
A Proinflammatory Diet May Increase Mortality Risk in Patients with Diabetes Mellitus


Abstract
:1. Introduction
2. Materials and Methods
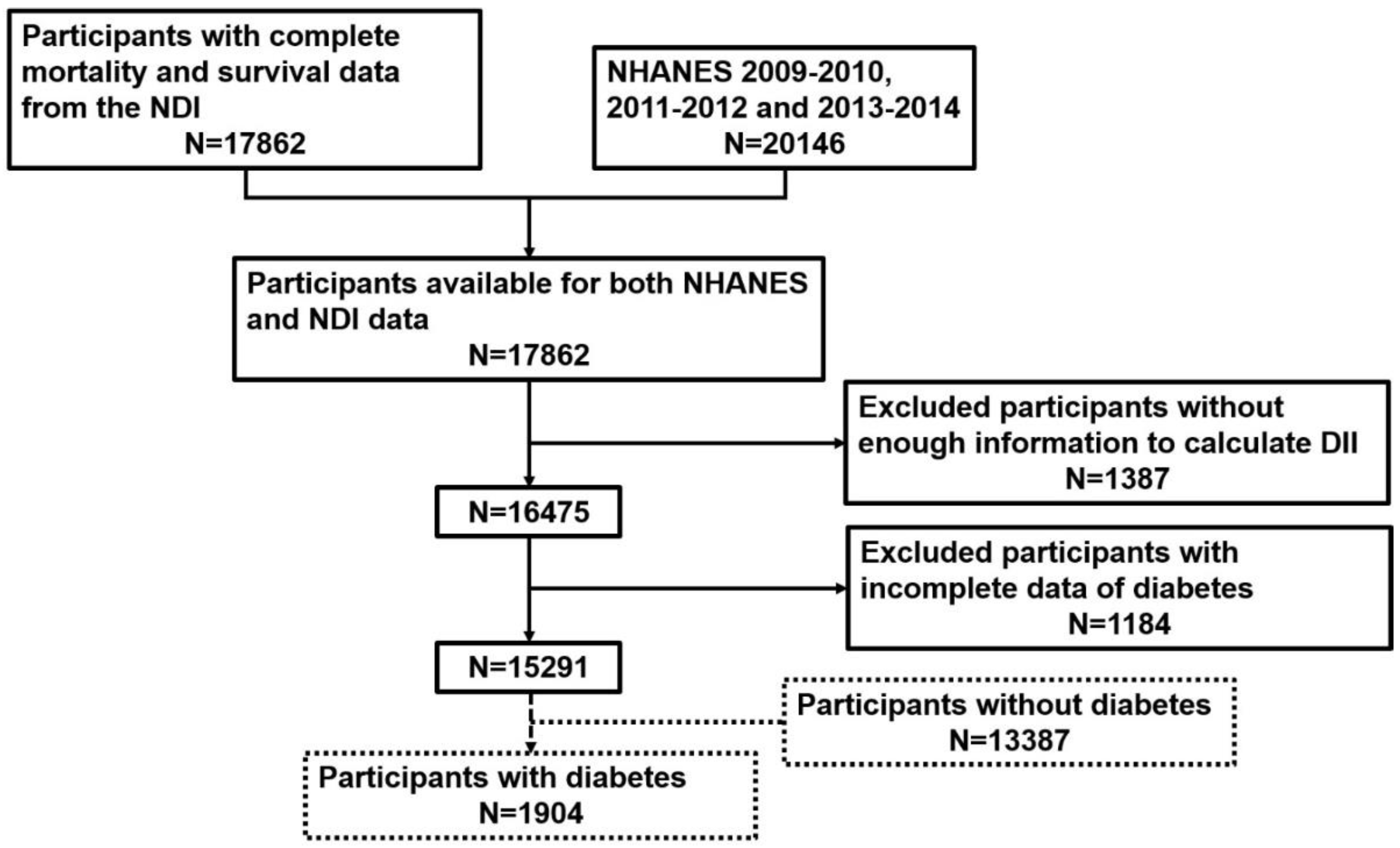
2.1. Participant Recruitment
2.2. Exposure and Outcome Definitions
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. The Association between DII and Diabetes Prevalence
3.2. The Association between DII and All-Cause Mortality among People with Diabetes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harcourt, B.E.; Penfold, S.A.; Forbes, J.M. Coming full circle in diabetes mellitus: From complications to initiation. Nat. Rev. Endocrinol. 2013, 9, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Calle, M.C.; Fernandez, M.L. Inflammation and type 2 diabetes. Diabetes Metab. 2012, 38, 183–191. [Google Scholar] [CrossRef] [PubMed]
- White, M.F. IRS proteins and the common path to diabetes. Am. J. Physiol. Endocrinol. Metab. 2002, 283, E413–E422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniguchi, C.M.; Emanuelli, B.; Kahn, C.R. Critical nodes in signalling pathways: Insights into insulin action. Nat. Rev. Mol. Cell Biol. 2006, 7, 85–96. [Google Scholar] [CrossRef]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Phillips, C.M.; Chen, L.W.; Heude, B.; Bernard, J.Y.; Harvey, N.C.; Duijts, L.; Mensink-Bout, S.M.; Polanska, K.; Mancano, G.; Suderman, M.; et al. Dietary Inflammatory Index and Non-Communicable Disease Risk: A Narrative Review. Nutrients 2019, 11, 1873. [Google Scholar] [CrossRef] [Green Version]
- Ahluwalia, N.; Dwyer, J.; Terry, A.; Moshfegh, A.; Johnson, C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical Considerations, and Uses to Inform Public Policy. Adv. Nutr. 2016, 7, 121–134. [Google Scholar] [CrossRef] [Green Version]
- Wan, Z.; Guo, J.; Pan, A.; Chen, C.; Liu, L.; Liu, G. Association of Serum 25-Hydroxyvitamin D Concentrations with All-Cause and Cause-Specific Mortality Among Individuals With Diabetes. Diabetes Care 2021, 44, 350–357. [Google Scholar] [CrossRef]
- Series 1: Programs and collection procedures. In Plan and operation of the Third National Health and Nutrition Examination Survey, 1988–1994; Vital Health Statistics: Atlanta, GA, USA, 1994; pp. 1–407.
- Zhang, C.; Bian, H.; Chen, Z.; Tian, B.; Wang, H.; Tu, X.; Cai, B.; Jin, K.; Zheng, X.; Yang, L.; et al. The Association between Dietary Inflammatory Index and Sex Hormones among Men in the United States. J. Urol. 2021, 206, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.; Zhao, J.; Li, J.; Yang, Q.; Geng, J.; Liao, R.; Su, B. Low lean mass is associated with lower urinary tract symptoms in US men from the 2005-2006 national health and nutrition examination survey dataset. Aging 2021, 13, 21421–21434. [Google Scholar] [CrossRef] [PubMed]
- Martorell, R.; Young, M.F. Patterns of stunting and wasting: Potential explanatory factors. Adv. Nutr. 2012, 3, 227–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michels, W.M.; Grootendorst, D.C.; Verduijn, M.; Elliott, E.G.; Dekker, F.W.; Krediet, R.T. Performance of the Cockcroft-Gault, MDRD, and new CKD-EPI formulas in relation to GFR, age, and body size. Clin. J. Am. Soc. Nephrol. 2010, 5, 1003–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, P.E.; Levin, A. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapter 1: Definition and classification of CKD. Kidney Int. Suppl. 2013, 3, 19–62. [CrossRef] [Green Version]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef]
- Qin, Z.; Zhao, J.; Geng, J.; Chang, K.; Liao, R.; Su, B. Higher Triglyceride-Glucose Index Is Associated with Increased Likelihood of Kidney Stones. Front. Endocrinol. 2021, 12, 774567. [Google Scholar] [CrossRef]
- Liu, N.; Ma, F.; Feng, Y.; Ma, X. The Association between the Dietary Inflammatory Index and Thyroid Function in U.S. Adult Males. Nutrients 2021, 13, 3330. [Google Scholar] [CrossRef]
- Cheung, C.L.; Sahni, S.; Cheung, B.M.; Sing, C.W.; Wong, I.C. Vitamin K intake and mortality in people with chronic kidney disease from NHANES III. Clin. Nutr. 2015, 34, 235–240. [Google Scholar] [CrossRef]
- Wiener, R.C. Serum Cotinine and Chronic Pain: NHANES 2003–2004. J. Drug Abus. 2015, 1, 3. [Google Scholar]
- Liu, N.; Feng, Y.; Zhan, Y.; Ma, F. Relationship between blood cadmium and abdominal aortic calcification: NHANES 2013-2014. J. Trace Elem. Med. Biol. 2022, 72, 126975. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Yano, Y.; Fujimoto, S.; Konta, T.; Iseki, K.; Moriyama, T.; Yamagata, K.; Tsuruya, K.; Yoshida, H.; Asahi, K.; et al. Glycohemoglobin not as predictive as fasting glucose as a measure of prediabetes in predicting proteinuria. Nephrol. Dial. Transplant. 2012, 27, 3862–3868. [Google Scholar] [CrossRef] [Green Version]
- Rohm, T.V.; Meier, D.T.; Olefsky, J.M.; Donath, M.Y. Inflammation in obesity, diabetes, and related disorders. Immunity 2022, 55, 31–55. [Google Scholar] [CrossRef]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef] [PubMed]
- Archundia Herrera, M.C.; Subhan, F.B.; Chan, C.B. Dietary Patterns and Cardiovascular Disease Risk in People with Type 2 Diabetes. Curr. Obes. Rep. 2017, 6, 405–413. [Google Scholar] [CrossRef]
- Papamichou, D.; Panagiotakos, D.B.; Itsiopoulos, C. Dietary patterns and management of type 2 diabetes: A systematic review of randomised clinical trials. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 531–543. [Google Scholar] [CrossRef]
- Esposito, K.; Ciotola, M.; Sasso, F.C.; Cozzolino, D.; Saccomanno, F.; Assaloni, R.; Ceriello, A.; Giugliano, D. Effect of a single high-fat meal on endothelial function in patients with the metabolic syndrome: Role of tumor necrosis factor-alpha. Nutr. Metab. Cardiovasc. Dis. NMCD 2007, 17, 274–279. [Google Scholar] [CrossRef]
- Becher, B.; Spath, S.; Goverman, J. Cytokine networks in neuroinflammation. Nat. Rev. Immunol. 2017, 17, 49–59. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef]
- Ukah, T.K.; Cattin-Roy, A.N.; Chen, W.; Miller, M.M.; Barik, S.; Zaghouani, H. On the Role IL-4/IL-13 Heteroreceptor Plays in Regulation of Type 1 Diabetes. J. Immunol. 2017, 199, 894–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Dietary Inflammatory Index | Overall | Anti-Inflammatory Diet (DII < 0) | Proinflammatory Diet (DII > 0) | p-Value |
|---|---|---|---|---|
| Participant number | 15,291 | 7377 | 7914 | - |
| Mean ± SD DII | 0.2 ± 1.8 | −1.5 ± 1.0 | 1.6 ± 1.1 | <0.0001 |
| Mean ± SD Age (years) | 47 ± 18 | 47 ± 17 | 46 ± 18 | <0.0001 |
| Mean ± SD Energy intake (kcal) | 2130 ± 1004 | 2610 ± 1044 | 1719 ± 674 | <0.0001 |
| Mean ± SD Protein intake (g) | 82 ± 43 | 102 ± 45 | 64 ± 29 | <0.0001 |
| Mean ± SD Systolic pressure (mmHg) | 122 ± 18 | 121 ± 16 | 121 ± 17 | 0.6522 |
| Mean ± SD Diastolic pressure (mmHg) | 70 ± 13 | 71 ± 12 | 70 ± 12 | 0.0003 |
| Mean ± SD Fasting glucose (mg/dL) | 107 ± 32 | 104 ± 27 | 105 ± 29 | 0.0879 |
| Mean ± SD Glycohemoglobin (%) | 5.7 ± 1.0 | 5.6 ± 0.8 | 5.6 ± 1.0 | <0.0001 |
| Mean ± SD eGFR (ml/min/1.73 m2) | 100 ± 17 | 99 ± 14 | 101 ± 16 | <0.0001 |
| Mean ± SD UACR (mg/g) | 39 ± 301 | 22 ± 156 | 32 ± 254 | 0.0033 |
| Gender (%) | <0.0001 | |||
| Male | 49 | 58 | 39 | |
| Female | 51 | 42 | 61 | |
| Race (%) | <0.0001 | |||
| Mexican American | 15 | 9 | 9 | |
| Other Hispanic | 10 | 5 | 6 | |
| Non-Hispanic White | 44 | 72 | 64 | |
| Non-Hispanic Black | 21 | 8 | 14 | |
| Other Race | 11 | 7 | 7 | |
| Hypertension (%) | 0.1191 | |||
| Yes | 17.2 | 15.1 | 16.1 | |
| No | 76.2 | 84.9 | 83.9 | |
| Diabetes (%) | <0.0001 | |||
| Yes | 13.3 | 8.9 | 11.4 | |
| No | 86.7 | 91.1 | 88.6 | |
| CKD (%) | <0.0001 | |||
| Yes | 11.5 | 7.7 | 10.5 | |
| CKD stage 1 | 5.6 | 3.8 | 5.4 | |
| CKD stage 2 | 5.6 | 3.6 | 4.9 | |
| CKD stage 3 | 0.3 | 0.2 | 0.3 | |
| CKD stage 4/5 | 0 | 0 | 0 | |
| No | 88.5 | 92.3 | 89.5 | |
| Physical activity (%) | <0.0001 | |||
| Vigorous physical activity | 35 | 45 | 33 | |
| Moderate physical activity | 32 | 33 | 33 | |
| Less than moderate | 33 | 22 | 34 | |
| Smoking exposure (%) | <0.0001 | |||
| Non-smoker | 27 | 34 | 27 | |
| Second-hand smoker | 49 | 45 | 45 | |
| Current smoker | 24 | 21 | 28 | |
| Alcohol intake (%) | <0.0001 | |||
| Non-drinker | 21 | 8 | 15 | |
| Former drinker | 12 | 8 | 13 | |
| Current drinker | 67 | 84 | 72 | |
| BMI (%) | <0.0001 | |||
| Normal (<25 kg/m2) | 31 | 32 | 29 | |
| Overweight (25–30 kg/m2) | 32 | 36 | 30 | |
| Obese (>30 kg/m2) | 37 | 32 | 41 | |
| All-cause mortality (%) | 4.02 | 2.50 | 3.61 | <0.0001 |
| Dietary Inflammatory Index (DII) | Model 1 a | Model 2 b | Model 3 c |
|---|---|---|---|
| Fasting glucose (mg/dL)-β d (95% CI e) p-value | |||
| Continuous | 0.45 (0.06, 0.84) 0.0236 | 0.83 (0.45, 1.22) < 0.0001 | 0.83 (0.30, 1.36) 0.0022 |
| DII < 0 | Ref = 0 | Ref = 0 | Ref = 0 |
| DII > 0 | 1.54 (0.09, 2.98) 0.0370 | 2.72 (1.31, 4.14) 0.0002 | 1.91 (0.16, 3.66) 0.0323 |
| Glycohemoglobin (%)-β d (95% CI e) p-value | |||
| Continuous | 0.02 (0.02, 0.03) < 0.0001 | 0.03 (0.02, 0.04) < 0.0001 | 0.02 (0.01, 0.03) 0.0009 |
| DII < 0 | Ref = 0 | Ref = 0 | Ref = 0 |
| DII > 0 | 0.07 (0.04, 0.10) < 0.0001 | 0.07 (0.04, 0.10) < 0.0001 | 0.03 (−0.01, 0.07) 0.1267 |
| Diabetes-OR f (95% CI e) p-value | |||
| Continuous | 1.07 (1.05, 1.10) < 0.0001 | 1.09 (1.06, 1.12) < 0.0001 | 1.05 (1.01, 1.09) 0.0139 |
| DII < 0 | Ref = 1 | Ref = 1 | Ref = 1 |
| DII > 0 | 1.31 (1.19, 1.44) < 0.0001 | 1.34 (1.21, 1.49) < 0.0001 | 1.18 (1.03, 1.34) 0.0141 |
| CKD-OR f (95% CI e) p-value | |||
| Continuous | 1.10 (1.07, 1.13) < 0.0001 | 1.10 (1.06, 1.13) < 0.0001 | 1.14 (0.99, 1.31) 0.0660 |
| DII < 0 | Ref = 1 | Ref = 1 | Ref = 1 |
| DII > 0 | 1.35 (1.22, 1.50) < 0.0001 | 1.31 (1.18, 1.46) < 0.0001 | 1.44 (0.93, 2.25) 0.1043 |
| All-cause mortality-OR f (95% CI e) p-value | |||
| Continuous | 1.08 (1.04, 1.13) 0.0003 | 1.12 (1.07, 1.17) < 0.0001 | 1.11 (1.03, 1.18) 0.0031 |
| DII < 0 | Ref = 1 | Ref = 1 | Ref = 1 |
| DII > 0 | 1.33 (1.13, 1.56) 0.0007 | 1.44 (1.21, 1.72) < 0.0001 | 1.26 (1.02, 1.57) 0.0357 |
| Dietary Inflammatory Index | Overall | Anti-Inflammatory Diet (DII < 0) | Proinflammatory Diet (DII > 0) | p-Value |
|---|---|---|---|---|
| Participant number | 1904 | 811 | 1093 | - |
| Mean ± SD DII | 0.4 ± 1.8 | −1.3 ± 0.9 | 1.6 ± 1.1 | <0.0001 |
| Mean ± SD Age (yrs) | 60 ± 14 | 59 ± 14 | 60 ± 14 | 0.1376 |
| Mean ± SD Energy intake (kcal) | 1925 ± 907 | 2545 ± 951 | 1583 ± 652 | <0.0001 |
| Mean ± SD Protein intake (g) | 79 ± 41 | 103 ± 42 | 63 ± 29 | <0.0001 |
| Mean ± SD Systolic pressure (mmHg) | 132 ± 19 | 130 ± 18 | 131 ± 19 | 0.6375 |
| Mean ± SD Diastolic pressure (mmHg) | 69 ± 14 | 71 ± 14 | 69 ± 15 | 0.0020 |
| Mean ± SD eGFR (ml/min/1.73 m2) | 90 ± 14 | 89 ± 13 | 89 ± 13 | 0.5731 |
| Mean ± SD UACR (mg/g) | 148 ± 700 | 96 ± 452 | 138 ± 673 | 0.1179 |
| Mean ± SD Fasting glucose (mg/dL) | 155 ± 55 | 157 ± 55 | 153 ± 51 | 0.1978 |
| Mean ± SD Glycohemoglobin (%) | 7.6 ± 1.8 | 7.5 ± 1.7 | 7.5 ± 1.7 | 0.9987 |
| Gender (%) | <0.0001 | |||
| Male | 54 | 67 | 42 | |
| Female | 46 | 33 | 58 | |
| Race (%) | 0.0012 | |||
| Mexican American | 17 | 10 | 10 | |
| Other Hispanic | 11 | 5 | 8 | |
| Non-Hispanic White | 37 | 66 | 58 | |
| Non-Hispanic Black | 24 | 11 | 16 | |
| Other Race | 11 | 8 | 9 | |
| CKD (%) | <0.0001 | |||
| Yes | 29.5 | 23.2 | 28.9 | |
| CKD stage 1 | 10.6 | 7.5 | 9.6 | |
| CKD stage 2 | 17.8 | 14.6 | 18.4 | |
| CKD stage 3 | 1.1 | 1.1 | 0.9 | |
| CKD stage 4/5 | 0 | 0 | 0 | |
| No | 70.5 | 76.8 | 71.1 | |
| Hypertension (%) | 0.8896 | |||
| Yes | 30.5 | 29.6 | 29.9 | |
| No | 61.8 | 70.4 | 70.1 | |
| Physical activity (%) | <0.0001 | |||
| Vigorous physical activity | 20 | 25 | 18 | |
| Moderate physical activity | 34 | 38 | 31 | |
| Less than moderate | 46 | 37 | 51 | |
| Smoking exposure (%) | 0.0002 | |||
| Non-smoker | 28 | 36 | 28 | |
| Second-hand smoker | 52 | 47 | 49 | |
| Current smoker | 20 | 17 | 23 | |
| Alcohol intake (%) | <0.0001 | |||
| Non-drinker | 22 | 12 | 19 | |
| Former drinker | 15 | 10 | 17 | |
| Current drinker | 63 | 78 | 64 | |
| BMI (%) | <0.0001 | |||
| Normal (<25 kg/m2) | 13 | 11 | 11 | |
| Overweight (25–30 kg/m2) | 28 | 26 | 25 | |
| Obese (>30 kg/m2) | 58 | 62 | 64 | |
| All-cause mortality (%) | 9.35 | 5.84 | 9.47 | <0.0001 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| HR 1 (95% CI 2) | p-Value | HR1 (95% CI 2) | p-Value | |
| DII > 0 (vs. DII < 0) | 1.68 (1.23, 2.30) | 0.0011 | 1.71 (1.13, 2.58) | 0.0108 |
| Female (vs. Male) | 0.59 (0.44, 0.81) | 0.0008 | 0.71 (0.49, 1.02) | 0.0638 |
| Non-Hispanic White (vs. Other races 3) | 2.02 (1.27, 3.21) | 0.0031 | 0.96 (0.58, 1.60) | 0.8739 |
| Age | 1.07 (1.05, 1.08) | <0.0001 | 1.07 (1.04, 1.09) | <0.0001 |
| Energy intake | 0.99 (0.99,1.01) | 0.0802 | 0.99 (0.99, 1.00) | 0.0056 |
| Protein intake | 0.99 (0.98,1.00) | 0.0128 | 0.99 (0.98, 1.02) | 0.2423 |
| eGFR 4 | 0.96 (0.95,0.97) | <0.0001 | 0.98 (0.95, 1.00) | 0.0601 |
| UACR 5 | 1.00 (1.00, 100) | <0.0001 | 1.00 (0.99, 1.00) | 0.0023 |
| Systolic pressure | 1.01 (1.00,1.02) | 0.0096 | 0.99 (0.98, 1.00) | 0.1786 |
| Diastolic pressure | 0.98 (0.97,0.99) | 0.0124 | 1.00 (0.99, 1.01) | 0.4671 |
| Non-drinker (vs. Current drinker) | 0.86 (0.60, 1.26) | 0.4510 | 1.27 (0.83, 1.94) | 0.7722 |
| Former drinker (vs. Current drinker) | 1.12 (0.75, 1.66) | 0.5760 | 0.94 (0.60, 1.45) | 0.2740 |
| Moderate physical activity (vs. Less than moderate) | 0.57 (0.41, 0.80) | 0.0011 | 0.73 (0.51, 1.03) | 0.0778 |
| Vigorous physical activity (vs. Less than moderate) | 0.40 (0.24, 0.66) | 0.0003 | 0.60 (0.34, 1.02) | 0.0576 |
| Obese (vs. Normal) | 0.56 (0.37, 0.85) | 0.0059 | 0.85 (0.54, 1.33) | 0.4673 |
| Non-smoker (vs. Current smoker) | 0.11 (0.07, 0.18) | <0.0001 | 0.06 (0.04, 0.11) | <0.0001 |
| Second-hand smoker (vs. Current smoker) | 0.63 (0.40, 0.99) | 0.0442 | 0.39 (0.24, 0.66) | 0.0003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, J.; Liu, N.; Sun, P.; Tang, Y.; Qin, W. A Proinflammatory Diet May Increase Mortality Risk in Patients with Diabetes Mellitus. Nutrients 2022, 14, 2011. https://doi.org/10.3390/nu14102011
Tan J, Liu N, Sun P, Tang Y, Qin W. A Proinflammatory Diet May Increase Mortality Risk in Patients with Diabetes Mellitus. Nutrients. 2022; 14(10):2011. https://doi.org/10.3390/nu14102011
Chicago/Turabian StyleTan, Jiaxing, Nuozhou Liu, Peiyan Sun, Yi Tang, and Wei Qin. 2022. "A Proinflammatory Diet May Increase Mortality Risk in Patients with Diabetes Mellitus" Nutrients 14, no. 10: 2011. https://doi.org/10.3390/nu14102011