
Postnatal Serum Total Thyroxine Level Associated with Short- and Long-Term Anthropometric Outcomes in Very Preterm Infants

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting, Thyroid Function Screening Policy, and Study Design
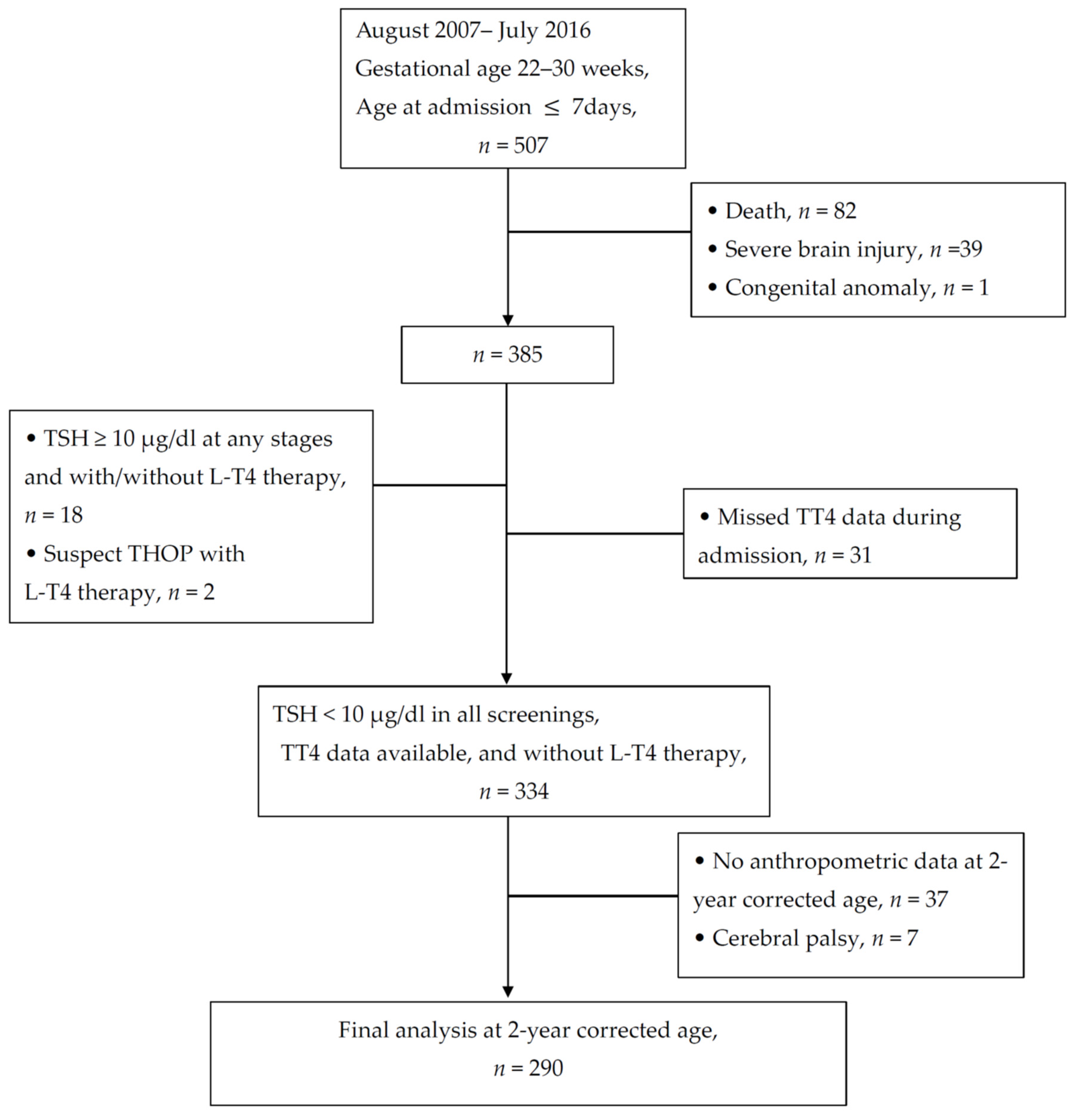
2.2. Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
- Maternal thyroid disease during pregnancy;
- Age > 7 days old at admission;
- Death at discharge;
- Severe brain injury, such as severe intraventricular hemorrhage (IVH) or periventricular leukomalacia (PVL), which may affect the hypothalamic–pituitary axis and thyroid function [6];
- Congenital anomalies or syndromic gene anomalies;
- Patients with any event of elevated TSH (≥10 μIU/mL) during serum or blood spot tests with/without thyroid hormone therapy at any stage;
- Treated with Levothyroxine;
- Total thyroxine and TSH data are not simultaneously available at stage II screening;
- Cerebral palsy, which may affect the measurement of anthropometry.
2.3. Independent Variable: Thyroid Function Data
2.4. Clinical Variables and Covariates
2.5. Outcomes
2.5.1. Primary Outcome
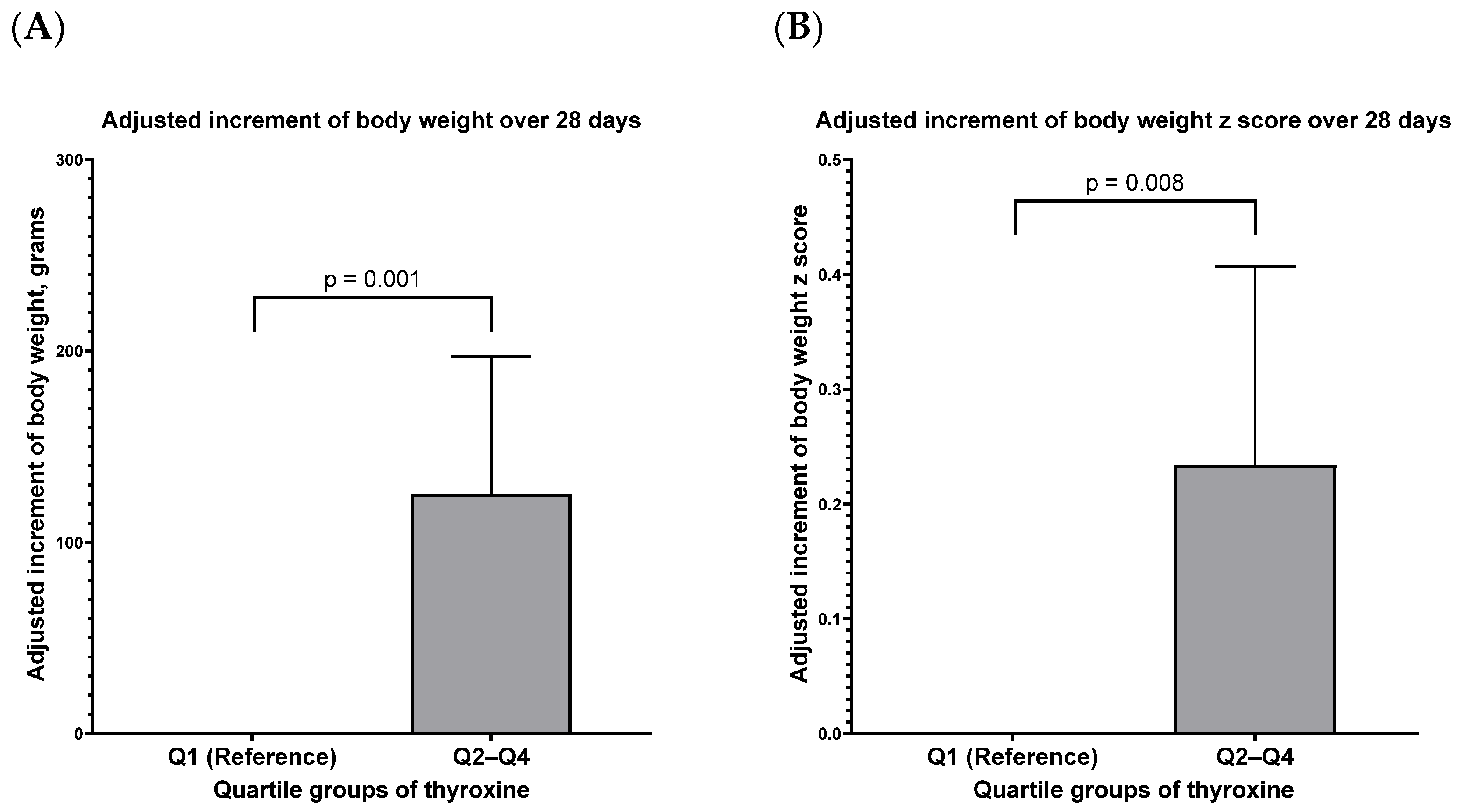
- Short-term growth: The increment in body weight and the z-score of body weight over 28 days after the screening in stage II were defined as the short-term outcomes.
- Long-term growth: The BMI z-score and weight status at the corrected age of 24 months were defined as the long-term outcomes.
2.5.2. Secondary Outcomes
2.6. Statistical Analysis
3. Results
3.1. The Enrollment of Neurologically Intact Survivors with Complete Thyroid Function Profiles during Hospitalization
3.2. The Association between Serum Total Thyroxine Concentration and the 28-Day Growth Increment after Stage II Screening
3.3. Dependence of the 24-Month Z-Score of BMI on Clinical Variables and Thyroxine
3.4. Lower Postnatal Thyroxine Concentrations Associated with Overweight Status at the Corrected Age of 24 Months
4. Discussion
4.1. Extra-Uterine Growth of Very Preterm Infants and Postnatal Thyroxine Concentration
4.2. Long-Term Anthropometry and Thyroxine Concentration in Early Life
4.3. The Optimal Total Thyroxine Concentration for Very Preterm Infants
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wassner, A.J.; Brown, R.S. Hypothyroidism in the newborn period. Curr. Opin. Endocrinol. Diabetes Obes. 2013, 20, 449–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wassner, A.J.; Brown, R.S. Congenital hypothyroidism: Recent advances. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-W. Three Decades of Newborn Screening in Taiwan; Health Promotion Administration, Ministry of Health and Welfare: Taichung, Taiwan, 2016. [Google Scholar]
- Ford, G.; LaFranchi, S.H. Screening for congenital hypothyroidism: A worldwide view of strategies. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Soneda, A.; Adachi, M.; Muroya, K.; Asakura, Y.; Yamagami, Y.; Hirahara, F. Overall usefulness of newborn screening for congenital hypothyroidism by using free thyroxine measurement. Endocr. J. 2014, 61, 1025–1030. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.R.; Jung, Y.H.; Choi, C.W.; Chung, H.R.; Kang, M.J.; Kim, B.I. Thyroid dysfunction in preterm infants born before 32 gestational weeks. BMC Pediatr. 2019, 19, 391. [Google Scholar] [CrossRef]
- Grob, F. Approaching the diagnosis of thyroid disorders in preterm infants. Pediatr. Res. 2022. [Google Scholar] [CrossRef]
- Hollanders, J.J.; Israels, J.; van der Pal, S.M.; Verkerk, P.H.; Rotteveel, J.; Finken, M.J.; Dutch, P.-C.S.G. No Association Between Transient Hypothyroxinemia of Prematurity and Neurodevelopmental Outcome in Young Adulthood. J. Clin. Endocrinol. Metab. 2015, 100, 4648–4653. [Google Scholar] [CrossRef] [Green Version]
- Flores-Robles, C.M.; Roldan-Valadez, E.; Martinez-Cruz, N.; Arce-Sanchez, L.; Priego-Zurita, A.L.; Estrada-Gutierrez, G.; Reyes-Munoz, E. Reference Percentiles and Changes over Time for Total Thyroxine in Preterm Infants: A Retrospective Cohort Study. Diagnostics 2020, 10, 475. [Google Scholar] [CrossRef]
- Eerdekens, A.; Langouche, L.; Van den Berghe, G.; Verhaeghe, J.; Naulaers, G.; Vanhole, C. Review shows that thyroid hormone substitution could benefit transient hypothyroxinaemia of prematurity but treatment strategies need to be clarified. Acta Paediatr. 2019, 108, 792–805. [Google Scholar] [CrossRef]
- Iijima, S. Current knowledge of transient hypothyroxinemia of prematurity: To treat or not to treat? J. Matern. Fetal Neonatal Med. 2019, 32, 2591–2597. [Google Scholar] [CrossRef]
- Kaluarachchi, D.C.; Allen, D.B.; Eickhoff, J.C.; Dawe, S.J.; Baker, M.W. Thyroid-Stimulating Hormone Reference Ranges for Preterm Infants. Pediatrics 2019, 144, e20190290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler, G.M.; Slaughter, J.L.; Chaudhari, M.; Singh, H.; Sanchez, P.J.; Bunch, D.R. Preterm to term infant postmenstrual age reference intervals for thyroid-stimulating hormone and free thyroxine. Pediatr. Res. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics; Rose, S.R.; Section on Endocrinology and Committee on Genetics; American Thyroid Association; Brown, R.S.; Public Health Committee; Lawson Wilkins Pediatric Endocrine Society. Update of newborn screening and therapy for congenital hypothyroidism. Pediatrics 2006, 117, 2290–2303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, D.A. Thyroid function and dysfunction in premature infants. Pediatr. Endocrinol. Rev. 2007, 4, 317–328. [Google Scholar]
- Osborn, D.A.; Hunt, R.W. Prophylactic postnatal thyroid hormones for prevention of morbidity and mortality in preterm infants. Cochrane Database Syst. Rev. 2007, CD005948. [Google Scholar] [CrossRef]
- Lin, Y.-C.; Wang, C.-Y.; Pan, Y.-W.; Chen, Y.-J.; Yu, W.-H.; Chou, Y.-Y.; Huang, C.-H.; Chu, W.-Y.; Lin, C.-H.; Iwata, O. Postnatal Serum Total Thyroxine of Very Preterm Infants and Long-Term Neurodevelopmental Outcome. Nutrients 2021, 13, 1055. [Google Scholar] [CrossRef]
- Uchiyama, A.; Kushima, R.; Watanabe, T.; Kusuda, S. Effect of L-thyroxine supplementation on very low birth weight infants with transient hypothyroxinemia of prematurity at 3 years of age. J. Perinatol. 2017, 37, 602–605. [Google Scholar] [CrossRef]
- Uchiyama, A.; Kushima, R.; Watanabe, T.; Kusuda, S. Effect of l-thyroxine supplementation on infants with transient hypothyroxinemia of prematurity at 18 months of corrected age: Randomized clinical trial. J. Pediatr. Endocrinol. Metab. 2015, 28, 177–182. [Google Scholar] [CrossRef]
- van Wassenaer-Leemhuis, A.; Ares, S.; Golombek, S.; Kok, J.; Paneth, N.; Kase, J.; LaGamma, E.F. Thyroid hormone supplementation in preterm infants born before 28 weeks gestational age and neurodevelopmental outcome at age 36 months. Thyroid 2014, 24, 1162–1169. [Google Scholar] [CrossRef] [Green Version]
- Briet, J.M.; van Wassenaer, A.G.; Dekker, F.W.; de Vijlder, J.J.; van Baar, A.; Kok, J.H. Neonatal thyroxine supplementation in very preterm children: Developmental outcome evaluated at early school age. Pediatrics 2001, 107, 712–718. [Google Scholar] [CrossRef]
- Ng, S.M.; Turner, M.A.; Weindling, A.M. Neurodevelopmental Outcomes at 42 Months After Thyroxine Supplementation in Infants Below 28 Weeks’ Gestation: A Randomized Controlled Trial. Thyroid 2020, 30, 948–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, L.O.; Tan, M.G.; Poon, W.B. Lack of association between hypothyroxinemia of prematurity and transient thyroid abnormalities with adverse long term neurodevelopmental outcome in very low birth weight infants. PLoS ONE 2019, 14, e0222018. [Google Scholar] [CrossRef]
- Williams, F.L.R.; Ogston, S.; Hume, R.; Watson, J.; Stanbury, K.; Willatts, P.; Boelen, A.; Juszczak, E.; Brocklehurst, P.; Team, I.S. Supplemental Iodide for Preterm Infants and Developmental Outcomes at 2 Years: An RCT. Pediatrics 2017, 139, e20163703. [Google Scholar] [CrossRef] [Green Version]
- Ares, S.; Quero, J.; Diez, J.; de Escobar, G.M. Neurodevelopment of preterm infants born at 28 to 36 weeks of gestational age: The role of hypothyroxinemia and long-term outcome at 4 years. J. Pediatr. Endocrinol. Metab. 2011, 24, 897–902. [Google Scholar] [CrossRef]
- Eerdekens, A.; Naulaers, G.; Ortibus, E.; Verhaeghe, J.; Langouche, L.; Vanhole, C. Evolution of circulating thyroid hormone levels in preterm infants during the first week of life: Perinatal influences and impact on neurodevelopment. J. Pediatr. Endocrinol. Metab. 2019, 32, 597–606. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Yu, W.-H.; Chen, L.-W.; Huang, C.-C.; Kang, L.; Lin, H.-S.; Iwata, O.; Kato, S.; Hussein, M.H.; Lin, Y.-C. Improved Survival of Periviable Infants after Alteration of the Threshold of Viability by the Neonatal Resuscitation Program 2015. Children 2021, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Shin, S.H.; Cho, H.; Shin, S.H.; Kim, S.H.; Song, I.G.; Kim, E.K.; Kim, H.S. Extrauterine growth restriction in extremely preterm infants based on the Intergrowth-21st Project Preterm Postnatal Follow-up Study growth charts and the Fenton growth charts. Eur. J. Pediatr. 2020, 180, 817–824. [Google Scholar] [CrossRef]
- WHO. WHO Anthro Survey Analyser and Other Tools. Available online: https://www.who.int/tools/child-growth-standards/software (accessed on 12 March 2022).
- Barlow, S.E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120 (Suppl. 4), S164–S192. [Google Scholar] [CrossRef] [Green Version]
- Walsh, V.; Brown, J.V.E.; Copperthwaite, B.R.; Oddie, S.J.; McGuire, W. Early full enteral feeding for preterm or low birth weight infants. Cochrane Database Syst. Rev. 2020, 12, Cd013542. [Google Scholar] [CrossRef]
- Dorling, J.; Abbott, J.; Berrington, J.; Bosiak, B.; Bowler, U.; Boyle, E.; Embleton, N.; Hewer, O.; Johnson, S.; Juszczak, E.; et al. Controlled Trial of Two Incremental Milk-Feeding Rates in Preterm Infants. N. Engl. J. Med. 2019, 381, 1434–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, C.; Franz, A.R.; von Krogh, S.; Arand, J.; Poets, C.F. Growth and morbidity of extremely preterm infants after early full enteral nutrition. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F79–F81. [Google Scholar] [CrossRef] [PubMed]
- Eng, L.; Lam, L. Thyroid Function During the Fetal and Neonatal Periods. Neoreviews 2020, 21, e30–e36. [Google Scholar] [CrossRef] [PubMed]
- Eerdekens, A.; Verhaeghe, J.; Darras, V.; Naulaers, G.; Van den Berghe, G.; Langouche, L.; Vanhole, C. The placenta in fetal thyroid hormone delivery: From normal physiology to adaptive mechanisms in complicated pregnancies. J. Matern. Fetal Neonatal Med. 2020, 33, 3857–3866. [Google Scholar] [CrossRef] [PubMed]
- Belet, N.; Imdat, H.; Yanik, F.; Kucukoduk, S. Thyroid function tests in preterm infants born to preeclamptic mothers with placental insufficiency. J. Pediatr. Endocrinol. Metab. 2003, 16, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Carriero, R.; Andermann, E.; Chen, M.F.; Eeg-Oloffson, O.; Kinch, R.A.; Klein, G.; Murphy, B.E. Thyroid function in epileptic mothers and their infants at birth. Am. J. Obstet. Gynecol. 1985, 151, 641–644. [Google Scholar] [CrossRef]
- Ballard, P.L.; Ballard, R.A.; Creasy, R.K.; Padbury, J.; Polk, D.H.; Bracken, M.; Moya, F.R.; Gross, I. Plasma thyroid hormones and prolactin in premature infants and their mothers after prenatal treatment with thyrotropin-releasing hormone. Pediatr. Res. 1992, 32, 673–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avramovska, M.; Karanfilski, B.; Dimitrov, G.; Dzikova, E.; Markova, A.D.; Lega, M.H.; Tofoski, G.; Sikole, A. Isolated Maternal Hypothyroxinemia and Its Perinatal Outcome in North Macedonia. Acta Clin. Croat. 2021, 60, 246–253. [Google Scholar] [CrossRef]
- Charoenratana, C.; Leelapat, P.; Traisrisilp, K.; Tongsong, T. Maternal iodine insufficiency and adverse pregnancy outcomes. Matern. Child. Nutr. 2016, 12, 680–687. [Google Scholar] [CrossRef]
- Chen, L.M.; Du, W.J.; Dai, J.; Zhang, Q.; Si, G.X.; Yang, H.; Ye, E.L.; Chen, Q.S.; Yu, L.C.; Zhang, C.; et al. Effects of subclinical hypothyroidism on maternal and perinatal outcomes during pregnancy: A single-center cohort study of a Chinese population. PLoS ONE 2014, 9, e109364. [Google Scholar] [CrossRef] [Green Version]
- Fan, J.; Zhang, Y.; Zhang, C.; Barjaktarovic, M.; Yang, X.; Peeters, R.P.; Huang, H.F.; Korevaar, T.I.M. Persistency of Thyroid Dysfunction from Early to Late Pregnancy. Thyroid 2019, 29, 1475–1484. [Google Scholar] [CrossRef] [PubMed]
- Saki, F.; Dabbaghmanesh, M.H.; Ghaemi, S.Z.; Forouhari, S.; Omrani, G.R.; Bakhshayeshkaram, M. Thyroid function in pregnancy and its influences on maternal and fetal outcomes. Int. J. Endocrinol. Metab. 2014, 12, e19378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitoris, G.; Veltri, F.; Kleynen, P.; Cogan, A.; Belhomme, J.; Rozenberg, S.; Pepersack, T.; Poppe, K. The Impact of Thyroid Disorders on Clinical Pregnancy Outcomes in a Real-World Study Setting. Thyroid 2020, 30, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Liu, Y.; Maraka, S.; Abdelouahab, N.; Huang, H.F.; Fraser, W.D.; Fan, J. Pregnancy and Neonatal Outcomes With Levothyroxine Treatment in Women With Subclinical Hypothyroidism Based on New Diagnostic Criteria: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2021, 12, 797423. [Google Scholar] [CrossRef]
- Maraka, S.; Ospina, N.M.S.; O’Keeffe, D.T.; Rodriguez-Gutierrez, R.; De Ycaza, A.E.E.; Wi, C.I.; Juhn, Y.J.; Coddington, C.C., 3rd; Montori, V.M.; Stan, M.N. Effects of Levothyroxine Therapy on Pregnancy Outcomes in Women with Subclinical Hypothyroidism. Thyroid 2016, 26, 980–986. [Google Scholar] [CrossRef] [Green Version]
- Feizi, A.; Hashemipour, M.; Hovsepian, S.; Amirkhani, Z.; Kelishadi, R.; Yazdi, M.; Heydari, K.; Sajadi, A.; Amini, M. Growth and Specialized Growth Charts of Children with Congenital Hypothyroidism Detected by Neonatal Screening in Isfahan, Iran. ISRN Endocrinol. 2013, 2013, 463939. [Google Scholar] [CrossRef]
- Kik, E.; Noczyńska, A. Evaluation of physical development of children with congenital hypothyroidism detected in the screening test--personal observations. Pediatr. Endocrinol. Diabetes Metab. 2011, 17, 96–106. [Google Scholar]
- Sun, Q.; Chen, Y.-L.; Yu, Z.-B.; Han, S.-P.; Dong, X.-Y.; Qiu, Y.-F.; Sha, L.; Guo, X.-R. Long-term Consequences of the Early Treatment of Children with Congenital Hypothyroidism Detected by Neonatal Screening in Nanjing, China: A 12-year Follow-up Study. J. Trop. Pediatr. 2011, 58, 79–80. [Google Scholar] [CrossRef] [Green Version]
- Grant, D.B. Growth in early treated congenital hypothyroidism. Arch. Dis. Child. 1994, 70, 464–468. [Google Scholar] [CrossRef] [Green Version]
- Leon, G.; Murcia, M.; Rebagliato, M.; Alvarez-Pedrerol, M.; Castilla, A.M.; Basterrechea, M.; Iniguez, C.; Fernandez-Somoano, A.; Blarduni, E.; Foradada, C.M.; et al. Maternal thyroid dysfunction during gestation, preterm delivery, and birthweight. The Infancia y Medio Ambiente Cohort, Spain. Paediatr. Perinat. Epidemiol. 2015, 29, 113–122. [Google Scholar] [CrossRef]
- Selva, K.A.; Mandel, S.H.; Rien, L.; Sesser, D.; Miyahira, R.; Skeels, M.; Nelson, J.C.; Lafranchi, S.H. Initial treatment dose of L-thyroxine in congenital hypothyroidism. J. Pediatr. 2002, 141, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Chen, Y.J.; Huang, C.C.; Shieh, C.C. Concentrated Preterm Formula as a Liquid Human Milk Fortifier at Initiation Stage in Extremely Low Birth Weight Preterm Infants: Short Term and 2-year Follow-up Outcomes. Nutrients 2020, 12, 2229. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.L.R.; Lindgren, A.; Watson, J.; Boelen, A.; Cheetham, T. Thyroid function in preterm infants and neurodevelopment at 2 years. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 105, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Deming, D.D.; Rabin, C.W.; Hopper, A.O.; Peverini, R.L.; Vyhmeister, N.R.; Nelson, J.C. Direct equilibrium dialysis compared with two non-dialysis free T4 methods in premature infants. J. Pediatr. 2007, 151, 404–408. [Google Scholar] [CrossRef] [PubMed]
- LaFranchi, S.H. Thyroid Function in Preterm/Low Birth Weight Infants: Impact on Diagnosis and Management of Thyroid Dysfunction. Front. Endocrinol. 2021, 12, 666207. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N for Analysis | 290 |
|---|---|
| Maternal and antenatal variables | |
| Maternal age, years | 32.1 ± 4.8 |
| Maternal education level (≥ college), n (%) | 170 (58.6) |
| Antenatal steroid, n (%) | 255 (87.9) |
| Pre-eclampsia, n (%) | 58 (20) |
| Gestational diabetes mellitus, n (%) | 12 (4.1) |
| Variables in perinatal period | |
| Gestational age, weeks | 27.6 ± 1.9 |
| Body weight at birth, grams | 1030 ± 242 |
| Z-score of body weight at birth | −0.210 ± 0.749 |
| Sex, male, n (%) | 159 (54.8) |
| Method of delivery, Cesarean section, n (%) | 166 (57.2) |
| Inborn, n (%) | 248 (85.5) |
| Multi-gestation, n (%) | 81 (27.9) |
| Resuscitation at birth (Intubation), n (%) | 21 (7.2) |
| Apgar score at 5 min, median (IQR) | 8 (7–9) |
| Early onset sepsis, n (%) | 7 (2.4) |
| Variables during hospital stay | |
| Surfactant-treated respiratory distress syndrome, n (%) | 75 (25.9) |
| Late-onset sepsis, n (%) | 49 (16.9) |
| Necrotizing enterocolitis (stage ≥ 2), n (%) | 13 (4.5) |
| Treated retinopathy of prematurity, n (%) | 23 (7.9) |
| Chronic lung disease (CLD), n (%) | 89 (30.7) |
| Postnatal steroid for CLD, n (%) | 25 (8.6) |
| Variables at thyroid function screening at stage II | |
| Postnatal age, days | 29.9 ± 4.9 |
| Postmenstrual age, weeks | 31.9 ± 1.9 |
| Serum thyroid-stimulating hormone, μIU/mL | 3.42 ± 1.94 |
| Serum total thyroxine concentration, μg/dL; | 6.58 ± 1.95 |
| Variables at discharge | |
| Postnatal age, days | 67.2 ± 25.6 |
| Postmenstrual age at discharge, weeks | 37.1 ± 2.5 |
| Increment in Bodyweight, Gram | Increment of Bodyweight z-Score | ||||||
|---|---|---|---|---|---|---|---|
| Reference | Mean | 95% CI | p-Value | Mean | 95% CI | p-Value | |
| Time after the screening, day | 21.5 | 20.3, 22.8 | <0.001 | −0.018 | −0.02, −0.015 | <0.001 | |
| GA, week | 145.8 | 129.1, 162.5 | <0.001 | −0.093 | −0.133, −0.053 | <0.001 | |
| SGA | no | −419.3 | −503.5, −335.1 | <0.001 | −1.261 | −1.484, −1.039 | <0.001 |
| Sex | female | 150.3 | 93.8, 206.8 | <0.001 | 0.074 | −0.066, 0.215 | 0.300 |
| Prenatal steroid | no | 36.1 | −39.9, 112.0 | 0.352 | 0.090 | −0.110, 0.290 | 0.379 |
| Surfactant for RDS | no | −23.7 | −90.3, 42.9 | 0.486 | −0.073 | −0.247, 0.102 | 0.414 |
| TT4, μg/dL | 25.7 | 11.3, 40.2 | <0.001 | 0.039 | 0.002, 0.075 | 0.037 | |
| Multivariate Model 1 | Multivariate Model 2 | Multivariate Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | 95% CI | p | β | 95% CI | p | β | 95% CI | p | |
| Gestational age | 0.063 | −0.031, 0.156 | 0.187 | 0.116 | 0.021, 0.210 | 0.016 | |||
| Birth body weight | 0.001 | 0.001, 0.002 | 0.001 | ||||||
| z-score of birth body weight | 0.448 | 0.247, 0.650 | <0.001 | ||||||
| Small for gestational age | −0.470 | −0.958, 0.019 | 0.060 | −0.127 | −0.631, 0.377 | 0.619 | |||
| Sex | −0.044 | −0.312, 0.224 | 0.744 | −0.145 | −0.415, 0.126 | 0.293 | −0.042 | −0.303, 0.219 | 0.752 |
| Pre-eclampsia | −0.400 | −0.756, −0.044 | 0.028 | −0.264 | −0.611, 0.083 | 0.135 | −0.157 | −0.523, 0.21 | 0.401 |
| Surfactant for RDS | −0.152 | −0.466, 0.162 | 0.341 | −0.143 | −0.445, 0.158 | 0.351 | −0.187 | −0.492, 0.118 | 0.228 |
| Surgery for PDA | −0.200 | −0.605, 0.204 | 0.331 | −0.111 | −0.506, 0.284 | 0.581 | −0.174 | −0.567, 0.219 | 0.385 |
| Surgery for ROP | −0.346 | −0.886, 0.195 | 0.209 | −0.238 | −0.769, 0.292 | 0.377 | −0.252 | −0.78, 0.276 | 0.348 |
| Postnatal steroid | −0.601 | −1.128, −0.074 | 0.026 | −0.488 | −0.998, 0.022 | 0.060 | −0.489 | −1.001, 0.024 | 0.061 |
| Total thyroxine, μg/dL | −0.074 | −0.148, 0.000 | 0.050 | −0.104 | −0.177, −0.03 | 0.006 | −0.097 | −0.170, −0.024 | 0.009 |
| Weight Status Category | Underweight (BMI < 5 Percentile) | Overweight (BMI ≥ 85 Percentile) | Obese (BMI ≥ 95 Percentile) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Thyroxine Concentration Quartiles | Ref. | aOR | 95% CI | p | aOR | 95% CI | p | aOR | 95% CI | p |
| Q2–Q4 | Q1 | 0.457 | 0.160, 1.304 | 0.143 | 0.342 | 0.040, 2.894 | 0.342 | 0.387 | 0.111, 1.351 | 0.387 |
| Q3–Q4 | Q1–Q2 | 1.065 | 0.378, 3.304 | 0.146 | 0.358 | 0.174, 0.737 | 0.005 | 0.498 | 0.165, 1.506 | 0.498 |
| Q4 | Q1–Q3 | 1.078 | 0.320, 3.635 | 0.136 | 0.839 | 0.387, 1.781 | 0.633 | 0.797 | 0.236, 2.689 | 0.715 |
| Multivariate Model 1 | Multivariate Model 2 | ||||||
|---|---|---|---|---|---|---|---|
| Reference | aOR | 95% CI | p | aOR | 95% CI | p | |
| Gestational age | 1.340 | 1.019, 1.761 | 0.036 | 1.343 | 1.026, 1.757 | 0.032 | |
| Z-score of birth body weight | 2.535 | 1.385, 4.64 | 0.003 | 2.574 | 1.401, 4.728 | 0.002 | |
| Sex | female | 0.821 | 0.416, 1.62 | 0.570 | 0.832 | 0.422, 1.639 | 0.594 |
| Pre-eclampsia | No | 0.687 | 0.224, 2.105 | 0.511 | 0.716 | 0.234, 2.19 | 0.558 |
| Surfactant for RDS | No | 0.993 | 0.433, 2.274 | 0.986 | 0.989 | 0.432, 2.264 | 0.979 |
| Surgery for PDA | No | 1.059 | 0.338, 3.315 | 0.922 | 1.084 | 0.345, 3.408 | 0.890 |
| Surgery for ROP | No | 0.353 | 0.039, 3.172 | 0.352 | 0.418 | 0.047, 3.695 | 0.433 |
| Postnatal steroid | no | 0.397 | 0.046, 3.456 | 0.402 | 0.382 | 0.043, 3.356 | 0.385 |
| Total thyroxine, μg/dL | 0.782 | 0.633, 0.966 | 0.022 | ||||
| Total thyroxine, Q3–Q4 | Q1–Q2 | 0.365 | 0.177, 0.754 | 0.006 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-J.; Chu, W.-Y.; Pan, Y.-W.; Wang, C.-Y.; Chou, Y.-Y.; Lin, C.-H.; Tsuda, K.; Iwata, O.; Yu, W.-H.; Lin, Y.-C. Postnatal Serum Total Thyroxine Level Associated with Short- and Long-Term Anthropometric Outcomes in Very Preterm Infants. Nutrients 2022, 14, 2056. https://doi.org/10.3390/nu14102056
Chen Y-J, Chu W-Y, Pan Y-W, Wang C-Y, Chou Y-Y, Lin C-H, Tsuda K, Iwata O, Yu W-H, Lin Y-C. Postnatal Serum Total Thyroxine Level Associated with Short- and Long-Term Anthropometric Outcomes in Very Preterm Infants. Nutrients. 2022; 14(10):2056. https://doi.org/10.3390/nu14102056
Chicago/Turabian StyleChen, Yen-Ju, Wei-Ying Chu, Yu-Wen Pan, Chen-Yueh Wang, Yen-Yin Chou, Chyi-Her Lin, Kennosuke Tsuda, Osuke Iwata, Wen-Hao Yu, and Yung-Chieh Lin. 2022. "Postnatal Serum Total Thyroxine Level Associated with Short- and Long-Term Anthropometric Outcomes in Very Preterm Infants" Nutrients 14, no. 10: 2056. https://doi.org/10.3390/nu14102056
APA StyleChen, Y.-J., Chu, W.-Y., Pan, Y.-W., Wang, C.-Y., Chou, Y.-Y., Lin, C.-H., Tsuda, K., Iwata, O., Yu, W.-H., & Lin, Y.-C. (2022). Postnatal Serum Total Thyroxine Level Associated with Short- and Long-Term Anthropometric Outcomes in Very Preterm Infants. Nutrients, 14(10), 2056. https://doi.org/10.3390/nu14102056