquired and inherited lipodystrophies. N. Engl. J. Med. 2004, 350, 1220–1234. [Google Scholar] [CrossRef]
- Savage, D.B. Mouse models of inherited lipodystrophy. Dis. Model Mech. 2009, 2, 554–562. [Google Scholar] [CrossRef] [Green Version]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Adipose tissue, obesity and non-alcoholic fatty liver disease. Minerva Endocrinol. 2017, 42, 92–108. [Google Scholar] [CrossRef]
- Rotman, Y.; Neuschwander-Tetri, B.A. Liver fat accumulation as a barometer of insulin responsiveness again points to adipose tissue as the culprit. Hepatology 2017, 65, 1088–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akinci, B.; Meral, R.; Oral, E.A. Phenotypic and Genetic Characteristics of Lipodystrophy: Pathophysiology, Metabolic Abnormalities, and Comorbidities. Curr. Diabetes Rep. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Schick, F.; Häring, H.U. Causes, Characteristics, and Consequences of Metabolically Unhealthy Normal Weight in Humans. Cell Metab. 2017, 26, 292–300. [Google Scholar] [CrossRef]
- Asterholm, I.W.; Halberg, N.; Scherer, P.E. Mouse Models of Lipodystrophy Key reagents for the understanding of the metabolic syndrome. Drug Discov. Today Dis. Models 2007, 4, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, T.Y.; Fan, J.G. What are the clinical settings and outcomes of lean NAFLD? Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 289–290. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Lonardo, A.; Loria, P. Nonalcoholic fatty liver disease activity score and Brunt’s pathologic criteria for the diagnosis of nonalcoholic steatohepatitis: What do they mean and do they agree? Hepatology 2011, 53, 2142–2143. [Google Scholar] [CrossRef]

{kind=link}
| Lean | Non-Lean | p Value | |||
|---|---|---|---|---|---|
| Non-NAFLD | NAFLD | Non-NAFLD | NAFLD | ||
| N = 227 | N = 108 | N = 54 | N = 217 | ||
| Age (years) | 41.1 ± 11.0 | 42.6 ± 11.6 | 44.5 ± 11.3 | 43.7 ± 11.8 | 0.061 |
| Male (%) | 47 (20.7%) | 37 (34.3%) | 25 (46.3%) | 123 (56.7%) | <0.001 |
| Female (%) | 180 (79.3%) | 71 (65.7%) | 29 (53.7%) | 94 (43.3%) | <0.001 |
| BMI (kg/m2) | 20.6 ± 1.8 | 21.9 ± 1.5 | 26.0 ± 1.7 | 28.1 ± 4.0 | <0.001 |
| WC (cm) | 73.1 ± 6.1 | 77.6 ± 6.5 | 85.4 ± 6.2 | 91.1 ± 8.3 | <0.001 |
| Body fat (%) | 25.6 ± 6.2 | 26.6 ± 6.0 | 30.0 ± 7.9 | 32.4 ± 8.4 | <0.001 |
| Systolic BP | 115.7 ± 15.7 | 121.6 ± 15.3 | 122.6 ± 17.0 | 130.4 ± 15.3 | <0.001 |
| Diastolic BP | 72.9 ± 11.2 | 77.2 ± 9.5 | 77.9 ± 13.8 | 82.2 ± 12.2 | <0.001 |
| TCHO (mmol/L) | 190.0 ± 33.8 | 196.9 ± 39.8 | 194.6 ± 29.3 | 201.7 ± 35.5 | 0.007 |
| TG (mmol/L) | 74.2 ± 37.2 | 109.2 ± 78.9 | 95.0 ± 43.5 | 160.2 ± 113.8 | <0.001 |
| HDL-C (mmol/L) | 66.7 ± 15.0 | 57.3 ± 13.2 | 59.5 ± 13.5 | 49.7 ± 12.6 | <0.001 |
| LDL-C (mmol/L) | 114.5 ± 31.2 | 125.4 ± 37.1 | 123.0 ± 29.2 | 131.7 ± 32.5 | <0.001 |
| Glucose (mmol/L) | 83.7 ± 13.0 | 85.3 ± 8.7 | 87.0 ± 10.4 | 94.2 ± 22.8 | <0.001 |
| Insulin (U/mL) | 5.29 ± 4.24 | 6.77 ± 5.21 | 7.1 ± 3.9 | 11.5 ± 8.9 | <0.001 |
| HOMA-IR | 0.68 ± 0.55 | 0.86 ± 0.65 | 0.91 ± 0.49 | 1.49 ± 1.10 | <0.001 |
| Current smoker (%) | 16 (7.0) | 11 (10.2) | 5 (9.3) | 35 (16.1) | 0.022 |
| Exercise (%) | 100 (44.1) | 46 (42.6) | 27 (50.0) | 92 (42.4) | 0.782 |
| GOT | 20.3 ± 6.8 | 21.7 ± 7.0 | 21.5 ± 5.9 | 25.8 ± 10.2 | <0.001 |
| GPT | 17.2 ± 9.4 | 23.8 ± 16.5 | 21.4 ± 10.6 | 36.7 ± 27.8 | <0.001 |
| CRP (mg/dL) | 0.11 ± 0.31 | 0.10 ± 0.13 | 0.17 ± 0.28 | 0.22 ± 0.25 | <0.001 |
| Metabolic factors | 0.39 ± 0.62 | 0.91 ± 0.89 | 1.15 ± 0.90 | 2.14 ± 1.18 | <0.001 |
| MetS (%) | 2 (2.5) | 6 (7.5) | 4 (5.0) | 68 (85) | <0.001 |
| Fetuin-A (mg/L) | 689.4 ± 672.4 | 882.6 ± 731.3 | 829.3 ± 429.3 | 855.9 ± 467.0 | 0.009 |
| Lean/NAFLD: | +/− vs. +/+ | +/− vs. −/− | +/− vs. −/+ | +/+ vs. −/− | +/+ vs. −/+ | −/− vs. −/+ |
|---|---|---|---|---|---|---|
| Age (years) | 0.663 | 0.199 | 0.079 | 0.754 | 0.856 | 0.966 |
| Male (%) | 0.059 | 0.002 | <0.001 | 0.400 | <0.001 | 0.451 |
| BMI (kg/m2) | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| WC (cm) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Body fat (%) | 0.610 | <0.001 | <0.001 | 0.024 | <0.001 | 0.122 |
| Systolic BP | 0.007 | 0.019 | <0.001 | 0.977 | <0.001 | 0.006 |
| Diastolic BP | 0.007 | 0.022 | <0.001 | 0.986 | 0.002 | 0.075 |
| TCHO (mmol/L) | 0.339 | 0.822 | 0.003 | 0.980 | 0.658 | 0.553 |
| TG (mmol/L) | 0.001 | 0.321 | <0.001 | 0.711 | <0.001 | <0.001 |
| HDL-C (mmol/L) | <0.001 | 0.003 | <0.001 | 0.745 | <0.001 | <0.001 |
| LDL-C (mmol/L) | 0.023 | 0.315 | <0.001 | 0.971 | 0.359 | 0.296 |
| Glucose (mmol/L) | 0.833 | 0.5448 | <0.001 | 0.928 | <0.001 | 0.024 |
| Insulin (U/mL) | 0.303 | 0.352 | <0.001 | 0.994 | <0.001 | <0.001 |
| HOMA-IR | 0.303 | 0.324 | <0.001 | 0.990 | <0.001 | <0.001 |
| GOT | 0.499 | 0.767 | <0.001 | 1.000 | <0.001 | 0.003 |
| GPT | 0.017 | 0.463 | <0.001 | 0.876 | <0.001 | <0.001 |
| CRP (mg/dL) | 0.961 | 0.439 | <0.001 | 0.321 | <0.001 | 0.672 |
| Fetuin-A (mg/L) | 0.030 | 0.413 | 0.019 | 0.951 | 0.981 | 0.991 |
| Q1 (N = 202) (≤821 mg/L) | Q2 (N = 201) (822–1012 mg/L) | Q3 (N = 203) (1013–1224 mg/L) | p for Trend | |
|---|---|---|---|---|
| Model 1 | 1.00 | 2.49 (1.64–3.77) ** | 2.62 (1.72–3.98) ** | <0.001 |
| Model 2 | 1.00 | 1.55 (0.94–2.56) | 1.80 (1.10–2.94) * | 0.020 |
| Model 3 | 1.00 | 1.49 (0.87–2.57) | 1.57 (0.92–2.67) | 0.099 |
| Lean NAFLD | ||||
| Q1 (N = 158) | Q2 (N = 75) | Q3 (N = 102) | p for Trend | |
| Model 1 | 1.00 | 1.01 (0.53–1.90) | 1.95 (1.14–3.34) * | 0.018 |
| Model 2 | 1.00 | 1.26 (0.63–2.50) | 2.26 (1.26–4.07) * | 0.007 |
| Model 3 | 1.00 | 1.33 (0.63–2.82) | 2.09 (1.09–3.98) * | 0.026 |
| Overweight/Obese NAFLD | ||||
| Q1 (N = 44) | Q2 (N = 126) | Q3 (N = 101) | p for Trend | |
| Model 1 | 1.00 | 1.48 (0.65–3.38) | 1.35 (0.57–3.21) | 0.603 |
| Model 2 | 1.00 | 1.20 (0.47–3.02) | 0.89 (0.34–2.33) | 0.688 |
| Model 3 | 1.00 | 0.95 (0.35–2.56) | 0.69 (0.24–1.95) | 0.422 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, C.-W.; Lee, Y.-C.; Chiang, C.-H.; Chang, H.-H.; Yang, W.-S.; Huang, K.-C. Independent Dose–Response Associations between Fetuin-A and Lean Nonalcoholic Fatty Liver Disease. Nutrients 2021, 13, 2928. https://doi.org/10.3390/nu13092928
Lu C-W, Lee Y-C, Chiang C-H, Chang H-H, Yang W-S, Huang K-C. Independent Dose–Response Associations between Fetuin-A and Lean Nonalcoholic Fatty Liver Disease. Nutrients. 2021; 13(9):2928. https://doi.org/10.3390/nu13092928
Chicago/Turabian StyleLu, Chia-Wen, Yi-Chen Lee, Chien-Hsieh Chiang, Hao-Hsiang Chang, Wei-Shiung Yang, and Kuo-Chin Huang. 2021. "Independent Dose–Response Associations between Fetuin-A and Lean Nonalcoholic Fatty Liver Disease" Nutrients 13, no. 9: 2928. https://doi.org/10.3390/nu13092928
APA StyleLu, C.-W., Lee, Y.-C., Chiang, C.-H., Chang, H.-H., Yang, W.-S., & Huang, K.-C. (2021). Independent Dose–Response Associations between Fetuin-A and Lean Nonalcoholic Fatty Liver Disease. Nutrients, 13(9), 2928. https://doi.org/10.3390/nu13092928