
Bacon, Brownie, or Broccoli? Beliefs about Stress-Relieving Foods and Their Relationship to Orthorexia Nervosa


Abstract
:1. Introduction
1.1. Nutritional Beliefs
1.2. Nutritional Beliefs about Comfort Foods
1.3. Comfort Foods and Stress Relief
1.4. The Role of Healthy Foods in Stress Relief
1.5. Orthorexia Nervosa and Beliefs about Stress-Relieving Foods
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Nutritional Beliefs about Stress-Relieving Foods
2.3.2. Orthorexic Tendencies
2.4. Statistical Analysis
2.4.1. Data Exclusion
2.4.2. Principal Component Analysis
2.4.3. Latent Profile Analysis
2.4.4. Multinominal Logistic Regression Analysis
3. Results
3.1. Sociodemographic Characteristics
Diet
3.2. Principal Component Analysis
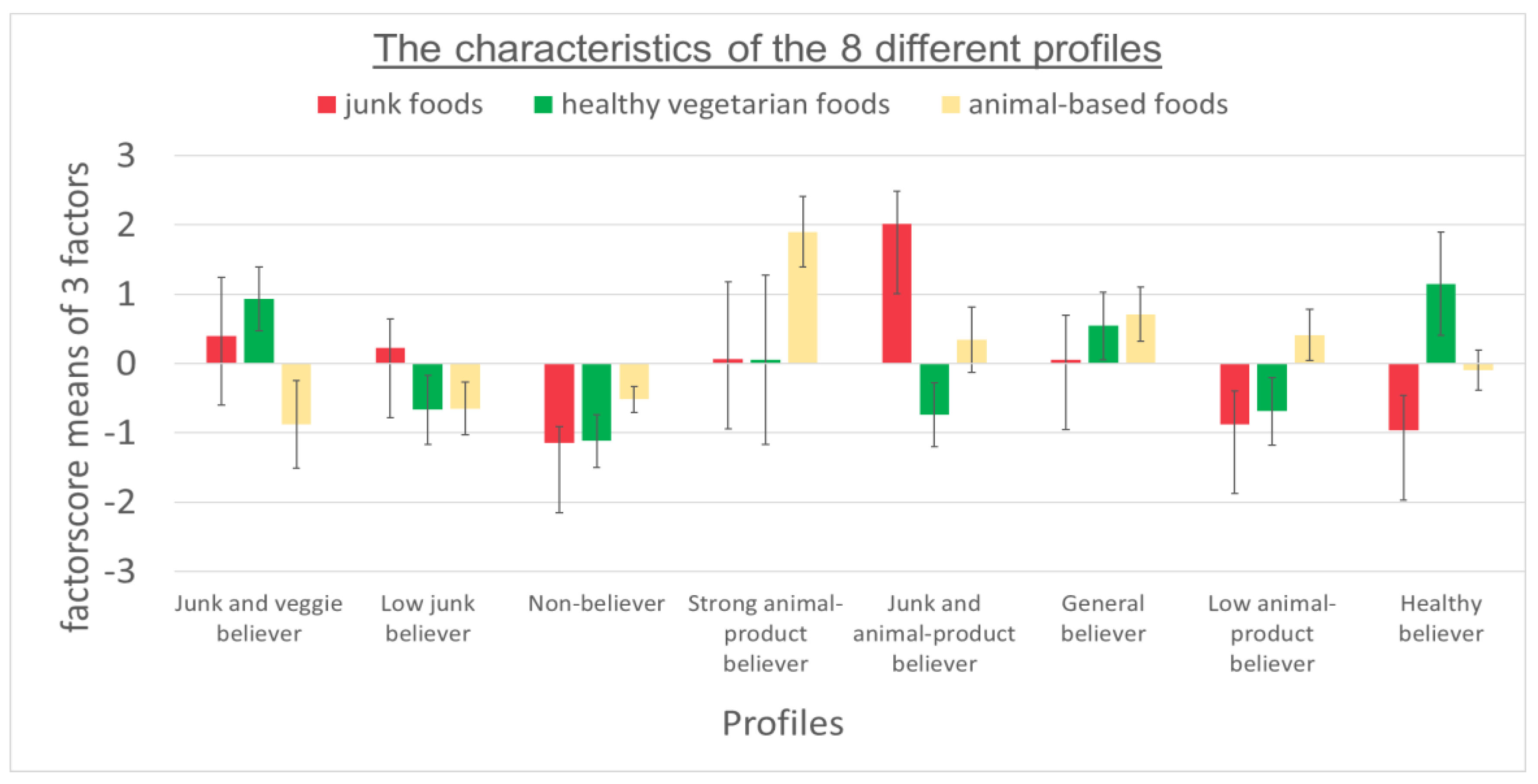
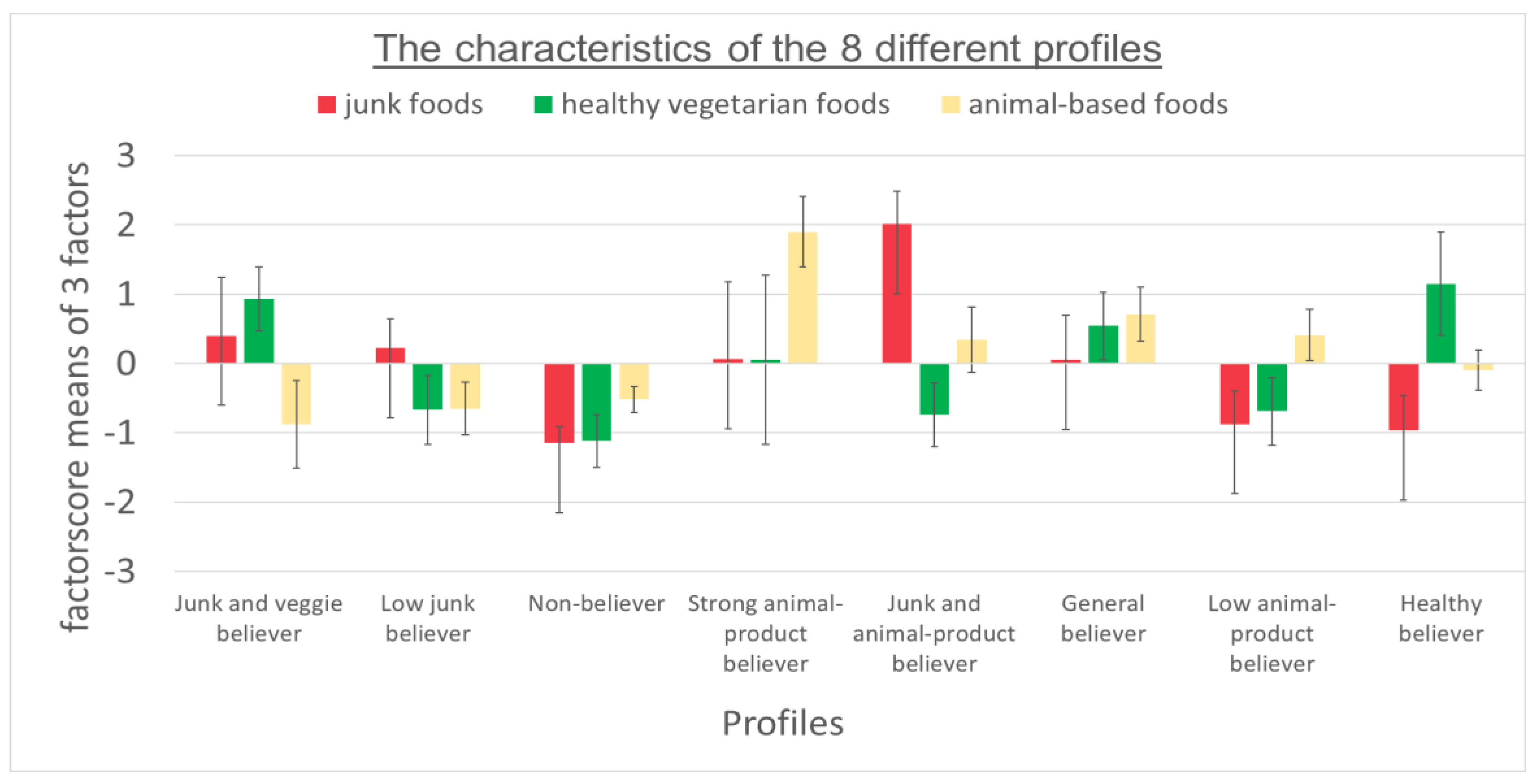
3.3. Latent Profile Analysis
3.4. Multivariate Logistic Regression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martins, Y.; Pliner, P. Human food choices: An examination of the factors underlying acceptance/rejection of novel and familiar animal and nonanimal foods. Appetite 2005, 45, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Loss, J.; Nagel, E. Social Marketing-Verführung zum gesundheitsbewussten Verhalten? Gesundheitswesen 2010, 72, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Spence, C. Comfort food: A review. Int. J. Gastron. Food Sci. 2017, 9, 105–109. [Google Scholar] [CrossRef]
- Wansink, B. Engineering Comfort Foods. Am. Demogr. 2014, 66–67. [Google Scholar] [CrossRef]
- Troisi, J.D.; Gabriel, S.; Derrick, J.L.; Geisler, A. Threatened belonging and preference for comfort food among the securely attached. Appetite 2015, 90, 58–64. [Google Scholar] [CrossRef]
- Gibson, E.L. The psychobiology of comfort eating: Implications for neuropharmacological interventions. Behav. Pharmacol. 2012, 23, 442–460. [Google Scholar] [CrossRef]
- Zellner, D.A.; Loaiza, S.; Gonzalez, Z.; Pita, J.; Morales, J.; Pecora, D.; Wolf, A. Food selection changes under stress. Physiol. Behav. 2006, 87, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Groesz, L.M.; McCoy, S. What is eating you? Stress and the Drive to Eat. Appetite 2012, 58, 717–721. [Google Scholar] [CrossRef]
- Mikolajczyk, R.T.; El Ansari, W.; Maxwell, A.E. Food consumption frequency and perceived stress and depressive symptoms among students in three European countries. Nutr. J. 2009, 8, 1–8. [Google Scholar] [CrossRef]
- Wallis, D.J.; Hetherington, M.M. Stress and eating: The effects of ego-threat and cognitive demand on food intake in restrained and emotional eaters. Appetite 2004, 43, 39–46. [Google Scholar] [CrossRef]
- Tomiyama, A.J.; Finch, L.E.; Cummings, J.R. Did that Brownie do its Job?: Stress, eating and the biobehavioral effects of Comfort food. Emerg. Trends Soc. Behav. Sci. 2015, 1, 1–15. [Google Scholar] [CrossRef]
- Conner, T.S.; Brookie, K.L.; Richardson, A.C.; Polak, M.A. On carrots and curiosity: Eating fruit and vegetables is associated with greater flourishing in daily life. Br. J. Health Psychol. 2015, 20, 413–427. [Google Scholar] [CrossRef]
- Conner, T.S.; Brookie, K.L. Let them eat fruit! The effect of fruit and vegetable consumption on psychological well-being in young adults: A randomized controlled trial. PLoS ONE 2017, 12, e0171206. [Google Scholar] [CrossRef] [PubMed]
- White, B.A.; Horwath, C.C.; Conner, T.S. Many apples a day keep the blues away--daily experiences of negative and positive affect and food consumption in young adults. Br. J. Health Psychol. 2013, 18, 782–798. [Google Scholar] [CrossRef] [PubMed]
- Franja, S.; Wahl, D.R.; Elliston, K.G.; Ferguson, S.G. Comfort eating: An observational study of affect in the hours immediately before, and after, snacking. Br. J. Health Psychol. 2021, 26, 825–838. [Google Scholar] [CrossRef]
- Liao, Y.; Schembre, S.M.; O’Connor, S.G.; Belcher, B.R.; Maher, J.P.; Dzubur, E.; Dunton, G.F. An Electronic Ecological Momentary Assessment Study to Examine the Consumption of High-Fat/High-Sugar Foods, Fruits/Vegetables, and Affective States Among Women. J. Nutr. Educ. Behav. 2018, 50, 626–631. [Google Scholar] [CrossRef]
- Horch, K.; Wirz, J. Nutzung von Gesundheitsinformationen. Bundesgesundheitsblatt Gesundh. Gesundh. 2005, 48, 1250–1255. [Google Scholar] [CrossRef]
- Finch, L.E.; Cummings, J.R.; Tomiyama, A.J. Cookie or clementine? Psychophysiological stress reactivity and recovery after eating healthy and unhealthy comfort foods. Psychoneuroendocrinology 2019, 107, 26–36. [Google Scholar] [CrossRef]
- Bratman, S. Health Food Junkies: Overcoming the Obsession with Healthful Eating, 1st ed.; Doubleday: New York, NY, USA, 2000; ISBN 0767906306. [Google Scholar]
- International Classification of Diseases Eleventh Revision (ICD-11); World Health Organization: Geneva, Switzerland, 2022.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 0-89042-555-8. [Google Scholar]
- Strahler, J.; Stark, R. Orthorexia nervosa: A behavioral condition or a new mental disorder. Suchttherapie 2019, 20, 24–34. [Google Scholar] [CrossRef]
- Ruf, A.; Koch, E.; Ebner-Priemer, U.; Knopf, M.; Reif, A.; Matura, S. Studying Microtemporal, Within-Person Processes of Diet, Physical Activity, and Related Factors Using the APPetite-Mobile-App: Feasibility, Usability, and Validation Study. J. Med. Internet. Res. 2021, 23, e25850. [Google Scholar] [CrossRef]
- Bavarian State Ministry of Food, Agriculture and Forestry. Lebensmittelkategorien. Available online: https://www.kern.bayern.de/mam/cms03/wissenschaft/dateien/lebensmittelkategorien.pdf (accessed on 2 August 2018).
- Barthels, F.; Meyer, F.; Pietrowsky, R. Duesseldorf Orthorexia Scale–Construction and Evaluation of a Questionnaire Measuring Orthorexic Eating Behavior. Klin Psych. Psychother 2015, 44, 97–105. [Google Scholar] [CrossRef]
- Meule, A.; Holzapfel, C.; Brandl, B.; Greetfeld, M.; Hessler-Kaufmann, J.B.; Skurk, T.; Quadflieg, N.; Schlegl, S.; Hauner, H.; Voderholzer, U. Measuring orthorexia nervosa: A comparison of four self-report questionnaires. Appetite 2020, 146, 104512. [Google Scholar] [CrossRef] [PubMed]
- Revelle, W. psych: Procedures for Psychological, Psychometric, and Personality Research; Northwestern University: Evanston, IL, USA, 2022; Available online: https://CRAN.R-project.org/package=psych (accessed on 20 August 2021).
- Kaiser, H.F. A second generation little jiffy. Psychometrika 1970, 35, 401–414. [Google Scholar] [CrossRef]
- Bartlett, M.S. Properties of Sufficiency and Statistical Tests. R. Soc. Publ. 1937, 160, 268–282. [Google Scholar]
- Hubert, M.; Debruyne, M. Minimum covariance determinant. WIREs Comp. Stat. 2010, 2, 36–43. [Google Scholar] [CrossRef]
- Velicer, W.F.; Eaton, C.A.; Fava, J.L. Construct Explication through Factor or Component Analysis: A Review and Evaluation of Alternative Procedures for Determining the Number of Factors or Components. In Problems and Solutions in Human Assessment; Goffin, R.D., Helmes, E., Eds.; Springer: Boston, MA, USA, 2000; pp. 41–71. ISBN 978-1-4613-6978-3. [Google Scholar]
- Rosenberg, J.M.; Beymer, P.N.; Anderson, D.J.; Van Lissa, C.J.; Schmidt, J.A. tidyLPA: An R Package to Easily Carry Out Latent Profile Analysis (LPA) Using Open-Source or Commercial Software. J. Open Source Softw. 2018, 3, 978. [Google Scholar] [CrossRef]
- Preacher, K.J.; Merkle, E.C. The problem of model selection uncertainty in structural equation modeling. Psychol. Methods 2012, 17, 1–14. [Google Scholar] [CrossRef]
- Tein, J.-Y.; Coxe, S.; Cham, H. Statistical Power to Detect the Correct Number of Classes in Latent Profile Analysis. Struct. Equ. Modeling 2013, 20, 640–657. [Google Scholar] [CrossRef]
- Spurk, D.; Hirschi, A.; Wang, M.; Valero, D.; Kauffeld, S. Latent profile analysis: A review and “how to” guide of its application within vocational behavior research. J. Vocat. Behav. 2020, 120, 103445. [Google Scholar] [CrossRef]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Modeling A Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Jung, T.; Wickrama, K. An Introduction to Latent Class Growth Analysis and Growth Mixture Modeling. Soc. Personal. Psychol. Compass 2008, 2, 302–317. [Google Scholar] [CrossRef]
- Wickrama, K.A.S.; Lee, T.K.; O’Neal, C.W.; Lorenz, F.O. Higher-Order Growth Curves and Mixture Modeling with Mplus: A Practical Guide; Routledge Taylor & Francis Group: New York, NY, USA, 2016; ISBN 9781138925151. [Google Scholar]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Newman, E.; O’Connor, D.B.; Conner, M. Daily hassles and eating behaviour: The role of cortisol reactivity status. Psychoneuroendocrinology 2007, 32, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.J.; Campbell, I.C.; Troop, N. Increases in weight during chronic stress are partially associated with a switch in food choice towards increased carbohydrate and saturated fat intake. Eur. Eat. Disord. Rev. 2014, 22, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Dubé, L.; LeBel, J.L.; Lu, J. Affect asymmetry and comfort food consumption. Physiol. Behav. 2005, 86, 559–567. [Google Scholar] [CrossRef]
- Mensink, G.B.M.; Truthmann, J.; Rabenberg, M.; Heidemann, C.; Haftenberger, M.; Schienkiewitz, A.; Richter, A. Obst- und Gemüsekonsum in Deutschland: Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1). Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 779–785. [Google Scholar] [CrossRef]
- Goldschmidt, A.B.; Wonderlich, S.A.; Crosby, R.D.; Engel, S.G.; Lavender, J.M.; Peterson, C.B.; Crow, S.J.; Cao, L.; Mitchell, J.E. Ecological momentary assessment of stressful events and negative affect in bulimia nervosa. J. Consult. Clin. Psychol. 2014, 82, 30–39. [Google Scholar] [CrossRef]
- Barthels, F.; Barrada, J.R.; Roncero, M. Orthorexia nervosa and healthy orthorexia as new eating styles. PLoS ONE 2019, 14, e0219609. [Google Scholar] [CrossRef]
- Barrada, J.R.; Roncero, M. Bidimensional structure of the orthorexia: Development and initial validation of a new instrument. An. Psicol 2018, 34, 283–291. [Google Scholar] [CrossRef]
- Depa, J.; Barrada, J.R.; Roncero, M. Are the Motives for Food Choices Different in Orthorexia Nervosa and Healthy Orthorexia? Nutrients 2019, 11, 697. [Google Scholar] [CrossRef]
- Haynos, A.F.; Wang, S.B.; LeMay-Russell, S. An empirical taxonomy of reward response patterns in a transdiagnostic eating disorder sample. Eat. Behav. 2021, 42, 101531. [Google Scholar] [CrossRef] [PubMed]
- Muthén, L.K.; Muthén, B.O. How to use a Monte Carlo study to decide on sample size and determine power. Struct. Equ. Modeling 2002, 9, 599–620. [Google Scholar] [CrossRef]
- Weller, B.E.; Bowen, N.K.; Faubert, S.J. Latent Class Analysis: A Guide to Best Practice. J. Black Psychol. 2020, 46, 287–311. [Google Scholar] [CrossRef]

{kind=link}
| Food Items Listed in the 29-Item Questionnaire | |||
|---|---|---|---|
| Bread | Butter/margarine | Cake | Cereals |
| Cheese | Couscous/bulgur/pseudocereals | Eggs | Fish |
| Fruits | Flax- or Chia seeds | Legumes | Meat |
| Meat substitute | Milk products | Nuts | Pasta |
| Potatoes | Plant-based milk/yoghurt | Ready meals | Ready sauces |
| Rice | Salad | Salty nibbles | Soups/stews |
| Sweet | Sweet spread | Vegetables | Vegetable oil |
| Vegetarian spread | |||
| Variables | N = 175 | % | |
|---|---|---|---|
| Gender | Male | 51 | 29 |
| Female | 124 | 71 | |
| Education | Mittlere Reife | 2 | 1 |
| Abitur | 71 | 40 | |
| Completed vocational training | 9 | 5 | |
| Degree of university of Applied Sciences | 5 | 3 | |
| Bachelor’s graduates | 39 | 22 | |
| Master’s graduates | 40 | 23 | |
| Ph.D. | 9 | 5 | |
| Diet | Omnivore | 142 | 81 |
| Pescetarian | 9 | 5 | |
| Vegetarian | 19 | 11 | |
| Vegan | 5 | 3 | |
| Body weight change | Yes, I am trying to reduce my body weight | 84 | 48 |
| No | 85 | 49 | |
| Yes, I am trying to gain body weight | 6 | 3 | |
| Age | Male | M = 29.7 (SD = 8.1) | |
| Female | M = 28.1 (SD = 7.7) | ||
| BMI | Male | M = 26.31 (SD = 3.96) | |
| Female | M = 23.60 (SD = 3.68) | ||
| Profiles | LogLik | AIC | BIC | SABIC | Entropy | BLRT_p |
|---|---|---|---|---|---|---|
| 3 | −692.284 | 1442.569 | 1534.348 | 1442.514 | 0.865402 | 0.039604 |
| 4 | −680.86 | 1439.721 | 1563.147 | 1439.646 | 0.779699 | 0.158416 |
| 5 | −674.253 | 1446.506 | 1601.58 | 1446.412 | 0.793919 | 0.90099 |
| 6 | −649.797 | 1417.594 | 1604.316 | 1417.482 | 0.868484 | 0.079208 |
| 7 | −659.24 | 1456.481 | 1674.851 | 1456.349 | 0.880146 | 0.742574 |
| 8 | −630.626 | 1419.253 | 1669.271 | 1419.102 | 0.918113 | 0.009901 |
| Profiles | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Six-profile solution | 28 | 31 | 28 | 33 | 5 | 50 | ||
| Eight-profile solution | 33 | 34 | 13 | 10 | 20 | 19 | 23 | 14 |
| Size (n) | Sex (m/f) | % of Total (m/f) | Age | BMI | DOS | |
|---|---|---|---|---|---|---|
| “Junk and veggie believer” | 37 | 5/32 | 9.8/25.8 | 27.84 ± 7.41 | 23.3 ± 3.58 | 19.41 ± 5.68 |
| “Low junk believer” | 39 | 9/30 | 17.6/24.2 | 28.59 ± 7.12 | 24.2 ± 3.36 | 17.51 ± 4.70 |
| “Non-believer” | 13 | 3/10 | 5.9/8 | 29.07 ± 8.1 | 24.4 ± 3.62 | 15.08 ± 3.04 |
| “Strong animal-product believer” | 20 | 8/12 | 15.6/9.7 | 27.25 ± 7.76 | 25.0 ± 3.7 | 17.40 ± 4.32 |
| “Junk and animal-product believer” | 10 | 1/9 | 1.9/7.3 | 26.4 ± 6.43 | 23.9 ± 3.52 | 18.30 ± 6.11 |
| “General believer” | 19 | 8/11 | 15.7/8.9 | 32.16 ± 9.56 | 26.7 ± 5.5 | 17.68 ± 4.04 |
| “Low animal-product believer” | 23 | 14/9 | 27.5/7.3 | 26.43 ± 6.56 | 23.6 ± 3.12 | 15.48 ± 6.11 |
| “Healthy believer” | 14 | 3/11 | 5.9/8.9 | 32.07 ± 9.7 | 24.9 ± 5.23 | 20.64 ± 4.91 |
| DOS Total Score | |||
|---|---|---|---|
| B (SE) | OR | 95% CI | |
| Non-believer vs. | |||
| Junk and veggie believer | 0.21 (0.09) * | 1.24 | 1.05; 1.46 |
| Low junk believer | 0.14 (0.85) | 1.15 | 0.97; 1.36 |
| Strong animal-product believer | 0.14 (0.09) | 1.15 | 0.96; 1.37 |
| Junk and animal-product believer | 0.17 (0.1) | 1.19 | 0.98; 1.45 |
| General believer | 0.15 (0.09) | 1.16 | 0.97; 1.39 |
| Low animal-product believer | 0.03 (0.09) | 1.03 | 0.86; 1.24 |
| Healthy believer | 0.25 (0.09) * | 1.28 | 1.07; 1.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinmann, A.; Ruf, A.; Ahrens, K.F.; Reif, A.; Matura, S. Bacon, Brownie, or Broccoli? Beliefs about Stress-Relieving Foods and Their Relationship to Orthorexia Nervosa. Nutrients 2022, 14, 3673. https://doi.org/10.3390/nu14183673
Steinmann A, Ruf A, Ahrens KF, Reif A, Matura S. Bacon, Brownie, or Broccoli? Beliefs about Stress-Relieving Foods and Their Relationship to Orthorexia Nervosa. Nutrients. 2022; 14(18):3673. https://doi.org/10.3390/nu14183673
Chicago/Turabian StyleSteinmann, Annebirth, Alea Ruf, Kira F. Ahrens, Andreas Reif, and Silke Matura. 2022. "Bacon, Brownie, or Broccoli? Beliefs about Stress-Relieving Foods and Their Relationship to Orthorexia Nervosa" Nutrients 14, no. 18: 3673. https://doi.org/10.3390/nu14183673
APA StyleSteinmann, A., Ruf, A., Ahrens, K. F., Reif, A., & Matura, S. (2022). Bacon, Brownie, or Broccoli? Beliefs about Stress-Relieving Foods and Their Relationship to Orthorexia Nervosa. Nutrients, 14(18), 3673. https://doi.org/10.3390/nu14183673