
Eating Slowly Is Associated with Undernutrition among Community-Dwelling Adult Men and Older Adult Women

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
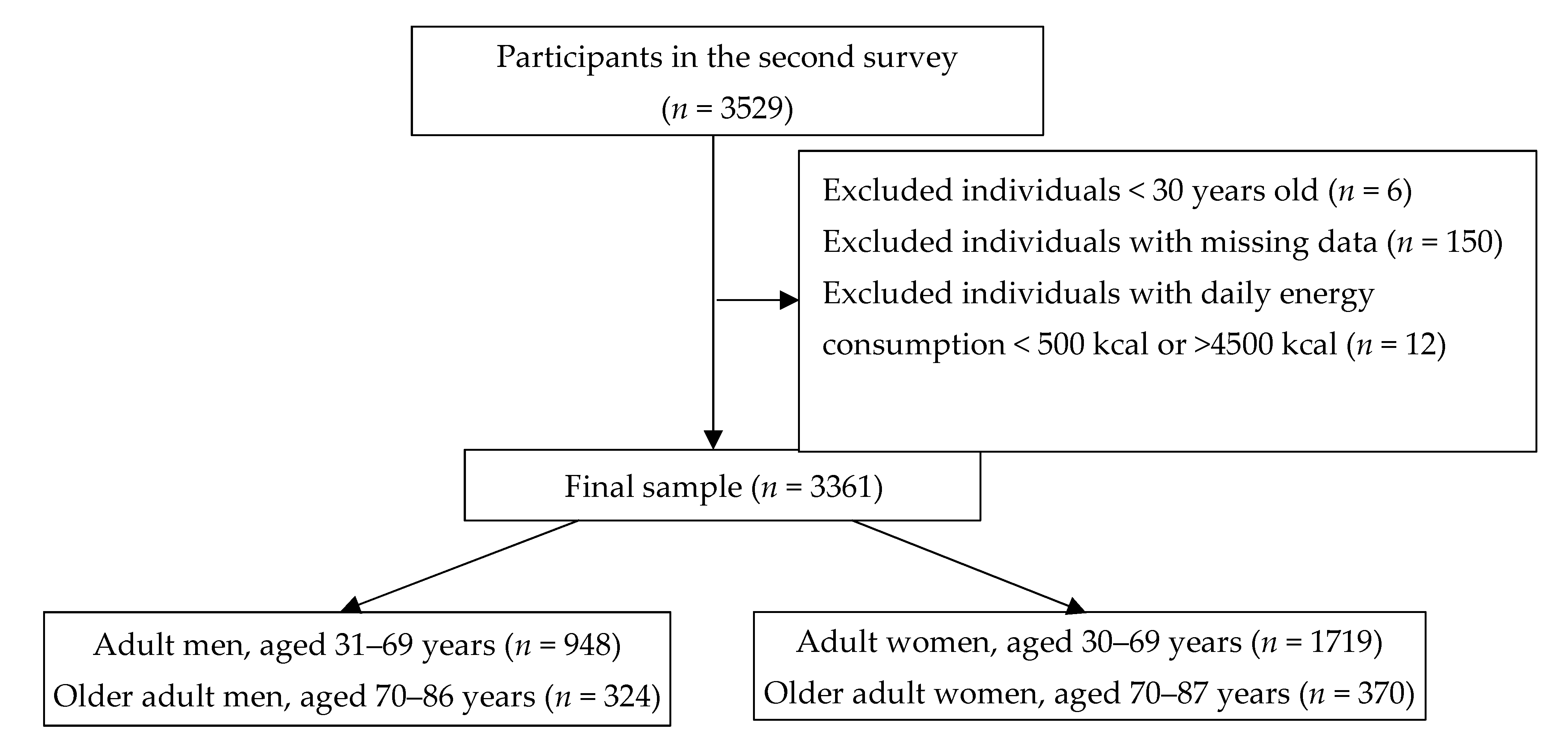
2.2. Study Population
2.3. Questionnaire and Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. The Double Burden of Malnutrition. Available online: https://apps.who.int/iris/bitstream/handle/10665/255413/WHO-NMH-NHD-17.3-eng.pdf (accessed on 31 October 2021).
- Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration (BMI Mediated Effects); Lu, Y.; Hajifathalian, K.; Ezzati, M.; Woodward, M.; Rimm, E.B.; Danaei, G. Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: A pooled analysis of 97 prospective cohorts with 1.8 million participants. Lancet 2014, 383, 970–983. [Google Scholar] [PubMed] [Green Version]
- Amarya, S.; Singh, K.; Sabharwal, M. Changes during aging and their association with malnutrition. J. Clin. Gerontol. Geriatr. 2015, 6, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Norman, K.; Haß, U.; Pirlich, M. Malnutrition in older adults-recent advances and remaining challenges. Nutrients 2021, 13, 2764. [Google Scholar] [CrossRef] [PubMed]
- Bardon, L.A.; Corish, C.A.; Lane, M.; Bizzaro, M.G.; Loayza Villarroel, K.; Clarke, M.; Power, L.C.; Gibney, E.R.; Dominguez Castro, P. Ageing rate of older adults affects the factors associated with, and the determinants of malnutrition in the community: A systematic review and narrative synthesis. BMC Geriatr. 2021, 21, 676. [Google Scholar] [CrossRef]
- Fatyga, P.; Pac, A.; Fedyk-Łukasik, M.; Grodzicki, T.; Skalska, A. The relationship between malnutrition risk and inflammatory biomarkers in outpatient geriatric population. Eur. Geriatr. Med. 2020, 11, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Mastronuzzi, T.; Paci, C.; Portincasa, P.; Montanaro, N.; Grattagliano, I. Assessing the nutritional status of older individuals in family practice: Evaluation and implications for management. Clin. Nutr. 2015, 34, 1184–1188. [Google Scholar] [CrossRef]
- Giezenaar, C.; Chapman, I.; Luscombe-Marsh, N.; Feinle-Bisset, C.; Horowitz, M.; Soenen, S. Ageing is associated with decreases in appetite and energy intake—A meta-analysis in healthy adults. Nutrients 2016, 8, 28. [Google Scholar] [CrossRef] [Green Version]
- Chatindiara, I.; Sheridan, N.; Kruger, M.; Wham, C. Eating less the logical thing to do? Vulnerability to malnutrition with advancing age: A qualitative study. Appetite 2020, 146, 104502. [Google Scholar] [CrossRef]
- van der Pols-Vijlbrief, R.; Wijnhoven, H.A.; Schaap, L.A.; Terwee, C.B.; Visser, M. Determinants of protein-energy malnutrition in community-dwelling older adults: A systematic review of observational studies. Ageing Res. Rev. 2014, 18, 112–131. [Google Scholar] [CrossRef]
- Nazri, N.S.; Vanoh, D.; Leng, S.K. Malnutrition, low diet quality and its risk factors among older adults with low socio-economic status: A scoping review. Nutr. Res. Rev. 2021, 34, 107–116. [Google Scholar] [CrossRef]
- Kitamura, K.; Watanabe, Y.; Nakamura, K.; Takahashi, A.; Takachi, R.; Oshiki, R.; Kobayashi, R.; Saito, T.; Tsugane, S.; Sasaki, A. Weight loss from 20 years of age is associated with cognitive impairment in middle-aged and elderly individuals. PLoS ONE 2017, 12, e0185960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanri, A.; Mizoue, T.; Takahashi, Y.; Noda, M.; Inoue, M.; Tsugane, S. Japan public health center- based prospective study group. Weight change and all-cause, cancer and cardiovascular disease mortality in Japanese men and women: The Japan public health center-based prospective study. Int. J. Obes. 2010, 34, 348–356. [Google Scholar] [CrossRef] [Green Version]
- Yoon, K.H.; Lee, J.H.; Kim, J.W.; Cho, J.H.; Choi, Y.H.; Ko, S.H.; Zimmet, P.; Son, H.Y. Epidemic obesity and type 2 diabetes in Asia. Lancet 2006, 368, 1681–1688. [Google Scholar] [CrossRef]
- Colosia, A.D.; Palencia, R.; Khan, S. Prevalence of hypertension and obesity in patients with type 2 diabetes mellitus in observational studies: A systematic literature review. Diabetes Metab. Syndr. Obes. 2013, 6, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crichton, M.; Craven, D.; Mackay, H.; Marx, W.; de van der Schueren, M.; Marshall, S. A systematic review, meta-analysis and meta-regression of the prevalence of protein-energy malnutrition: Associations with Geographical Region and Sex. Age Ageing 2019, 48, 38–48. [Google Scholar] [CrossRef]
- East-West Center. Asia’s Aging Population. Available online: https://www.eastwestcenter.org/sites/default/files/fileadmin/stored/misc/FuturePop08Aging.pdf (accessed on 31 October 2021).
- Ministry of Health, Labour and Welfare Japan. National Health and Nutrition Survey in 2019. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/eiyou/r1-houkoku_00002.html (accessed on 31 October 2021).
- Saunders, J.; Smith, T. Malnutrition: Causes and consequences. Clin. Med. 2010, 10, 624–627. [Google Scholar] [CrossRef]
- Streicher, M.; van Zwienen-Pot, J.; Bardon, L.; Nagel, G.; The, R.; Meisinger, C.; Colombo, M.; Torbahn, G.; Kiesswetter, E.; Flechtner-Mors, M.; et al. Determinants of incident malnutrition in community-dwelling older adults: A MaNuEL multicohort meta-analysis. J. Am. Geriatr. Soc. 2018, 66, 2335–2343. [Google Scholar] [CrossRef] [Green Version]
- Robinson, E.; Almiron-Roig, E.; Rutters, F.; de Graaf, C.; Forde, C.G.; Tudur Smith, C.; Nolan, S.J.; Jebb, S.A. A systematic review and meta-analysis examining the effect of eating rate on energy intake and hunger. Am. J. Clin. Nutr. 2014, 100, 123–151. [Google Scholar] [CrossRef] [Green Version]
- Shiga University of Medical Science, Takashima Cohort Study. Available online: https://www.shiga-med.ac.jp/hqcera/project/takashima_study/takashima_cohort/zenkokugan.html (accessed on 10 December 2021).
- Takashima, N.; Turin, T.C.; Matsui, K.; Rumana, N.; Nakamura, Y.; Kadota, A.; Saito, Y.; Sugihara, H.; Morita, Y.; Ichikawa, M.; et al. The relationship of brachial-ankle pulse wave velocity to future cardiovascular disease events in the general Japanese population: The Takashima study. J. Hum. Hypertens. 2014, 28, 323–327. [Google Scholar] [CrossRef]
- Kita, Y.; Turin, T.C.; Rumana, N.; Sugihara, H.; Morita, Y.; Hirose, K.; Okayama, A.; Nakamura, Y.; Ueshima, H. Takashima stroke registry. surveillance and measuring trends of stroke in Japan: The Takashima stroke registry (1988–Present). Int. J. Stroke 2007, 2, 129–132. [Google Scholar] [CrossRef]
- Turin, T.C.; Kita, Y.; Rumana, N.; Takashima, N.; Kadota, A.; Matsui, K.; Sugihara, H.; Morita, Y.; Nakamura, Y.; Miura, K.; et al. Brachial-ankle pulse wave velocity predicts all-cause mortality in the general population: Findings from the Takashima Study, Japan. Hypertens. Res. 2010, 33, 922–925. [Google Scholar] [CrossRef] [Green Version]
- Matsui, K.; Kita, Y. Why do people consent to participate in genetic epidemiological studies? Jpn. J. Public Health 2010, 57, 977–987. [Google Scholar]
- Shiga Prefecture. Report on the "Shiga Health and Nutrition Map Survey" in 2015. Available online: https://www.pref.shiga.lg.jp/ippan/kenkouiryouhukushi/kenkou/15050.html (accessed on 10 March 2021).
- Misawa, A.; Yoshita, K.; Fukumura, T.; Tanaka, T.; Tamaki, J.; Takebayashi, T.; Kusaka, Y.; Nakagawa, H.; Yamato, H.; Okayama, A.; et al. Effects of a long-term intervention in a work cafeteria on employee vegetable intake. J. Occup. Health 2015, 57, 97–107. [Google Scholar]
- Japanese Association for Nutritional Assessment (JARD). New standard values of physical measurements for Japanese (JARD 2001). Nutr. Assess. Nutr. 2002, 19, 1–81. [Google Scholar]
- Outline of the Establishment of Takashima Health Promotion Staff. Available online: http://www.city.takashima.lg.jp/reiki/reiki_honbun/r152RG00000551.html (accessed on 10 December 2021).
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Japan Society for the Study of Obesity. Available online: http://www.jasso.or.jp/contents/english/index.html (accessed on 1 March 2020).
- The Japanese Society of Cardiovascular Disease Prevention. Cardiovascular Disease Prevention Handbook, 6th ed.; Hokendoujinsha: Tokyo, Japan, 2003. [Google Scholar]
- The Japanese Society of Hypertension. Hypertension for the Management Guidelines 6. Available online: https://www.jpnsh.jp/data/jsh2019/JSH2019_hp.pdf (accessed on 31 March 2019). (In Japanese).
- Kinoshita, M.; Yokote, K.; Arai, H.; Iida, M.; Ishigaki, Y.; Ishibashi, S.; Umemoto, S.; Egusa, G.; Ohmura, H.; Okamura, T.; et al. Committee for epidemiology and clinical management of atherosclerosis. Japan Atherosclerosis Society (JAS) guidelines for prevention of atherosclerotic cardiovascular diseases 2017. J Atheroscler. Thromb. 2018, 25, 846–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Imai, T.; Miyamoto, K.; Sezaki, A.; Kawase, F.; Shirai, Y.; Abe, C.; Fukaya, A.; Kato, T.; Sanada, M.; Shimokata, H. Traditional Japanese Diet Score—Association with obesity, incidence of ischemic heart disease, and healthy life expectancy in a global comparative study. J. Nutr. Health Aging 2019, 23, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Toyomitsu, M.; Ogawa, H.; Matsumoto, N. Comparison of preference for foods of younger generations and older person−3 generation family and 2 generation family. J. Integr. Stud. Diet. Habits 2004, 14, 289–297. [Google Scholar] [CrossRef]
- Otsuka, R.; Tamakoshi, K.; Yatsuya, H.; Wada, K.; Matsushita, K.; OuYang, P.; Hotta, Y.; Takefuj, S.; Mitsuhashi, H.; Sugiura, K.; et al. Eating fast leads to insulin resistance: Findings in middle-aged Japanese men and women. Prev. Med. 2008, 46, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, B.L.; Lissner, L. Overvaegtige fejlbedømmer deres kostindtag—Hvilke naeringsstoffer underrapporteres? Ugeskr. Laeger 1996, 158, 6902–6906. [Google Scholar] [PubMed]
- Miyazawa, I.; Morino, K.; Fuse, K.; Kondo, K.; Ohi, A.; Nishida, K.; Kurihara, M.; Yasuhara, S.; Nakanishi, N.; Nishida, Y.; et al. Impact of obesity on underreporting of energy intake in type 2 diabetic patients: Clinical evaluation of energy requirements in patients with diabetes mellitus (CLEVER-DM) study. Clin. Nutr. ESPEN 2020, 39, 251–254. [Google Scholar] [CrossRef]
- Reddy, N.L.; Peng, C.; Carreira, M.C.; Halder, L.; Hattersley, J.; Piya, M.K.; Tripathi, G.; Randeva, H.S.; Casanueva, F.F.; McTernan, P.G.; et al. Enhanced thermic effect of food, postprandial NEFA suppression and raised adiponectin in obese women who eat slowly. Clin. Endocrinol. 2015, 82, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Kokkinos, A.; le Roux, C.W.; Alexiadou, K.; Tentolouris, N.; Vincent, R.P.; Kyriaki, D.; Perrea, D.; Ghatei, M.A.; Bloom, S.R.; Katsilambros, N. Eating slowly increases the postprandial response of the anorexigenic gut hormones, peptide YY and glucagon-like peptide-1. J. Clin. Endocrinol. Metab. 2010, 95, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Shin, W.S. Differences in eating behaviors and masticatory performances by gender and obesity status. Physiol. Behav. 2015, 138, 69–74. [Google Scholar] [CrossRef]
- Kalra, S.; Unnikrishnan, A.G.; Baruah, M.P.; Sahay, R.; Bantwal, G. Metabolic and energy imbalance in dysglycemia-based chronic disease. Diabetes Metab. Syndr. Obes. 2021, 14, 165–184. [Google Scholar] [CrossRef]
- Yaguchi-Tanaka, Y.; Ishikawa, H.; Shao, L.; Sasaki, S.; Fukao, A. Association between smoking and nutrition and food group intakes among community-dwelling Japanease adults. J. Jpn. Soc. Nutr. Food Sci. 2011, 64, 159–167. [Google Scholar] [CrossRef]
- Hozawa, A.; Hirata, T.; Yatsuya, H.; Murakami, Y.; Kuriyama, S.; Tsuji, I.; Sugiyama, D.; Satoh, A.; Tanaka-Mizuno, S.; Miura, K.; et al. Association between body mass index and all-cause death in Japanese population: Pooled individual participant data analysis of 13 cohort studies. J. Epidemiol. 2019, 29, 457–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochiai, H.; Shirasawa, T.; Nanri, H.; Nishimura, R.; Hoshino, H.; Kokaze, A. Relationship between eating quickly and overweight: A cohort study of schoolchildren in Japan. Acta. Med. Okayama 2018, 72, 121–128. [Google Scholar] [PubMed]
- Fagerberg, P.; Charmandari, E.; Diou, C.; Heimeier, R.; Karavidopoulou, Y.; Kassari, P.; Koukoula, E.; Lekka, I.; Maglaveras, N.; Maramis, C.; et al. Fast eating is associated with increased BMI among high-school students. Nutrients 2021, 13, 880. [Google Scholar] [CrossRef]
- Wuren, M.A.; Endoh, K.; Kuriki, K.; Shizuoka-Sakuragaoka J-MICC Study group. Eating rate as risk for body mass index and waist circumference obesity with appropriate confounding factors: A cross-sectional analysis of the Shizuoka-Sakuragaoka J-MICC Study. Asia. Pac. J. Clin. Nutr. 2019, 28, 79–91. [Google Scholar]
- Jayne, J.M.; Karl, J.P.; McGraw, S.M.; O’Connor, K.; Di Chiara, A.J.; Cole, R.E. Eating behaviors are associated with physical fitness and body composition among US army soldiers. J. Nutr. Educ. Behav. 2021, 53, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Cox, N.J.; Ibrahim, K.; Sayer, A.A.; Robinson, S.M.; Roberts, H.C. Assessment and treatment of the anorexia of aging: A systematic review. Nutrients 2019, 11, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, S.; Katagiri, A.; Tsuji, T.; Shimoda, T.; Amano, K. Self-reported rate of eating correlates with body mass index in 18-y-old Japanese women. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1405–1410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, K.; Sato, S.; Ohira, T.; Maeda, K.; Noda, H.; Kubota, Y.; Nishimura, S.; Kitamura, A.; Kiyama, M.; Okada, T.; et al. The joint impact on being overweight of self reported behaviours of eating quickly and eating until full: Cross sectional survey. BMJ 2008, 337, a2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Eating Speed | Fast | Moderate | Slow | p | p for Trend | |||
|---|---|---|---|---|---|---|---|---|
| Adult men (31–69 years) | ||||||||
| n (%) | 395 | (41.7%) | 443 | (46.7%) | 110 | (11.6%) | ||
| Age (years) | 57.8 | (10.0) | 59.9 | (10.0) | 62.3 | (7.4) | <0.001 | <0.001 |
| Body weight (kg) | 69.1 | (10.5) | 64.4 | (9.4) | 61.7 | (9.3) | <0.001 | <0.001 |
| BMI (kg/m2) | 24.4 | (3.1) | 23.2 | (2.8) | 22.5 | (2.7) | <0.0 1 | <0.001 |
| Body weight at age 20 years (kg) | 21.6 | (2.3) | 21.6 | (3.2) | 21.2 | (2.4) | <0.001 | <0.001 |
| Body-weight change (kg) | 2.7 | (2.8) | 1.7 | (3.0) | 1.3 | (2.8) | <0.001 | <0.001 |
| Energy intake (kcal/day) | 2228 | (706) | 2216 | (675) | 2287 | (757) | 0.781 | 0.812 |
| Habit of exercise, yes, n (%) | 183 | (46.3%) | 204 | (46.0%) | 54 | (49.1%) | 0.845 | 0.726 |
| Habit of smoking, yes, n (%) | 106 | (26.8%) | 142 | (32.1%) | 35 | (31.8%) | 0.229 | 0.133 |
| Habit of drinking, yes, n (%) | 277 | (70.1%) | 322 | (72.7%) | 89 | (80.9%) | 0.081 | 0.039 |
| Hypertension, n (%) | 104 | (26.3%) | 120 | (27.1%) | 29 | (26.4%) | 0.966 | 0.883 |
| Dyslipidemia, n (%) | 138 | (34.9%) | 125 | (28.2%) | 26 | (23.6%) | 0.027 | 0.004 |
| Diabetes, n (%) | 43 | (10.9%) | 33 | (7.4%) | 6 | (5.5%) | 0.094 | 0.028 |
| Cancer, n (%) | 8 | (2.0%) | 14 | (3.2%) | 9 | (8.2%) | 0.006 | 0.021 |
| Myocardial infarction, n (%) | 9 | (2.3%) | 5 | (1.1%) | - | - | - | - |
| Cerebrovascular disease, n (%) | 8 | (2.0%) | 13 | (2.9%) | 3 | (2.7%) | 0.152 | 0.044 |
| Older adult men (70–86 years) | ||||||||
| n (%) | 102 | (31.5%) | 162 | (50.0%) | 60 | (18.5%) | ||
| Age (years) | 72.9 | (2.4) | 73.0 | (2.5) | 73.1 | (3.2) | 0.844 | 0.815 |
| Body weight (kg) | 59.1 | (8.2) | 57.7 | (6.4) | 57.6 | (7.0) | 0.668 | 0.453 |
| BMI (kg/m2) | 24.1 | (2.5) | 23.0 | (2.7) | 22.5 | (2.6) | <0.001 | <0.001 |
| Body weight at age 20 years (kg) | 69.1 | (10.5) | 64.4 | (9.4) | 61.7 | (9.3) | <0.001 | <0.001 |
| Body-weight change (kg) | 7.9 | (8.1) | 4.7 | (8.2) | 3.6 | (7.8) | <0.001 | <0.001 |
| Energy intake (kcal/day) | 2108 | (570) | 2222 | (703) | 2331 | (682) | 0.107 | 0.040 |
| Habit of exercise, yes, n (%) | 67 | (65.7%) | 101 | (62.3%) | 36 | (60.0%) | 0.749 | 0.452 |
| Habit of smoking, yes, n (%) | 12 | (11.8%) | 31 | (19.1%) | 11 | (18.3%) | 0.273 | 0.199 |
| Habit of drinking, yes, n (%) | 64 | (62.2%) | 118 | (72.8%) | 44 | (73.3%) | 0.176 | 0.106 |
| Hypertension, n (%) | 30 | (29.4%) | 47 | (29.0%) | 27 | (45.0%) | 0.060 | 0.099 |
| Dyslipidemia, n (%) | 37 | (36.3%) | 43 | (26.5%) | 15 | (25.0%) | 0.172 | 0.084 |
| Diabetes, n (%) | 11 | (10.8%) | 21 | (13.0%) | 7 | (11.7%) | 0.865 | 0.767 |
| Cancer, n (%) | 14 | (13.7%) | 17 | (10.5%) | 9 | (15.0%) | 0.582 | 0.987 |
| Myocardial infarction, n (%) | 7 | (6.9%) | 3 | (1.9%) | 1 | (1.7%) | 0.065 | 0.065 |
| Cerebrovascular disease, n (%) | 4 | (3.9% | 9 | (5.6%) | 2 | (3.3%) | 0.719 | 0.975 |
| Adult women (30–69 years) | ||||||||
| n (%) | 648 | (37.6%) | 872 | (50.7%) | 201 | (11.7%) | ||
| Age (years) | 56.2 | (11.1) | 57.4 | (10.6) | 56.9 | (10.3) | 0.129 | 0.15 |
| Body weight (kg) | 55.1 | (8.6) | 52.7 | (7.1) | 51.0 | (7.8) | <0.001 | <0.001 |
| BMI (kg/m2) | 22.8 | (3.4) | 22.0 | (2.9) | 21.6 | (3.1) | <0.001 | <0.001 |
| Body weight at age 20 years (kg) | 51.2 | (6.4) | 50.4 | (5.8) | 49.1 | (6.2) | <0.001 | <0.001 |
| Body-weight change (kg) | 3.9 | (7.6) | 2.3 | (6.8) | 1.9 | (7.0) | <0.001 | <0.001 |
| Energy intake (kcal/day) | 1870 | (524) | 1851 | (545) | 1866 | (483) | 0.567 | 0.636 |
| Habit of exercise, yes, n (%) | 339 | (52.5%) | 467 | (53.6%) | 100 | (49.8%) | 0.616 | 0.741 |
| Habit of smoking, yes, n (%) | 31 | (4.8%) | 37 | (4.2%) | 15 | (7.5%) | 0.158 | 0.344 |
| Habit of drinking, yes, n (%) | 211 | (32.7%) | 279 | (32.0%) | 71 | (35.3%) | 0.663 | 0.680 |
| Hypertension, n (%) | 135 | (20.9%) | 201 | (23.1%) | 33 | (16.4%) | 0.107 | 0.719 |
| Dyslipidemia, n (%) | 91 | (14.1%) | 97 | (11.1%) | 30 | (14.9%) | 0.137 | 0.489 |
| Diabetes, n (%) | 27 | (4.2%) | 34 | (3.9%) | 5 | (2.5%) | 0.547 | 0.365 |
| Cancer, n (%) | 24 | (3.7%) | 47 | (5.4%) | 12 | (6.0%) | 0.233 | 0.088 |
| Myocardial infarction, n (%) | 2 | (0.3%) | 1 | (0.1%) | - | - | 0.547 | 0.281 |
| Cerebrovascular disease, n (%) | 4 | (0.6%) | 14 | (1.6%) | 3 | (1.5%) | 0.209 | 0.084 |
| Older adult women (70–87 years) | ||||||||
| n (%) | 97 | (26.2%) | 210 | (56.8%) | 63 | (17.0%) | ||
| Age (years) | 72.9 | (2.3) | 72.9 | (2.3) | 73.0 | (2.2) | 0.855 | 0.871 |
| Body weight (kg) | 55.7 | (7.8) | 51.3 | (7.5) | 47.8 | (7.2) | 0.021 | 0.050 |
| BMI (kg/m2) | 23.2 | (3.2) | 22.7 | (3.1) | 21.8 | (3.1) | 0.036 | 0.012 |
| Body weight at age 20 years (kg) | 50.0 | (6.2) | 50.1 | (5.9) | 47.7 | (6.6) | 0.021 | 0.050 |
| Body-weight change (kg) | 2.7 | (8.2) | 1.2 | (8.0) | 0.1 | (8.0) | 0.104 | 0.042 |
| Energy intake (kcal/day) | 1825 | (482) | 1812 | (444) | 1882 | (557) | 0.673 | 0.431 |
| Habit of exercise, yes, n (%) | 58 | (59.8%) | 138 | (65.7%) | 39 | (61.9%) | 0.580 | 0.667 |
| Habit of smoking, yes, n (%) | 0 | 0.0%) | 2 | (1.0%) | 3 | (4.8%) | 0.029 | 0.017 |
| Habit of drinking, yes, n (%) | 14 | (14.4%) | 32 | (15.2%) | 12 | (19.0%) | 0.710 | 0.465 |
| Hypertension, n (%) | 40 | (41.2%) | 90 | (42.9%) | 20 | (31.7%) | 0.285 | 0.332 |
| Dyslipidemia, n (%) | 21 | (21.6%) | 31 | (14.8%) | 12 | (19.0%) | 0.307 | 0.502 |
| Diabetes, n (%) | 6 | (6.2%) | 15 | (7.1%) | 5 | (7.9%) | 0.910 | 0.663 |
| Cancer, n (%) | 6 | (6.2%) | 15 | (7.1%) | 3 | (4.8%) | 0.790 | 0.806 |
| Myocardial infarction, n (%) | - | - | 1 | (0.5%) | 1 | (1.6%) | 0.401 | 0.267 |
| Cerebrovascular disease, n (%) | 2 | (2.1%) | 7 | (3.3%) | 4 | (6.3%) | 0.347 | 0.197 |
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |||
| Adult men (31–69 years) | ||||||
| Eating speed | ||||||
| Fast | Ref | Ref | ||||
| Moderate | 4.90 | (1.40–17.10) | 0.004 | 4.20 | (1.14–15.50) | 0.031 |
| Slow | 13.94 | (3.63–53.51) | <0.001 | 9.68 | (2.32–40.51) | 0.002 |
| Age (years) | 0.97 | (0.93–1.00) | 0.064 | 0.96 | (0.92–1.01) | 0.111 |
| Body weight at age 20 years (kg) | 0.85 | (0.79–0.92) | <0.001 | |||
| Energy intake (kcal/day) | 1.00 | (1.00–1.00) | 0.104 | |||
| Habit of exercise | 1.99 | (0.76–5.24) | 0.164 | |||
| Habit of smoking | 3.30 | (1.39–7.80) | 0.007 | |||
| Habit of drinking | 1.87 | (0.54–4.30) | 0.422 | |||
| Hypertension | 0.26 | (0.07–0.96) | 0.042 | |||
| Dyslipidemia | 0.41 | (0.14–1.23) | 0.112 | |||
| Diabetes | 1.99 | (0.48–8.31) | 0.346 | |||
| Cancer | 1.76 | (0.16–19.41) | 0.645 | |||
| Myocardial infarction | 19.92 | (1.57–277.7) | 0.021 | |||
| Cerebrovascular disease | - | - | - | |||
| Older adult men (70–86 years) | ||||||
| Eating speed | ||||||
| Fast | Ref | Ref | ||||
| Moderate | 2.64 | (1.04–6.73) | 0.042 | 0.75 | (0.16–3.47) | 0.711 |
| Slow | 3.57 | (1.25–10.24) | 0.018 | 1.65 | (0.31–8.73) | 0.554 |
| Age (years) | 1.03 | (0.92–1.58) | 0.624 | 1.12 | (0.94–1.33) | 0.223 |
| Body weight at age 20 years (kg) | 0.90 | (0.87–0.94) | <0.001 | |||
| Energy intake (kcal/day) | 1.00 | (1.00–1.00) | 0.590 | |||
| Habit of exercise | 1.36 | (0.37–4.95) | 0.644 | |||
| Habit of smoking | 0.56 | (0.06–4.97) | 0.600 | |||
| Habit of drinking | 0.60 | (0.13–2.77) | 0.508 | |||
| Hypertension | 1.08 | (0.29–4.03) | 0.907 | |||
| Dyslipidemia | 0.23 | (0.02–2.10) | 0.186 | |||
| Diabetes | 1.10 | (0.20–6.13) | 0.911 | |||
| Cancer | - | - | - | |||
| Myocardial infarction | - | - | - | |||
| Cerebrovascular disease | - | - | - | |||
| Adult women (30~69 years) | ||||||
| Eating speed | ||||||
| Fast | Ref | Ref | ||||
| Moderate | 1.36 | (0.93–1.99) | 0.114 | 1.21 | (0.81–1.79) | 0.351 |
| Slow | 1.90 | (1.13–3.21) | 0.308 | 1.45 | (0.83–2.51) | 0.189 |
| Age (years) | 0.95 | (0.94–0.97) | <0.001 | 0.96 | (0.94–0.97) | <0.001 |
| Body weight at age 20 years (kg) | 0.87 | (0.84–0.90) | <0.001 | |||
| Energy intake (kcal/day) | 1.00 | (1.00–1.00) | 0.660 | |||
| Habit of exercise | 1.24 | (0.86–1.78) | 0.242 | |||
| Habit of smoking | 1.56 | (0.81–3.01) | 0.184 | |||
| Habit of drinking | 0.87 | (0.56–1.33) | 0.510 | |||
| Hypertension | 0.78 | (0.48–1.28) | 0.325 | |||
| Dyslipidemia | 0.24 | (0.10–0.61) | 0.003 | |||
| Diabetes | 1.33 | (0.50–3.53) | 0.564 | |||
| Cancer | 1.64 | (0.74–3.62) | 0.221 | |||
| Myocardial infarction | - | - | - | |||
| Cerebrovascular disease | 0.97 | (0.13–7.52) | 0.978 | |||
| Older adult women (70–87 years) | ||||||
| Eating speed | ||||||
| Fast | Ref | Ref | ||||
| Moderate | 2.52 | (1.18–5.41) | 0.018 | 2.44 | (1.11–5.38) | 0.027 |
| Slow | 3.91 | (1.63–9.40) | 0.002 | 3.82 | (1.51–9.69) | 0.005 |
| Age (years) | 1.01 | (0.96–1.14) | 0.824 | 1.03 | (0.92–1.16) | 0.572 |
| Body weight at age 20 years (kg) | 0.92 | (0.87–0.96) | <0.001 | |||
| Energy intake (kcal/day) | 1.00 | (1.00–1.00) | 0.424 | |||
| Habit of exercise | 0.60 | (0.32–1.13) | 0.112 | |||
| Habit of smoking | 0.62 | (0.06–6.73) | 0.690 | |||
| Habit of drinking | 1.07 | (0.44–2.57) | 0.888 | |||
| Hypertension | 0.62 | (0.35–1.13) | 0.118 | |||
| Dyslipidemia | 0.16 | (0.05–0.49) | 0.001 | |||
| Diabetes | 0.48 | (0.13–1.78) | 0.275 | |||
| Cancer | 1.66 | (0.56–4.94) | 0.362 | |||
| Myocardial infarction | - | - | - | |||
| Cerebrovascular disease | 0.22 | (0.03–1.90) | 0.169 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, T.; Nakamura, Y.; Takashima, N.; Kadota, A.; Miura, K.; Ueshima, H.; Kita, Y. Eating Slowly Is Associated with Undernutrition among Community-Dwelling Adult Men and Older Adult Women. Nutrients 2022, 14, 54. https://doi.org/10.3390/nu14010054
Nakamura T, Nakamura Y, Takashima N, Kadota A, Miura K, Ueshima H, Kita Y. Eating Slowly Is Associated with Undernutrition among Community-Dwelling Adult Men and Older Adult Women. Nutrients. 2022; 14(1):54. https://doi.org/10.3390/nu14010054
Chicago/Turabian StyleNakamura, Tomiyo, Yasuyuki Nakamura, Naoyuki Takashima, Aya Kadota, Katsuyuki Miura, Hirotsugu Ueshima, and Yosikuni Kita. 2022. "Eating Slowly Is Associated with Undernutrition among Community-Dwelling Adult Men and Older Adult Women" Nutrients 14, no. 1: 54. https://doi.org/10.3390/nu14010054
APA StyleNakamura, T., Nakamura, Y., Takashima, N., Kadota, A., Miura, K., Ueshima, H., & Kita, Y. (2022). Eating Slowly Is Associated with Undernutrition among Community-Dwelling Adult Men and Older Adult Women. Nutrients, 14(1), 54. https://doi.org/10.3390/nu14010054