Growth and Gastrointestinal Tolerance in Healthy Term Infants Fed Milk-Based Infant Formula Supplemented with Five Human Milk Oligosaccharides (HMOs): A Randomized Multicenter Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Study Treatments
2.4. Study Outcome Measures and Procedures
2.5. Statistical Analyses
3. Results
3.1. Disposition of Participants
3.2. Demographic and Other Baseline Characteristics
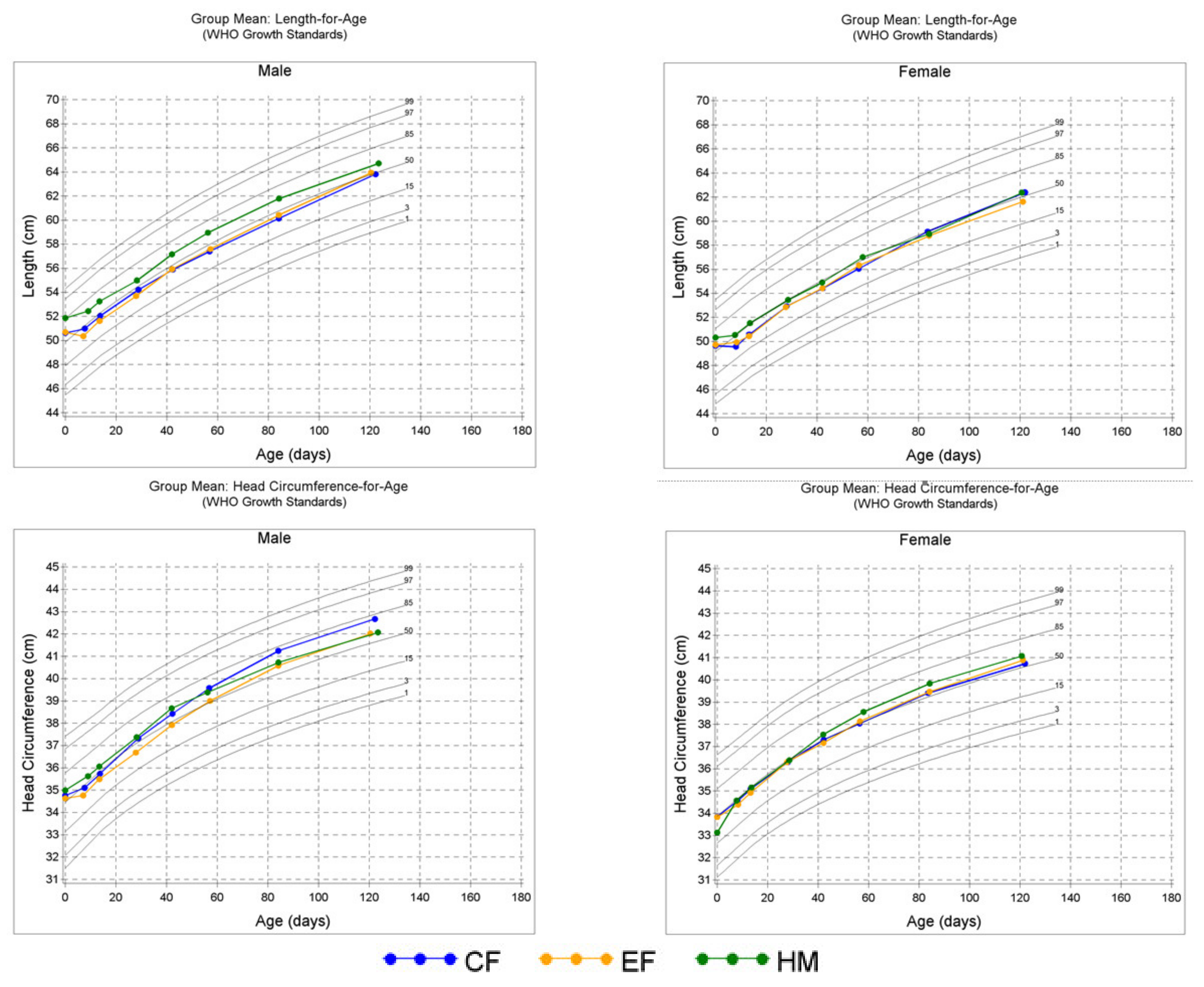
3.3. Growth
3.4. Formula Intake and GI Tolerance
3.5. Parental Responses to Study Questionnaires
3.6. Safety and Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, D.R.; Chow, J.M.; Buck, R.H. Multifunctional benefits of prevalent HMOs: Implications for infant health. Nutrients 2021, 13, 3364. [Google Scholar] [CrossRef] [PubMed]
- Azad, M.B.; Robertson, B.; Atakora, F.; Becker, A.B.; Subbarao, P.; Moraes, T.J.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.L.; Sears, M.R. Human milk oligosaccharide concentrations are associated with multiple fixed and modifiable maternal characteristics, environmental factors, and feeding practices. J. Nutr. 2018, 148, 1733–1742. [Google Scholar] [CrossRef] [PubMed]
- Thum, C.; Wall, C.R.; Weiss, G.A.; Wang, W.; Szeto, I.M.-Y.; Day, L. Changes in HMO concentrations throughout lactation: Influencing factors, health effects and opportunities. Nutrients 2021, 13, 2272. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.-T.; Chen, C.; Newburg, D.S. Utilization of major fucosylated and sialylated human milk oligosaccharides by isolated human gut microbes. Glycobiology 2013, 23, 1281–1292. [Google Scholar] [CrossRef] [Green Version]
- Özcan, E.; Sela, D.A. Inefficient metabolism of the human milk oligosaccharides lacto-N-tetraose and lacto-N-neotetraose shifts bifidobacterium longum subsp. infantis physiology. Front. Nutr. 2018, 5, 46. [Google Scholar] [CrossRef]
- Kaiko, G.E.; Ryu, S.H.; Koues, O.I.; Collins, P.L.; Solnica-Krezel, L.; Pearce, E.J.; Pearce, E.L.; Oltz, E.M.; Stappenbeck, T.S. The colonic crypt protects stem cells from microbiota-derived metabolites. Cell 2016, 165, 1708–1720. [Google Scholar] [CrossRef] [Green Version]
- Koh, A.; De Vadder, F.; Kovatcheva-Datchary, P.; Bäckhed, F. From dietary fiber to host physiology: Short-chain fatty acids as key bacterial metabolites. Cell 2016, 165, 1332–1345. [Google Scholar] [CrossRef] [Green Version]
- Natividad, J.M.; Rytz, A.; Keddani, S.; Bergonzelli, G.; Garcia-Rodenas, C.L. Blends of human milk oligosaccharides confer intestinal epithelial barrier protection in vitro. Nutrients 2020, 12, 3047. [Google Scholar] [CrossRef]
- Weichert, S.; Jennewein, S.; Hüfner, E.; Weiss, C.; Borkowski, J.; Putze, J.; Schroten, H. Bioengineered 2′-fucosyllactose and 3-fucosyllactose inhibit the adhesion of pseudomonas aeruginosa and enteric pathogens to human intestinal and respiratory cell lines. Nutr. Res. 2013, 33, 831–838. [Google Scholar] [CrossRef]
- Idota, T.; Kawakami, H.; Murakami, Y.; Sugawara, M. Inhibition of cholera toxin by human milk fractions and sialyllactose. Biosci. Biotechnol. Biochem. 1995, 59, 417–419. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.-J.; Kim, J.W. Bacterial clearance is enhanced by α2, 3-and α2, 6-sialyllactose via receptor-mediated endocytosis and phagocytosis. Infect. Immun. 2019, 87, e00694-18. [Google Scholar] [CrossRef] [Green Version]
- Jantscher-Krenn, E.; Lauwaet, T.; Bliss, L.A.; Reed, S.L.; Gillin, F.D.; Bode, L. Human milk oligosaccharides reduce entamoeba histolytica attachment and cytotoxicity in vitro. Br. J. Nutr. 2012, 108, 1839–1846. [Google Scholar] [CrossRef] [Green Version]
- Lin, A.E.; Autran, C.A.; Szyszka, A.; Escajadillo, T.; Huang, M.; Godula, K.; Prudden, A.R.; Boons, G.-J.; Lewis, A.L.; Doran, K.S. Human milk oligosaccharides inhibit growth of group B streptococcus. J. Biol. Chem. 2017, 292, 11243–11249. [Google Scholar] [CrossRef] [Green Version]
- Stepans, M.B.F.; Wilhelm, S.L.; Hertzog, M.; Rodehorst, T.K.C.; Blaney, S.; Clemens, B.; Polak III, J.J.; Newburg, D.S. Early consumption of human milk oligosaccharides is inversely related to subsequent risk of respiratory and enteric disease in infants. Breastfeed. Med. 2006, 1, 207–215. [Google Scholar] [CrossRef]
- Goehring, K.C.; Marriage, B.J.; Oliver, J.S.; Wilder, J.A.; Barrett, E.G.; Buck, R.H. Similar to those who are breastfed, infants fed a formula containing 2′-fucosyllactose have lower inflammatory cytokines in a randomized controlled trial. J. Nutr. 2016, 146, 2559–2566. [Google Scholar] [CrossRef] [Green Version]
- Berger, P.K.; Plows, J.F.; Jones, R.B.; Alderete, T.L.; Yonemitsu, C.; Poulsen, M.; Ryoo, J.H.; Peterson, B.S.; Bode, L.; Goran, M.I. Human milk oligosaccharide 2’-fucosyllactose links feedings at 1 month to cognitive development at 24 months in infants of normal and overweight mothers. PLoS ONE 2020, 15, e0228323. [Google Scholar] [CrossRef]
- Jorgensen, J.M.; Young, R.; Ashorn, P.; Ashorn, U.; Chaima, D.; Davis, J.C.; Goonatilleke, E.; Kumwenda, C.; Lebrilla, C.B.; Maleta, K. Associations of human milk oligosaccharides and bioactive proteins with infant growth and development among Malawian mother-infant dyads. Am. J. Clin. Nutr. 2021, 113, 209–220. [Google Scholar] [CrossRef]
- Oliveros, E.; Martín, M.; Torres-Espínola, F.; Segura-Moreno, M.; Ramírez, M. Human milk levels of 2-fucosyllactose and 6-sialyllactose are positively associated with infant neurodevelopment and are not impacted by maternal BMI or diabetic status. J Nutr Food Sci. 2021, 4, 100024. [Google Scholar]
- Marriage, B.J.; Buck, R.H.; Goehring, K.C.; Oliver, J.S.; Williams, J.A. Infants fed a lower calorie formula with 2′FL show growth and 2′FL uptake like breast-fed infants. J. Pediatric Gastroenterol. Nutr. 2015, 61, 649. [Google Scholar] [CrossRef] [Green Version]
- Reverri, E.J.; Devitt, A.A.; Kajzer, J.A.; Baggs, G.E.; Borschel, M.W. Review of the clinical experiences of feeding infants formula containing the human milk oligosaccharide 2′-fucosyllactose. Nutrients 2018, 10, 1346. [Google Scholar] [CrossRef] [Green Version]
- Puccio, G.; Alliet, P.; Cajozzo, C.; Janssens, E.; Corsello, G.; Sprenger, N.; Wernimont, S.; Egli, D.; Gosoniu, L.; Steenhout, P. Effects of infant formula with human milk oligosaccharides on growth and morbidity: A randomized multicenter trial. J. Pediatric Gastroenterol. Nutr. 2017, 64, 624. [Google Scholar] [CrossRef] [Green Version]
- Parschat, K.; Melsaether, C.; Jäpelt, K.R.; Jennewein, S. Clinical evaluation of 16-Week supplementation with 5HMO-mix in healthy-term human infants to determine tolerability, safety, and effect on growth. Nutrients 2021, 13, 2871. [Google Scholar] [CrossRef]
- Austin, S.; De Castro, C.A.; Bénet, T.; Hou, Y.; Sun, H.; Thakkar, S.K.; Vinyes-Pares, G.; Zhang, Y.; Wang, P. Temporal change of the content of 10 oligosaccharides in the milk of Chinese urban mothers. Nutrients 2016, 8, 346. [Google Scholar] [CrossRef] [Green Version]
- Coppa, G.; Pierani, P.; Zampini, L.; Carloni, I.; Carlucci, A.; Gabrielli, O. Oligosaccharides in human milk during different phases of lactation. Acta Paediatr. 1999, 88, 89–94. [Google Scholar] [CrossRef]
- Kunz, C.; Meyer, C.; Collado, M.C.; Geiger, L.; García-Mantrana, I.; Bertua-Ríos, B.; Martínez-Costa, C.; Borsch, C.; Rudloff, S. Influence of gestational age, secretor, and lewis blood group status on the oligosaccharide content of human milk. J. Pediatric Gastroenterol. Nutr. 2017, 64, 789–798. [Google Scholar] [CrossRef]
- McGuire, M.K.; Meehan, C.L.; McGuire, M.A.; Williams, J.E.; Foster, J.; Sellen, D.W.; Kamau-Mbuthia, E.W.; Kamundia, E.W.; Mbugua, S.; Moore, S.E. What’s normal? Oligosaccharide concentrations and profiles in milk produced by healthy women vary geographically. Am. J. Clin. Nutr. 2017, 105, 1086–1100. [Google Scholar] [CrossRef]
- Sprenger, N.; Lee, L.Y.; De Castro, C.A.; Steenhout, P.; Thakkar, S.K. Longitudinal change of selected human milk oligosaccharides and association to infants’ growth, an observatory, single center, longitudinal cohort study. PLoS ONE 2017, 12, e0171814. [Google Scholar] [CrossRef] [Green Version]
- Thurl, S.; Munzert, M.; Henker, J.; Boehm, G.; Müller-Werner, B.; Jelinek, J.; Stahl, B. Variation of human milk oligosaccharides in relation to milk groups and lactational periods. Br. J. Nutr. 2010, 104, 1261–1271. [Google Scholar] [CrossRef] [Green Version]
- Tonon, K.M.; Miranda, A.; Abrão, A.C.F.; de Morais, M.B.; Morais, T.B. Validation and application of a method for the simultaneous absolute quantification of 16 neutral and acidic human milk oligosaccharides by graphitized carbon liquid chromatography–electrospray ionization–mass spectrometry. Food Chem. 2019, 274, 691–697. [Google Scholar] [CrossRef]
- Walsh, C.; Lane, J.A.; van Sinderen, D.; Hickey, R.M. Human milk oligosaccharides: Shaping the infant gut microbiota and supporting health. J. Funct. Foods 2020, 72, 104074. [Google Scholar] [CrossRef]
- Grummer-Strawn, L.; Krebs, N.F.; Reinold, C.M. Use of World Health Organization and CDC Growth Charts for Children Aged 0–59 Months in the United States. 2009. Available online: https://www.cdc.gov/mmwr/pdf/rr/rr5909.pdf (accessed on 13 October 2020).
- Infant Formula Act of 1980. Public Law 96-359, 26 September 1980. Available online: https://www.govinfo.gov/content/pkg/STATUTE-94/pdf/STATUTE-94-Pg1190.pdf#page=4 (accessed on 30 October 2020).
- Food and Drug Administration. Code of Federal Regulations Title 21, Infant Nutrition: Nutrient Specifications; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2019.
- Callaway, C.W.; Chumlea, W.C.; Bouchard, C.; Himes, J.H. Lohman TG, Martin AD, Mitchell CD, Mueller WH, Roche AF, Seefeldt VD: Circumference. In Anthropometric Standardization Reference Manual; Lohman, T.G., Roche, A.F., Martorell, R., Eds.; Human Kinetics Books: Champaign, IL, USA, 1988; pp. 39–54. [Google Scholar]
- Gordon, C.C.; Chumlea, W.C.; Roche, A.F. Stature, Recumbent Length, and Weight; Anthropometric Standardization Reference Manual: Champaign, IL, USA, 1988; pp. 3–8. [Google Scholar]
- Food and Drug Administration. FDA Guidance on Conduct of Clinical Trials of Medical Products during COVID-19 Public Health Emergency: Guidance for Industry, Investigators, and Institutional Review Boards; Department of Health and Human Services: 2020. Available online: https://www.hhs.gov/guidance/document/fda-guidance-conduct-clinical-trials-medical-products-during-covid-19-public-health (accessed on 20 August 2020).
- Jacobs, J.; Ostrom, K.; Fligner, M.; Verducci, J. Validation of Pediatric Tolerance Questionnaires. FASEB J. 2002, 16, A659–A660. [Google Scholar]
- Lasekan, J.B.; Linke, H.K.; Oliver, J.S.; Carver, J.D.; Blatter, M.M.; Kuchan, M.J.; Cramer, J.M.; Pollack, P.F. Milk protein–based infant formula containing rice starch and low lactose reduces common regurgitation in healthy term infants: A randomized, blinded, and prospective trial. J. Am. Coll. Nutr. 2014, 33, 136–146. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics, Committee on Nutrition. Clinical Testing of Infant Formulas with Respect to Nutritional Suitability for Term Infants; 1988. Report to the FDA; AAP: Elk Grove Village, IL, USA, 1998. [Google Scholar]
- Song, C.Q.; Kuznetsova, O. Fitting Gompertz Nonlinear Mixed Models to Infancy Growth Data with SAS Version 8 Procedure NLMIXED. In SAS Conference Proceedings: PharmaSUG; 2001; pp. 20–23. Available online: https://www.lexjansen.com/pharmasug/2001/Proceed/Stats/SP03_song.pdf (accessed on 20 August 2020).
- Hyams, J.S.; Treem, W.R.; Etienne, N.L.; Weinerman, H.; MacGilpin, D.; Hine, P.; Choy, K.; Burke, G. Effect of infant formula on stool characteristics of young infants. Pediatrics 1995, 95, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, B.; Halter, R.J.; Kuchan, M.J.; Baggs, G.E.; Ryan, A.S.; Masor, M.L. Formula tolerance in postbreastfed and exclusively formula-fed infants. Pediatrics 1999, 103, e7. [Google Scholar] [CrossRef] [Green Version]
- Kajzer, J.; Oliver, J.; Marriage, B. Gastrointestinal tolerance of formula supplemented with oligosaccharides. FASEB J. 2016, 30, 671.4. [Google Scholar]
- Bode, L. Human milk oligosaccharides: Prebiotics and beyond. Nutr. Rev. 2009, 67 (Suppl. 2), S183–S191. [Google Scholar]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Gotoh, A.; Katoh, T.; Sakanaka, M.; Ling, Y.; Yamada, C.; Asakuma, S.; Urashima, T.; Tomabechi, Y.; Katayama-Ikegami, A.; Kurihara, S. Sharing of human milk oligosaccharides degradants within bifidobacterial communities in faecal cultures supplemented with bifidobacterium bifidum. Sci. Rep. 2018, 8, 13958. [Google Scholar] [CrossRef]
- Lawson, M.A.; O’Neill, I.J.; Kujawska, M.; Javvadi, S.G.; Wijeyesekera, A.; Flegg, Z.; Chalklen, L.; Hall, L.J. Breast milk-derived human milk oligosaccharides promote bifidobacterium interactions within a single ecosystem. ISME J. 2020, 14, 635–648. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CF (n = 126) | EF (n = 128) | HM (n = 102) | Total (n = 356) | |
|---|---|---|---|---|
| Sex, n (%) | ||||
| Male | 62 (49.2) | 62 (48.4) | 49 (48.0) | 173 (48.6) |
| Female | 64 (50.8) | 66 (51.6) | 53 (52.0) | 183 (51.4) |
| Ethnicity, n (%) | ||||
| Hispanic or Latino | 25 (19.8) | 26 (20.3) | 25 (24.5) | 76 (21.3) |
| Not Hispanic or Latino | 100 (79.4) | 102 (79.7) | 77 (75.5) | 279 (78.4) |
| Not Reported | 1 (0.8) | 0 (0.0) | 0 (0.0) | 1 (0.3) |
| Race, n (%) | ||||
| American Indian or Alaska Native | 0 (0.0) | 1 (0.8) | 2 (2.0) | 3 (0.8) |
| Asian | 1 (0.8) | 1 (0.8) | 1 (1.0) | 3 (0.8) |
| Black or African American | 43 (34.1) | 37 (28.9) | 17 (16.7) | 97 (27.2) |
| Native Hawaiian or Other Pacific Islanders | 0 (0.0) | 0 (0.0) | 1 (1.0) | 1 (0.3) |
| White | 73 (57.9) | 78 (60.9) | 71 (69.6) | 222 (62.4) |
| Others | 9 (7.2) | 11 (8.6) | 10 (9.8) | 30 (8.5) |
| Mode of Delivery, n (%) | ||||
| Vaginal | 85 (67.5) | 83 (64.8) | 72 (70.6) | 240 (67.4) |
| C-Section | 41 (32.5) | 45 (35.2) | 30 (29.4) | 116 (32.6) |
| Gestational age, weeks 1 | 38.8 ± 0.1 | 38.9 ± 0.1 | 38.9 ± 0.1 | 38.8 ± 0.1 |
| Age at enrollment, days 1 | 7.8 ± 0.3 | 7.2 ± 0.3 | 8.0 ± 0.4 | 7.6 ± 0.2 |
| Birth weight (g) 1 | 3356 ± 38 | 3372 ± 38 | 3381 ± 43 | 3369 ± 23 |
| Birth length (cm) 1 | 50.2 ± 0.2 | 50.3 ± 0.2 | 50.9 ± 0.2 | 50.4 ± 0.1 |
| Birth head circumference (cm) 1 | 34.2 ± 0.2 | 34.6 ± 0.2 | 34.1 ± 0.3 | 34.3 ± 0.1 |
| Protocol Evaluable Cohorts (PE) | Study Groups (n) | D14-D119 2 | p-Values # | D14-D28 | D28-D42 | D42-D56 | D56-D84 | D84-D119 | |
|---|---|---|---|---|---|---|---|---|---|
| Weight gain, g/day | All Pre & Post COVID-19 | CF (77) | 29.9 ± 0.7 | 0.348 | 39.6 ± 1.2 | 37.0 ± 1.0 | 38.9 ± 0.7 | 22.3 ± 0.9 | 22.3 ± 0.9 |
| EF (72) | 29.4 ± 0.7 | 38.1 ± 1.3 | 35.9 ±1.1 | 33.1 ± 0.9 | 28.7 ± 0.8 | 22.4 ± 0.8 | |||
| HM (73) | 27.9 ± 0.8 | 39.5 ± 1.4 | 36.0 ± 1.1 | 32.1 ± 0.9 | 26.5 ± 0.8 | 19.5 ± 0.9 | |||
| Post COVID-19 | CF (72) | 30.0 ± 0.7 | 0.337 | 39.7 ± 1.2 | 37.1 ± 1.0 | 34.0 ± 0.8 | 29.1 ± 0.8 | 22.5 ± 0.9 | |
| EF (69) | 29.4 ± 0.8 | 38.3 ± 1.3 | 36.0 ± 1.1 | 33.2 ± 0.9 | 28.7 ± 0.8 | 22.4 ± 0.8 | |||
| HM (68) | 28.1 ± 0.8 | 39.4 ± 1.5 | 36.0 ± 1.2 | 32.3 ± 1.0 | 26.8 ± 0.8 | 19.9 ± 0.9 | |||
| Length gain, cm/day | All Pre & Post COVID-19 | CF (77) | 0.109 ± 0.003 | 0.890 | 0.148 ± 0.006 | 0.131 ± 0.004 | 0.118 ± 0.003 | 0.102 ± 0.003 | 0.088 ± 0.005 |
| EF (72) | 0.110 ± 0.002 | 0.153 ± 0.006 | 0.135 ± 0.004 | 0.120 ± 0.002 | 0.103 ± 0.002 | 0.086 ± 0.005 | |||
| HM (73) | 0.103 ± 0.002 | 0.140 ± 0.006 | 0.125 ± 0.004 | 0.112 ± 0.003 | 0.098 ± 0.003 | 0.085 ± 0.004 | |||
| Post COVID-19 | CF (72) | 0.109 ± 0.003 | 0.918 | 0.150 ± 0.006 | 0.133 ± 0.004 | 0.119 ± 0.003 | 0.103 ± 0.003 | 0.087 ± 0.005 | |
| EF (69) | 0.110 ± 0.002 | 0.153 ± 0.006 | 0.135 ± 0.004 | 0.120 ± 0.003 | 0.103 ± 0.003 | 0.086 ± 0.005 | |||
| HM (68) | 0.110 ± 0.002 | 0.141 ± 0.006 | 0.126 ± 0.004 | 0.113 ± 0.003 | 0.099 ± 0.003 | 0.085 ± 0.005 | |||
| Head circumference gain, cm/day | All Pre & Post COVID-19 | CF (77) | 0.058 ± 0.001 | SI $ | 0.092 ± 0.003 | 0.078 ± 0.002 | 0.066 ± 0.002 | 0.052 ± 0.001 | 0.039 ± 0.002 |
| EF (72) | 0.059 ± 0.002 | 0.089 ± 0.003 | 0.077 ± 0.002 | 0.066 ± 0.002 | 0.054 ± 0.002 | 0.042 ± 0.002 | |||
| HM (72) | 0.056 ± 0.001 | 0.092 ± 0.004 | 0.076 ± 0.002 | 0.063 ± 0.002 | 0.049 ± 0.001 | 0.035 ± 0.002 | |||
| Post COVID-19 | CF (72) | 0.058 ± 0.001 | 0.739 | 0.092 + 0.004 | 0.078 ± 0.002 | 0.066 ± 0.002 | 0.053 ± 0.001 | 0.039 ± 0.002 | |
| EF (69) | 0.059 ± 0.002 | 0.089 ± 0.003 | 0.077 ± 0.002 | 0.066 ± 0.002 | 0.054 ± 0.002 | 0.042 ± 0.003 | |||
| HM (68) | 0.056 ± 0.001 | 0.091 ± 0.004 | 0.076 ± 0.003 | 0.063 ± 0.002 | 0.049 ± 0.001 | 0.036 ± 0.002 | |||
| Intent-to-treat Cohorts (ITT) | |||||||||
| Weight gain, g/day | All Pre & Post COVID-19 | CF (86) | 29.9 ± 0.6 | 0.271 | 39.6 ± 1.1 | 37.0 ± 0.9 | 33.9 ± 0.8 | 28.9 ± 0.7 | 22.3 ± 0.8 |
| EF (86) | 29.5 ± 0.7 | 37.8 ± 1.1 | 35.8 ± 1.0 | 33.1 ± 0.8 | 28.9 ± 0.7 | 22.8 ± 0.7 | |||
| HM (86) | 28.1 ± 0.7 | 38.7 ± 1.3 | 35.5 ± 1.0 | 32.0 ± 0.9 | 26.7 ± 0.7 | 20.3 ± 0.9 | |||
| Post COVID-19 | CF (82) | 30.0 ± 0.6 | 0.279 | 39.7 ± 1.1 | 37.2 ± 0.9 | 34.0 ± 0.8 | 29.1 ± 0.7 | 22.5 ± 0.8 | |
| EF (82) | 29.6 ± 0.7 | 38.0 ± 1.2 | 35.9 ± 1.0 | 33.2 ± 0.8 | 28.9 ± 0.7 | 22.8.0 ± 0.8 | |||
| HM (81) | 28.2 ± 0.7 | 38.4 ± 1.3 | 35.4 ± 1.1 | 32.0 ± 0.9 | 27.0 ± 0.8 | 20.7 ± 0.9 | |||
| Length gain, cm/day | All Pre & Post COVID-19 | CF (86) | 0.108 ± 0.002 | 0.708 | 0.147 ± 0.005 | 0.131 ± 0.004 | 0.117 ± 0.003 | 0.102 ± 0.002 | 0.087 ± 0.004 |
| EF (86) | 0.110 ± 0.002 | 0.151 ± 0.005 | 0.135 ± 0.003 | 0.121 ± 0.002 | 0.104 ± 0.002 | 0.088 ± 0.004 | |||
| HM (88) | 0.104 ± 0.002 | 0.143 ± 0.005 | 0.126 ± 0.003 | 0.112 ± 0.003 | 0.098 ± 0.003 | 0.084 ± 0.004 | |||
| Post COVID-19 | CF (81) | 0.109 ± 0.002 | 0.627 | 0.149 ± 0.005 | 0.132 ± 0.004 | 0.118 ± 0.003 | 0.102 ± 0.002 | 0.086 ± 0.004 | |
| EF (82) | 0.110 ± 0.002 | 0.151 ± 0.005 | 0.135 ± 0.003 | 0.121 ± 0.002 | 0.105 ± 0.002 | 0.089 ± 0.004 | |||
| HM (81) | 0.104 ± 0.002 | 0.143 ± 0.005 | 0.126 ± 0.003 | 0.112 ± 0.003 | 0.098 ± 0.003 | 0.084 ± 0.004 | |||
| Head circumference gain, cm/day | All Pre & Post COVID-19 | CF (86) | 0.038 ± 0.002 | SI $ | 0.092 ± 0.003 | 0.078 ± 0.002 | 0.066 ± 0.002 | 0.052 ± 0.001 | 0.058 ± 0.001 |
| EF (86) | 0.043 ± 0.003 | 0.086 ± 0.003 | 0.075 ± 0.002 | 0.065 ± 0.001 | 0.054 ± 0.001 | 0.059 ± 0.001 | |||
| HM (88) | 0.036 ± 0.002 | 0.090 ± 0.004 | 0.074 ± 0.002 | 0.062 ± 0.002 | 0.054 ± 0.001 | 0.055 ± 0.001 | |||
| Post COVID-19 | CF (81) | 0.039 ± 0.002 | SI $ | 0.092 ± 0.003 | 0.078 ± 0.002 | 0.066 ± 0.002 | 0.053 ± 0.001 | 0.058 ± 0.001 | |
| EF (82) | 0.043 ± 0.003 | 0.086 ± 0.003 | 0.075 ± 0.002 | 0.065 ± 0.002 | 0.054 ± 0.001 | 0.059 ± 0.001 | |||
| HM (81) | 0.036 ± 0.002 | 0.090 ± 0.004 | 0.075 ± 0.002 | 0.063 ± 0.002 | 0.049 ± 0.001 | 0.056 ± 0.001 |
| Protocol Evaluable Cohort (PE) 1 | Intent-to-treat Cohort (ITT) 1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study Days | Control Formula (CF) | Experimental Formula (EF) | Human Milk (HM) | p-Values | Control Formula (CF) | Experimental Formula (EF) | Human Milk (HM) | p-Values # | |
| Study formula intake, mL | D1-D28 | 683 ± 14 (76) | 682 ± 16 (72) | NM * | 0.916 | 662 ± 12 (102) | 657 ± 13 (117) | NM * | 0.864 |
| Spit-up/Vomit as percent of feeding, % | D1-D28 | 13.0 ± 1.4 (76) | 16.6 ± 2.9 (72) | 14.4 ± 2.0 (73) | 0.546 | 15.1 ± 1.5 (106) | 16.4 ± 2.2 (118) | 13.4 ± 1.6 (100) | 0.973 |
| Stool frequency, #/day | D1-D28 | 2.0 ± 0.2 (75) | 3.0 ± 0.2 (72) | 5.4 ± 0.3 (73) | <0.001 | 1.9 ± 0.1 (101) | 3.2 ± 0.2 (117) | 5.4 ± 0.2 (99) | <0.001 |
| D119 | 1.5 ± 0.1 (73) | 1.9 ± 0.1 (67) | 2.0 ± 0.2 (71) | 0.004 | 1.5 ± 0.1 (76) | 1.8 ± 0.1 (71) | 2.1 ± 0.2 (82) | 0.005 | |
| Mean rank stool consistency (MRSC), score 2 | D1-D28 | 2.19 ± 0.06 (75) | 2.05 ± 0.06 (72) | 1.88 ± 0.06 (73) | 0.177 | 2.27 ± 0.06 (102) | 2.05 ± 0.05 (118) | 1.87 ± 0.05 (100) | <0.001 |
| D119 | 2.53 ± 0.07 (73) | 2.29 ± 0.08 (67) | 1.99 ± 0.08 (67) | 0.038 | 2.57 ± 0.07 (77) | 2.30 ± 0.08 (71) | 1.99 ± 0.07 (78) | 0.036 | |
| Predominant stool consistency, n (%) | D1-D28
| 8 (10.8) 44 (59.5) 21 (28.4) 1 (1.4) 0 (0.0) | 13 (18.3) 40 (56.3) 17 (23.9 1 (1.4)) 0 (0.0) | 18 (25.0) 43 (59.7) 11 (15.3) 0 (0.0) 0 (0.0) | 0.379 | 8 (7.9) 60 (59.4) 30 (59.4) 3 (3.0) 0 (0.0) | 23 (20.0) 63 (54.8) 28 (24.3) 1 (0.9) 0(0.0) | 24 (24.2) 63 (62.6) 13 (13.1) 0(0.0) 0(0.0) | 0.004 |
| Predominant stool color, n (%) | D1-D28
| 28 (38.4) 27 (37.0) 17 (23.3) 1 (1.4) | 39 (54.9) 17 (23.9) 15 (21.1) 0 (0.0) | 69 (94.5) 3 (4.1) 1 (1.4) 0 (0.0) | 0.363 | 39 (39.4) 36 (36.4) 23 (23.2) 1 (1.0) | 74 (63.2) 22 (18.8) 21 (17.9) 0(0.0) | 95 (95) 4 (4.0) 1 (1.0) 0(0.0) | 0.013 |
| Average constipation dimension 3 | D119 | 1.70 ± 0.06 (76) | 1.52 ± 0.05 (72) | 1.50 ± 0.06 (73) | 0.030 | 1.76 ± 0.07 (84) | 1.55 ± 0.05 (83) | 1.50 ± 0.05 (88) | 0.020 |
| Average loose stools dimension 3 | D119 | 1.76 ± 0.06 (76) | 2.03 ± 0.09 (72) | 1.90 ± 0.06 (73) | 0.006 | 1.79 ± 0.06 (84) | 2.0 ± 0.08 (83) | 1.89 ± 0.06 (88) | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lasekan, J.; Choe, Y.; Dvoretskiy, S.; Devitt, A.; Zhang, S.; Mackey, A.; Wulf, K.; Buck, R.; Steele, C.; Johnson, M.; et al. Growth and Gastrointestinal Tolerance in Healthy Term Infants Fed Milk-Based Infant Formula Supplemented with Five Human Milk Oligosaccharides (HMOs): A Randomized Multicenter Trial. Nutrients 2022, 14, 2625. https://doi.org/10.3390/nu14132625
Lasekan J, Choe Y, Dvoretskiy S, Devitt A, Zhang S, Mackey A, Wulf K, Buck R, Steele C, Johnson M, et al. Growth and Gastrointestinal Tolerance in Healthy Term Infants Fed Milk-Based Infant Formula Supplemented with Five Human Milk Oligosaccharides (HMOs): A Randomized Multicenter Trial. Nutrients. 2022; 14(13):2625. https://doi.org/10.3390/nu14132625
Chicago/Turabian StyleLasekan, John, Yong Choe, Svyatoslav Dvoretskiy, Amy Devitt, Sue Zhang, Amy Mackey, Karyn Wulf, Rachael Buck, Christine Steele, Michelle Johnson, and et al. 2022. "Growth and Gastrointestinal Tolerance in Healthy Term Infants Fed Milk-Based Infant Formula Supplemented with Five Human Milk Oligosaccharides (HMOs): A Randomized Multicenter Trial" Nutrients 14, no. 13: 2625. https://doi.org/10.3390/nu14132625
APA StyleLasekan, J., Choe, Y., Dvoretskiy, S., Devitt, A., Zhang, S., Mackey, A., Wulf, K., Buck, R., Steele, C., Johnson, M., & Baggs, G. (2022). Growth and Gastrointestinal Tolerance in Healthy Term Infants Fed Milk-Based Infant Formula Supplemented with Five Human Milk Oligosaccharides (HMOs): A Randomized Multicenter Trial. Nutrients, 14(13), 2625. https://doi.org/10.3390/nu14132625