
Prenatal Environmental Exposure to Persistent Organic Pollutants and Indices of Overweight and Cardiovascular Risk in Dutch Adolescents

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Prenatal Levels of POPs
2.3. Measurement of Anthropometric Measurements at Adolescence
2.4. Assessment of Hormones and Cardiovascular Markers at Adolescence
2.5. Statistical Analyses
3. Results
3.1. Study Group
3.2. Maternal Characteristics and Outcomes in Offspring at Adolescence
3.3. Anthropometric Measurements and Blood Pressure
3.4. Hormones and Metabolic Cardiovascular Markers
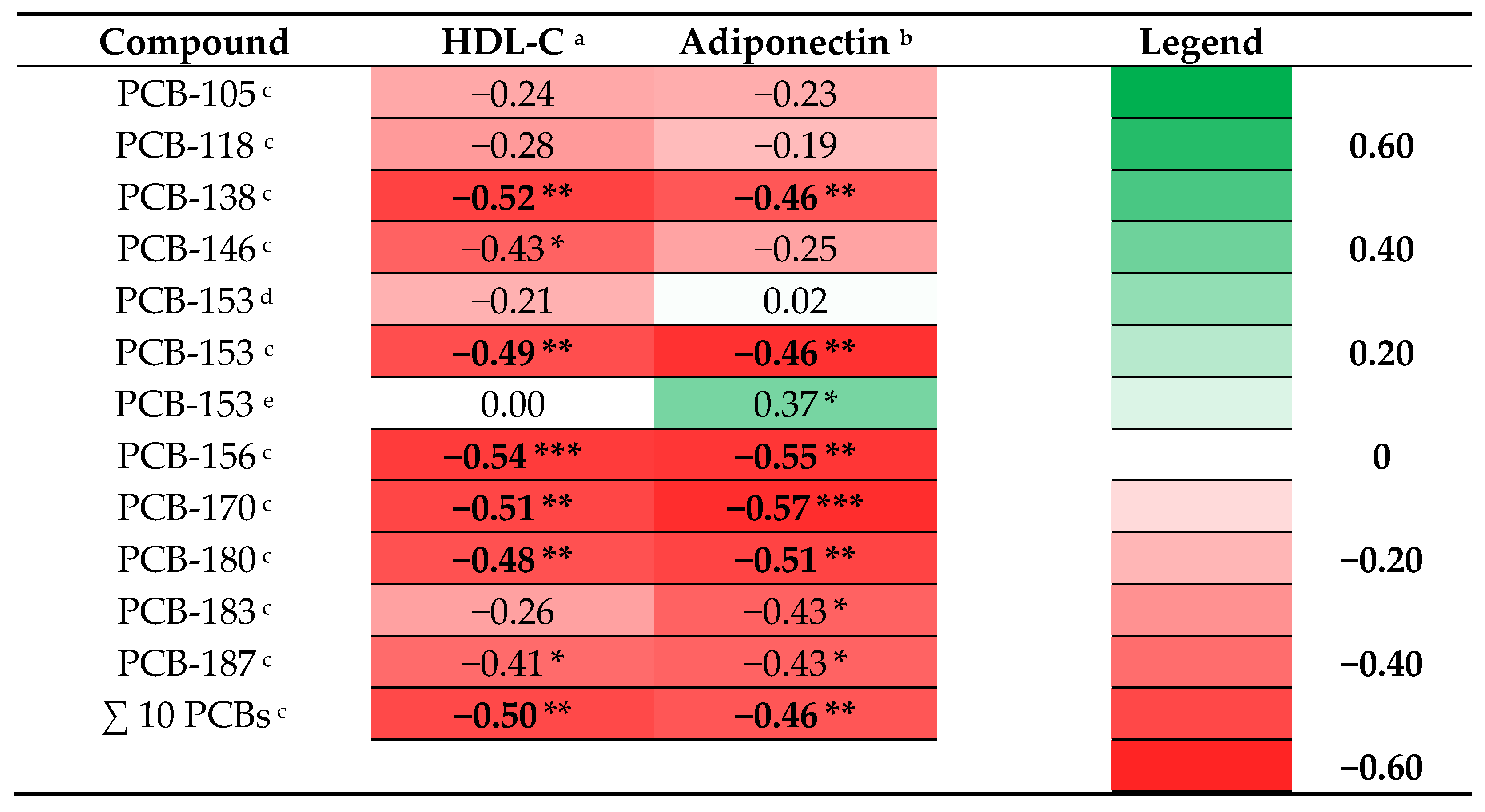
3.5. Prenatal PCB Levels and Indices for Overweight and Cardiovascular Risk in Adolescence
3.6. Prenatal PBDE Levels and Indices for Overweight and Cardiovascular Risk in Adolescence
3.7. Prenatal OH-PCB, DDE, PCP, HBCDD, and Outcomes in Adolescence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Botton, J.; Kadawathagedara, M.; de Lauzon-Guillain, B. Endocrine disrupting chemicals and growth of children. Ann. D’endocrinologie 2017, 78, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Faroon, O.M.; Keith, L.S.; Smith-Simon, C.; De Rosa, C.T. Polychlorinated Biphenyls: Human Health Aspects; Concise international Chemical Assessment Document; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Soechitram, S.D.; Athanasiadou, M.; Hovander, L.; Bergman, A.; Sauer, P.J. Fetal Exposure to PCBs and Their Hydroxylated Metabolites in a Dutch Cohort. Environ. Health Perspect. 2004, 112, 1208–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyer, D.B.; Meredith, R.M. Environmental toxicology: Sensitive periods of development and neurodevelopmental disorders. NeuroToxicology 2017, 58, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Shafei, A.E.-S.; Nabih, E.S.; Shehata, K.A.; Elfatah, E.S.M.A.; Sanad, A.B.A.; Marey, M.Y.; Hammouda, A.A.M.A.; Mohammed, M.M.M.; Mostafa, R.; Ali, M.A. Prenatal Exposure to Endocrine Disruptors and Reprogramming of Adipogenesis: An Early-Life Risk Factor for Childhood Obesity. Child. Obes. 2018, 14, 18–25. [Google Scholar] [CrossRef]
- Liu, Y.; Peterson, K.E. Maternal Exposure to Synthetic Chemicals and Obesity in the Offspring: Recent Findings. Curr. Environ. Health Rep. 2015, 2, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Khalil, N.; Chen, A.; Lee, M. Endocrine disruptive compounds and cardio-metabolic risk factors in children. Curr. Opin. Pharmacol. 2014, 19, 120–124. [Google Scholar] [CrossRef]
- Heindel, J.J.; Vom Saal, F.S.; Blumberg, B.; Bovolin, P.; Calamandrei, G.; Ceresini, G.; Cohn, B.A.; Fabbri, E.; Gioiosa, L.; Kassotis, C.; et al. Parma consensus statement on metabolic disruptors. Environ. Health 2015, 14, 54. [Google Scholar] [CrossRef] [Green Version]
- La Merrill, M.; Emond, C.; Kim, M.J.; Antignac, J.-P.; Le Bizec, B.; Clément, K.; Birnbaum, L.S.; Barouki, R. Toxicological Function of Adipose Tissue: Focus on Persistent Organic Pollutants. Environ. Health Perspect. 2013, 121, 162–169. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, S.; Sata, F.; Miyashita, C.; Miura, R.; Azumi, K.; Kobayashi, S.; Goudarzi, H.; Araki, A.; Ishizuka, M.; Todaka, T.; et al. Gender-specific association of exposure to non-dioxin-like polychlorinated biphenyls during pregnancy with methylation levels of H19 and long interspersed nuclear element-1 in cord blood in the Hokkaido study. Toxicology 2017, 390, 135–145. [Google Scholar] [CrossRef]
- Stratakis, N.; Rock, S.; La Merrill, M.A.; Saez, M.; Robinson, O.; Fecht, D.; Vrijheid, M.; Valvi, D.; Conti, D.V.; McConnell, R.; et al. Prenatal exposure to persistent organic pollutants and childhood obesity: A systematic review and meta-analysis of human studies. Obes. Rev. 2021, 23, e13383. [Google Scholar] [CrossRef]
- Gladen, B.C.; Ragan, N.B.; Rogan, W.J. Pubertal growth and development and prenatal and lactational exposure to polychlorinated biphenyls and dichlorodiphenyl dichloroethene. J. Pediatr. 2000, 136, 490–496. [Google Scholar] [CrossRef]
- Blanck, H.M.; Marcus, M.; Rubin, C.; Tolbert, P.E.; Hertzberg, V.S.; Henderson, A.K.; Zhang, R.H. Growth in Girls Exposed In Utero and Postnatally to Polybrominated Biphenyls and Polychlorinated Biphenyls. Epidemiology 2002, 13, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Dallaire, R.; Dewailly, É.; Ayotte, P.; Forget-Dubois, N.; Jacobson, S.W.; Jacobson, J.L.; Muckle, G. Growth in Inuit children exposed to polychlorinated biphenyls and lead during fetal development and childhood. Environ. Res. 2014, 134, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karmaus, W.; Osuch, J.R.; Eneli, I.; Mudd, L.M.; Zhang, J.; Mikucki, D.; Haan, P.; Davis, S. Maternal levels of dichlorodiphenyl-dichloroethylene (DDE) may increase weight and body mass index in adult female offspring. Occup. Environ. Med. 2009, 66, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warner, M.; Ye, M.; Harley, K.; Kogut, K.; Bradman, A.; Eskenazi, B. Prenatal DDT exposure and child adiposity at age 12: The CHAMACOS study. Environ. Res. 2017, 159, 606–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Shin, H.J.; Ding, E.L.; Van Dam, R.M. Adiponectin levels and risk of type 2 diabetes: A systematic review and meta-analysis. JAMA 2009, 302, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Jaramillo, P.; Gómez-Arbeláez, D.; López-López, J.; López-López, C.; Martínez-Ortega, J.; Gómez-Rodríguez, A.; Triana-Cubillos, S. The role of leptin/adiponectin ratio in metabolic syndrome and diabetes. Horm. Mol. Biol. Clin. Investig. 2014, 18, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Güil-Oumrait, N.; Valvi, D.; Garcia-Esteban, R.; Guxens, M.; Sunyer, J.; Torrent, M.; Casas, M.; Vrijheid, M. Prenatal exposure to persistent organic pollutants and markers of obesity and cardiometabolic risk in Spanish adolescents. Environ. Int. 2021, 151, 106469. [Google Scholar] [CrossRef]
- Tang-Péronard, J.L.; Heitmann, B.L.; Jensen, T.K.; Vinggaard, A.M.; Madsbad, S.; Steuerwald, U.; Grandjean, P.; Weihe, P.; Nielsen, F.; Andersen, H.R. Prenatal exposure to persistent organochlorine pollutants is associated with high insulin levels in 5-year-old girls. Environ. Res. 2015, 142, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Leijs, M.M.; Koppe, J.G.; Vulsma, T.; Olie, K.; Van Aalderen, W.M.C.; De Voogt, P.; Legler, J.; Gavin, W. Alterations in the programming of energy metabolism in adolescents with background exposure to dioxins, dl-PCBs and PBDEs. PLoS ONE 2017, 12, e0184006. [Google Scholar] [CrossRef] [Green Version]
- Meijer, L.; Weiss, J.; van Velzen, M.; Brouwer, A.; Bergman, Å.; Sauer, P.J.J. Serum Concentrations of Neutral and Phenolic Organohalogens in Pregnant Women and Some of Their Infants in The Netherlands. Environ. Sci. Technol. 2008, 42, 3428–3433. [Google Scholar] [CrossRef] [PubMed]
- Ballschmiter, K.; Mennel, A.; Buyten, J. Long chain alkyl-polysiloxanes as non-polar stationary phases in capillary gas chromatography. Fresenius J. Anal. Chem. 1993, 346, 396–402. [Google Scholar] [CrossRef]
- Letcher, R.J.; Klasson-Wehler, E.; Bergman, A. Methyl Sulfone and Hydroxylated Metabolites of Polychlorinated Biphenyls. In Volume 3 Anthropogenic Compounds Part K; Springer: Berlin, Germany, 2000; pp. 315–359. [Google Scholar]
- Berghuis, S.A.; Van Braeckel, K.N.; Sauer, P.J.; Bos, A.F. Prenatal exposure to persistent organic pollutants and cognition and motor performance in adolescence. Environ. Int. 2018, 121, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Boutot, M.E.; Whitcomb, B.W.; Abdelouahab, N.; Baccarelli, A.A.; Boivin, A.; Caku, A.; Gillet, V.; Martinez, G.; Pasquier, J.-C.; Zhu, J.; et al. In Utero Exposure to Persistent Organic Pollutants and Childhood Lipid Levels. Metabolites 2021, 11, 657. [Google Scholar] [CrossRef]
- Aminian, O.; Moinfar, Z.; Eftekhari, S.; Esser, A.; Schettgen, T.; Felten, M.; Kaifie, A.; Kraus, T. Association of plasma levels of lipid and polychlorinated biphenyls in Iranian adult. Heliyon 2020, 6, e03775. [Google Scholar] [CrossRef]
- Lim, J.-E.; Jee, S.H. Association between serum levels of adiponectin and polychlorinated biphenyls in Korean men and women. Endocrine 2015, 48, 211–217. [Google Scholar] [CrossRef]
- Sandesara, P.B.; Virani, S.S.; Fazio, S.; Shapiro, M.D. The Forgotten Lipids: Triglycerides, Remnant Cholesterol, and Atherosclerotic Cardiovascular Disease Risk. Endocr. Rev. 2019, 40, 537–557. [Google Scholar] [CrossRef] [Green Version]
- Karlsen, M.; Grandjean, P.; Weihe, P.; Steuerwald, U.; Oulhote, Y.; Valvi, D. Early-life exposures to persistent organic pollutants in relation to overweight in preschool children. Reprod. Toxicol. 2017, 68, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Høyer, B.; Ramlau-Hansen, C.H.; Henriksen, T.B.; Pedersen, H.S.; Goralczyk, K.; Zviezdai, V.; Jönsson, B.; Heederik, D.; Lenters, V.; Vermeulen, R.; et al. Body mass index in young school-age children in relation to organochlorine compounds in early life: A prospective study. Int. J. Obes. 2014, 38, 919–925. [Google Scholar] [CrossRef]
- Cupul-Uicab, L.A.; Klebanoff, M.A.; Brock, J.W.; Longnecker, M.P. Prenatal Exposure to Persistent Organochlorines and Childhood Obesity in the U.S. Collaborative Perinatal Project. Environ. Health Perspect. 2013, 121, 1103–1109. [Google Scholar] [CrossRef]
- Vafeiadi, M.; Georgiou, V.; Chalkiadaki, G.; Rantakokko, P.; Kiviranta, H.; Karachaliou, M.; Fthenou, E.; Venihaki, M.; Sarri, K.; Vassilaki, M.; et al. Association of Prenatal Exposure to Persistent Organic Pollutants with Obesity and Cardiometabolic Traits in Early Childhood: The Rhea Mother–Child Cohort (Crete, Greece). Environ. Health Perspect. 2015, 123, 1015–1021. [Google Scholar] [CrossRef]
- Warner, M.; Wesselink, A.; Harley, K.G.; Bradman, A.; Kogut, K.; Eskenazi, B. Prenatal exposure to dichlorodiphenyltrichloroethane and obesity at 9 years of age in the CHAMACOS study cohort. Am. J. Epidemiol. 2014, 179, 1312–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valvi, D.; Mendez, M.A.; Martinez, D.; Grimalt, J.; Torrent, M.; Sunyer, J.; Vrijheid, M. Prenatal Concentrations of Polychlorinated Biphenyls, DDE, and DDT and Overweight in Children: A Prospective Birth Cohort Study. Environ. Health Perspect. 2012, 120, 451–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delvaux, I.; Van Cauwenberghe, J.; Hond, E.D.; Schoeters, G.; Govarts, E.; Nelen, V.; Baeyens, W.; Van Larebeke, N.; Sioen, I. Prenatal exposure to environmental contaminants and body composition at age 7–9 years. Environ. Res. 2014, 132, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Cano-Sancho, G.; Salmon, A.G.; La Merrill, M.A. Association between Exposure to p, p′-DDT and its Metabolite p, p′-DDE with Obesity: Integrated Systematic Review and Meta-Analysis. Environ. Health Perspect. 2017, 125, 096002. [Google Scholar] [CrossRef] [Green Version]
- Reaves, D.K.; Ginsburg, E.; Bang, J.J.; Fleming, J.M. Persistent Organic Pollutants and Obesity: Are they Potential Mechanisms for Breast Cancer Promotion? Endocr. Relat. Cancer 2015, 22, R69–R86. [Google Scholar] [CrossRef] [Green Version]
- Aaseth, J.; Javorac, D.; Djordjevic, A.B.; Bulat, Z.; Skalny, A.V.; Zaitseva, I.P.; Aschner, M.; Tinkov, A.A. The Role of Persistent Organic Pollutants in Obesity: A Review of Laboratory and Epidemiological Studies. Toxics 2022, 10, 65. [Google Scholar] [CrossRef]
- Arsenescu, V.; Arsenescu, R.I.; King, V.; Swanson, H.; Cassis, L.A. Polychlorinated Biphenyl-77 Induces Adipocyte Differentiation and Proinflammatory Adipokines and Promotes Obesity and Atherosclerosis. Environ. Health Perspect. 2008, 116, 761–768. [Google Scholar] [CrossRef] [Green Version]
- Pereira-Fernandes, A.; Dirinck, E.; Dirtu, A.C.; Malarvannan, G.; Covaci, A.; Van Gaal, L.; Vanparys, C.; Jorens, P.G.; Blust, R. Expression of Obesity Markers and Persistent Organic Pollutants Levels in Adipose Tissue of Obese Patients: Reinforcing the Obesogen Hypothesis? PLoS ONE 2014, 9, e84816. [Google Scholar] [CrossRef] [Green Version]
- Stel, J.; Legler, J. The Role of Epigenetics in the Latent Effects of Early Life Exposure to Obesogenic Endocrine Disrupting Chemicals. Endocrinology 2015, 156, 3466–3472. [Google Scholar] [CrossRef] [Green Version]
- Albuquerque, D.; Stice, E.; Rodríguez-López, R.; Manco, L.; Nóbrega, C. Current review of genetics of human obesity: From molecular mechanisms to an evolutionary perspective. Mol. Genet. Genom. 2015, 290, 1191–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, L.-J.; Zhu, H.; He, H.; Wu, K.-H.; Li, J.; Chen, X.-D.; Zhang, J.-G.; Shen, H.; Tian, Q.; Krousel-Wood, M.; et al. Replication of 6 Obesity Genes in a Meta-Analysis of Genome-Wide Association Studies from Diverse Ancestries. PLoS ONE 2014, 9, e96149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Characteristic | Value | |
|---|---|---|
| Sex (boy/girl) | 55/46 (54.5/45.5%) | |
| Age at examination (years) | 14.4 ± 0.8 | |
| Gestational age (weeks) | 40 (37–42) | |
| Maternal age at delivery (years) | 32.0 ± 3.8 | |
| Maternal pre-pregnancy body mass index (BMI; kg/m2) a (n = 98) | 24.5 ± 4.0 | |
| Maternal education [<14/≥14 years’ school education] | 50/51 (50/51%) | |
| Maternal smoking during pregnancy [yes/no] | 13/88 (13/87%) | |
| Maternal alcohol consumption during pregnancy [yes/no] | 21/80 (21/79%) | |
| Maternal parity history [nulliparous/multiparous] | 36/65 (36/64%) | |
| Boys (n = 55) | Girls (n = 46) | |
| Height (cm) | 172.5 ± 9.1 | 166.8 ± 6.2 |
| Weight (kg) | 58.4 ± 15.4 | 57.7 ± 9.9 |
| Body mass index (BMI; kg/m2) a | 19.5 ± 3.8 | 20.7 ± 3.2 |
| BMI z-score b | 0.03 ± 1.20 | 0.24 ± 1.07 |
| BMI-SDS > 1.1 (overweight) | 4 (7%) | 11 (24%) |
| BMI-SDS > 2.3 (obese) | 4 (7%) | 0 (0%) |
| Waist circumference (cm) | 70.8 ± 9.0 | 69.1 ± 7.2 |
| Hip circumference (cm) | 80.0 ± 9.0 | 83.0 ± 7.9 |
| Waist/height ratio c | 0.4 ± 0.0 | 0.4 ± 0.0 |
| Systolic blood pressure (mmHg) d | 119.1 ± 9.1 | 113.7 ± 8.0 |
| Diastolic blood pressure (mmHg) d | 59.0 ± 6.7 | 59.4 ± 7.0 |
| Variable | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|
| n | Median | Min | Max | n | Median | Min | Max | |
| Insulin (µU/mL serum) | 54 | 8.15 | 3.50 | 40.30 | 43 | 9.00 | 3.90 | 22.50 |
| Fasting glucose (mmol/L plasma) | 52 | 5.20 | 4.60 | 6.00 | 41 | 5.20 | 4.00 | 5.90 |
| Cholesterol (mmol/L serum) | 54 | 3.65 | 2.34 | 5.92 | 43 | 3.92 | 2.90 | 5.73 |
| HDL-C (mmol/L serum) | 54 | 1.43 | 0.87 | 2.39 | 43 | 1.41 | 0.91 | 2.23 |
| LDL-C (mmol/L serum) | 54 | 1.95 | 0.93 | 4.10 | 43 | 2.22 | 1.30 | 3.76 |
| Triglycerides (mmol/L serum) | 54 | 0.72 | 0.35 | 1.94 | 43 | 0.79 | 0.36 | 1.82 |
| Leptin (ng/mL plasma) | 48 | 1.93 | 0.16 | 49.06 | 40 | 11.48 | 2.52 | 62.58 |
| Adiponectin (in ng/mL plasma) c | 48 | 16.80 | 3.32 | 32.24 | 39 | 12.41 | 3.35 | 26.50 |
| LDL-C/HDL-C ratio (mean ± SD) | 54 | 1.53 ± 0.63 | 43 | 1.70 ± 0.69 | ||||
| HOMA2-IR d (mean ± SD) | 52 | 1.16 ± 0.54 | 41 | 1.27 ± 0.51 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berghuis, S.A.; Bos, A.F.; Sauer, P.J.J.; Bocca, G. Prenatal Environmental Exposure to Persistent Organic Pollutants and Indices of Overweight and Cardiovascular Risk in Dutch Adolescents. Nutrients 2022, 14, 2269. https://doi.org/10.3390/nu14112269
Berghuis SA, Bos AF, Sauer PJJ, Bocca G. Prenatal Environmental Exposure to Persistent Organic Pollutants and Indices of Overweight and Cardiovascular Risk in Dutch Adolescents. Nutrients. 2022; 14(11):2269. https://doi.org/10.3390/nu14112269
Chicago/Turabian StyleBerghuis, Sietske A., Arend F. Bos, Pieter J. J. Sauer, and Gianni Bocca. 2022. "Prenatal Environmental Exposure to Persistent Organic Pollutants and Indices of Overweight and Cardiovascular Risk in Dutch Adolescents" Nutrients 14, no. 11: 2269. https://doi.org/10.3390/nu14112269
APA StyleBerghuis, S. A., Bos, A. F., Sauer, P. J. J., & Bocca, G. (2022). Prenatal Environmental Exposure to Persistent Organic Pollutants and Indices of Overweight and Cardiovascular Risk in Dutch Adolescents. Nutrients, 14(11), 2269. https://doi.org/10.3390/nu14112269