
Using a Community-Based Participatory Mixed Methods Research Approach to Develop, Evaluate, and Refine a Nutrition Intervention to Replace Sugary Drinks with Filtered Tap Water among Predominantly Central-American Immigrant Families with Infants and Toddlers: The Water Up @Home Pilot Evaluation Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Stage 1—Connecting and Diagnosing
2.1.1. Connecting with the Community
2.1.2. Exploratory Mixed Methods for Diagnosis
2.2. Stage 2—Prescribing-Implementing (Design of Intervention)
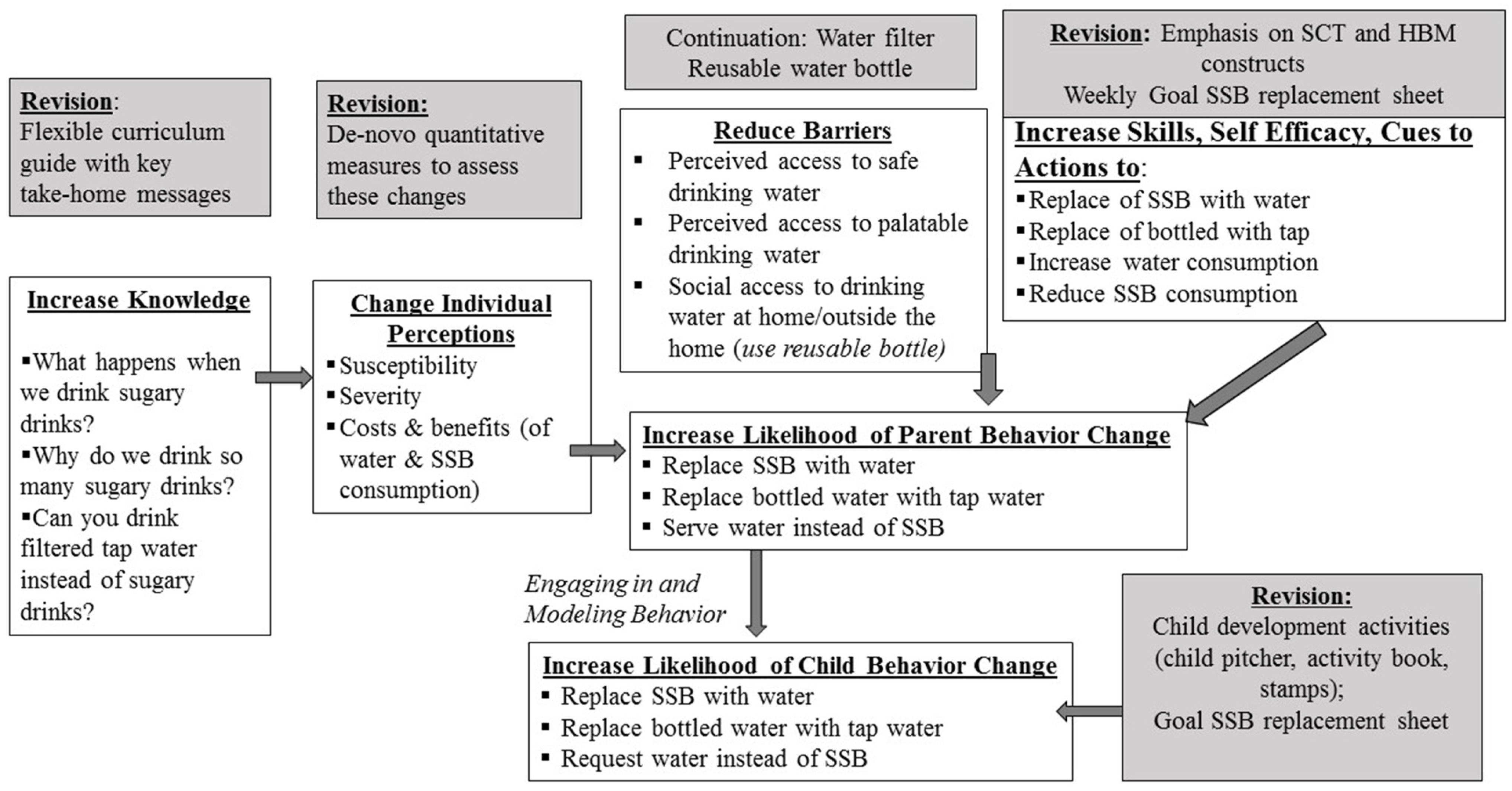
2.2.1. Co-Learning to Develop Theoretical Framework
2.2.2. Addressing the Theoretical Constructs of Knowledge, Susceptibility, Severity, Costs and Benefits in the Vulnerability, Epistemology, Perceived Physiological, and Health Protection Domains via a Curriculum
2.2.3. Addressing the Physiological Domain: Real and Perceived Physical Barriers to Drink Tap Water Instead of SSB
2.2.4. Increasing Skills and Self-Efficacy
2.2.5. Implementation Design
2.3. Stage 3—Evaluation of Implementation and Impact
2.3.1. Methods of Stage 3
2.3.2. Results of Stage 3 Intervention Evaluation
2.3.3. Mixed Methods Results for Behavior Change and Theoretical Underpinnings
Theme 1: Knowledge Gains after Intervention
Theme 2: Perceptions of Susceptibility, Severity, Costs and Benefits
Theme 3: Perceived Physical Barriers to Drinking Filtered Tap Water
Theme 4: Skills and Self-Efficacy
Theme 5: Parental Behavior Change in Beverage Consumption
Theme 6: Parental Decision and Modeling in Child Beverage Consumption
2.4. Stage 4—Dissemination and Refinement of the Intervention
2.4.1. Dissemination
2.4.2. Refinement of Intervention
3. Discussion
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stoecker, R. Research Methods for Community Change: A Project-Based Approach, 2nd ed.; SAGE Publications: Los Angeles, CA, USA, 2013. [Google Scholar] [CrossRef] [Green Version]
- Wallerstein, N.; Duran, B. Community-based participatory research contributions to intervention research: The intersection of science and practice to improve health equity. Am. J. Public Health 2010, 100 (Suppl. 1), S40–S46. [Google Scholar] [CrossRef]
- Espinosa, P.R.; Sussman, A.; Pearson, C.R.; Oetzel, J.G.; Wallerstein, N. Personal outcomes in community-based participatory research partnerships: A cross-site mixed methods study. Am. J. Community Psychol. 2020, 66, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Coombe, C.M.; Cheezum, R.R.; Schulz, A.J.; McGranaghan, R.J.; Lichtenstein, R.; Reyes, A.G.; Clement, J.; Burris, A. Community-based participatory research: A capacity-building approach for policy advocacy aimed at eliminating health disparities. Am. J. Public Health 2010, 100, 2094–2102. [Google Scholar] [CrossRef]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of community-based research: Assessing partnership approaches to im-prove public health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elwood, W.N.; Corrigan, J.G.; Morris, K.A. NIH-funded CBPR: Self-reported community partner and investigator perspectives. J. Community Health 2019, 44, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Jagosh, J.; Macaulay, A.C.; Pluye, P.; Salsberg, J.; Bush, P.; Henderson, J.; Sirett, E.; Wong, G.; Cargo, M.; Herbert, C.P.; et al. Uncovering the benefits of participatory research: Implications of a realist review for health research and practice. Milbank Q. 2012, 90, 311–346. [Google Scholar] [CrossRef] [Green Version]
- Lucero, J.; Wallerstein, N.; Duran, B.; Alegria, M.; Greene-Moton, E.; Israel, B.; Kastelic, S.; Magarati, M.; Oetzel, J.; Pearson, C.; et al. Development of a mixed methods investigation of process and outcomes of community-based participatory research. J. Mix. Methods Res. 2016, 12, 55–74. [Google Scholar] [CrossRef] [Green Version]
- Cresswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research; Sage Publications: London, UK, 2011. [Google Scholar]
- Dejonckheere, M.; Lindquist-Grantz, R.; Toraman, S.; Haddad, K.; Vaughn, L.M. Intersection of mixed methods and community-based participatory research: A methodological review. J. Mix. Methods Res. 2018, 13, 481–502. [Google Scholar] [CrossRef]
- Rosinger, A.Y.; Bethancourt, H.; Francis, L.A. Association of caloric intake from sugar-sweetened beverages with water intake among US children and young adults in the 2011-2016 National Health and Nutrition examination survey. JAMA Pediatr. 2019, 173, 602–604. [Google Scholar] [CrossRef]
- Kit, B.K.; Fakhouri, T.H.; Park, S.; Nielsen, S.J.; Ogden, C.L. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999–2010. Am. J. Clin. Nutr. 2013, 98, 180–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among adults in the United States: Cross-sectional study using data from NHANES 2005–2010. BMC Public Health 2013, 13, 1068. [Google Scholar] [CrossRef] [Green Version]
- Gorelick, M.H. Perceptions about water and increased use of bottled water in minority children. Arch. Pediatr. Adolesc. Med. 2011, 165, 928–932. [Google Scholar] [CrossRef] [Green Version]
- Hobson, W.L.; Knochel, M.L.; Byington, C.L.; Young, P.C.; Hoff, C.J.; Buchi, K.F. Bottled, filtered, and tap water use in Latino and non-Latino children. Arch. Pediatr. Adolesc. Med. 2007, 161, 457–461. [Google Scholar] [CrossRef] [Green Version]
- Scherzer, T.; Barker, J.C.; Pollick, H.; Weintraub, J.A. Water consumption beliefs and practices in a rural Latino community: Impli-cations for fluoridation. J. Public Health Dent. 2010, 70, 337–343. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.I.; Bogart, L.M.; Klein, D.J.; Schuster, M.A.; Elliott, M.N.; Hawes-Dawson, J.; Lamb, S.; Uyeda, K.E. Increasing the availability and consumption of drinking water in middle schools: A pilot study. Prev. Chronic Dis. 2011, 8, A60. [Google Scholar] [PubMed]
- Onufrak, S.J.; Park, S.; Sharkey, J.R.; Sherry, B. The relationship of perceptions of tap water safety with intake of sugar-sweetened beverages and plain water among US adults. Public Health Nutr. 2012, 17, 179–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, M.M.; MacDonald, G.; Collazos, J.; Levinger, B.; Leighton, E.; Ball, J. From Cradle to Career: The Multiple Challenges Facing Immigrant Families to Langley Park Promise; Urban Institute: Washington, DC, USA, 2014. [Google Scholar]
- Edberg, M.; Cleary, S.; Simmons, L.B.; Cubilla-Batista, I.; Andrade, E.L.; Gudger, G. Defining the “community” for a community-based public health intervention addressing Latino immigrant health disparities: An application of ethnographic methods. Hum. Organ. 2015, 74, 27–41. [Google Scholar] [CrossRef]
- Andrade, E.L.; Evans, W.D.; Barrett, N.; Edberg, M.C.; Cleary, S.D. Strategies to increase Latino immigrant youth engagement in health promotion using social media: Mixed-methods study. JMIR Public Health Surveill. 2018, 4, e71. [Google Scholar] [CrossRef] [PubMed]
- Colón-Ramos, U.; Monge-Rojas, R.; Cremm, E.; Rivera, I.M.; Andrade, E.L.; Edberg, M.C. How Latina mothers navigate a ‘food swamp’ to feed their children: A photovoice approach. Public Health Nutr. 2017, 20, 1941–1952. [Google Scholar] [CrossRef] [Green Version]
- Kumar, G.S.; Pan, L.; Park, S.; Lee-Kwan, S.H.; Onufrak, S.; Blanck, H.M. Sugar-sweetened beverage consumption among adults—18 states, 2012. MMWR Morb. Mortal Wkly. Rep. 2014, 63, 686–690. [Google Scholar]
- Park, S.; Xu, F.; Town, M.; Blanck, H.M. Prevalence of sugar-sweetened beverage intake among adults—23 states and the district of Columbia, 2013. MMWR. Morb. Mortal. Wkly. Rep. 2016, 65, 169–174. [Google Scholar] [CrossRef]
- Harris, J.L.; Schwartz, M.B.; Brownell, K.D. Evaluating Sugary Drink Nutrition Hand Marketing to Youth. Available online: https://pdfs.semanticscholar.org/4c0c/fc3aaea547fed24315181d9a4b5318547b56.pdf (accessed on 4 May 2017).
- Hu, Z.; Morton, L.W.; Mahler, R.L. Bottled water: United States consumers and their perceptions of water quality. Int. J. Environ. Res. Public Health 2011, 8, 565–578. [Google Scholar] [CrossRef] [PubMed]
- Wall, T.P.; Brown, L.J. Dental visits among Hispanics in the United States, 1999. J. Am. Dent. Assoc. 2004, 135, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General; U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health: Rockville, MD, USA, 2000.
- Ayala, G.X.; Castro, I.A.; Pickrel, J.L.; Williams, C.B.; Lin, S.-F.; Madanat, H.; Jun, H.-J.; Zive, M. A restaurant-based intervention to promote sales of healthy children’s menu items: The Kids’ Choice Restaurant Program cluster randomized trial. BMC Public Health 2016, 16, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayala, G.X.; Baquero, B.; Pickrel, J.L.; Mayer, J.; Belch, G.; Rock, C.L.; Linnan, L.; Gittelsohn, J.; Sanchez-Flack, J.; Elder, J.P. A store-based intervention to increase fruit and vegetable consumption: The El Valor de Nuestra Salud cluster randomized controlled trial. Contemp. Clin. Trials 2015, 42, 228–238. [Google Scholar] [CrossRef] [Green Version]
- United States Department of Agriculture and Food and Nutrition Service. Healthy Hunger-Free Kids Act. Available online: https://www.fns.usda.gov/cn/healthy-hunger-free-kids-act (accessed on 25 February 2021).
- Partnership for a Healthier America. Drink Up. Available online: https://www.ahealthieramerica.org/articles/about-drink-up-260#:~:text=Drink%20Up%20was%20a%20collaboration,families%20%2D%20and%20stakeholders%20across%20the (accessed on 25 February 2021).
- Barrett, N.; Colón-Ramos, U.; Elkins, A.; Rivera, I.; Evans, W.D.; Edberg, M. Formative research to design a promotional campaign to increase drinking water among central American Latino youth in an urban area. J. Health Commun. 2017, 60, 1–10. [Google Scholar] [CrossRef]
- Plested, B.A.; Edwards, R.W.; Jumper-Thurman, P. Community Readiness: A Handbook for Successful Change, Tri-Ethnic Center for Prevention Research 2006. Available online: www.TriEthnicCenter.ColoState.edu/communityreadiness/ (accessed on 24 August 2021).
- Hanna-Attisha, M.; Lachance, J.; Sadler, R.C.; Schnepp, A.C. Elevated blood lead levels in children associated with the flint drinking water crisis: A spatial analysis of risk and public health response. Am. J. Public Health 2016, 106, 283–290. [Google Scholar] [CrossRef]
- Dixon, J.K.; Dixon, J.P. An integrative model for environmental health research. ANS Adv. Nurs. Sci. 2002, 24, 43–57. [Google Scholar] [CrossRef] [PubMed]
- Balazs, C.L.; Ray, I. The drinking water disparities framework: On the origins and persistence of inequities in exposure. Am. J. Public Health 2014, 104, 603–611. [Google Scholar] [CrossRef]
- Hochbaum, G.; Rosenstock, I.; Kegels, S. Health Belief Model; United States Public Health Service: Washington, DC, USA, 1952.
- Hedrick, V.E.; Comber, D.L.; Estabrooks, P.A.; Savla, J.; Davy, B.M. The beverage intake questionnaire: Determining initial validity and reliability. J. Am. Diet. Assoc. 2010, 110, 1227–1232. [Google Scholar] [CrossRef] [Green Version]
- Lora, K.; Davy, B.; Hedrick, V.; Ferris, A.M.; Anderson, M.P.; Wakefield, D. Assessing initial validity and reliability of a beverage intake questionnaire in Hispanic preschool-aged children. J. Acad. Nutr. Diet. 2016, 116, 1951–1960. [Google Scholar] [CrossRef]
- Hedrick, V.E.; Comber, D.L.; Ferguson, K.E.; Estabrooks, P.A.; Savla, J.; Dietrich, A.M.; Serrano, E.; Davy, B.M. A rapid beverage intake questionnaire can detect changes in beverage intake. Eat. Behav. 2012, 14, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedrick, V.; Comber, D.; Flack, K.; Estabrooks, P.; Savla, J.; Davy, B. Development of a Brief Questionnaire to Assess Habitual Beverage Intake: Sugar-Sweetened Beverages and Total Beverage Energy Intake. J. Am. Diet. Assoc. 2010, 110, A26. [Google Scholar] [CrossRef]
- Hill, C.E.; MacDougall, C.R.; Riebl, S.K.; Savla, J.; Hedrick, V.E.; Davy, B.M. Evaluation of the relative validity and test-retest reliability of a 15-item beverage intake questionnaire in children and adolescents. J. Acad. Nutr. Diet. 2017, 117, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Bernard, H.R. Research Methods in Anthropology: Qualitative and Quantitative Approaches, 4th ed.; AltaMira Press: Lanham, MD, USA, 2006. [Google Scholar]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis; Sage: London, UK, 2006. [Google Scholar]
- Bryman, A. Barriers to Integrating Quantitative and Qualitative Research. J. Mix. Methods Res. 2007, 1, 8–22. [Google Scholar] [CrossRef]
- Bandura, A. Social Cognitive Theory: An Agentic Perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandura, A. Human agency in social cognitive theory. Am. Psychol. 1989, 44, 1175–1184. [Google Scholar] [CrossRef]
- Vargas-Garcia, E.; Evans, C.; Prestwich, A.; Sykes-Muskett, B.; Hooson, J.; Cade, J. Interventions to reduce consumption of sugar-sweetened beverages or increase water intake: Evidence from a systematic review and meta-analysis. Obes. Rev. 2017, 18, 1350–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United States Department of Health and Human Services, Administration for Children and Families, Office of Head Start. Head Start Early Learning Outcomes Framework: Ages Birth to Five 2015. Available online: https://eclkc.ohs.acf.hhs.gov/interactive-head-start-early-learning-outcomes-framework-ages-birth-five (accessed on 24 August 2021).
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; United States Department of Agriculture, Department of Health and Human Services: Washington, DC, USA, 2015.
- Wong, J.M.W.; Ebbeling, C.B.; Robinson, L.; Feldman, H.A.; Ludwig, D.S. Effects of Advice to Drink 8 Cups of Water per Day in Adolescents with Overweight or Obesity: A Randomized Clinical Trial. JAMA Pediatr. 2017, 171, e170012. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.I.; Schmidt, L.A. Water Access in the United States: Health Disparities Abound and Solutions Are Urgently Needed. Am. J. Public Health 2017, 107, 1354–1356. [Google Scholar] [CrossRef] [PubMed]
- Demmer, E.; Cifelli, C.J.; Houchins, J.A.; Fulgoni, V.L. Ethnic disparities of beverage consumption in infants and children 0–5 years of age; National Health and Nutrition Examination Survey 2011 to 2014. Nutr. J. 2018, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B. Resolved: There is sufficient scientific evidence that decreasing sugar-sweetened beverage consumption will reduce the prevalence of obesity and obesity-related diseases. Obes. Rev. 2013, 14, 606–619. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Li, R.; Park, S.; Galuska, D.A.; Sherry, B.; Freedman, D.S. A Longitudinal Analysis of Sugar-Sweetened Beverage Intake in Infancy and Obesity at 6 Years. Pediatrics 2014, 134, S29–S35. [Google Scholar] [CrossRef] [Green Version]
- Dibay Moghadam, S.; Krieger, J.W.; Louden, D.K.N. A systematic review of the effective-ness of promoting water intake to reduce sugar-sweetened beverage consumption. Obes. Sci. Pract. 2020, 6, 229–246. [Google Scholar] [CrossRef]
- Vercammen, K.A.; Frelier, J.M.; Lowery, C.M.; Moran, A.J.; Bleich, S.N. Strategies to reduce sugar-sweetened beverage consumption and in-crease water access and intake among young children: Perspectives from expert stakeholders. Public Health Nutr. 2018, 21, 3440–3449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyman, M.B.; Abrams, S.A.; Gastroenterology, H.S.O. Committee on Nutrition Fruit Juice in Infants, Children, and Adolescents: Current Recommendations. Pediatrics 2017, 139, e20170967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, J.K.; Haapanen, K.A.; Backus, A.; Mack, S.M.; Lindsey, M.; Andrade, K. Aligning Community-Engaged Research to Context. Int. J. Environ. Res. Public Health 2020, 17, 1187. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Characteristics | n (%) or Mean (SD) |
|---|---|
| Sex n = 35 | |
| Male | 2 (5.71) |
| Female | 33 (94.28) |
| Age categories n = 36 | |
| 18–25 years | 5 (13.89) |
| 26–30 years | 7 (19.44) |
| 30–34 years | 13 (36.11) |
| 35–40 years | 8 (22.22) |
| 41–65 years | 3 (8.33) |
| Education n = 33 | |
| 0–6 years | 15 (45.45) |
| 7–12 years | 13 (39.39) |
| >13 years | 5 (15.15) |
| Country of birth n = 36 | |
| El Salvador | 17 (47.22) |
| Guatemala | 12 (33.33) |
| Honduras | 4 (11.11) |
| Mexico | 2 (5.56) |
| U.S. | 1 (2.78) |
| Number of years in US n = 35 | |
| 3–5 years | 5 (14.28) |
| 6–10 years | 8 (22.85) |
| 10–20 years | 22 (62.86) |
| Household income n = 36 | |
| $1–5 K | 1 (2.78) |
| $5–10 K | 3 (8.33) |
| $10–15 K | 6 (16.67) |
| $15–20 K | 16 (44.44) |
| $20–30 K | 6 (16.67) |
| $30–40 K | 3 (8.33) |
| $>40 K | 1 (2.78) |
| Mean age of children in months, n = 36 | 29.53 (10.87) |
| Household size, n = 36 | |
| 1 person | 1 (2.78) |
| 2–4 people | 10 (27.78) |
| 5–6 people | 14 (38.89) |
| >7 people | 11 (30.56) |
| Number of hours spent with child 1 at home, n = 36 | |
| 4–6 h | 5 (13.89) |
| >7 h | 31 (86.11) |
| Where did you obtain water outside of U.S.?, n= 35 | |
| Bottle | 4 (11.42) |
| Filtered | 4 (11.46) |
| Tap/Faucet | 16 (45.71) |
| Well/Spring | 11 (31.42) |
| Where did you obtain water in the U.S.?, n = 35 | |
| Bottle | 31 (88.57) |
| Filtered | 2 (5.71) |
| Tap/Faucet | 2 (5.71) |
| How much do you spend in water? n = 36 | |
| $25 bi-weekly | 8 (22.22) |
| $25 per week | 7 (19.44) |
| >$25 per month | 11(19.44) |
| $25 per month | 4 (11.11) |
| <$25 per month | 6 (13.89) |
| Theme 1: Knowledge Gained after the Intervention | |||||
| Survey Variable | Baseline, Mean (SD) | Follow-Up, Mean (SD) | Difference | p-Value 3 | |
| Meta-Inference: The curriculum lessons provided participants with new knowledge about key concepts regarding health risks associated with consuming sugary drinks and benefits of drinking water. | Knowledge Score 1 n = 27 | 8.07 (1.04) | 9.15 (1.23) | 1.07 | 0.002 |
| Illustrative Explanatory Quotes | 1.1: “…where the water comes from, knowing the amount of sugar that we need in our bodies… and knowing how much sugar is in the sugary drinks that we consume daily”. | ||||
| 1.2: “I learned a lot because I had an… incorrect concept [about water] because I was told when I arrived in this country [the U.S.] that I could not drink tap water because it was not drinkable. Therefore, I did not trust using it. After the program was delivered, and they taught us about the water and that it was good, I understood how important it is, and how much more economical”. | |||||
| 1.3: “What I liked most was learning how much sugar we need as people. […]since we were accustomed to drinking coffee [with sugar], soda, and everything else sweet that one eats, you go over the six teaspoons”. | |||||
| 1.4: “… soda, pop, sweet coffee, drinks, it is saying that all sugar, it can give you diabetes”. | |||||
| Theme 2: Perceptions of susceptibility, severity, and costs & benefits | |||||
| Illustrative Explanatory Quotes | 2.1: “As Hispanics, we are most likely to get sick from sugar, to have diabetes, and I believe that it is because we don’t drink water, because we don’t have the information… that sugar can cause us harm in the near future if we continue drinking too many sugary drinks”. | ||||
| 2.2: “… they are things that one needs to know… because sometimes one can be causing themselves harm; speaking of diseases, primarily diabetes, which is a disease that humans can suffer from due to consuming a lot of sugar”. | |||||
| Theme 3: Perceived physical barriers to drinking filtered tap water | |||||
| Survey Variable | Baseline n (%) | Follow-Up n (%) | p-Value 3 | ||
| Meta-Inference: Concerns about tap water safety continued throughout the intervention but the use of the water filter may have mitigated some of those concerns, and motivated parents to move from bottled to tap water consumption. | Do you drink tap water at home? n = 36 | 0.08 | |||
| Always | 4 (11.11) | 14 (38.89) | |||
| Sometimes | 8 (22.22) | 7 (19.44) | |||
| Never | 24 (66.67) | 15 (41.67) | |||
| Do you give your children tap water at home? n = 35 | 0.51 | ||||
| Always | 2 (5.71) | 12 (34.29) | |||
| Sometimes | 6 (17.14) | 7 (20.00) | |||
| Never | 27 (77.14) | 16 (45.71) | |||
| How often do your children drink bottled water at home? n = 35 | 0.7 | ||||
| Always | 29 (82.86) | 10 (28.57) | |||
| Sometimes | 6 (17.14) | 17 (48.57) | |||
| Never | 0 (0) | 8 (22.86) | |||
| If your children don’t drink tap water at home, why not? n = 31 | 0.71 | ||||
| Don’t like taste | 4 (12.90) | 4 (12.90) | |||
| Makes me sick | 21 (67.74) | 18 (58.06) | |||
| Told not to | 3 (9.68) | 1 (3.23) | |||
| Other | 3 (9.68) | 8 (25.81) | |||
| Do you like the taste of water? n = 36 | 0.56 | ||||
| Don’t like at all | 0 (0) | 1 (2.78) | |||
| Don’t like too much | 0 (0) | 0 (0) | |||
| Slightly Like | 7 (19.44) | 0 (0) | |||
| Like | 7 (19.44) | 10 (27.78) | |||
| Strongly Like | 22 (61.11) | 25 (69.44) | |||
| Illustrative Explanatory Quotes | 3.1: “Tap water has lead; I say that that tap water is bad. Filtered is another thing, but I don’t like tap water”. | ||||
| 3.2: “I didn’t have a filter. I bought water and I spent a lot [of money] on water, so with this filter I save a lot”. | |||||
| 3.3: “The barrier was starting to drink water without filtering it. [After receiving the filter] everything was fine, since I was more trusting; even the children were drinking this water”. | |||||
| 3.4: “With the filter I believe that the flavor is good… I smelled the scent of the unfiltered water, and the scent of the filtered water is totally different”. | |||||
| Theme 4: Skills and self-efficacy | |||||
| Survey Variable | Baseline Mean (SD) | Follow-Up Mean (SD) | Difference | p-Value3 | |
| Meta-Inference: Intervention increased self-efficacy to drink water instead of SSB, and identified areas of future work (providing support for partners or entities outside the home for targeted behaviors). | Self-efficacy 2 n = 28 | 51.57 (4.65) | 54.21 (2.48) | 2.64 | 0.007 |
| Illustrative Explanatory Quotes | 4.1: “[The intervention] helped me a lot because there was a time when it was very hot… and first I thought of soda, but after I said, ‘no, I need to drink water because it is healthier’, and that is how I put into practice what I had been told”. | ||||
| 4.2: “This is the first thing I do now; before…when one does not have the adequate information one only goes and looks… to see what is on sale, but now I try to recall the [information] about the teaspoons of sugar that every drink contains and I focus on the [nutrition] label”. | |||||
| 4.3: what [was more difficult] was my husband and still today since he always says after eating: I want something sweet (,,,).he tells me always: make me a sweet tea…I want to drink something sweet’. | |||||
| Theme 5: Parental behavior change in beverage consumption (n = 36) | ||||
| Survey Variable Beverage | Baseline Mean (SD) | Follow-up Mean (SD) | Mean Difference (95% CI) | p-Value 3 |
| Total Water Intake | 45.36 | 44.94 | −0.42 | 0.91 |
| (14.42) | (16.11) | (−7.72, 6.88) | ||
| 100% Fruit Juice | 8.41 | 3.09 | −5.32 | 0.005 |
| (11.39) | (5.03) | (−8.88, −1.76) | ||
| Fruit-flavored drinks | 5.71 | 4.07 | −1.64 | 0.19 |
| (8.31) | (5.28) | (−4.11, 0.84) | ||
| Whole Milk | 4.77 | 3.56 | −1.21 | 0.35 |
| (6.92) | (5.27) | (−3.79, 1.36) | ||
| Reduced Fat Milk (2%) | 2.56 | 1.31 | −1.25 | 0.19 |
| (6.95) | (2.81) | (−3.14, 0.64) | ||
| Low Fat/Fat Free Milk (1%, Skim) | 3.28 | 3.56 | 0.28 | 0.84 |
| (6.27) | (5.83) | (−2.45, 3.01) | ||
| Soda | 2.77 | 1.32 | −1.45 | 0.11 |
| (5.62) | (2.77) | (−3.27, 0.36) | ||
| Diet Soda | 0.11 | 0.09 | −0.02 | 0.86 |
| (0.41) | (0.35) | (−0.22, 0.18) | ||
| Sweet Coffee/tea | 9.71 | 9.29 | −0.42 | 0.87 |
| (14.02) | (13.07) | (−5.49, 4.66) | ||
| Sports Drinks | 0.33 | 0.05 | −0.29 | 0.05 |
| (0.85) | (0.28) | (−0.57, 0.003) | ||
| Composite Sugar Sweetened Beverages 1 | 18.52 | 14.73 | −3.79 | 0.26 |
| (19.53) | (13.02) | (−10.48, 2.89) | ||
| Meta-Inference: Participants increased filtered tap water consumption after the intervention, and likely reduced added sugar to home-made drinks, in addition to reductions reported in the quantitative survey | 5.1: “Now I am no longer buying water and we don’t buy juice; we are saving a lot [of money]. I feel that it is healthier for me and my kids”. | |||
| 5.2: “I have noticed that because of the filter… [before I bought] up to 3 boxes [of water bottles]. Now I keep only one [box] because we use [water] from the tap… the filter serves me well, because I have it here and I use it”. | ||||
| 5.3: “…for example, before I drank coffee and abundant sugar, lots of sugar I noticed…’ | ||||
| 5.4: “and the coffee and what we love are the teas, I loved them with sugar, but right now I consume them but it’s not as much, I consume water first”. | ||||
| 5.5: “…now if it used to have one tablespoon, I put like one third of it”. | ||||
| Theme 6: Parental decisions and modeling in infant and toddler beverage consumption (n = 36) | ||||
| Survey Variable Beverage | Baseline Mean (SD) | Follow-up Mean (SD) | Mean Difference (95% CI) | p-value 3 |
| 2.04 | 9.08 | 7.04 | ||
| Tap Water (filtered) | (4.62) | (6.82) | (4.46, 9.61) | <0.001 |
| Bottled Water | 14.73 | |||
| (6.11) 7.20 | ||||
| (6.99) | ||||
| (7.52) | ||||
| (−10.75, −4.29) | ||||
| <0.001 | ||||
| 100% Fruit Juice | 6.48 | 3.58 | −2.89 | 0.002 |
| (5.13) | (3.17) | (−4.62, −1.18) | ||
| Fruit-flavored Drinks | 1.82 | 1.12 | −0.69 | 0.18 |
| (3.09) | (2.03) | (−1.74, 0.34) | ||
| Whole Milk | 9.58 | 7.69 | −1.89 | 0.17 |
| (8.72) | (8.23) | (−4.64, 0.86) | ||
| Reduced Fat Milk (2% | 1.2 | 1.42 | 0.22 | 0.7 |
| (3.3) | (3.92) | (−0.92, 1.35) | ||
| Low Fat/Fat Free Milk (1%, Skim) | 2.24 | 4.82 | 2.58 | 0.01 |
| (5.44) | (6.74) | (0.62, 4.54) | ||
| Flavored Milk | 1.19 | 0.29 | −0.9 | 0.13 |
| (3.89) | (1.2) | (−2.09, 0.29) | ||
| Soda | 0.23 | 0.31 | 0.08 | 0.53 |
| (0.88) | (1.2) | (−0.19, 0.35) | ||
| Diet Soda | 0 | 0 | 0 | NA |
| Sweet Tea/Coffee | 0.31 | 0.44 | 0.12 | 0.4 |
| (1.2) | (1.45) | (−0.17, 0.42) | ||
| Sports Drinks | 0.02 | 0.18 | 0.16 | 0.2 |
| −0.12 | −0.85 | (−0.09, 0.41) | ||
| Caffeinated Drinks | 0 | 0 | 0 | NA |
| Composite Sugar Sweetened Beverages 2 | 3.79 | 2.34 | −1.45 | 0.11 |
| (5.82) | (3.92) | (−3.27, 0.37) | ||
| Meta-Inference: Parents reported change in the types of beverages that children consume, and a potential mechanism for this change is the parents themselves engaging in the desired behavior, and modeling this behavior to their children, as well as the older children voicing their preference for the modeled behavior. | 6.1: “Before, I sometimes gave my child one or two juices. Now I almost never give him juice… I give him water”. | |||
| 6.2: “We did activities, like putting fruit in the water and drinking water together with my daughter, things like that, to encourage her to drink a little more water”. | ||||
| 6.3: “As a mom I go to the park… when the kids are playing and get thirsty, they ask for water. I carry water [with me], I don’t bring juices when I am with them”. | ||||
| 6.4: “…As a mother you eat or you feed the child, and the child looks at you and sees what you are doing, so then I also am practicing that I have to eat it so that they look at me, see me enjoying it (even if I don’t like it) […]grab my glass of water, and my youngest girl says to me: mami, water—because she sees me drinking water, and so then I feel happy because, really, it is something healthy for the life of my family”. | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCarley, S.; López-Ríos, M.; Burgos Gil, R.; Turner, M.M.; Cleary, S.D.; Edberg, M.; Colón-Ramos, U. Using a Community-Based Participatory Mixed Methods Research Approach to Develop, Evaluate, and Refine a Nutrition Intervention to Replace Sugary Drinks with Filtered Tap Water among Predominantly Central-American Immigrant Families with Infants and Toddlers: The Water Up @Home Pilot Evaluation Study. Nutrients 2021, 13, 2942. https://doi.org/10.3390/nu13092942
McCarley S, López-Ríos M, Burgos Gil R, Turner MM, Cleary SD, Edberg M, Colón-Ramos U. Using a Community-Based Participatory Mixed Methods Research Approach to Develop, Evaluate, and Refine a Nutrition Intervention to Replace Sugary Drinks with Filtered Tap Water among Predominantly Central-American Immigrant Families with Infants and Toddlers: The Water Up @Home Pilot Evaluation Study. Nutrients. 2021; 13(9):2942. https://doi.org/10.3390/nu13092942
Chicago/Turabian StyleMcCarley, Shannon, Mairyn López-Ríos, Rosalina Burgos Gil, Monique Mitchell Turner, Sean D. Cleary, Mark Edberg, and Uriyoán Colón-Ramos. 2021. "Using a Community-Based Participatory Mixed Methods Research Approach to Develop, Evaluate, and Refine a Nutrition Intervention to Replace Sugary Drinks with Filtered Tap Water among Predominantly Central-American Immigrant Families with Infants and Toddlers: The Water Up @Home Pilot Evaluation Study" Nutrients 13, no. 9: 2942. https://doi.org/10.3390/nu13092942