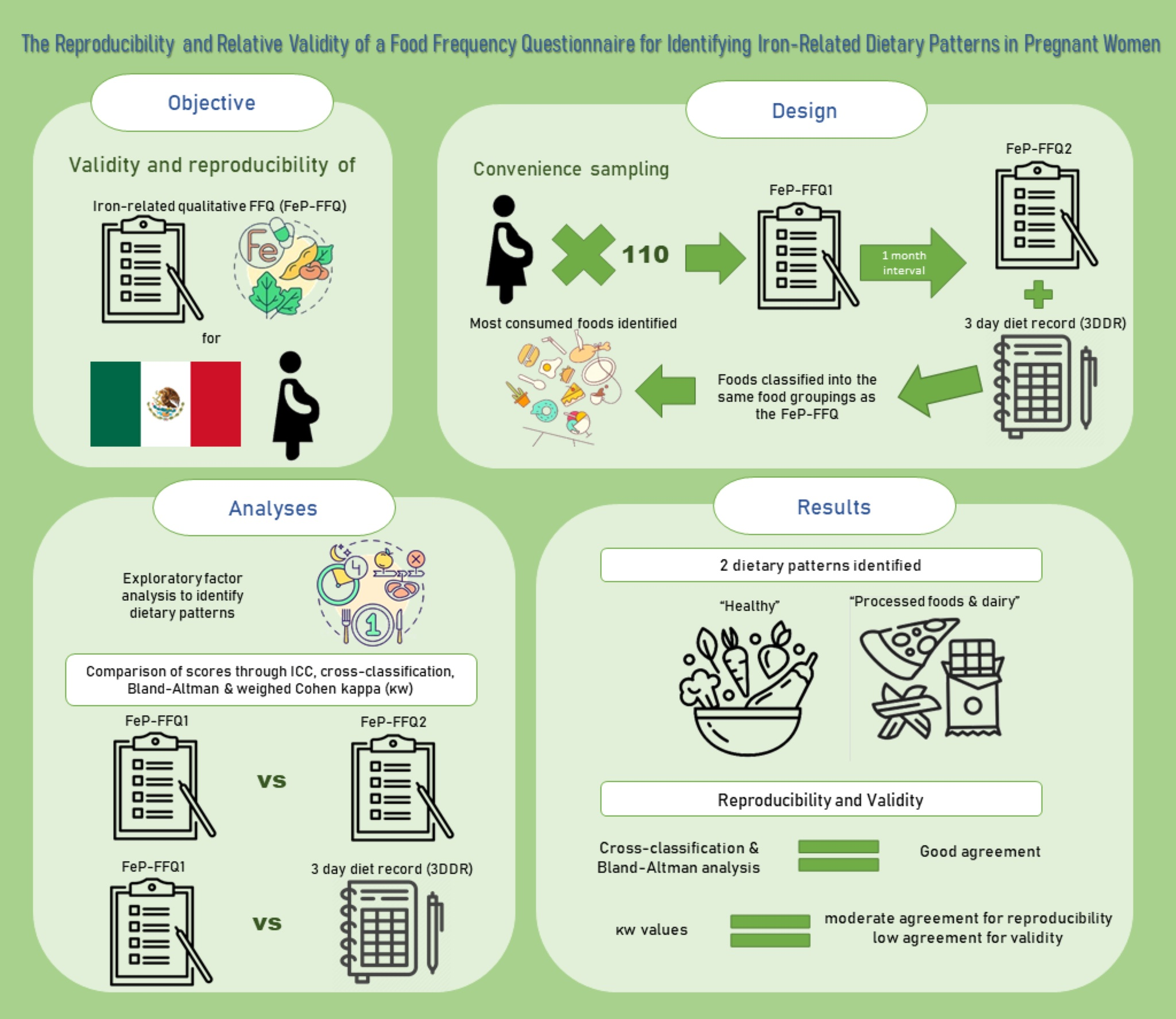
The Reproducibility and Relative Validity of a Food Frequency Questionnaire for Identifying Iron-Related Dietary Patterns in Pregnant Women

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Design
2.3. FeP-FFQ Development and Application
2.4. Measurements
2.4.1. Sociodemographic, Anthropometric Data and Iron Status
2.4.2. Diet Records
2.5. Statistical Analysis
2.5.1. Identification of the Most Frequently Consumed Food Items
2.5.2. Identification of Dietary Patterns from the FeP-FFQs and the Diet Records
3. Results
3.1. Participant Characteristics
3.2. Food Intake Frequency
3.3. Identification of Dietary Patterns
3.4. Reproducibility and Validity of Dietary Patterns
4. Discussion
4.1. Reproducibility and Validity of FeP-FFQ
4.2. Reproducibility and Validity of Dietary Patterns
4.3. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Anaemia in Women and Children. Available online: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children (accessed on 15 May 2022).
- Shamah-Levy, T.; Vielma-Orozco, E.; Heredia-Hernández, O.; Romero-Martínez, M.; Mojica-Cuevas, J.; Cuevas-Nasu, L.; Santaella-Castell, J.A.; Rivera-Dommarco, J. Encuesta Nacional de Salud y Nutrición 2018-19: Resultados Nacionales; Instituto Nacional de Salud Pública: Cuernavaca, México, 2020. [Google Scholar]
- Breymann, C. Iron deficiency anemia in pregnancy. In Seminars in Hematology; Elsevier: Amsterdam, The Netherlands, 2015; Volume 52, pp. 339–347. [Google Scholar] [CrossRef]
- Ramakrishnan, U. Functional Consequences of Nutritional Anemia during Pregnancy and Early Childhood; CRC Press, LLC: Boca Raton, FL, USA, 2001; pp. 43–68. [Google Scholar]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/handle/10665/85839. (accessed on 22 May 2018).
- Resnik, R.; Lockwood, C.J.; Moore, T.; Greene, M.F.; Copel, J.; Silver, R.M. Creasy and Resnik’s Maternal-Fetal Medicine: Principles and Practice E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- World Health Organization. Global Health Observatory Data Repository/World Health Statistics. Available online: https://apps.who.int/gho/data/node.main.ANEMIAPREGNANTWOMAN?lang=en (accessed on 30 May 2018).
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Demuth, I.R.; Martin, A.; Weissenborn, A. Iron supplementation during pregnancy-A cross-sectional study undertaken in four German states. BMC Pregnancy Childbirth 2018, 18, 491. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Nutritional Anaemias: Tools for Effective Prevention and Control. Available online: https://apps.who.int/iris/rest/bitstreams/1091289/retrieve (accessed on 4 June 2018).
- Cao, C.; O’Brien, K.O. Pregnancy and iron homeostasis: An update. Nutr. Rev. 2013, 71, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ballart, J.D. Iron metabolism during pregnancy. Clin. Drug Investig. 2000, 19, 9–19. [Google Scholar] [CrossRef]
- Msemo, O.A.; Bygbjerg, I.C.; Møller, S.L.; Nielsen, B.B.; Ødum, L.; Perslev, K.; Lusingu, J.P.A.; Kavishe, R.A.; Minja, D.T.R.; Schmiegelow, C. Prevalence and risk factors of preconception anemia: A community-based cross-sectional study of rural women of reproductive age in northeastern Tanzania. PLoS ONE 2018, 13, e0208413. [Google Scholar] [CrossRef]
- Kaufer-Horwitz, M.; Pérz-Lizaur, A.B.; Arroyo, P. Nutriología Médica; Panamericana: Singapore, 2015. [Google Scholar]
- Głąbska, D.; Guzek, D.; Ślązak, J.; Włodarek, D. Assessing the validity and reproducibility of an iron dietary intake questionnaire conducted in a group of young Polish women. Nutrients 2017, 9, 199. [Google Scholar] [CrossRef] [Green Version]
- Beck, K.L. Iron Deficiency in Young Women: Causes, Consequences and Solutions: A Thesis Presented in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy in Nutritional Science at Massey University. Ph.D. Thesis, Massey University, Albany, New Zealand, 2013. [Google Scholar]
- Fayet, F.; Flood, V.; Petocz, P.; Samman, S. Relative and biomarker-based validity of a food frequency questionnaire that measures the intakes of vitamin B12, folate, iron, and zinc in young women. Nutr. Res. 2011, 31, 14–20. [Google Scholar] [CrossRef]
- Beck, K.L.; Kruger, R.; Conlon, C.A.; Heath, A.-L.M.; Coad, J.; Matthys, C.; Jones, B.; Stonehouse, W. The relative validity and reproducibility of an iron food frequency questionnaire for identifying iron-related dietary patterns in young women. J. Acad. Nutr. Diet. 2012, 112, 1177–1187. [Google Scholar] [CrossRef]
- Willett, W.; Lenart, E. Nutritional Epidemiology, 3rd ed.; New York Oxford University Press: New York, NY, USA, 2013; pp. 96–141. [Google Scholar] [CrossRef]
- Zhou, G.; Gan, Y.; Miao, M.; Hamilton, K.; Knoll, N.; Schwarzer, R. The role of action control and action planning on fruit and vegetable consumption. Appetite 2015, 91, 64–68. [Google Scholar] [CrossRef]
- Pérez-Lizaur, A.B.; Palacios-González, B.; Castro-Becerra, A.L.; Flores-Galicia, I. SMAE: Sistema Mexicano de Alimentos Equivalentes, 4th ed.; Porrúa: Ciudad de México, Mexico, 2014; ISBN 9786070079283. [Google Scholar]
- Cohen, J.A. Power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Atalah, E.; Castillo, C.; Castro, R.A.A. Propuesta de un nuevo estándar de evaluación nutricional en embarazadas. Rev. Med. Chile 1997, 15, 1429–1436. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Asociación Mexicana de Agencias de Inteligencia de Mercado y Opinión Pública. Índice de Niveles Socioeconómicos. Available online: https://www.amai.org/NSE/index.php (accessed on 10 January 2018).
- Heath, A.L.; Skeaff, C.M.; Gibson, R.S. The relative validity of a computerized food frequency questionnaire for estimating intake of dietary iron and its absorption modifiers. Eur. J. Clin. Nutr. 2000, 54, 592–599. [Google Scholar] [CrossRef] [Green Version]
- Trinidad-Rodríguez, I.; Fernández-Ballart, J.; Cucó-Pastor, G.; Biarnés-Jordà, E.; Arija-Val, V. Validación de un cuestionario de frecuencia de consumo alimentario corto: Reproducibilidad y validez. Nutr. Hosp. 2008, 23, 242–252. [Google Scholar]
- Baer, H.J.; Blum, R.E.; Rockett, H.R.H.; Leppert, J.; Gardner, J.D.; Suitor, C.W.; A Colditz, G. Use of a food frequency questionnaire in American Indian and Caucasian pregnant women: A validation study. BMC Public Health 2005, 5, 135. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.E.; Buzzard, I.M.; Jacobs, D.R., Jr.; Hannan, P.J.; Kushi, L.H.; Barosso, G.M.; Schmid, L.A. A food frequency questionnaire can detect pregnancy-related changes in diet. J. Am. Diet. Assoc. 1996, 96, 262–266. [Google Scholar] [CrossRef]
- Robinson, S.; Godfrey, K.; Osmond, C.; Cox, V.; Barker, D. Evaluation of a food frequency questionnaire used to assess nutrient intakes in pregnant women. Eur. J. Clin. Nutr. 1996, 50, 302–308. [Google Scholar] [PubMed]
- Galante, A.P.; Colli, C. Development and use of an on-line semiquantitative food-frequency questionnaire to evaluate calcium and iron intake. Rev. Bras. Epidemiol. 2008, 11, 402–410. [Google Scholar] [CrossRef]
- Brunst, K.; Kannan, S.; Ni, Y.-M.; Gennings, C.; Ganguri, H.; Wright, R. Validation of a Food Frequency Questionnaire for Estimating Micronutrient Intakes in an Urban US Sample of Multi-Ethnic Pregnant Women. Matern. Child Health J. 2015, 20, 250–260. [Google Scholar] [CrossRef] [Green Version]
- Forsythe, H.E.; Gage, B. Use of a multicultural food-frequency questionnaire with pregnant and lactating women. Am. J. Clin. Nutr. 1994, 59, 203S–206S. [Google Scholar] [CrossRef]
- Zhou, S.J.; Schilling, M.J.; Makrides, M. Evaluation of an iron specific checklist for the assessment of dietary iron intake in pregnant and postpartum women. Nutrition 2005, 21, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires–a review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [Green Version]
- Thompson, F.; Byers, T. Manual de Instrumentos de Evaluación Dietética; INCAP/MDE156: Guatemala, 2006; ISBN 9993968072. [Google Scholar]
- Serra-Majem, L.; Andersen, L.F.; Henríque-Sánchez, P.; Doreste-Alonso, J.; Sánchez-Villegas, A.; Ortiz-Andrelluchi, A.; Negri, E.; La Vecchia, C. Evaluating the quality of dietary intake validation studies. Br. J. Nutr. 2009, 102 (Suppl. S1), S3–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baranowski, T. 24-hour recall and diet record methods. In Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013; Volume 40, pp. 49–69. [Google Scholar] [CrossRef]
- Erkkola, M.; Karppinen, M.; Javanainen, J.; Räsänen, L.; Knip, M.; Virtanen, S.M. Validity and reproducibility of a food frequency questionnaire for pregnant Finnish women. Am. J. Epidemiol. 2001, 154, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Matthys, C.; Pynaert, I.; Roe, M.; Fairweather-Tait, S.J.; Heath, A.-L.; De Henauw, S. Validity and reproducibility of a computerised tool for assessing the iron, calcium and vitamin C intake of Belgian women. Eur. J. Clin. Nutr. 2004, 58, 1297–1305. [Google Scholar] [CrossRef] [Green Version]
- Pynaert, I.; Matthys, C.; De Bacquer, D.; De Backer, G.; De Henauw, S. Evaluation of a 2-day food record to determine iron, calcium and vitamin C intake in young Belgian women. Eur. J. Clin. Nutr. 2008, 62, 104–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shateinstein, B.; Xu, H.; Luo, Z.C.; Fraser, W. Relative validity of a Food frequency questionnaire for pregnant women. Can. J. Diet. Pract. Res. 2011, 72, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Togo, P.; Heitmann, B.L.; Sørensen, T.I.A.; Osler, M. Consistency of food intake factors by different dietary assessment methods and population groups. Br. J. Nutr. 2003, 90, 667–678. [Google Scholar] [CrossRef] [Green Version]
- Khani, B.R.; Ye, W.; Terry, P.; Wolk, A. Reproducibility and validity of major dietary patterns among Swedish women assessed with a food-frequency questionnaire. J. Nutr. 2004, 134, 1541–1545. [Google Scholar] [CrossRef]
- Crozier, S.R.; Inskip, H.M.; Godfrey, K.M.; Robinson, S.M. Dietary patterns in pregnant women: A comparison of food-frequency questionnaires and 4 d prospective diaries. Br. J. Nutr. 2008, 99, 869–875. [Google Scholar] [CrossRef] [Green Version]
- Ambrosini, G.L.; O’Sullivan, T.A.; De Klerk, N.H.; Mori, T.A.; Beilin, L.J.; Oddy, W.H. Relative validity of adolescent dietary patterns: A comparison of a FFQ and 3 d food record. Br. J. Nutr. 2011, 105, 625–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanri, A.; Shimazu, T.; Ishihara, J.; Takachi, R.; Mizoue, T.; Inoue, M.; Tsugane, S. Reproducibility and validity of dietary patterns assessed by a food frequency questionnaire used in the 5-year follow-up survey of the Japan Public Health Center-Based Prospective Study. J. Epidemiol. 2012, 22, 205–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Hu, X.; Yuan, B.; Pan, X.; Dai, Y.; Holmboe-Ottesen, G. Association between dietary patterns and anaemia in adults from Jiangsu Province in Eastern China. Br. J. Nutr. 2006, 96, 906–912. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, J.A.; Castro, T.G.; Grant, C.C.; Wall, C.R.; da Silva Castro, A.L.; Francisco, R.P.V.; Vieira, S.E.; Saldiva, S.R.D.M.; Marchioni, D.M. Dietary patterns are influenced by sociodemographic conditions of women in childbearing age: A cohort study of pregnant women. BMC Public Health 2018, 18, 301. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Masson, L.F.; Mcneill, G.; Tomany, J.O.; Simpson, J.; Peace, H.; Wei, L.; Grubb, D.; Bolton-Smith, C. Statistical approaches for assessing the relative validity of a food-frequency questionnaire: Use of correlation coefficients and the kappa statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Weighted kappa: Nominal scale agreement provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70, 213. [Google Scholar] [CrossRef]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Okubo, H.; Murakami, K.; Sasaki, S.; Kim, M.K.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Relative validity of dietary patterns derived from a self-administered diet history questionnaire using factor analysis among Japanese adults. Public Health Nutr. 2010, 13, 1080–1089. [Google Scholar] [CrossRef]
- Hodgson, J.M.; Hsu-Hage, B.H.; Wahlqvist, M.L. Food variety as a quantitative descriptor of food intake. Ecol. Food Nutr. 1994, 32, 137–148. [Google Scholar] [CrossRef]
- Milman, N.T. A review of nutrients and compounds, which promote or inhibit intestinal iron absorption: Making a platform for dietary measures that can reduce iron uptake in patients with genetic haemochromatosis. J. Nutr. Metab. 2020, 2020, 7373498. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Characteristics | n (%) | |
|---|---|---|
| Civil status | Married | 33 (30) |
| Free union | 60 (54.5) | |
| Single | 16 (14.5) | |
| Divorced | 1 (1) | |
| Education level | None | 0 (0) |
| Knows how to write and read | 1 (0.9) | |
| Elementary school | 12 (10.9) | |
| Secondary school | 51 (46.4) | |
| High school | 36 (37.2) | |
| Bachelor degree | 9 (8.2) | |
| Graduate degree | 1 (0.9) | |
| Occupation | Housewife | 89 (80.9) |
| Paid job | 19 (17.3) | |
| Student | 2 (1.8) | |
| Socioeconomic status * | AB (high class) | 3 (2.7) |
| C+ (middle-high class) | 5 (4.5) | |
| C (middle class) | 19 (17.3) | |
| C− (middle-low class) | 22 (20) | |
| D+ (low-middle class) | 35 (31.8) | |
| D (low class) | 26 (23.6) | |
| E (extreme poverty) | 0 (0) | |
| Anthropometric characteristics | ||
| Height (m) | Mean (SD) | 1.6 (0.1) |
| Pregestational weight (kg) ** | Mean (SD) | 66.1 (15.2) |
| Pregestational BMI *** | Mean (SD) | 26.0 (5.7) |
| Pregestational BMI status | Low | 11 (10) |
| Normal | 48 (43.6) | |
| Overweight | 25 (22.7) | |
| Obese | 26 (23.6) | |
| Current weight (kg) | Mean (SD) | 73.2 (15.2) |
| Current BMI | Mean (SD) | 28.8 (5.6) |
| Current BMI status **** | Low | 10 (9.1) |
| Normal | 35 (31.8) | |
| Overweight | 39 (35.5) | |
| Obese | 26 (23.6) | |
| Iron status | ||
| Hemoglobin (g/dL) ***** | Mean (SD) | 12.15 (1.04) |
| Hemoglobin status ***** | Anemia (≤11.0) | 16 (14.5) |
| Normal (≥11.1) | 94 (85.5) | |
| Frequency of Intake over 3 Days Mean ± SD | Difference Mean ± SD | Correlation Coefficients ® † | |||||
|---|---|---|---|---|---|---|---|
| Items | FeP-FFQ1 | FeP-FFQ2 | 3DDR | FeP-FFQ1 vs. 3DDR | FeP-FFQ1 vs. FeP-FFQ2 | FeP-FFQ1 vs. 3DDR | FeP-FFQ1 vs. FeP-FFQ2 |
| Water | 15.54 ± 6.07 | 15.62 ± 5.69 | 20.30 ± 8.56 | −4.84 ± 8.20 **b | −0.17 ± 5.73 | 0.41 ** | 0.52 ** |
| Corn tortilla | 6.07 ± 3.56 | 5.78 ± 3.49 | 4.30 ± 1.78 | 1.77 ± 3.41 **a | 0.28 ± 3.19 | 0.33 ** | 0.59 ** |
| Tomato | 4.91 ± 4.96 | 3.94 ± 4.11 | 2.78 ± 1.52 | 2.12 ± 5.17 **a | 0.96 ± 4.56 * | 0.01 | 0.50 ** |
| Citrus fruits c | 4.20 ± 4.57 | 2.72 ± 3.38 | 1.92 ± 1.54 | 2.28 ± 4.80 **a | 1.48 ± 3.94 **a | 0.01 | 0.54 ** |
| Lime d | 4.06 ± 5.12 | 3.05 ± 3.72 | 1.36 ± 1.37 | 2.69 ± 4.91 **a | 1.00 ± 3.42 * | 0.28 * | 0.74 ** |
| Onion | 3.40 ± 3.72 | 3.16 ± 3.16 | 2.51 ± 1.65 | 0.89 ± 3.92 * | 0.24 ± 3.84 | 0.09 | 0.38 ** |
| Milk | 3.32 ± 3.55 | 3.09 ± 2.63 | 2.73 ± 1.76 | 0.59 ± 3.38 | 0.23 ± 3.20 | 0.34 ** | 0.49 ** |
| Stone fruits e | 3.08 ± 3.91 | 2.13 ± 3.27 | 0.76 ± 0.99 | 2.31 ± 3.80 **b | 0.94 ± 3.43 * | 0.23 * | 0.55 ** |
| Homemade beans | 2.64 ± 2.75 | 2.25 ± 2.17 | 1.45 ± 1.25 | 1.19 ± 2.83 **a | 0.39 ± 2.08 * | 0.15 | 0.68 ** |
| Chilies f | 2.64 ± 3.32 | 2.10 ± 2.47 | 2.17 ± 1.84 | 0.46 ± 3.18 | 0.53 ± 2.92 | 0.35 ** | 0.52 ** |
| Banana and fried plantain | 2.46 ± 3.57 | 1.94 ± 2.70 | 1.19 ± 1.09 | 1.27 ± 3.74 **a | 0.52 ± 3.71 | −0.00 | 0.32 ** |
| Apple | 2.21 ± 3.62 | 1.62 ± 3.11 | 0.65 ± 0.86 | 1.56 ± 3.59 **a | 0.59 ± 2.49 * | 0.15 | 0.73 ** |
| Lettuce | 1.86 ± 2.35 | 1.36 ± 2.02 | 0.76 ± 0.98 | 1.09 ± 2.51 **a | 0.49 ± 2.56 * | 0.04 | 0.31 ** |
| Carrot | 1.69 ± 2.53 | 1.21 ± 1.37 | 0.74 ± 0.99 | 0.95 ± 2.57 **a | 0.48 ± 2.91 | 0.15 | 0.23 ** |
| Soda | 1.62 ± 2.55 | 1.89 ± 2.75 | 1.35 ± 1.49 | 0.27 ± 2.15 | −0.27 ± 2.09 | 0.54 ** | 0.69 ** |
| Eggs | 1.58 ± 2.12 | 1.36 ± 2.02 | 1.51 ± 1.06 | 0.07 ± 2.03 | 0.22 ± 2.19 | 0.33 ** | 0.17 ** |
| Melon | 1.53 ± 3.80 | 0.93 ± 2.28 | 0.34 ± 0.56 | 1.19 ± 3.78 **a | 0.60 ± 2.84 * | 0.12 | 0.66 ** |
| Watermelon | 1.41 ± 3.54 | 0.45 ± 0.90 | 0.22 ± 0.47 | 1.18 ± 3.52 **a | 0.96 ± 3.35 * | 0.11 | 0.33 ** |
| Sour cream | 1.39 ± 1.58 | 1.29 ± 1.49 | 0.86 ± 0.96 | 0.52 ± 1.67 **a | 0.10 ± 1.14 | 0.21 * | 0.72 ** |
| Rice | 1.35 ± 1.51 | 0.94 ± 0.56 | 0.69 ± 0.87 | 0.65 ± 1.66 **a | 0.41 ± 1.47 * | 0.10 | 0.25 * |
| Yogurt g | 1.26 ± 1.28 | 1.12 ± 1.37 | 0.43 ± 0.67 | 0.82 ± 1.23 **b | 0.14 ± 1.04 | 0.34 ** | 0.69 |
| Pasta soup | 1.19 ± 1.63 | 1.11 ± 1.28 | 0.55 ± 0.73 | 0.63 ± 1.68 **a | 0.07 ± 1.68 | 0.15 | 0.34 ** |
| Potato | 1.15 ± 1.55 | 1.00 ± 0.96 | 0.87 ± 0.91 | 0.28 ± 1.78 ** | 0.15 ± 1.07 | 0.02 | 0.73 ** |
| Mexican sweet bread | 1.13 ± 1.83 | 0.83 ± 0.83 | 0.75 ± 0.93 | 0.37 ± 1.98 * | 0.29 ± 1.65 | 0.09 | 0.43 ** |
| Cookies | 1.12 ± 1.99 | 0.95 ± 1.34 | 0.56 ± 1.98 | 0.55 ± 2.82 * | 0.16 ± 1.94 | 0.00 | 0.37 ** |
| Poultry | 1.09 ± 1.62 | 0.88 ± 0.82 | 0.81 ± 0.77 | 0.28 ± 1.77 | 0.21 ± 1.70 | 0.04 | 0.16 ** |
| Cheese | 1.07 ± 1.54 | 0.96 ± 1.55 | 0.66 ± 0.86 | 0.40 ± 1.79 * | 0.10 ± 0.74 | −0.03 | 0.88 ** |
| Papaya | 1.00 ± 2.02 | 0.82 ± 1.94 | 0.31 ± 0.63 | 0.69 ± 2.04 **a | 0.17 ± 1.94 | 0.13 | 0.51 ** |
| Ice-cream, sorbet, popsicles | 0.93 ± 1.81 | 0.67 ± 1.21 | 0.09 ± 0.31 | 0.83 ± 1.80 **a | 0.26 ± 1.53 | 0.15 | 0.54 ** |
| Grains | 0.91 ± 1.87 | 0.70 ± 1.15 | 0.45 ± 0.69 | 0.46 ± 1.79 * | 0.20 ± 1.65 | 0.30 ** | 0.48 ** |
| Beef | 0.90 ± 0.61 | 0.82 ± 0.57 | 1.70 ± 1.28 | −0.79 ± 1.32 **b | 0.08 ± 0.60 | 0.17 | 0.47 ** |
| Sausages and ham | 0.90 ± 1.32 | 0.97 ± 1.33 | 0.95 ± 0.95 | −0.58 ± 1.52 | −0.07 ± 1.17 | 0.14 | 0.61 ** |
| Dietary Pattern | ||||||
|---|---|---|---|---|---|---|
| Healthy | Industrialized Food and Dairy | |||||
| Items | FeP-FFQ1 | FeP-FFQ2 | 3DDR | FeP-FFQ1 | FeP-FFQ2 | 3DDR |
| Melon | 0.84 | 0.77 | 0.48 | |||
| Watermelon | 0.78 | 0.19 | 0.29 | 0.39 | −0.24 | |
| Banana and fried plantain | 0.76 | 0.34 | 0.35 | −0.42 | ||
| Citrus fruits | 0.75 | 0.67 | 0.50 | 0.39 | ||
| Stone fruits | 0.75 | 0.72 | 0.37 | 0.23 | ||
| Grains | 0.63 | 0.44 | 0.25 | −0.46 | ||
| Apple | 0.62 | 0.83 | 0.69 | |||
| Potato | 0.60 | 0.23 | 0.56 | |||
| Lime | 0.59 | 0.66 | 0.56 | 0.21 | ||
| Tomato | 0.51 | 0.66 | 0.39 | 0.52 | ||
| Eggs | 0.49 | 0.20 | ||||
| Onion | 0.48 | 0.53 | 0.70 | |||
| Papaya | 0.47 | 0.30 | 0.30 | −0.26 | 0.31 | |
| Homemade beans | 0.42 | 0.38 | ||||
| Lettuce | 0.39 | 0.73 | 0.22 | |||
| Carrot | 0.38 | 0.71 | 0.32 | |||
| Rice | 0.36 | 0.33 | 0.35 | 0.45 | 0.27 | |
| Corn tortilla | 0.34 | 0.24 | 0.42 | 0.33 | ||
| Milk | 0.28 | 0.25 | 0.48 | −0.42 | ||
| Chilies (fresh, minced, dried, whole) | 0.27 | 0.32 | 0.44 | 0.44 | ||
| Ice cream, sorbet, popsicles | 0.22 | 0.34 | 0.44 | 0.29 | ||
| Beef | 0.20 | 0.39 | 0.40 | |||
| Soda | −0.26 | 0.38 | 0.54 | 0.40 | ||
| Pasta soup | 0.77 | 0.34 | 0.21 | |||
| Sausages and ham | 0.66 | 0.61 | 0.20 | |||
| Cheese | 0.63 | 0.39 | −0.30 | |||
| Sour cream | 0.25 | 0.44 | 0.52 | |||
| Mexican sweet bread | −0.22 | 0.21 | 0.48 | |||
| Cookies | 0.40 | 0.15 | 0.41 | |||
| Yogurt | 0.33 | 0.42 | 0.40 | |||
| Poultry | 0.60 | 0.31 | ||||
| Water | 0.25 | 0.32 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Padilla, M.L.; Bernal-Orozco, M.F.; Fernández-Ballart, J.; Vizmanos, B.; Rodríguez-Rocha, N.P.; Macedo-Ojeda, G. The Reproducibility and Relative Validity of a Food Frequency Questionnaire for Identifying Iron-Related Dietary Patterns in Pregnant Women. Nutrients 2022, 14, 2313. https://doi.org/10.3390/nu14112313
Navarro-Padilla ML, Bernal-Orozco MF, Fernández-Ballart J, Vizmanos B, Rodríguez-Rocha NP, Macedo-Ojeda G. The Reproducibility and Relative Validity of a Food Frequency Questionnaire for Identifying Iron-Related Dietary Patterns in Pregnant Women. Nutrients. 2022; 14(11):2313. https://doi.org/10.3390/nu14112313
Chicago/Turabian StyleNavarro-Padilla, Mayra Lizeth, María Fernanda Bernal-Orozco, Joan Fernández-Ballart, Barbara Vizmanos, Norma Patricia Rodríguez-Rocha, and Gabriela Macedo-Ojeda. 2022. "The Reproducibility and Relative Validity of a Food Frequency Questionnaire for Identifying Iron-Related Dietary Patterns in Pregnant Women" Nutrients 14, no. 11: 2313. https://doi.org/10.3390/nu14112313
APA StyleNavarro-Padilla, M. L., Bernal-Orozco, M. F., Fernández-Ballart, J., Vizmanos, B., Rodríguez-Rocha, N. P., & Macedo-Ojeda, G. (2022). The Reproducibility and Relative Validity of a Food Frequency Questionnaire for Identifying Iron-Related Dietary Patterns in Pregnant Women. Nutrients, 14(11), 2313. https://doi.org/10.3390/nu14112313