How Parenting and Family Characteristics Predict the Use of Feeding Practices among Parents of Preschoolers: A Cross-Sectional Study in Beijing, China

 ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedures
2.1.1. Study Design and Sampling
2.1.2. Procedures
2.2. Measurement
2.2.1. Parental Feeding Practices
2.2.2. Parenting
2.2.3. Family Characteristics and Children’s BMI
2.3. Ethical Consideration
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Scores of Feeding Practices
3.3. Parenting
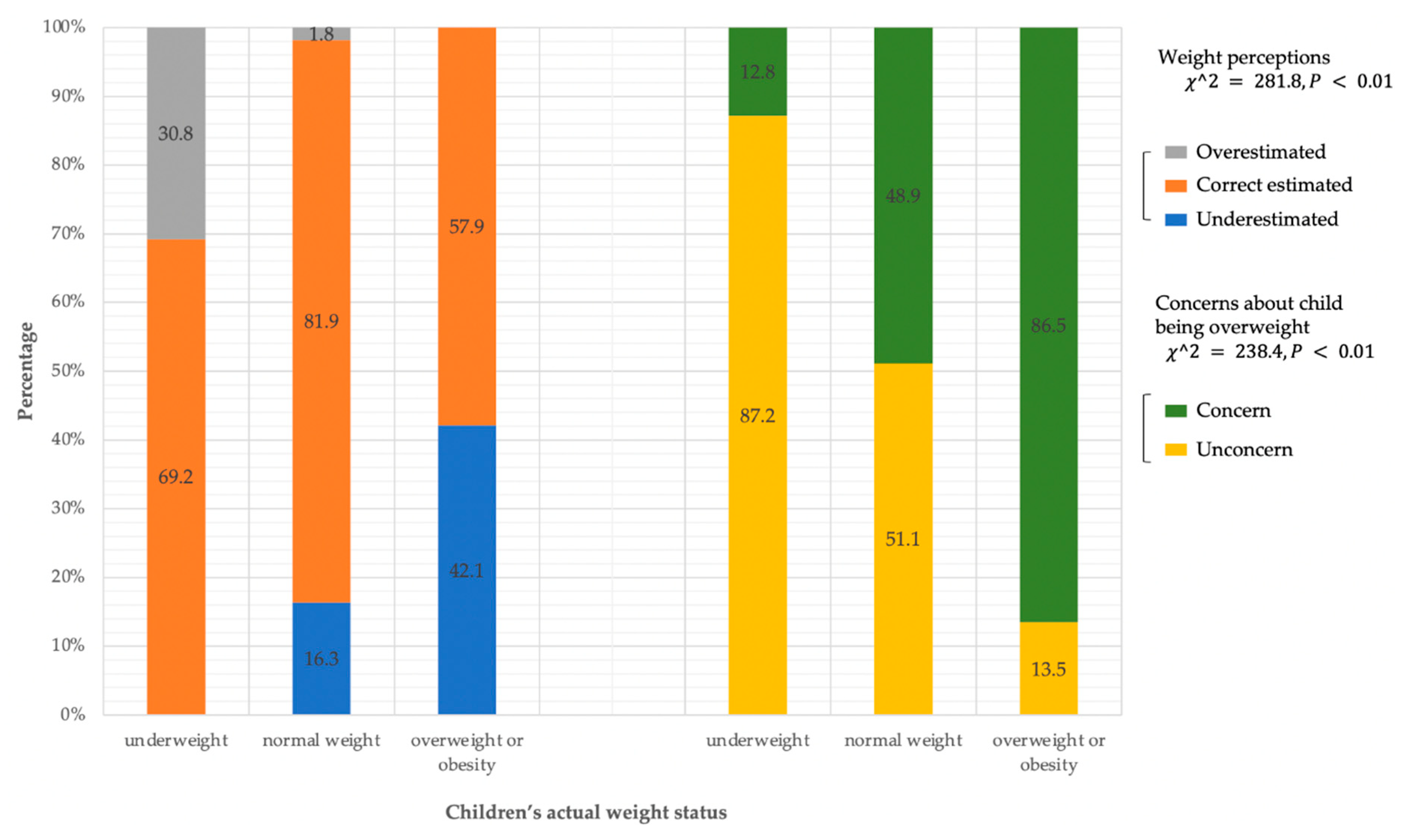
3.3.1. Parents’ Perceptions and Concerns about Weight
3.3.2. Parenting Stress and Competence
3.4. Family Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collaboration, N.C.D.R.F. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.F.; Wang, L.; Pan, A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef]
- Colquitt, J.L.; Loveman, E.; O’Malley, C.; Azevedo, L.B.; Mead, E.; Al-Khudairy, L.; Ells, L.J.; Metzendorf, M.I.; Rees, K. Diet, physical activity, and behavioural interventions for the treatment of overweight or obesity in preschool children up to the age of 6 years. Cochrane Database Syst. Rev. 2016, 3, Cd012105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, C.; Zhang, Y.; Yong, C.; Xi, Y.; Huo, J.; Zou, H.; Liang, J.; Jiang, Z.; Lin, Q. Association between Parents’ Perceptions of Preschool Children’s Weight, Feeding Practices and Children’s Dietary Patterns: A Cross-Sectional Study in China. Nutrients 2021, 13, 3767. [Google Scholar] [CrossRef]
- Burnett, A.J.; Lacy, K.E.; Russell, C.G.; Spence, A.C.; Worsley, A.; Lamb, K.E. Groups of mothers based on feeding practices and their associations with dietary quality of pre-school children: A latent profile analysis. Appetite 2021, 168, 105754. [Google Scholar] [CrossRef]
- Campbell, K.; Andrianopoulos, N.; Hesketh, K.; Ball, K.; Crawford, D.; Brennan, L.; Corsini, N.; Timperio, A. Parental use of restrictive feeding practices and child BMI z-score. A 3-year prospective cohort study. Appetite 2010, 55, 84–88. [Google Scholar] [CrossRef]
- Guo, S.; Wang, Y.; Fries, L.R.; Li, Y.; Zhang, N.; Zhang, H.; Wei, H.; Jiang, X.; Shang, L. Infant and preschooler feeding behaviors in Chinese families: A systematic review. Appetite 2021, 168, 105768. [Google Scholar] [CrossRef]
- Gicevic, S.; Aftosmes-Tobio, A.; Manganello, J.A.; Ganter, C.; Simon, C.L.; Newlan, S.; Davison, K.K. Parenting and childhood obesity research: A quantitative content analysis of published research 2009-2015. Obes. Rev. 2016, 17, 724–734. [Google Scholar] [CrossRef]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [Green Version]
- Finnane, J.M.; Jansen, E.; Mallan, K.M.; Daniels, L.A. Mealtime Structure and Responsive Feeding Practices Are Associated With Less Food Fussiness and More Food Enjoyment in Children. J. Nutr. Educ. Behav. 2017, 49, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniels, L.A. Feeding Practices and Parenting: A Pathway to Child Health and Family Happiness. Ann. Nutr. Metab. 2019, 74, 29–42. [Google Scholar] [CrossRef] [PubMed]
- DiSantis, K.I.; Hodges, E.A.; Johnson, S.L.; Fisher, J.O. The role of responsive feeding in overweight during infancy and toddlerhood: A systematic review. Int. J. Obes. 2011, 35, 480–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, M.M.; Aboud, F.E. Responsive feeding is embedded in a theoretical framework of responsive parenting. J. Nutr. 2011, 141, 490–494. [Google Scholar] [CrossRef] [Green Version]
- Hurley, K.M.; Cross, M.B.; Hughes, S.O. A systematic review of responsive feeding and child obesity in high-income countries. J. Nutr. 2011, 141, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Chan, L.; Magarey, A.M.; Daniels, L.A. Maternal feeding practices and feeding behaviors of Australian children aged 12–36 months. Mater. Child Health J. 2011, 15, 1363–1371. [Google Scholar] [CrossRef] [Green Version]
- Vaughn, A.E.; Ward, D.S.; Fisher, J.O.; Faith, M.S.; Hughes, S.O.; Kremers, S.P.J.; Musher-Eizenman, D.R.; O’Connor, T.M.; Patrick, H.; Power, T.G. Fundamental constructs in food parenting practices: A content map to guide future research. Nutr. Rev. 2016, 74, 98–117. [Google Scholar] [CrossRef] [Green Version]
- Lydecker, J.A.; Grilo, C.M. The apple of their eye: Attitudinal and behavioral correlates of parents’ perceptions of child obesity. Obesity 2016, 24, 1124–1131. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhu, D.; Cheng, X.; Liuzhou, Y.; Zhu, B.; Montgomery, S.; Cao, Y. Maternal perception of child weight and concern about child overweight mediates the relationship between child weight and feeding practices. Public Health Nutr. 2022, 25, 1780–1789. [Google Scholar] [CrossRef]
- Faith, M.S.; Scanlon, K.S.; Birch, L.L.; Francis, L.A.; Sherry, B. Parent-child feeding strategies and their relationships to child eating and weight status. Obes. Res. 2004, 12, 1711–1722. [Google Scholar] [CrossRef]
- Francis, L.A.; Hofer, S.M.; Birch, L.L. Predictors of maternal child-feeding style: Maternal and child characteristics. Appetite 2001, 37, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Rietmeijer-Mentink, M.; Paulis, W.D.; van Middelkoop, M.; Bindels, P.J.; van der Wouden, J.C. Difference between parental perception and actual weight status of children: A systematic review. Matern. Child Nutr. 2013, 9, 3–22. [Google Scholar] [CrossRef]
- Hurley, K.M.; Black, M.M.; Papas, M.A.; Caulfield, L.E.; Caufield, L.E. Maternal symptoms of stress, depression, and anxiety are related to nonresponsive feeding styles in a statewide sample of WIC participants. J. Nutr. 2008, 138, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Farrow, C.V.; Blissett, J.M. Is maternal psychopathology related to obesigenic feeding practices at 1 year? Obes. Res. 2005, 13, 1999–2005. [Google Scholar] [CrossRef] [PubMed]
- Chi, P.; Li, X.; Tam, C.C.; Du, H.; Zhao, G.; Zhao, J. Parenting Mediates the Impact of Caregivers’ Distress on Children’s Well-Being in Families Affected by HIV/AIDS. AIDS Behav. 2015, 19, 2130–2139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salarkia, N.; Omidvar, N.; Zaeri, F.; Zeinab, H.E.; Neyestani, T.R. Mother’s Self-Efficacy Mediates the Relationship Between Household Food Insecurity and Maternal Infant Feeding Styles. Matern. Child Health J. 2016, 20, 602–612. [Google Scholar] [CrossRef]
- Mitchell, S.; Brennan, L.; Hayes, L.; Miles, C.L. Maternal psychosocial predictors of controlling parental feeding styles and practices. Appetite 2009, 53, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Duraccio, K.M.; Zaugg, K.K.; Nottingham, K.; Jensen, C.D. Maternal self-efficacy is associated with mother-child feeding practices in middle childhood. Eat. Behav. 2021, 40, 101475. [Google Scholar] [CrossRef]
- Holley, C.E.; Haycraft, E. Mothers’ perceptions of self-efficacy and satisfaction with parenting are related to their use of controlling and positive food parenting practices. Matern. Child Nutr. 2021, 18, e13272. [Google Scholar] [CrossRef] [PubMed]
- Yang, J. China’s one-child policy and overweight children in the 1990s. Soc. SCI. Med. 2007, 64, 2043–2057. [Google Scholar] [CrossRef] [PubMed]
- Potter, C.; Gibson, E.L.; Ferriday, D.; Griggs, R.L.; Coxon, C.; Crossman, M.; Norbury, R.; Rogers, P.J.; Brunstrom, J.M. Associations between number of siblings, birth order, eating rate and adiposity in children and adults. Clin. Obes. 2021, 11, e12438. [Google Scholar] [CrossRef] [PubMed]
- Min, K.; Wang, J.; Liao, W.; Astell-Burt, T.; Feng, X.; Cai, S.; Liu, Y.; Zhang, P.; Su, F.; Yang, K.; et al. Dietary patterns and their associations with overweight/obesity among preschool children in Dongcheng District of Beijing: A cross-sectional study. BMC Public Health 2021, 21, 223. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Charlotte, J.; Eric, J.M. A Measure of Parenting Satisfaction and Efficacy. J. Clin. Child Psychol. 2010, 18, 167–175. [Google Scholar]
- World Health Organization (WHO). Child Growth Standards. Available online: http://www.who.int/childgrowth/standards/bmi_for_age/en (accessed on 12 October 2018).
- World Health Organization (WHO). Growth Reference 5–19 Years. Available online: http://www.who.int/growthref/who2007_bmi_for_age/en (accessed on 13 October 2018).
- de Onis, M.; Lobstein, T. Defining obesity risk status in the general childhood population: Which cut-offs should we use? Int. J. Pediatr. Obes. 2010, 5, 458–460. [Google Scholar] [CrossRef]
- Ayine, P.; Selvaraju, V.; Venkatapoorna, C.M.K.; Geetha, T. Parental Feeding Practices in Relation to Maternal Education and Childhood Obesity. Nutrients 2020, 12, 1033. [Google Scholar] [CrossRef] [Green Version]
- Gebru, N.W.; Gebreyesus, S.H.; Yirgu, R.; Habtemariam, E.; Abebe, D.S. The relationship between caregivers’ feeding practices and children’s eating behaviours among preschool children in Ethiopia. Appetite 2021, 157, 104992. [Google Scholar] [CrossRef]
- Jessica, S.G.; Sanne, M.G.; Stef, P.K. The association of parenting practices with toddlers’ dietary intake and BMI, and the moderating role of general parenting and child temperament. Public Health Nutr. 2020, 23, 2521–2529. [Google Scholar]
- Shloim, N.; Edelson, L.R.; Martin, N.; Hetherington, M.M. Parenting Styles, Feeding Styles, Feeding Practices, and Weight Status in 4–12 Year-Old Children: A Systematic Review of the Literature. Front. Psychol. 2015, 6, 1849. [Google Scholar] [CrossRef] [Green Version]
- Webber, L.; Hill, C.; Cooke, L.; Carnell, S.; Wardle, J. Associations between child weight and maternal feeding styles are mediated by maternal perceptions and concerns. Eur. J. Clin. Nutr. 2010, 64, 259–265. [Google Scholar] [CrossRef] [Green Version]
- Gregory, J.E.; Paxton, S.J.; Brozovic, A.M. Maternal feeding practices, child eating behaviour and body mass index in preschool-aged children: A prospective analysis. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, J.; Wang, V.H.; Xue, H.; Mi, J.; Wang, Y. Maternal perception of child overweight status and its association with weight-related parenting practices, their children’s health behaviours and weight change in China. Public Health Nutr. 2017, 20, 2096–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.Y.; Lemon, S.C.; Pagoto, S.L.; Barton, B.A.; Lapane, K.L.; Goldberg, R.J. Personal and parental weight misperception and self-reported attempted weight loss in US children and adolescents, National Health and Nutrition Examination Survey, 2007–2008 and 2009–2010. Prev. Chronic. Dis. 2014, 11, E132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos Salas, X.; Buoncristiano, M.; Williams, J.; Kebbe, M.; Spinelli, A.; Nardone, P.; Rito, A.; Duleva, V.; Musić Milanović, S.; Kunesova, M.; et al. Parental Perceptions of Children’s Weight Status in 22 Countries: The WHO European Childhood Obesity Surveillance Initiative: COSI 2015/2017. Obes. Facts 2021, 14, 658–674. [Google Scholar] [CrossRef]
- Park, S.H. Asian Parents’ Perception of Child Weight Status: A Systematic Review. J. Child Fam. Stud. 2017, 26, 2363–2373. [Google Scholar] [CrossRef]
- Lundahl, A.; Kidwell, K.M.; Nelson, T.D. Parental underestimates of child weight: A meta-analysis. Pediatrics 2014, 133, e689–e703. [Google Scholar] [CrossRef] [Green Version]
- Alshahrani, A.; Shuweihdi, F.; Swift, J.; Avery, A. Underestimation of overweight weight status in children and adolescents aged 0–19 years: A systematic review and meta-analysis. Obes. SCI. Pract. 2021, 7, 760–796. [Google Scholar] [CrossRef]
- Freitas, F.R.; Moraes, D.E.B.; Warkentin, S.; Mais, L.A.; Ivers, J.F.; Taddei, J. Maternal restrictive feeding practices for child weight control and associated characteristics. J. Pediatr. 2019, 95, 201–208. [Google Scholar] [CrossRef]
- Martínez, A.M.S.; Franco, H.F.C.; de León, D.B.E.; Franco, G.E.M.; de la Garza, F.J.G.; Rocha, G.M.N. Estimating and differentiating maternal feeding practices in a country ranked first in childhood obesity. Public Health Nutr. 2020, 23, 620–630. [Google Scholar] [CrossRef]
- Zhang, T.; Cai, L.; Jing, J.; Ma, L.; Ma, J.; Chen, Y. Parental perception of child weight and its association with weight-related parenting behaviours and child behaviours: A Chinese national study. Public Health Nutr. 2018, 21, 1671–1680. [Google Scholar] [CrossRef] [Green Version]
- Loth, K.A.; Mohamed, N.; Trofholz, A.; Tate, A.; Berge, J.M. Associations between parental perception of- and concern about-child weight and use of specific food-related parenting practices. Appetite 2021, 160, 105068. [Google Scholar] [CrossRef] [PubMed]
- Ek, A.; Sorjonen, K.; Eli, K.; Lindberg, L.; Nyman, J.; Marcus, C.; Nowicka, P. Associations between Parental Concerns about Preschoolers’ Weight and Eating and Parental Feeding Practices: Results from Analyses of the Child Eating Behavior Questionnaire, the Child Feeding Questionnaire, and the Lifestyle Behavior Checklist. PLoS ONE 2016, 11, e0147257. [Google Scholar] [CrossRef] [Green Version]
- Haines, J.; Downing, K.L.; Tang, L.; Campbell, K.J.; Hesketh, K.D. Associations between maternal concern about child’s weight and related behaviours and maternal weight-related parenting practices: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 104. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, M.J.; Canavarro, M.C.; Moreira, H. How can mindful parenting be related to emotional eating and overeating in childhood and adolescence? The mediating role of parenting stress and parental child-feeding practices. Appetite 2019, 138, 102–114. [Google Scholar] [CrossRef]
- Satter, E. The feeding relationship: Problems and interventions. J. Pediatr. 1990, 117, S181–S189. [Google Scholar] [PubMed]
- Birch, L.L. Child feeding practices and the etiology of obesity. Obesity 2006, 14, 343. [Google Scholar]
- Mosli, R.H.; Lumeng, J.C.; Kaciroti, N.; Peterson, K.E.; Rosenblum, K.; Baylin, A.; Miller, A.L. Higher weight status of only and last-born children. Maternal feeding and child eating behaviors as underlying processes among 4–8 year olds. Appetite 2015, 92, 167–172. [Google Scholar]
- Pratt, M.; Hoffmann, D.; Taylor, M.; Musher-Eizenman, D. Structure, coercive control, and autonomy promotion: A comparison of fathers’ and mothers’ food parenting strategies. J. Health Psychol. 2019, 24, 1863–1877. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | n | % |
|---|---|---|
| Children’s characteristics | ||
| Gender | ||
| Male | 1546 | 51.7 |
| Female | 1444 | 48.3 |
| Age (Month) | ||
| Mean (SD) | 66.3 | 7.3 |
| Median (Min, Max) | 65.0 | [33.0, 84.0] |
| Only child status | ||
| Yes | 2059 | 68.9 |
| No | 931 | 31.1 |
| BMI | ||
| Mean (SD) | 15.6 | 1.8 |
| Median (Min, Max) | 15.3 | [10.6, 34.7] |
| Weight status | ||
| Normal weight | 2419 | 80.9 |
| Underweight | 39 | 1.3 |
| Overweight | 363 | 12.1 |
| Obesity | 169 | 5.7 |
| Parents’ characteristics | ||
| Family roles | ||
| Father | 688 | 23.0 |
| Mother | 2302 | 77.0 |
| Marital status | ||
| Married | 2851 | 95.4 |
| Others | 139 | 4.6 |
| Household income per capita (CNY) | ||
| 80,000 | 261 | 8.7 |
| 81,000–100,000 | 386 | 12.9 |
| 101,000–150,000 | 591 | 19.8 |
| >150,000 | 1605 | 53.7 |
| From a one-child family | ||
| Father | 466 | 15.6 |
| Mother | 554 | 18.5 |
| Both | 1333 | 44.6 |
| None | 637 | 21.3 |
| Perception of children’s weight | ||
| Correct perception | 2315 | 77.4 |
| Misperception | 675 | 22.6 |
| Parenting stress | ||
| Mean (SD) | 2.3 | 0.8 |
| Median (Min, Max) | 2.2 | [1.0, 5.0] |
| Parenting competence | ||
| Mean (SD) | 4.0 | 0.6 |
| Median (Min, Max) | 4.0 | [1.0, 5.0] |
| Feeding Practices | Children’s Actual Weight Status | Total (n = 2990) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Normal Weight (n = 2419) | Underweight (n = 39) | Overweight (n = 363) | Obesity (n = 169) | Mean (SD) | Median [Min, Max] | ||
| Restriction | 3.8 (0.8) a | 3.7 (0.8) ab | 3.9 (0.7) b | 4.0 (0.8) b | 3.8 (0.8) | 4.0 [1.0, 5.0] | <0.001 |
| Pressure to eat | 3.3 (0.8) a | 3.7 (0.6) b | 3.1 (0.8) c | 2.9 (0.9) c | 3.2 (0.8) | 3.0 [1.0, 5.0] | <0.001 |
| Monitoring | 3.9 (1.0) | 3.9 (1.0) | 3.9 (1.0) | 4.0 (1.0) | 3.9 (1.0) | 4.0 [1.0, 5.0] | 0.215 |
| Restriction β (95%CI) | Pressure to Eat β (95%CI) | Monitoring β (95%CI) | |
|---|---|---|---|
| Normal weight (n = 2419) | |||
| Misperception of child’s weight | |||
| Correct estimate | 1 | 1 | 1 |
| Underestimate | 0.028 (−0.060, 0.117) | 0.333 (0.243, 0.423) ** | −0.063 (−0.174, 0.049) |
| Overestimate | 0.136 (−0.106, 0.379) | −0.272 (−0.518, −0.026) * | −0.259 (−0.564, 0.046) |
| Concern about their child being overweight | |||
| Unconcerned | 1 | 1 | 1 |
| Concerned | 0.207 (0.140, 0.273) ** | −0.078 (−0.145, −0.011) * | 0.129 (0.046, 0.213) ** |
| Underweight (n = 39) | |||
| Misperception of child’s weight | |||
| Correct estimate | 1 | 1 | 1 |
| Overestimate | 0.074 (−0.672, 0.819) | −0.290 (−0.767, 0.186) | 0.112 (−0.863, 1.087) |
| Concern about their child being overweight | |||
| Unconcerned | 1 | 1 | 1 |
| Concerned | −0.168 (−1.147, 0.811) | −0.415 (−1.041, 0.211) | −0.069 (−1.350, 1.212) |
| Overweight or obesity (n = 532) | |||
| Misperception of child’s weight | |||
| Correct estimate | 1 | 1 | 1 |
| Overestimate | −0.012 (−0.140, 0.116) | 0.122 (−0.022, 0.266) | −0.087 (−0.264, 0.089) |
| Concern about their child being overweight | |||
| Unconcerned | 1 | 1 | 1 |
| Concerned | 0.501 (0.316, 0.686) ** | 0.103 (−0.105, 0.311) | 0.356 (0.102, 0.611) ** |
| Restriction β (95%CI) | Pressure to Eat β (95%CI) | Monitoring β (95%CI) | |
|---|---|---|---|
| Parenting stress and competence | |||
| Parenting stress | 0.048 (0.010, 0.087) * | 0.159 (0.120, 0.198) ** | −0.026 (−0.074, 0.022) |
| Parenting competence | 0.057 (0.084, 0.105) * | 0.060 (0.010, 0.109) * | 0.253 (0.193, 0.314) ** |
| Only child status for children | |||
| Yes | 1 | 1 | 1 |
| No | 0.007 (−0.055, 0.069) | 0.108 (0.044, 0.171) ** | 0.000 (−0.078, 0.078) |
| From a one-child family | |||
| None | 1 | 1 | 1 |
| Father | −0.041 (−0.137, 0.054) | −0.071 (−0.169, 0.027) | 0.011 (−0.110, 0.106) |
| Mother | −0.109 (−0.200, −0.019) * | −0.097 (−0.190, −0.004) * | 0.108 (−0.007, 0.222) |
| Both | −0.096 (−0.171, −0.020) * | −0.058 (−0.135, 0.019) | 0.115 (0.019, 0.210) * |
| Parental family role | |||
| Mother | 1 | 1 | 1 |
| Father | 0.038 (−0.030, 0.105) | 0.222 (0.153, 0.291) ** | −0.220 (−0.305, −0.135) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, D.; Tang, Y.; Zheng, L.; Min, K.; Su, F.; Wang, J.; Liao, W.; Yan, R.; Wang, Y.; Li, X.; et al. How Parenting and Family Characteristics Predict the Use of Feeding Practices among Parents of Preschoolers: A Cross-Sectional Study in Beijing, China. Nutrients 2022, 14, 3109. https://doi.org/10.3390/nu14153109
Hu D, Tang Y, Zheng L, Min K, Su F, Wang J, Liao W, Yan R, Wang Y, Li X, et al. How Parenting and Family Characteristics Predict the Use of Feeding Practices among Parents of Preschoolers: A Cross-Sectional Study in Beijing, China. Nutrients. 2022; 14(15):3109. https://doi.org/10.3390/nu14153109
Chicago/Turabian StyleHu, Denghui, Yuxiang Tang, Lutong Zheng, Kaiyuan Min, Fenghua Su, Jing Wang, Wei Liao, Ruijie Yan, Yueqing Wang, Xiaoyan Li, and et al. 2022. "How Parenting and Family Characteristics Predict the Use of Feeding Practices among Parents of Preschoolers: A Cross-Sectional Study in Beijing, China" Nutrients 14, no. 15: 3109. https://doi.org/10.3390/nu14153109
APA StyleHu, D., Tang, Y., Zheng, L., Min, K., Su, F., Wang, J., Liao, W., Yan, R., Wang, Y., Li, X., & Zhang, J. (2022). How Parenting and Family Characteristics Predict the Use of Feeding Practices among Parents of Preschoolers: A Cross-Sectional Study in Beijing, China. Nutrients, 14(15), 3109. https://doi.org/10.3390/nu14153109