
Infant Feeding Practices That Substitute Exclusive Breastfeeding in a Semi-Rural Mexican Community: Types, Moments, and Associated Factors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Study Variables and Statistical Analyses
2.2.1. Sociodemographic Factors
2.2.2. Maternal and Infant Factors
2.2.3. Previous Infant Feeding Experience, Breastfeeding Information, Difficulties, Beliefs, and Thoughts
- “Formula milk is an important food to accompany breast milk before six months”.
- “I am convinced that giving only breast milk until the baby is six months old, without giving any other food, is the best for her/him”.
- “When the baby is not full, you should give her/him powdered milk or some other food, even if she/he is less than six months old”.
- “If the baby is ‘small in size’ she/he should receive other foods to grow faster”.
- “When breastfeeding, you are always sure that your baby under six months is full”.
- “When it is very hot you should give your baby under six months water or some other liquid to drink”.
2.2.4. Statistical Analyses
3. Results
3.1. Study Population
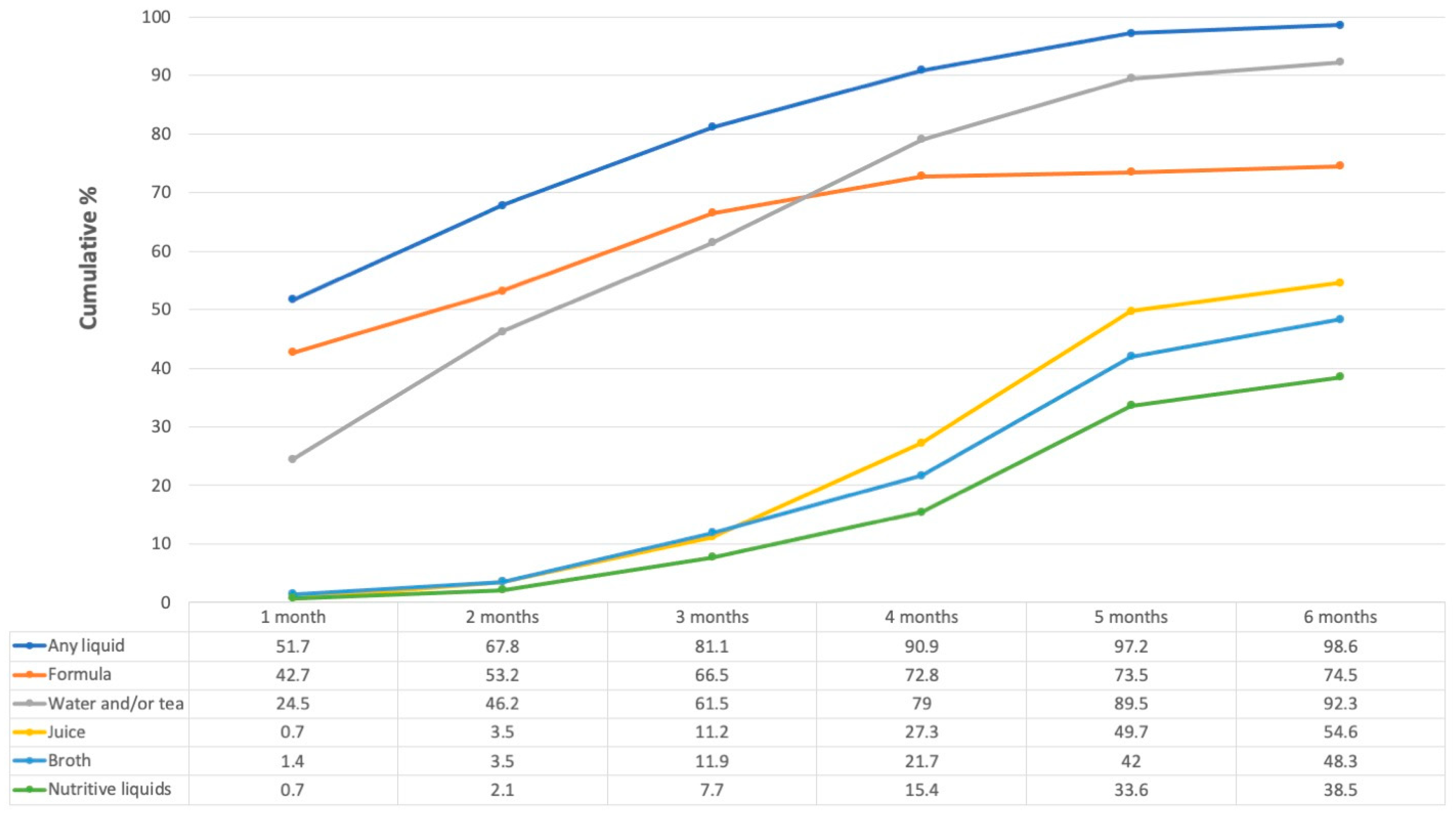
3.2. Consumption of Liquids
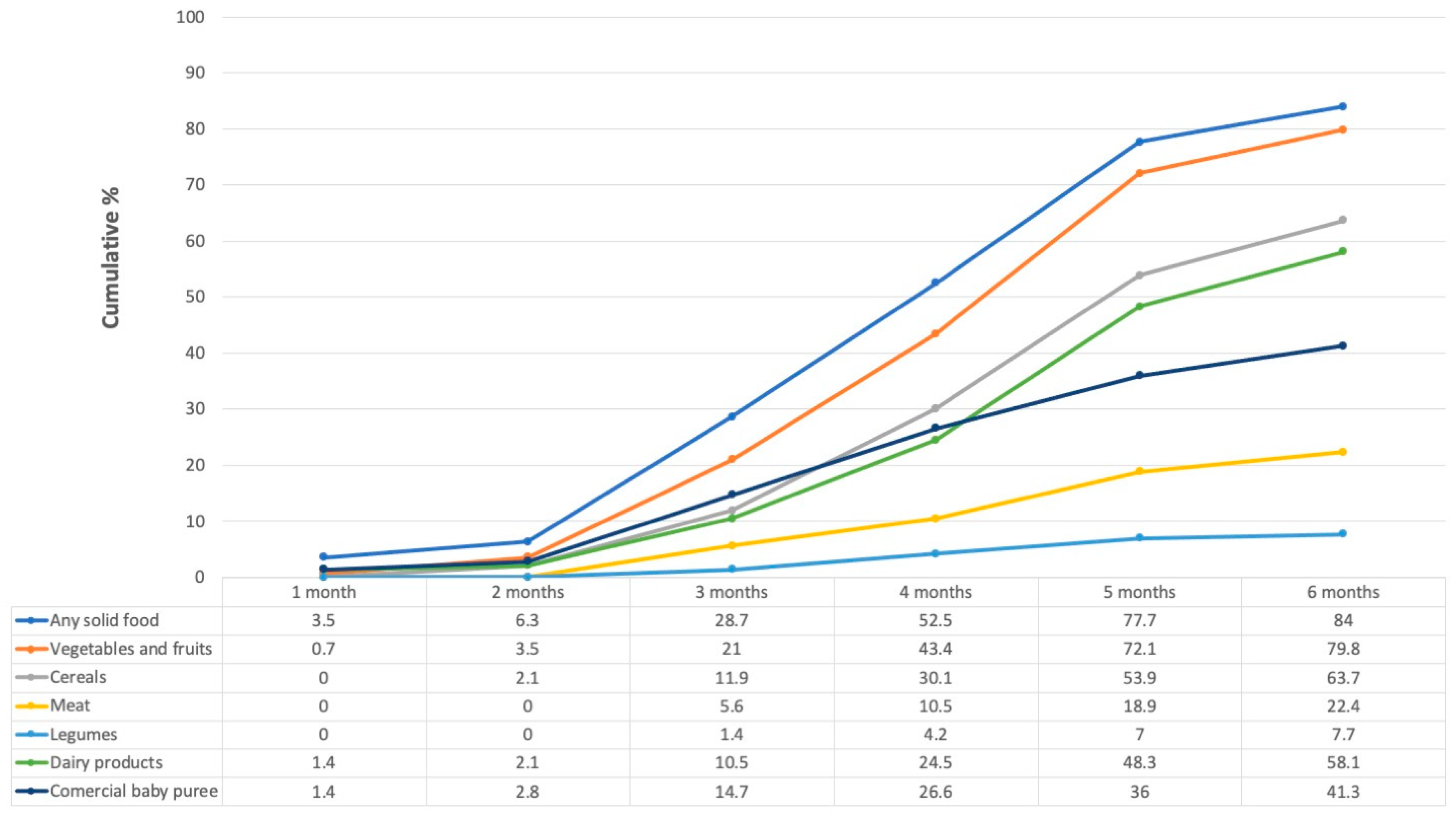
3.3. Consumption of Solid Foods
4. Discussion
4.1. Early Introduction of Liquids
4.1.1. Formula Milk
4.1.2. Water and Other Non-Nutritive Liquids
4.2. Early or Timely Introduction of Complementary Feeding
4.3. Study Limitations
4.4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AMAI | Spanish abbreviation for Mexican Association of Market Intelligence and Public Opinion Agencies |
| BFSE | breastfeeding self-efficacy |
| BMI | body mass index |
| CESSA | Spanish abbreviation for health center with expanded services |
| CF | complementary feeding |
| EBF | exclusive breastfeeding |
| ECF | early complementary feeding |
| ELCSA | Latin American and Caribbean Food Security Scale |
| ENSANUT | National Health and Nutrition Survey (Mexico) |
| FIV | variance inflation factor |
| FLPHU | first-level public health units |
| FM | formula milk |
| LAZ | length-for-age z-score |
| SEL | socioeconomic level |
| TCF | timely complementary feeding |
| WLZ | weight-for-age z-score |
References
- World Health Organization; United Nations Children’s Fund (UNICEF). Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003; ISBN 9789241562218. [Google Scholar]
- Walker, M. Formula Supplementation of Breastfed Infants. ICAN Infant Child Adolesc. Nutr. 2015, 7, 198–207. [Google Scholar] [CrossRef] [Green Version]
- González-Castell, D.; De Cosío, T.G.; Rodríguez-Ramírez, S.; Escobar-Zaragoza, L. Early consumption of liquids different to breast milk in Mexican infants under 1 year: Results of the probabilistic National Health and Nutrition Survey 2012. Nutr. Hosp. 2016, 33, 14–20. [Google Scholar]
- Wang, L.; Van Grieken, A.; Van Der Velde, L.A.; Vlasblom, E.; Beltman, M.; L’Hoir, M.P.; Boere-Boonekamp, M.M.; Raat, H. Factors associated with early introduction of complementary feeding and consumption of non-recommended foods among Dutch infants: The BeeBOFT study. BMC Public Health 2019, 19, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Rebhan, B.; Kohlhuber, M.; Schwegler, U.; Koletzko, B.V.; Fromme, H. Infant Feeding Practices and Associated Factors Through the First 9 Months of Life in Bavaria, Germany. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 467–473. [Google Scholar] [CrossRef]
- Sriraman, N.K. The Nuts and Bolts of Breastfeeding: Anatomy and Physiology of Lactation. Curr. Probl. Pediatr. Adolesc. Health Care 2017, 47, 305–310. [Google Scholar] [CrossRef]
- Tachimoto, H.; Imanari, E.; Mezawa, H.; Okuyama, M.; Urashima, T.; Hirano, D.; Gocho, N.; Urashima, M. Effect of Avoiding Cow’s Milk Formula at Birth on Prevention of Asthma or Recurrent Wheeze Among Young Children: Extended Follow-up From the ABC Randomized Clinical Trial. JAMA Netw Open 2020, 3, e2018534. [Google Scholar] [CrossRef]
- Mastrorilli, C.; Santoro, A.; Caffarelli, C. Primary prevention of allergic diseases: The role of early exposure to cow′s milk formula. Front. Pediatr. 2020, 8, 420. [Google Scholar] [CrossRef]
- Güngör, D.; Nadaud, P.; Lapergola, C.C.; Dreibelbis, C.; Wong, Y.P.; Terry, N.; Abrams, S.A.; Beker, L.; Jacobovits, T.; Järvinen, K.M.; et al. Infant milk-feeding practices and diabetes outcomes in offspring: A systematic review. Am. J. Clin. Nutr. 2019, 109, 817S–837S. [Google Scholar] [CrossRef]
- Kapourchali, F.R.; Cresci, G.A.M. Early-Life Gut Microbiome—The Importance of Maternal and Infant Factors in Its Establishment. Nutr. Clin. Pract. 2020, 35, 386–405. [Google Scholar] [CrossRef]
- Ley, D.; Desseyn, J.-L.; Mischke, M.; Knol, J.; Turck, D.; Gottrand, F. Early-life origin of intestinal inflammatory disorders. Nutr. Rev. 2017, 75, 175–187. [Google Scholar] [CrossRef]
- Lamberti, L.M.; Walker, C.L.F.; Noiman, A.; Victora, C.; Black, R.E. Breastfeeding and the risk for diarrhea morbidity and mortality. BMC Public Health 2011, 11 (Suppl. 3), S15. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.; Zhang, G.; Swaminathan, B.; Doyle, M.; Bowen, A. Efficacy of Protocols for Cleaning and Disinfecting Infant Feeding Bottles in Less Developed Communities. Am. J. Trop. Med. Hyg. 2009, 81, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Cortes, J.Z.; Osti, L.E.T.; Torres, M.O.; Vargas, L.M.; Gress, A.A.O. Poor breastfeeding, complementary feeding and Dietary Diversity in children and their relationship with stunting in rural communities. Nutr. Hosp. 2018, 35, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.; Liu, L.; Zhu, Y.; Huang, G.; Wang, P.P. The association between breastfeeding and childhood obesity: A meta-analysis. BMC Public Health 2014, 14, 1267. [Google Scholar] [CrossRef] [Green Version]
- Qiao, J.; Dai, L.-J.; Zhang, Q.; Ouyang, Y.-Q. A Meta-Analysis of the Association Between Breastfeeding and Early Childhood Obesity. J. Pediatr. Nurs. 2020, 53, 57–66. [Google Scholar] [CrossRef]
- Jimenez-Cruz, A.; Bacardi-Gascon, M.; Pichardo-Osuna, A.; Mandujano-Trujillo, Z.; Castillo-Ruiz, O. Infant and toddlers′ feeding practices and obesity amongst low-income families in Mexico. Asia Pac. J. Clin. Nutr. 2010, 19, 316–323. [Google Scholar]
- Weaver, L.T. Rapid Growth in Infancy: Balancing the Interests of the Child. J. Pediatr. Gastroenterol. Nutrition 2006, 43, 428–432. [Google Scholar]
- Shamah-Levy, T.; Vielma-Orozco, E.; Heredia-Hernández, O.; Romero-Martínez, M.; Mojica-Cuevas, J.; Cuevas-Nasu, L.; Santaella-Castell, J.A.; Rivera-Dommarco, J. Encuesta Nacional de Salud Y Nutrición 2018–19: Resultados Nacionales. Salud Pública De México 2020, 62, 614–617. [Google Scholar] [CrossRef]
- Afeiche, M.C.; Villalpando-Carrión, S.; Reidy, K.C.; Fries, L.R.; Eldridge, A.L. Many infants and young children are not compliant with Mexican and international complementary feeding recommendations for milk and other beverages. Nutrients 2018, 10, 466. [Google Scholar] [CrossRef] [Green Version]
- Swigart, T.M.; Bonvecchio, A.; Théodore, F.L.; Zamudio-Haas, S.; Villanueva-Borbolla, M.A.; Thrasher, J.F. Breastfeeding practices, beliefs, and social norms in low-resource communities in Mexico: Insights for how to improve future promotion strategies. PLoS ONE 2017, 12, e0180185. [Google Scholar] [CrossRef]
- Becerril-Montekio, V.M.; Alcalde Rabanal, J.E. (Eds.) Diseño de Intervenciones Para Mejorar La Implementación Local de Programas de Salud Materna Desde La Perspectiva Del Conocimiento Tácito Y El Marco Lógico; Centro de Investigaciones y Estudios de la Salud, Universidad Nacional Autónoma de Nicaragua: Managua, Nicaragua; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2015. [Google Scholar]
- Formative Research: A Guide to Support the Collection and Analysis of Qualitative Data for Integrated Maternal and Child Nutrition Program Planning; Cooperative for Assistance and Relief Everywhere, Inc. (CARE): Geneva, Switzerland, 2013.
- González de Cosío, T.; Escobar-Zaragoza, L.; González-Castell, L.D. Prácticas de alimentación infantil y deterioro de la lactancia materna en México. Salud Pública De México 2013, 55, 170–179. [Google Scholar]
- Tang, L.; Lee, A.H.; Binns, C.W. Predictors of early introduction of complementary feeding: Longitudinal study. Pediatr. Int. 2014, 57, 126–130. [Google Scholar] [CrossRef]
- Vázquez-Osorio, I.M.; Vega-Sánchez, R.; Maas-Mendoza, E.; Rouassant, S.H.; Flores-Quijano, M.E. Exclusive Breastfeeding and Factors Influencing Its Abandonment During the 1st Month Postpartum Among Women From Semi-rural Communities in Southeast Mexico. Front. Pediatr. 2022, 10, 826295. [Google Scholar] [CrossRef]
- Prell, C.; Koletzko, B. Breastfeeding and Complementary Feeding. Dtsch. Ärzteblatt Int. 2016, 113, 435–444. [Google Scholar] [CrossRef] [Green Version]
- López-Romo, H. ACTUALIZACIÓN REGLA AMAI NSE 8 × 7 Congreso AMAI. 2011. Available online: http://www.amai.org/congreso/2011/ponencias/heriberto_lopez.pdf (accessed on 7 April 2021).
- Encuesta Nacional de Salud Y Nutrición 2012. Resultados Nacionales. Available online: https://paperpile.com/app/p/2ceca709-55e3-02b8-9bfb-1eccb6ed308c (accessed on 4 March 2022).
- Lohman, T.G.; Roch, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 1998; pp. 3–8, 39–70. [Google Scholar]
- WHO Anthro Survey Analyser. Available online: www.who.int.tools/child-growth-standards/software (accessed on 17 June 2021).
- World Health Organization; United Nations Children’s Fund (UNICEF). Indicators for Assessing Infant and Young Child Feeding Practices: Definitions and Measurement Methods; WHO/UNICEF: Geneva, Switzerland, 2021. [Google Scholar]
- González-Castell, L.D.; Unar-Munguía, M.; Quezada-Sánchez, A.D.; Bonvecchio-Arenas, A.; Rivera-Dommarco, J. Breastfeeding and complementary feeding practices in Mexico: Results from Ensanut 2018–19. Salud Publica Mex. 2020, 62, 704–713. [Google Scholar] [CrossRef]
- González de Cossío, T.; Escobar-Zaragoza, L.; González-Castell, D.; Reyes-Vázquez, H.; Rivera-Dommarco, J.A. Breastfeeding in Mexico Was Stable, on Average, but Deteriorated among the Poor, Whereas Complementary Feeding Improved: Results from the 1999 to 2006 National Health and Nutrition Surveys. J. Nutr. 2013, 143, 664–671. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Salud Pública y UNICEF México. Encuesta Nacional de Niños, Niñas Y Mujeres 2015—Encuesta de Indicadores Múltiples Por Conglomerados 2015, Informe Final; Instituto Nacional de Salud Pública y UNICEF: Ciudad de México, México, 2016. [Google Scholar]
- Hernández-Cordero, S.; Lozada-Tequeanes, A.L.; Fernández-Gaxiola, A.C.; Shamah-Levy, T.; Sachse, M.; Veliz, P.; Cosío-Barroso, I. Barriers and facilitators to breastfeeding during the immediate and one month postpartum periods, among Mexican women: A mixed methods approach. Int. Breastfeed. J. 2020, 15, 1–12. [Google Scholar] [CrossRef]
- Rivera-Pasquel, M.; Escobar-Zaragoza, L.; De Cosío, T.G. Breastfeeding and Maternal Employment: Results from Three National Nutritional Surveys in Mexico. Matern. Child Health J. 2014, 19, 1162–1172. [Google Scholar] [CrossRef]
- Navarro-Estrella, M.; Duque-López, M.X.; Trejo y Pérez, J.A. Factors associated with short duration of breast-feeding in Mexican working women. Salud Publica Mex. 2003, 45, 276–284. [Google Scholar]
- Lesorogol, C.; Bond, C.; Dulience, S.J.L.; Iannotti, L. Economic determinants of breastfeeding in Haiti: The effects of poverty, food insecurity, and employment on exclusive breastfeeding in an urban population. Matern. Child Nutr. 2017, 14, e12524. [Google Scholar] [CrossRef] [Green Version]
- Hight-Laukaran, V.; Rutstein, S.O.; Peterson, A.E.; Labbok, M.H. The use of breast milk substitutes in developing countries: The impact of women′s employment. Am. J. Public Health 1996, 86, 1235–1240. [Google Scholar] [CrossRef] [Green Version]
- Hasan, A.M.R.; Smith, G.; Selim, M.A.; Akter, S.; Khan, N.U.Z.; Sharmin, T.; Rasheed, S. Work and breast milk feeding: A qualitative exploration of the experience of lactating mothers working in ready made garments factories in urban Bangladesh. Int. Breastfeed. J. 2020, 15, 1–11. [Google Scholar] [CrossRef]
- Green, M.; Pries, A.M.; Hadihardjono, D.N.; Izwardy, D.; Zehner, E.; Moran, V.H. Breastfeeding and breastmilk substitute use and feeding motivations among mothers in Bandung City, Indonesia. Matern. Child Nutr. 2021, 17, e13189. [Google Scholar] [CrossRef]
- Amin, R.M.; Said, Z.M.; Sutan, R.; Shah, S.A.; Darus, A.; Shamsuddin, K. Work related determinants of breastfeeding discontinuation among employed mothers in Malaysia. Int. Breastfeed. J. 2011, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Cordero, S.; Lozada-Tequeanes, A.L.; Shamah-Levy, T.; Lutter, C.; González de Cosío, T.; Saturno-Hernández, P.; Rivera Dommarco, J.; Grummer-Strawn, L. Violations of the international code of marketing of Breast-Milk Substitutes in Mexico. Matern. Child Nutr. 2019, 15, e12682. [Google Scholar]
- Rothstein, J.D.; Winch, P.J.; Pachas, J.; Cabrera, L.Z.; Ochoa, M.; Gilman, R.H.; Caulfield, L.E. Vulnerable families and costly formula: A qualitative exploration of infant formula purchasing among peri-urban Peruvian households. Int. Breastfeed. J. 2021, 16, 1–15. [Google Scholar] [CrossRef]
- Sacco, L.M.; Caulfield, L.E.; Gittelsohn, J.; Martínez, H. The Conceptualization of Perceived Insufficient Milk among Mexican Mothers. J. Hum. Lact. 2006, 22, 277–286. [Google Scholar] [CrossRef]
- Neifert, M.R. Prevention of breastfeeding tragedies. Pediatr. Clin. N. Am. 2001, 48, 273–297. [Google Scholar] [CrossRef]
- Smith, L.J. Postpartum Care. In Breastfeeding and Human Lactation, 6th ed.; Wambach, K., Spencer, B., Eds.; Jones and Bartlett Learning: Burlington, MA, USA, 2021; pp. 247–280. [Google Scholar]
- Doak, C.M.; van der Starre, R.E.; van Beusekom, I.; Ponce, M.C.; Vossenaar, M.; Solomons, N.W. Earlier introduction of agüitas is associated with higher risk of stunting in infants and toddlers in the Western Highlands of Guatemala. Am. J. Clin. Nutr. 2013, 97, 631–636. [Google Scholar] [CrossRef] [Green Version]
- Gupta, N.; Gehri, M.; Stettler, N. Early introduction of water and complementary feeding and nutritional status of children in northern Senegal. Public Health Nutr. 2007, 10, 1299–1304. [Google Scholar] [CrossRef] [Green Version]
- Breastfeeding Q&A. Available online: https://www.who.int/news-room/q-a-detail/breastfeeding (accessed on 18 August 2021).
- Instituto Nacional de Salud Pública Encuesta. Nacional de Salud Y Nutrición 2012. Resultados Por Entidad Federativa, Tabasco; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2013. [Google Scholar]
- Trovão, T.; Cavalcante, M.C.V.; Rodrigues, M.C.; Ferraro, A.A.; Bettiol, H.; Saraiva, M.C.P.; Lamy, Z.C.; Lamy-Filho, F. Determinants of the introduction of early complementary feeding before and after the third month of life: A multinomial analysis. Braz. J. Med. Biol. Res. 2021, 54, e10115. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.-L. Theoretical Underpinnings of Breastfeeding Confidence: A Self-Efficacy Framework. J. Hum. Lact. 1999, 15, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, K.G.; Johnson, W.; Sonko, B.; Prentice, A.M.; Darboe, M.K.; Moore, S.E. Following the World Health Organization’s Recommendation of Exclusive Breastfeeding to 6 Months of Age Does Not Impact the Growth of Rural Gambian Infants. J. Nutr. 2016, 147, 248–255. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Maternal Characteristics (n = 143) | |
|---|---|
| Maternal age (years, median, p25–p75) | 23 (19–27) |
| Schooling (years, median, p25–p75) | 9 (8–12) |
| Lived with their infant’s father (n, %) | 123 (86.0) |
| Stay-at-home mother (n, %) | 127 (88.8) |
| Family type nuclear household (n, %) extended family (n, %) monoparental (n, %) | 79 (55.0) 60 (42.0) 4 (2.8) |
| At least one previous live birth (n, %) | 86 (60.1) |
| Low socioeconomic level (lowest three AMAI SEL categories) (n, %) | 105 (73.0) |
| Food insecurity mild (n, %) moderate (n, %) severe (n, %) | 68 (47.6) 26 (18.2) 16 (1.2) |
| Maternal BMI * (median, p25–p75) | 25.63 (22.6–29.0) |
| Infant Characteristics (n = 143) | |
| Vaginal delivery | 113 (79%) |
| Infants’ sex | 76 female (53.1%) |
| Infants’ age * (months, median, p25–p75) | 5.75 (4.8–6.3) |
| Infants’ LAZ (median, p25–p75) | −0.67 (−1.33–0.35) |
| Infants’ WAZ (median, p25–p75) | −0.14 (−0.98–0.63) |
| Factor | PR (Adjusted 95%CI) | p |
|---|---|---|
| Occupation | ||
| Works away from home (yes) | 1.27 (1.06, 1.54) | 0.011 |
| “Formula milk is an important food to accompany breast milk before six months” | ||
| Agree (yes) | 1.38 (1.19, 1.70) | 0.003 |
| “When you finish breastfeeding, you are always sure that your baby under six months is full” | ||
| Agree (yes) | 0.75 (0.61, 0.92) | 0.007 |
| PR (Adjusted 95%CI) | p | |
|---|---|---|
| During her prenatal care visits, the mother was told the optimal age to start CF is 6 months. | ||
| Yes | 1.17 (1.06, 1.29) | 0.002 |
| “I am convinced that giving only breast milk until the baby is six months old, without giving any other food, is the best for her/him” | ||
| Agree | 1.15 (1.03, 1.29) | 0.012 |
| “When the baby is not full, you should give her/him powdered milk or some other food, even if she/he is less than six months old” | ||
| Agree | 0.87 (0.78, 0.96) | 0.009 |
| WLZ | ||
| (at study visit) | 1.04 (1.00, 1.08) | 0.022 |
| LAZ | ||
| (at study visit) | 1.04 (1.00, 1.09) | 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maas-Mendoza, E.; Vega-Sánchez, R.; Vázquez-Osorio, I.M.; Heller-Rouassant, S.; Flores-Quijano, M.E. Infant Feeding Practices That Substitute Exclusive Breastfeeding in a Semi-Rural Mexican Community: Types, Moments, and Associated Factors. Nutrients 2022, 14, 2017. https://doi.org/10.3390/nu14102017
Maas-Mendoza E, Vega-Sánchez R, Vázquez-Osorio IM, Heller-Rouassant S, Flores-Quijano ME. Infant Feeding Practices That Substitute Exclusive Breastfeeding in a Semi-Rural Mexican Community: Types, Moments, and Associated Factors. Nutrients. 2022; 14(10):2017. https://doi.org/10.3390/nu14102017
Chicago/Turabian StyleMaas-Mendoza, Erick, Rodrigo Vega-Sánchez, Inocente Manuel Vázquez-Osorio, Solange Heller-Rouassant, and María Eugenia Flores-Quijano. 2022. "Infant Feeding Practices That Substitute Exclusive Breastfeeding in a Semi-Rural Mexican Community: Types, Moments, and Associated Factors" Nutrients 14, no. 10: 2017. https://doi.org/10.3390/nu14102017
APA StyleMaas-Mendoza, E., Vega-Sánchez, R., Vázquez-Osorio, I. M., Heller-Rouassant, S., & Flores-Quijano, M. E. (2022). Infant Feeding Practices That Substitute Exclusive Breastfeeding in a Semi-Rural Mexican Community: Types, Moments, and Associated Factors. Nutrients, 14(10), 2017. https://doi.org/10.3390/nu14102017