
Intraindividual Double Burden of Malnutrition in Chinese Children and Adolescents Aged 6–17 Years: Evidence from the China Health and Nutrition Survey 2015

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Dietary Micronutrient Intakes
2.3. Assessment of Overweight and Obesity
2.4. Defining Micronutrient Deficiency and Intraindividual DBM
2.5. Assessment of Covariates
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics and Intraindividual DBM
3.2. Disparity in Micronutrient Intake across Different Body Weight Status
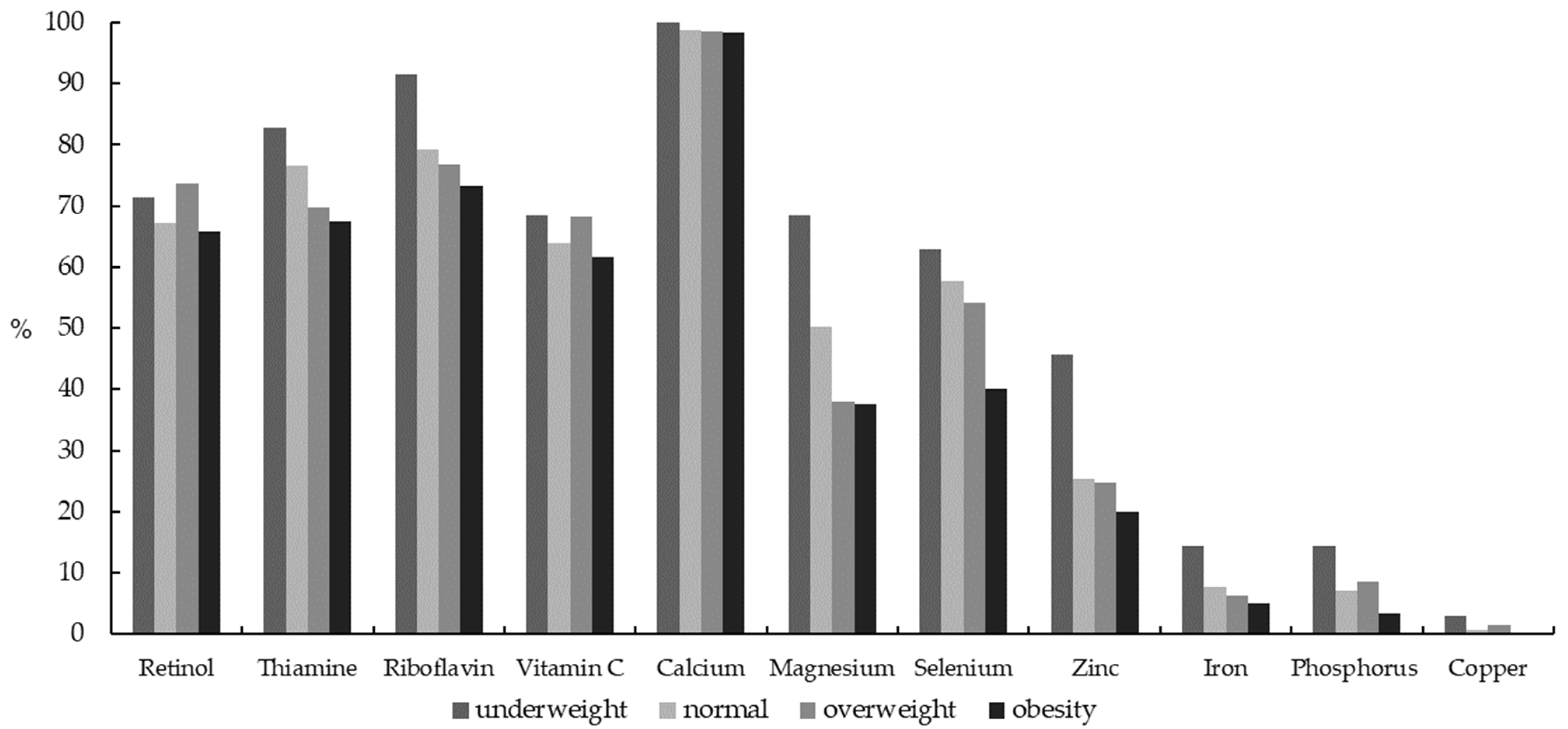
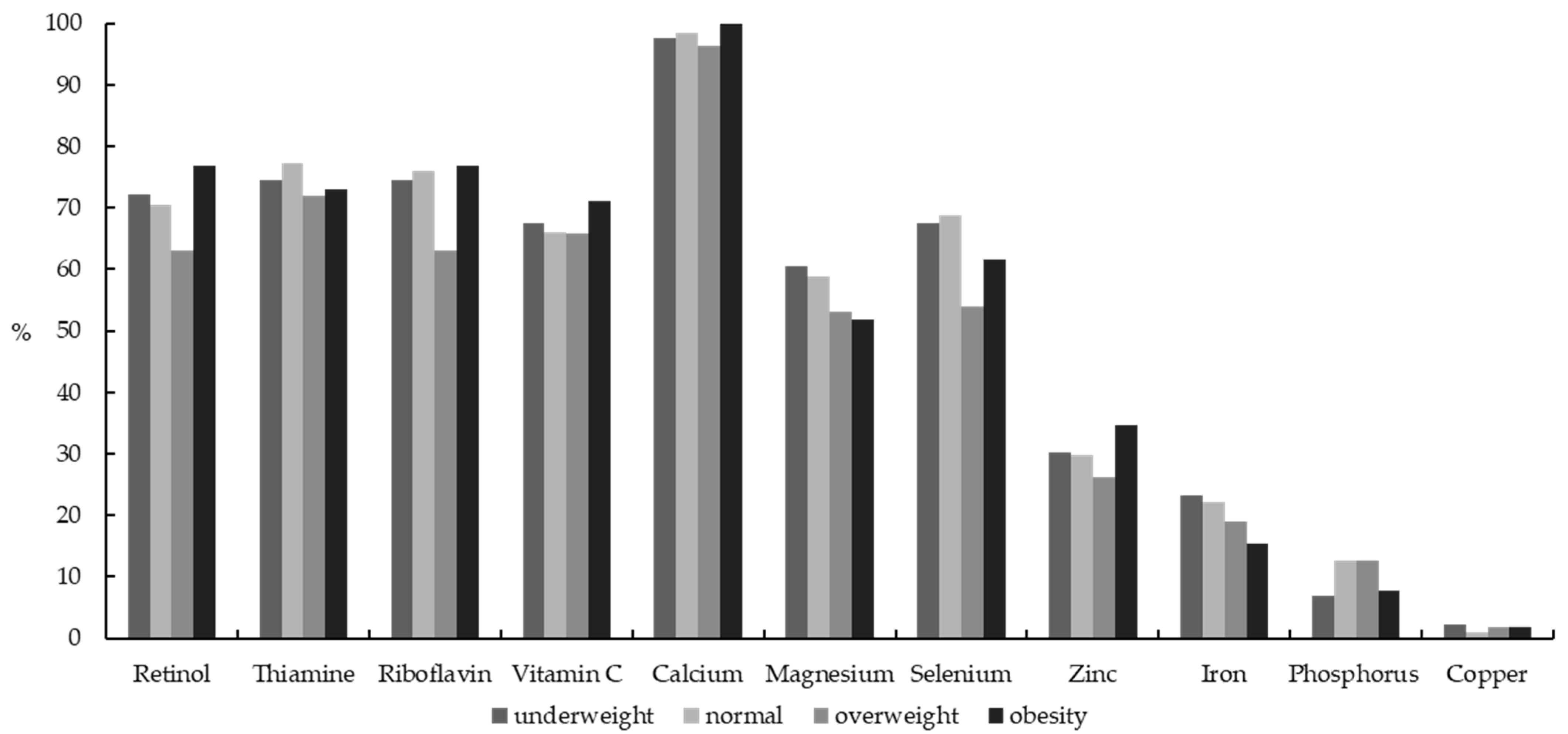
3.3. Disparity in Micronutrient Deficiency Status across Different Body Weight Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Development Initiatives. 2020 Global Nutrition Report: Action on Equity to End Malnutrition. 2020. Available online: https://globalnutritionreport.org/reports/global-nutrition-report-2020/ (accessed on 3 January 2021).
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- Barth-Jaeggi, T.; Zandberg, L.; Bahruddinov, M.; Kiefer, S.; Rahmarulloev, S.; Wyss, K. Nutritional status of Tajik children and women: Transition towards a double burden of malnutrition. Matern. Child Nutr. 2020, 16, e12886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Nguyen, B.K.; Le Thi, H.; Nguyen, D.V.; Tran, T.N.; Nguyen, H.C.; Thanh, D.T.; Deurenberg, P.; Khouw, I. Double burden of undernutrition and overnutrition in Vietnam in 2011: Results of the SEANUTS study in 0.5–11-year-old children. Br. J. Nutr. 2013, 110 (Suppl. 3), S45–S56. [Google Scholar]
- Adair, L.S.; Gordon-Larsen, P.; Du, S.F.; Zhang, B.; Popkin, B.M. The emergence of cardiometabolic disease risk in Chinese children and adults: Consequences of changes in diet, physical activity and obesity. Obes. Rev. 2014, 15 (Suppl. 1), 49–59. [Google Scholar] [PubMed]
- Dearth-Wesley, T.; Wang, H.; Popkin, B.M. Under- and overnutrition dynamics in Chinese children and adults (1991–2004). Eur. J. Clin. Nutr. 2008, 62, 1302–1307. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Xue, H.; Zhang, J.; Wang, Y. Time trend and demographic and geographic disparities in childhood obesity prevalence in china-evidence from twenty years of longitudinal data. Int. J. Environ. Res. Public Health 2017, 14, 369. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, H.; Wang, Z.; Du, W.; Su, C.; Zhang, J.; Jiang, H.; Jia, X.; Huang, F.; Ouyang, Y.; et al. Prevalence and stabilizing trends in overweight and obesity among children and adolescents in China, 2011–2015. BMC Public Health 2018, 18, 571. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Yin, X.; Wu, H.; Chai, X.; Yang, X. Trends in overweight and obesity among children and adolescents in China from 1991 to 2015: A meta-analysis. Int. J. Environ. Res. Public Health 2019, 16, 4656. [Google Scholar]
- Cui, Z.; Dibley, M.J. Trends in dietary energy, fat, carbohydrate and protein intake in Chinese children and adolescents from 1991 to 2009. Br. J. Nutr. 2012, 108, 1292–1299. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.H.; Zhai, F.Y.; Wang, H.J.; Zhang, J.G.; Du, W.W.; Su, C.; Zhang, J.; Jiang, H.R.; Zhang, B. Secular trends in meat and seafood consumption patterns among Chinese adults, 1991–2011. Eur. J. Clin. Nutr. 2015, 69, 227–233. [Google Scholar] [CrossRef]
- Wang, H.; Wang, D.; Ouyang, Y.; Huang, F.; Ding, G.; Zhang, B. Do chinese children get enough micronutrients? Nutrients 2017, 9, 397. [Google Scholar] [CrossRef]
- Mai, T.; Pham, N.O.; Tran, T.; Baker, P.; Gallegos, D.; Do, T.; van der Pols, J.C.; Jordan, S.J. The double burden of malnutrition in Vietnamese school-aged children and adolescents: A rapid shift over a decade in Ho Chi Minh City. Eur. J. Clin. Nutr. 2020, 74, 1448–1456. [Google Scholar] [CrossRef]
- Zhou, S.; Ye, B.; Fu, P.; Li, S.; Yuan, P.; Yang, L.; Zhan, X.; Chao, F.; Zhang, S.; Wang, M.Q.; et al. Double burden of malnutrition: Examining the growth profile and coexistence of undernutrition, overweight, and obesity among school-aged children and adolescents in urban and rural counties in Henan Province, China. J. Obes. 2020, 2020, 2962138. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort profile: The China health and nutrition survey—Monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- WHO Child Growth Standards: Length/Height-for Age Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; WHO Multicenter Growth Reference Study Group: Geneva, Switzerland, 2006.
- Jones-Smith, J.C.; Popkin, B.M. Understanding community context and adult health changes in China: Development of an urbanicity scale. Soc. Sci. Med. 2010, 71, 1436–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinese Dietary Reference Intakes—Part 3: Trace Element; National Health Commission of People’s Republic of China: Beijing, China, 2017.
- Chinese Dietary Reference Intakes—Part 4: Lipid-Soluble Vitamin; National Health Commission of People’s Republic of China: Beijing, China, 2018.
- Chinese Dietary Reference Intakes—Part 5: Water-Soluble Vitamin; National Health Commission of People’s Republic of China: Beijing, China, 2018.
- Huang, Q.; Wang, L.; Jiang, H.; Wang, H.; Zhang, B.; Zhang, J.; Jia, X.; Wang, Z. Intra-individual double burden of malnutrition among adults in China: Evidence from the China Health and Nutrition Survey 2015. Nutrients 2020, 12, 2811. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, H.; Wang, Z.; Zhang, J.; Du, W.; Su, C.; Jiang, H.; Zhai, F.; Zhang, B. Trend in dietary calcium intake among Chinese children and adolescents aged 4 to 17 years in nine provinces from 1991 to 2009. Zhonghua Liu Xing Bing Xue Za Zhi 2013, 34, 857–862. [Google Scholar]
- Zhang, J.; Zhang, B.; Wang, H.; Wang, Z.; Zhang, J.; Zhai, F. Nutrients intake trend of Chinese population in nine provinces from 1991 to 2009 (X) zinc intake trend of Chinese children aged 7–17 years. Acta Nutr. 2013, 35, 131–133. [Google Scholar]
- Wang, Z.; Zhang, B.; Wang, H.; Zhang, J.; Du, W.; Su, C.; Zhang, J.; Zhai, F. Trend in dietary vitamin C intake among Chinese children and adolescents between 1991 and 2009. Zhonghua Yu Fang Yi Xue Za Zhi 2012, 46, 1069–1073. [Google Scholar]
- Wang, X.; Su, C.; Ouyang, Y.; Li, W.; Zhang, B.; Wang, H. Trends of the Chinese in dietary pattern of children and adolescents in communities at different urbanization levels. Acta Nutr. 2016, 38, 119–123. [Google Scholar]
- Su, C.; Wang, H.; Wang, Z.; Zhang, J.; Du, W.; Zhang, J.; Zhai, F.; Zhang, B. Current status and trends of both dietary fat and cholesterol intake among Chinese children and adolescents aged 7 to 17 years old in 9 provinces of China, from 1991 to 2009. Zhonghua Liu Xing Bing 2012, 12, 1208–1212. [Google Scholar]
- Closa-Monasterolo, R.; Zaragoza-Jordana, M.; Ferre, N.; Luque, V.; Grote, V.; Koletzko, B.; Verduci, E.; Vecchi, F.; Escribano, J. Adequate calcium intake during long periods improves bone mineral density in healthy children. Data from the Childhood Obesity Project. Clin. Nutr. 2018, 37, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.; Zhang, C.; Yao, X.; Zhu, Z. Association between dietary calcium intake and BMD in children and adolescents. Endocr. Connect. 2020, 9, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Skinner, J.D.; Bounds, W.; Carruth, B.R.; Ziegler, P. Longitudinal calcium intake is negatively related to children’s body fat indexes. J. Am. Diet Assoc. 2003, 103, 1626–1631. [Google Scholar] [PubMed]
- Davies, K.M.; Heaney, R.P.; Recker, R.R.; Lappe, J.M.; Barger-Lux, M.J.; Rafferty, K.; Hinders, S. Calcium intake and body weight. J. Clin. Endocrinol. Metab. 2000, 85, 4635–4638. [Google Scholar] [PubMed] [Green Version]
- He, Y.; Yang, X.; Xia, J.; Zhao, L.; Yang, Y. Consumption of meat and dairy products in China: A review. Proc. Nutr. Soc. 2016, 75, 385–391. [Google Scholar] [PubMed] [Green Version]
- He, Y.; Fang, Y.; Yang, Y. Whole grains and mixed beans intake among Chinese adolescents aged 6–17 years. Acta Nutr. 2019, 41, 220–224. [Google Scholar]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar]
- Chung, S.J.; Ersig, A.L.; McCarthy, A.M. The influence of peers on diet and exercise among adolescents: A systematic review. J. Pediatr. Nurs. 2017, 36, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Black, M.M. Micronutrient deficiencies and cognitive functioning. J. Nutr. 2003, 133, 3927S–3931S. [Google Scholar] [CrossRef] [Green Version]
- Meng, L.; Wang, Y.; Li, T.; Loo-Bouwman, C.; Zhang, Y.; Man-Yau, S.I. Dietary diversity and food variety in Chinese children aged 3–17 years: Are they negatively associated with dietary micronutrient inadequacy? Nutrients 2018, 10, 1674. [Google Scholar] [CrossRef] [Green Version]
- Du, W.; Wang, H.; Wang, D.; Su, C.; Zhang, J.; Ouyang, Y.; Jia, X.; Huang, F.; Zhang, B. Meal and snack consumption among Chinese children and adolescents in twelve provinces. Wei Sheng Yan Jiu 2016, 45, 876–905. [Google Scholar]

{kind=link}
{kind=link}
| Characteristics | Participants | Underweight | Overweight | Obesity | Underweight and Micronutrient Deficiency | Overweight/Obesity and Micronutrient Deficiency | UMD% 2 | OMD% 3 |
|---|---|---|---|---|---|---|---|---|
| Number of subjects | 1555 (100.0) | 78 (5.02) | 240 (15.43) | 172 (11.06) | 77 (4.95) | 408 (26.24) | 77 (98.72) | 408 (99.03) |
| Sex | ||||||||
| Boys | 806 (51.83) | 35 (4.34) | 129 (16.00) | 120 (14.89) c | 35 (4.34) | 247 (30.65) | 35 (100.00) | 247 (99.20) |
| Girls | 749 (48.17) | 43 (5.74) | 111 (14.82) | 52 (6.94) | 42 (5.61) | 161 (21.50) | 42 (97.67) | 161 (98.77) |
| Age (year) | ||||||||
| 6–10 | 858 (55.18) | 41 (4.78) | 128 (14.92) | 111 (12.94) c, t | 40 (4.66) | 236 (27.51) | 40 (97.56) | 236 (98.74) |
| 11–13 | 417 (26.82) | 23 (5.52) | 75 (17.99) | 39 (9.35) | 23 (5.52) | 114 (27.34) | 23 (100.00) | 114 (100.00) |
| 14–17 | 280 (18.01) | 14 (5.00) | 37 (13.21) | 22 (7.86) | 14 (5.00) | 58 (20.71) | 14 (100.00) | 58 (98.31) |
| Urban and rural | ||||||||
| Urban | 499 (32.09) | 21 (4.21) | 94 (18.84) c | 63 (12.63) | 21 (4.21) | 154 (30.86) | 21 (100.00) | 154 (98.09) |
| Rural | 1056 (67.91) | 57 (5.40) | 146 (13.83) | 109 (10.32) | 56 (5.30) | 254 (24.05) | 56 (98.25) | 254 (99.61) |
| Yearly Income | ||||||||
| Low | 519 (33.38) | 34 (6.55) t | 65 (12.52) c, t | 44 (8.48) | 34 (6.55) | 109 (21.00) | 34 (100.00) | 109 (100.00) |
| Medium | 518 (33.31) | 24 (4.63) | 72 (13.90) | 60 (11.58) | 24 (4.63) | 131 (25.29) | 24 (100.00) | 131 (99.24) |
| High | 518 (33.31) | 20 (3.86) | 103 (19.88) | 68 (13.13) | 19 (3.67) | 168 (32.43) | 19 (95.00) | 168 (98.25) |
| Urbanicity index | ||||||||
| Low | 521 (33.50) | 27 (5.18) | 61 (11.71) c, t | 47 (9.02) | 27 (5.18) | 108 (20.73) | 27 (100.00) | 108 (100.00) |
| Medium | 516 (33.18) | 27 (5.23) | 89 (17.25) | 62 (12.02) | 27 (5.23) | 150 (29.07) | 27 (100.00) | 150 (99.34) |
| High | 518 (33.31) | 24 (4.63) | 90 (17.37) | 63 (12.16) | 23 (4.44) | 150 (28.96) | 23 (95.83) | 150 (98.04) |
| Micronutrient | Underweight | Normal | Overweight | Obesity |
|---|---|---|---|---|
| Retinol (µg RAE) | 614.72 ± 148.56 | 487.93 ± 38.39 | 421.42 ± 77.23 | 434.25 ± 81.14 |
| Thiamine (mg) | 0.68 ± 0.06 a | 0.76 ± 0.02 | 0.81 ± 0.03 | 0.83 ± 0.03 b |
| Riboflavin (mg) | 0.64 ± 0.06 a | 0.71 ± 0.02 a, c | 0.78 ± 0.03 b | 0.76 ± 0.03 |
| Vitamin C (mg) | 57.35 ± 36.77 | 60.54 ± 9.50 a | 54.33 ± 19.12 a, b | 114.08 ± 19.84 c |
| Calcium (mg) | 308.82 ± 28.78 | 317.65 ± 7.44 a | 356.67 ± 14.96 b | 348.70 ± 15.52 |
| Phosphorus (mg) | 744.83 ± 48.75 a | 799.88 ± 12.60 a, d | 882.21 ± 25.34 b | 903.73 ± 26.30 b, c |
| Magnesium (mg) | 224.24 ± 15.84 | 220.69 ± 4.09 a | 236.94 ± 8.23 | 243.82 ± 8.55 b |
| Iron (mg) | 17.49 ± 1.78 | 19.15 ± 0.46 | 21.03 ± 0.93 | 20.36 ± 0.96 |
| Zinc (mg) | 8.12 ± 0.58 a | 9.02 ± 0.15 a, c, d | 9.83 ± 0.30 b | 9.70 ± 0.31 b, c |
| Copper (mg) | 1.46 ± 0.15 | 1.48 ± 0.04 | 1.49 ± 0.08 | 1.54 ± 0.08 |
| Selenium (µg) | 37.92 ± 3.71 a, d | 39.13 ± 0.96 a, c | 44.25 ± 1.93 b, d | 47.29 ± 2.00 b |
| Micronutrient | Underweight | Normal | Overweight | Obesity |
|---|---|---|---|---|
| Retinol (µg RAE) | 313.19 ± 123.83 | 426.06 ± 34.84 | 479.71 ± 77.00 | 293.56 ± 113.08 |
| Thiamine (mg) | 0.67 ± 0.05 | 0.70 ± 0.01 | 0.73 ± 0.03 | 0.68 ± 0.05 |
| Riboflavin (mg) | 0.65 ± 0.05 | 0.67 ± 0.01 a | 0.75 ± 0.03 b | 0.64 ± 0.05 |
| Vitamin C (mg) | 52.88 ± 14.83 | 61.10 ± 4.17 | 63.44 ± 9.22 | 49.22 ± 13.54 |
| Calcium (mg) | 287.27 ± 29.32 | 306.36 ± 8.24 | 336.00 ± 18.23 | 328.41 ± 26.77 |
| Phosphorus (mg) | 734.00 ± 43.44 | 750.82 ± 12.22 a | 815.52 ± 27.01 b | 746.40 ± 39.67 |
| Magnesium (mg) | 199.69 ± 15.68 | 214.05 ± 4.41 | 214.36 ± 9.75 | 208.69 ± 14.32 |
| Iron (mg) | 16.54 ± 1.58 | 17.81 ± 0.44 | 18.34 ± 0.98 | 17.97 ± 1.44 |
| Zinc (mg) | 8.28 ± 0.53 | 8.51 ± 0.15 | 8.85 ± 0.33 | 7.92 ± 0.49 |
| Copper (mg) | 1.26 ± 0.12 | 1.39 ± 0.03 | 1.43 ± 0.08 | 1.26 ± 0.11 |
| Selenium (µg) | 35.17 ± 3.14 | 36.24 ± 0.88 a | 41.14 ± 1.95 b | 35.68 ± 2.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, X.; Jiang, H.; Wang, H.; Zhang, B.; Zhang, J.; Jia, X.; Wang, L.; Wang, Z.; Ding, G. Intraindividual Double Burden of Malnutrition in Chinese Children and Adolescents Aged 6–17 Years: Evidence from the China Health and Nutrition Survey 2015. Nutrients 2021, 13, 3097. https://doi.org/10.3390/nu13093097
Hu X, Jiang H, Wang H, Zhang B, Zhang J, Jia X, Wang L, Wang Z, Ding G. Intraindividual Double Burden of Malnutrition in Chinese Children and Adolescents Aged 6–17 Years: Evidence from the China Health and Nutrition Survey 2015. Nutrients. 2021; 13(9):3097. https://doi.org/10.3390/nu13093097
Chicago/Turabian StyleHu, Xiao, Hongru Jiang, Huijun Wang, Bing Zhang, Jiguo Zhang, Xiaofang Jia, Liusen Wang, Zhihong Wang, and Gangqiang Ding. 2021. "Intraindividual Double Burden of Malnutrition in Chinese Children and Adolescents Aged 6–17 Years: Evidence from the China Health and Nutrition Survey 2015" Nutrients 13, no. 9: 3097. https://doi.org/10.3390/nu13093097