Abstract
Vitamin B12 deficiency, mostly of maternal origin in newborns, is a well-treatable condition but can cause severe neurologic sequelae in infants. Early detection of vitamin B12 deficiency allows the pre-symptomatic treatment of affected children. This evaluation assesses the characteristics of maternal vitamin B12 deficiency detected by newborn screening. In a prospective single-center study, a systematic screening strategy for vitamin B12 deficiency using a combination of two second-tier strategies was applied. In addition to confirmatory diagnostics in children, the systematic work-up of vitamin B12 status was also performed for their mothers. Maternal characteristics were assessed including ethnic origin, diet, and vitamin supplementation during pregnancy. For affected mothers, a work-up by internal medicine was recommended. In total, 121 mother–infant couples were analyzed. 66% of mothers adhered to a balanced diet including meat. The cause of maternal vitamin B12 deficiency was unknown in 56% of cases, followed by dietary causes in 32%, and organic causes in 8%. All mothers following a vegan diet and most mothers with a vegetarian diet took vitamin preparations during pregnancy, whereas only 55.8% of mothers with a balanced diet took folic acid or other vitamins. Maternal vitamin B12, folic acid, and homocysteine levels were significantly correlated with the child’s folic acid levels, and with homocysteine, methylmalonic, and methylcitric acid levels in first and second NBS dried blood spots. Most children had normal blood counts and showed normocytosis. Although 36.7% of mothers showed anemia, only one presented with macrocytosis. Adherence to vitamin supplementation in pregnancy is low despite the recommendation for supplementation of folic acid. Ideally, the evaluation of mothers for vitamin B12 levels and appropriate therapy should be initiated in early pregnancy. In infants detected through newborn screening, the multidisciplinary assessment and therapy of both children and mothers should be performed.
1. Introduction
1.1. Uptake and Function of Vitamin B12
Vitamin B12 (cobalamin) is a water-soluble vitamin that is synthesized by microorganisms. Major sources of dietary vitamin B12 are foods of animal origin, including meat, milk, eggs, and fish, with plants and fungi contributing little vitamin B12 to the human diet [1]. The human body is not able to produce vitamin B12 and is therefore dependent on external supply [2]. After dietary intake, vitamin B12 underlies a complex pathway of intestinal absorption and intracellular processing. Uptake in the gastrointestinal tract depends on an intrinsic factor, which is synthesized by the gastric parietal cells, and on the cubulin-amnionless (cubam) receptor in the distal ileum [1,2,3,4]. In blood, vitamin B12 is bound to transcobalamin or haptocorrin, whereby only transcobalamin-bound vitamin B12 (holoTC) is active and available for uptake by CD320, the B12 receptor expressed on most cells [1]. Cobalamin functions as a cofactor for two enzymes in human metabolism: methionine synthase and methylmalonyl–coenzyme A mutase [2]. Metabolic changes due to vitamin B12 deficiency result from the dysfunction of these enzymes, leading to an increase in the functional parameters homocysteine (Hcy), methylmalonic acid (MMA), and potentially methylcitric acid (MCA) [2,3]. Vitamin B12 plays an essential role in all human cells and many organ systems, especially in tissues with a high cell turnover [2]. Along with folic acid, vitamin B12 is necessary for the synthesis of deoxyribonucleic acid (DNA) and ribonucleic acid (RNA), lipids, and protein, which are essential for the development, myelination, and normal function of the central and peripheral nervous system. Furthermore, it is required for effective erythropoiesis [2].
1.2. Causes and Symptoms of Vitamin B12 Deficiency
Inadequate intake, inadequate bioavailability, or malabsorption are reasons for vitamin B12 deficiency [5]. The most common cause in adults with a prevalence of 50 to 4000 cases per 100,000 persons is a loss of intrinsic factor due to autoimmune atrophic gastritis (pernicious anemia) [2,4]. Between 2.5% and 26% of the general population is affected by vitamin B12 deficiency [5,6,7], with a wide spectrum of disease, from asymptomatic to life-threatening pancytopenia or myelopathy [2]. In women of child-bearing age and pregnant women, vitamin B12 deficiency is prevalent with frequencies between 10% and 50% across the world, with especially high rates in studies from the Indian subcontinent, Eastern Mediterranean, and South American regions [2,8,9,10,11,12,13,14]. During pregnancy, low circulating levels of vitamin B12 or folic acid have been associated with complications such as neural tube defects, spontaneous abortion, premature birth, and possibly low birth weight [8,15]. Vitamin B12 deficiency in newborns is usually of unrecognized maternal origin [11]. Cobalamin status in the neonate depends on maternal cobalamin status during pregnancy, placental function, and gestational age at birth [16]. Newborns affected by vitamin B12 deficiency are usually asymptomatic at birth [2,10]. Clinical signs of vitamin B12 deficiency appear mostly at the age of 4–6 months [2,11]. Symptoms include developmental delay, muscular hypotonia, irritability, regression, feeding difficulties, and failure to thrive, as well as tremors and seizures [2,11]. Hematologic abnormalities with anemia may be present [2,11]. Untreated vitamin B12 deficiency can lead to coma or even death [11]. Because of the late onset of often non-specific symptoms, the diagnosis is often not established until the second half of the first year of life [11,17,18,19]. Many children with symptomatic vitamin B12 deficiency show improvement in clinical symptoms after supplementation with vitamin B12 [11,17,18,19]. However, long-term neurological and intellectual outcomes following severe and especially long-term vitamin B12 deficiency are poor with permanent deficits [11,17,18,19].
1.3. Early Detection through Newborn Screening for Vitamin B12 Deficiency
Children with vitamin B12 deficiency are asymptomatic at birth but may develop severe multisystemic symptoms. As vitamin B12 deficiency is a well-treatable condition if identified early, it is a potential target for newborn screening (NBS) [11]. The prevalence of vitamin B12 deficiency detected by NBS varies between countries, also depending on the NBS strategies applied. The NBS for vitamin B12 deficiency has been shown to be feasible under the application of second-tier strategies with a prevalence between 1 in 30,000 [20] and 1 in 5300 detected newborns in Germany [21,22]. An Italian study found a prevalence of 1 per 5000 in a cohort of 35,000 newborns [12]. The screening program in Estonia reported an incidence of vitamin B12 deficiency of 1 in 2500 newborns detected by elevated propionylcarnitine (C3) as an incidental finding in the NBS for methylmalonic and propionic acidemias [23]. The NBS program in the US state of Minnesota reported a detection rate of vitamin B12 deficiency in 1 in 33,000 newborns [24].
2. Material and Methods
2.1. Study Population and Study Design
The study population included 121 pairs of newborns and their mothers. In total, 120 patients were identified in the pilot project Newborn Screening 2020 (NBS 2020/NBS 2025; DRKS-ID DRKS00025324) at the Dietmar Hopp Metabolic Center, Heidelberg University Hospital, between 1 August 2016, and 31 December 2020, with a diagnosis of vitamin B12 deficiency or maternal vitamin B12 deficiency. One infant born in January 2021 was additionally included because an older sibling had already been diagnosed with vitamin B12 deficiency as part of the pilot project.
NBS 2020/NBS 2025 is a prospective single-center study evaluating an extension of the German NBS panel (14 disorders at study initiation, currently 19 target disorders) by an additional 28 conditions [25]. Details on the screening algorithms of NBS for vitamin B12 deficiency developed for this study using a combination of two second-tier strategies have been previously published [22]. Primary screening measures used in the second-tier algorithms were C3, ratio C3/acetyl carnitine (C3/C2), methionine (Met), and the ratio of methionine/phenylalanine (Met/Phe). One second-tier strategy analyzed MMA, 3-OH-propionic acid (3-OH-PA), and MCA [26] based on abnormal first-tier results for C3 and C3/C2 (C3 + C3/C2 > cut-off, or C3/C2 > cutoff, or C3 > alarm limit). The second method analyzed total homocysteine (tHcy) [27] after an abnormal first-tier result for Met (<cut-off low) or Met/Phe (<cut-off low or > cut-off high). Patients with vitamin B12 deficiency could be reliably identified by elevated tHcy, elevated MMA/MCA, or a combination of both. A diagnosis of “vitamin B12 deficiency” was established in cases with elevation of 1 or more functional markers of vitamin B12 deficiency (MMA in plasma and/or urine and homocysteine in plasma), in the presence of low vitamin B12 serum levels, and of “functional vitamin B12 deficiency” in cases with elevation of 1 or more functional markers of vitamin B12 deficiency and vitamin B12 in the low normal range [28]. Normalization of functional markers and of vitamin B12 serum levels under supplementation had to be documented for final confirmation of the diagnosis in the child.
The study NBS 2020 has been approved by the ethics committee of the University Hospital Heidelberg (Number S-533/2015). Written informed consent was obtained from a legal guardian before participation in the study.
2.2. Data Collection
Data on the NBS results including second-tier markers as well as confirmatory diagnostics including vitamin B12 status and functional markers were collected at the NBS center and metabolic laboratory at Heidelberg University. Data on gestational age, birth weight, and congenital heart defects were obtained from the submission forms, the physicians’ letters, or subsequently by contacting the attending pediatricians. In all cases, a work-up of the maternal vitamin B12 status, including functional markers, was recommended, and a laboratory work-up was offered at Heidelberg University Hospital metabolic laboratory in cooperation with the central laboratory in the context of the newborns’ confirmatory diagnostics. In cases with confirmatory diagnostics in the child and/or mother performed in external laboratories, data were retrieved from the transmitted reports. “Maternal vitamin B12 deficiency” was diagnosed if the mother’s vitamin B12 level was below the normal range and/or functional markers were elevated. A further diagnostic work-up was recommended to mothers with vitamin B12 deficiency not clearly explained by dietary reasons and was offered and performed in collaboration with the department of Internal Medicine at the Heidelberg University Hospital. If this work-up was performed at an external hospital, data were retrieved from the submitted reports. Information on mothers’ ethnic origin, diet during pregnancy, vitamin supplementation, cause of vitamin B12 deficiency, or subsequent pregnancies was obtained at contact with the family during the work-up of the child or mother or by contacting the mothers or attending pediatricians of the affected newborns. The mothers’ ethnic origin was classified according to topographical criteria as defined by the United Nations Group of Experts on Geographical Names [29].
2.3. Study Objective
The primary objective of this analysis was to evaluate causes and characteristics of maternal vitamin B12 deficiency detected by abnormal newborn screening of the child and influences on maternal vitamin B12 status. Secondary endpoints were the correlation of maternal and infant vitamin B12 status and blood counts. Data were also collected on gestational age, birth weight, and congenital heart defects. Furthermore, as part of confirmatory diagnostics concerning vitamin B12 deficiency, the initial treatment response of the newborns with vitamin B12 deficiency was assessed.
2.4. Statistical Analysis
A statistical analysis was performed using IBM SPSS® 28.0. For continuous variables, the mean, median, standard deviation, and interquartile range were calculated. For categorical variables, the absolute and relative numbers were calculated. Correlations of categorical variables were analyzed by cross-tabulations, and statistical significance was determined by a chi-square test with a p-value < 0.05. Statistical significance for interval scaled variables was evaluated with a linear regression analysis or multiple linear regression analysis with a p-value < 0.05. Statistical significance for dichotomous variables was determined with a logistic regression analysis with a p-value < 0.05. Missing data which could not be retrieved and implausible data that could not be verified were treated as cases that were missing for the respective analysis.
3. Results
3.1. Maternal and Child Characteristics
In total, 121 mother–infant couples were analyzed. Furthermore, 66% of mothers adhered to a balanced diet including meat, followed by rarely meat in 17% of cases, and a vegetarian diet in 9% of cases. 63.3% of mothers took vitamin preparations during pregnancy, and 16 mothers reported feeding disorders. The assumed cause of maternal vitamin B12 deficiency was unknown in 56% of cases, followed by dietary causes in 32%, and organic causes in 8%. 43.6% of the mothers had a Central European origin, 30.7% of the mothers were of West Asian origin, and 9.9% were of Southeast European origin.
Infants were born with a mean birth weight of 3138 g ± 583 SD (range 1100–4850 g) at a mean gestational age of 38 weeks ± 2 SD (range 29–42 weeks). In addition, 62.2% of newborns were breastfed, followed by 19.8% who were breastfed and formula-fed, and 16.2% who were formula-fed only. 6.5% of newborns had a congenital heart defect.
Maternal and child characteristics are displayed in Tables S1 and S2 in the Supplementary Materials section.
3.2. Maternal Diagnoses
Maternal causes for vitamin B12 deficiency were divided into four diagnostic categories: nutritional, organic, nutritional and organic, and unknown cause. In 11 mothers, a comprehensive evaluation was performed in cooperation with physicians from the Department of Internal Medicine at Heidelberg University Hospital. In two cases, the diagnosis of autoimmune gastritis and pernicious anemia with antibodies against parietal cells could be confirmed. Gastritis was suspected in five additional cases, but esophagogastroduodenoscopy was pending at the time of data collection. In three mothers, gastrointestinal malabsorption could be ruled out or diet was identified as the cause of vitamin B12 deficiency. Additional diagnoses in the mothers, whose diagnostics were performed internally or externally, included ulcerative colitis, gastric bypass, HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome, gestational diabetes, severe pancytopenia due to vitamin B12 and folic acid deficiency, and carbamazepine treatment during pregnancy. Maternal diagnoses according to the above-named diagnostic categories and vitamin supplementation during pregnancy were not significantly related. Diagnoses and affected subsequent pregnancies were also not significantly correlated. Three out of three mothers (100%) on a vegan diet whose vitamin intake data are known took vitamins during pregnancy. For vegetarian mothers, the percentage was 80% (4 out of 5 mothers). Among mothers who had a balanced diet, 55.8% (24 out of 43 mothers) took vitamins during pregnancy. No significant correlation was found between diet and vitamin intake or type of vitamin supplementation during pregnancy. Similarly, no significant effect was found between diet and iron supplementation. Diet during pregnancy and ethnicity showed no significant correlation. Forty-one mothers were of German origin, and sixty mothers (49.6%) had a migration background. Among two German mothers with a subsequent pregnancy, the siblings were not affected by vitamin B12 deficiency. Among the mothers with a migration background, 62.5% (n = 5) were not affected, 25% (n = 2) subsequent pregnancies suffered again from vitamin B12 deficiency, and n = 1 remained unknown. Migration background and affected subsequent pregnancies were not significantly correlated.
3.3. Maternal Vitamin B12 Status
Maternal vitamin B12 status was assessed at a mean of 4.5 weeks ± 3.5 SD (range 0–20 weeks) postpartum. Laboratory results are depicted in Table 1. In all, 41.1% (n = 44) of mothers had serum vitamin B12 levels below the normal range (160–679 pmol/L), with the lowest level being 36 pmol/L.

Table 1.
Maternal vitamin B12 status.
The influence of diet, cause of maternal vitamin B12 deficiency, vitamin supplementation during pregnancy, and ethnic origin on maternal vitamin B12 status were analyzed. Neither diet during pregnancy, nor diagnoses, nor vitamin supplementation, nor maternal ethnic origin had a significant effect on serum vitamin B12 levels. In addition, no effect on the homocysteine level in plasma could be shown. However, a multiple regression analysis showed that diet, diagnoses, vitamin supplementation, and ethnic origin had an influence on folic acid levels (p = 0.038). Mothers with an ethnic origin from West Asia had lower serum folic acid levels by 11.35 units compared to the origin from Middle Europe (p = 0.019). There was also an effect on methylmalonic acid levels (conventional method) in urine (p = 0.002). Mothers with organic causes of vitamin B12 deficiency showed higher values by 12.89 units compared to those with an unknown diagnosis (p = 0.009). When considering children’s nutrition and maternal vitamin B12 status, an association could be shown with folic acid levels (p = 0.048). Mothers whose children were fed by formula or parenteral nutrition showed higher folic acid levels by 25.96 units than mothers whose children were breastfed (p = 0.044).
3.4. Blood Counts of Mothers and Children
The hemoglobin level and mean corpuscular volume were obtained from mothers and children. The hemoglobin value was classified as normal, anemia, or polyglobuly, and the mean corpuscular volume (MCV) was classified as normo-, micro-, or macrocystosis. The results are depicted in Table 2.
Table 2.
Blood counts of mothers and children.
Most children had normal blood counts and normocytosis. Although 36.7% of mothers showed anemia, only one had a blood count with macrocytosis. Diagnosis, diet during pregnancy, and vitamin supplementation were not significantly related to maternal hemoglobin or MCV. However, there was a significant correlation between the type of vitamin intake and hemoglobin (p = 0.026), but not with MCV. Mothers who supplemented folic acid during pregnancy were significantly more likely to have normal hemoglobin levels. Iron supplementation had no correlation with the classification of hemoglobin and MCV. A logistic regression analysis showed no effect of maternal vitamin B12 status on blood counts. The blood count characteristics of mothers and children were not significantly correlated.
3.5. Neonatal Vitamin B12 Status
The results of newborns’ vitamin B12 status are depicted in Table 3.
Table 3.
Newborns’ vitamin B12 status.
3.6. Effect of Maternal Vitamin B12 Status on Infant Metabolism
The effect of maternal vitamin B12 status was analyzed separately on the child’s vitamin B12 status for confirmatory diagnostics and screening data.
Maternal vitamin B12, folic acid, and homocysteine levels did not show a significant effect on infant vitamin B12 levels, neither in the combined, nor in the separate analysis. Maternal MMA and MMA-I levels in plasma and urine also did not have a significant correlation with newborns’ vitamin B12 levels. The significant correlations of maternal vitamin B12 status on infant metabolism in confirmatory diagnostics are depicted in Table 4.
Table 4.
Effect of maternal vitamin B12 status on infant metabolism.
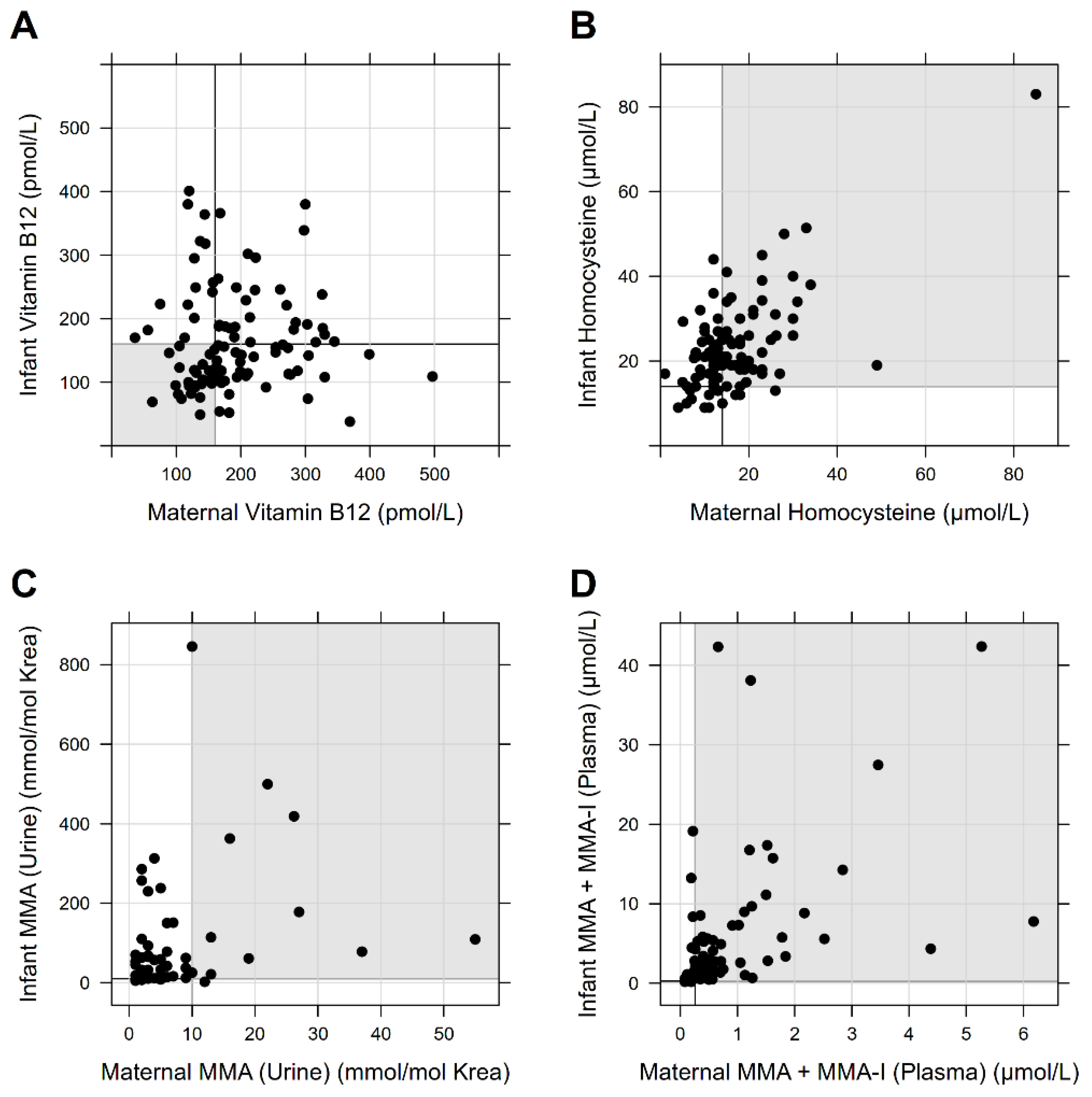
Figure 1 shows the relation of maternal and infant vitamin B12 status based on vitamin B12 levels and functional parameters.
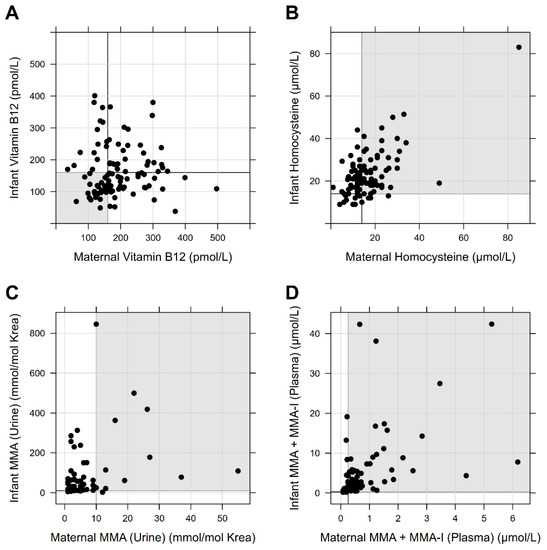
Figure 1.
Relation of maternal and infant vitamin B12 status. (A–D) illustrates the correlation of the maternal and infant vitamin B12 status based on the vitamin B12 levels and the functional parameters Hcy, MMA in urine, and MMA or MMA-I in plasma as a point cloud. Bold lines mark the cut-off of the normal range. Individuals in the gray marked area showed values outside the normal range for both mother and child.
For NBS data, only the results of second-tier analyses (tHcy, MMA, MCA) were considered. Maternal vitamin B12, folic acid, and homocysteine levels showed an impact on the infant homocysteine level in the first NBS sample (p < 0.001). The significant correlations of maternal vitamin B12 status on the results of the first DBS are depicted in Table 4.
Considering the results of the second-tier analyses in the second DBS, the maternal vitamin B12 level showed no effect on tHcy and MCA but on MMA. As in the first DBS, the combined analysis of maternal vitamin B12, folic acid, and Hcy also showed a significant effect (p < 0.001) on infant tHcy, MMA, and MCA levels from the second DBS. The results are depicted in Table 4.
3.7. Effect of Neonatal Nutrition on Newborns’ Vitamin B12 Status
The mean value of the serum vitamin B12 level at confirmatory diagnostics in exclusively breastfed children was 129 pmol/L with a range of 38 to 249 pmol/L. In children who were not exclusively breastfed but received formula or parenteral nutrition, the mean value was 217 pmol/L with a range of 94 to 401 pmol/L. Neonatal nutrition showed a significant impact on newborns’ vitamin B12 status in confirmatory diagnostics but not on the screening data. Neonates who were partially formula fed, formula fed alone, or received a combination of parenteral and formula feeding showed higher serum vitamin B12 concentrations than fully breastfed neonates (p < 0.001). Infants who were formula fed had significantly lower homocysteine concentrations than newborns who were fully breastfed (p = 0.009). There was no significant effect of neonatal nutrition on MMA levels.
3.8. Gestational Age, Birth Weight, and Congenital Heart Defects
Maternal vitamin B12, Hcy, and MMA levels did not show a correlation with gestational age and birth weight. There was a significant correlation between infants’ vitamin B12 levels and gestational age, but not for Hcy and MMA levels. The univariate regression analysis for newborns’ vitamin B12 levels showed an inverse effect, the decrease in gestational age in weeks by 0.006 showed an increase of vitamin B12 levels by one unit (p = 0.012). There was no significant correlation for children’s vitamin B12, Hcy, and MMA levels and infants’ birth weight. Three children in this cohort suffered from a congenital heart defect. One child had a ventricular septal defect (VSD), one child suffered from a patent foramen ovale (PFO), and one child had a PFO and a patent ductus arteriosus (PDA). The child with the PDA was born at 29 weeks of gestation.
3.9. Infants’ Response to Therapy
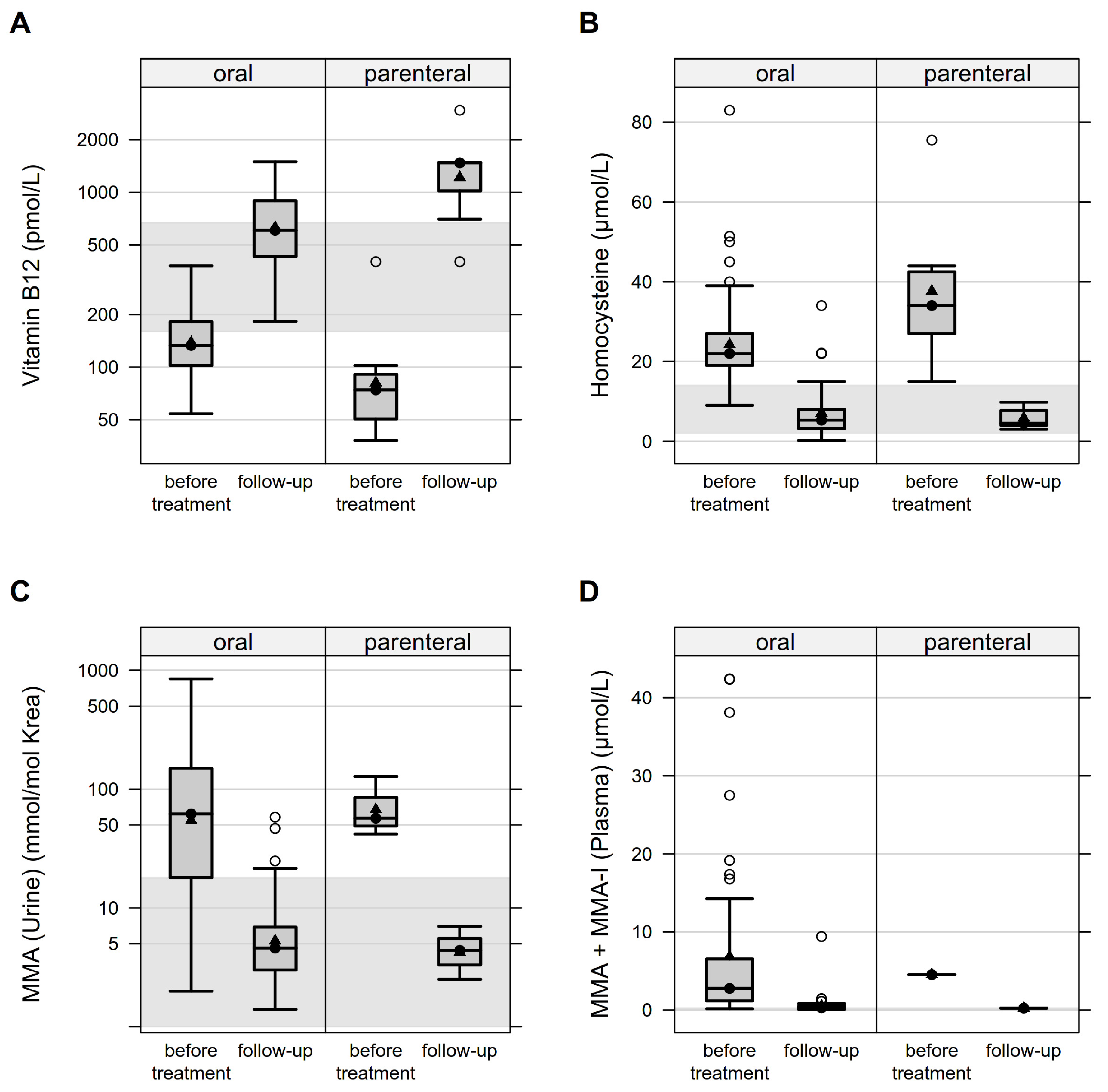
The confirmation of vitamin B12 deficiency requires the evaluation of the initial response to treatment. One hundred and ten infants received treatment with vitamin B12. In six cases in which only the mother was affected by vitamin B12 deficiency, no therapy was performed for the child. Four of those children received formula feeding exclusively, one child was breast and formula fed, and one child received parenteral and formula feeding. In the remaining 5 children with vitamin B12 deficiency who did not receive therapy, 4 children were fed only by formula and 1 child was breastfed and formula fed. Of the 108 newborns whose supplementation scheme was known, 99 (91.7%) received oral, n = 2 (1.9%) intramuscular, n = 5 (4.6%) a combination of oral and intramuscular, n = 1 (0.9%) intravenous, and n = 1 (0.9%) a combination of intravenous and oral therapy. Treatment was started at a mean age of 4 weeks (SD = 3.1) and first follow-up samples were analyzed at a mean age of 7 weeks (SD = 3.6). Comparisons with oral-only versus also parenteral therapy showed mean percent increases in vitamin B12 levels of 78% and 1254%, respectively, with parenteral therapy resulting in vitamin B12 concentrations well above the normal range with a mean of 1422 pmol/L (SD = 807.5) at follow-up. Homocysteine levels showed a mean percent decrease of 70% with oral-only versus 80% with parenteral therapy. Plasma or urine MMA concentrations (conventional method and isotopes) showed mean percentage decreases of 90–92% with oral-only and 92–96% with parenteral treatment. Figure 2 illustrates the therapeutic response of purely oral versus also parenteral supplementation based on the increase in vitamin B12 levels and decrease in functional parameters.
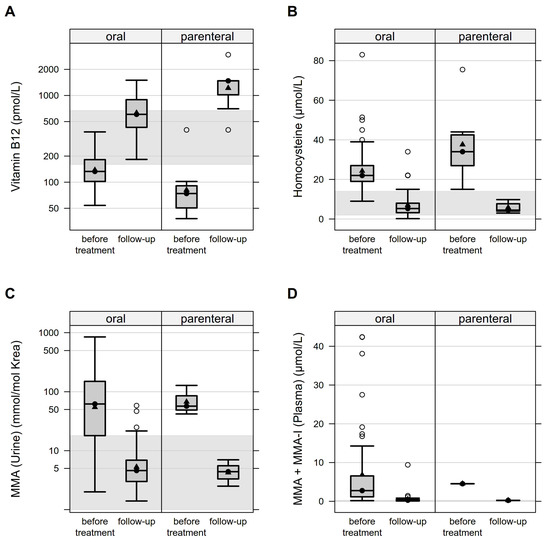
Figure 2.
Therapeutic response of vitamin B12 supplementation: oral versus parenteral administration. Figure 2 (A–D) represents the infants’ response to therapy with oral versus also parenteral vitamin supplementation as a boxplot. The gray marked area represents the normal value range. There is an increase in the vitamin B12 level and a decrease in the functional parameters Hcy, MMA in urine, and MMA or MMA-I in plasma.
4. Discussion
A diagnostic work-up of vitamin B12 deficiency in newborns should always include a comprehensive analysis of the maternal vitamin B12 status and diet, as vitamin B12 deficiency in children of this age group is mostly of maternal origin. Here, we report the results of the confirmatory work-up in mothers of 121 children with vitamin B12 deficiency detected by an NBS pilot study.
4.1. Maternal Diet and Causes of Vitamin B12 Deficiency
In this study, about two-thirds of mothers with vitamin B12 deficiency reported a balanced diet including meat. A vegan or vegetarian diet, as described frequently in other screening programs [22,30,31], was rarely reported in this cohort. Recommendations from the German Federal Center for Nutrition include a balanced diet and the initiation of folate supplementation before pregnancy for all women [22,32]. For women who follow a vegetarian or vegan diet, the initiation of micronutrient supplementation before pregnancy, including vitamin B12, and monitoring throughout pregnancy is recommended [22,32]. Despite a general recommendation for folic acid supplementation in Germany [32], only 63% of women in our cohort had taken any vitamin supplementation during pregnancy. This low compliance with the recommendations on prenatal folic acid supplementation is consistent with previous national surveys in Germany [11,33]. In other countries, adherence to prenatal B-vitamin supplementation is much higher, e.g., 93% in a Canadian study [11,34]. Some mothers reported feeding difficulties in pregnancy, iron supplementation due to anemia, or use of carbamazepine during pregnancy. Despite these risk factors [35] or symptoms, no diagnostic work-up for vitamin B12 deficiency had been performed during pregnancy. This emphasizes that caregivers of pregnant women should pay increased attention to vitamin B12 deficiency. In women with anemia, the coexistence of iron, folate, and vitamin B12 deficiency has been reported [22,36]. Hematologic changes caused by vitamin B12 deficiency may be masked by concomitant iron deficiency [22,36]. This is also reflected in the blood counts of the mothers in this cohort, who mostly showed normocytic or microcytic anemia. Therefore, the isolated evaluation of blood counts in pregnancy is not sufficient to differentiate maternal vitamin B12 deficiency from other nutritional deficiencies. Even in the presence of iron deficiency, vitamin B12 should be determined in anemic women. National German maternity guidelines do currently not include the routine evaluation of vitamin B12 status [22,32]. As women with gastrointestinal malabsorption would not benefit from a general recommendation for vitamin B12 supplementation in pregnancy and are often clinically asymptomatic, an ideal prevention strategy would include the routine testing of vitamin B12 status in early pregnancy [11,30]. Vitamin B12 deficiency can also be associated with HELLP syndrome [37] or gestational diabetes [38], which were also present in our cohort and again have implications for the fetus.
In the majority of mothers from our cohort, no gastrointestinal cause for vitamin B12 deficiency was found. Most mothers in this cohort had an unknown reason for vitamin B12 deficiency followed by dietary causes. Although further diagnostics were recommended for all mothers without a clear nutritional cause of vitamin B12 deficiency, a thorough etiological work-up by internal medicine was only performed in a minority of cases. This work-up was able to clarify the reasons in 90% of cases. This emphasizes the advantages of a structured work-up in parallel to confirmatory diagnostics in the child in cooperation with internal medicine in maternal vitamin B12 deficiency detected by NBS. Mothers in our study were of various ethnic origins, and 50% had a migration background. This is an overrepresentation of women with a migration background compared to the general population in Germany of about 27% [29]. The lack of vitamin supplementation during pregnancy may particularly affect women with a migration background due to a lack of information, language barriers, or greater hesitation to attend preventive prenatal care appointments [11,22,39]. However, in this cohort, ethnicity showed no significant association with diet, vitamin supplementation, or subsequent affected pregnancies. Nevertheless, it must be taken into account that, in contrast to other evaluations [21], ethnic background was considered in the analysis, but not language skills or school education which might also play a role.
In two cases, subsequent pregnancies were again affected by vitamin B12 deficiency despite the diagnosis being previously established in the older sibling and mother. Considering the high rate of unknown maternal causes as mentioned above and the fact that there has been only little systematic etiologic evaluation by internal medicine apart from the cooperation with the Department of Internal Medicine at the Heidelberg study site, a collaborative evaluation program for affected children with vitamin B12 deficiency and their mothers is recommended for an optimal prevention strategy.
4.2. Maternal and Infants’ Vitamin B12 Status
A meta-analysis showed that rates of vitamin B12 insufficiency are especially high in certain populations, e.g., the Indian subcontinent and Eastern Mediterranean [13]. In our cohort, however, there was no effect of ethnic background on maternal vitamin B12 status, but rather on folic acid levels. As the cause of vitamin B12 deficiency, diet during pregnancy, and vitamin supplementation did not correlate with migration background, the cause of this effect remains unclear. More than half of the mothers had a normal vitamin B12 status at confirmatory evaluation, and maternal vitamin B12 status showed no significant correlation with infant vitamin B12 status. This could be explained by the fact that laboratory values of mothers were taken on average 5 weeks postpartum. In a study from Norway, maternal vitamin B12 levels were shown to increase again about 6 weeks after birth [16]. The postpartum increase in maternal serum cobalamin may be a physiologic adaptation to enhance the cobalamin transfer to the infant by increasing the cobalamin concentration in breast milk [16]. Maternal vitamin B12 concentration at the gestational age of 18 weeks has been shown to be a predictor of cobalamin, tHcy, and MMA concentrations in the mother during pregnancy and lactation and in the infant at 6 months of age [16].
It cannot be excluded that some children identified with milder functional vitamin B12 deficiency would not have developed symptoms without treatment. This depends on the choice of nutrition following birth. Breast feeding, which was the preferred way of child nutrition in our study, by a mother with vitamin B12 deficiency or suboptimal vitamin B12 status poses a relevant risk, as reported cases diagnosed with severe clinical symptoms of vitamin B12 deficiency had vitamin B12 levels at diagnosis of about 100 pmol/L after prolonged episodes of exclusive breast milk feeding. These cases might well have had higher neonatal vitamin B12 levels still resulting in symptomatic vitamin B12 deficiency with breast feeding by a vitamin B12-deficient mother [40].
A serum vitamin B12 level of >394 pmol/L at week 18 of pregnancy is recommended [16]. Therefore, vitamin B12 levels of pregnant women need to be carefully assessed early in pregnancy to provide appropriate recommendations for diet and supplementation during pregnancy and to ensure an optimal fetal and neonatal nutrient supply [16,41].
4.3. Gestational Age, Birth Weight, and Congenital Heart Defects
In a meta-analysis from Norway [42], maternal vitamin B12 deficiency was associated with preterm birth. This correlation could not be shown in our evaluation. Data on the relationship between vitamin B12 levels and birth weight have been controversial [41]. Vitamin B12 deficiency has been associated with low birth weight and intrauterine growth restriction [41,42]. However, some studies did not find any association [41,43,44,45]. In our cohort, neither infant vitamin B12 levels nor maternal vitamin B12 levels showed any association with gestational age or birth weight. However, it must be emphasized that in our analysis, maternal levels were determined postpartum, whereas in the study from India [41], low birth weight was associated with low maternal vitamin B12 levels in the first and second trimesters.
Other studies have postulated an association between vitamin B12 deficiency or hyperhomocysteinemia and congenital heart defects [46]. The birth prevalence of congenital heart defects is 9 per 1000 live births [47,48]. In our cohort, one patient suffered from a VSD resulting in a prevalence of 2.1% with respect to all cases with data reported on this aspect. However, in relation to the total cohort of 121 cases, the prevalence is only 0.08%, which is in accordance with the overall prevalence in the normal population. Thus, given the limitation of available data, no clearly increased incidence of congenital heart defects could be shown for newborns in this cohort.
4.4. Infantiles’ Response to Therapy
Most children were treated by an oral supplementation regimen developed for this NBS pilot study. The treatment response as part of confirmatory diagnostics and clinical follow-up showed that this is an effective and feasible alternative to invasive intramuscular applications [21,22,49]. The parenteral supplementation regimen (including intramuscular and intravenous supplementation) showed a higher response in terms of vitamin B12 levels but may also point to an over-treatment given the supranormal vitamin B12 levels achieved. An at least normal range of vitamin B12 levels and rapid normalization of functional parameters are reached with both oral and parenteral treatment.
5. Conclusions
Vitamin B12 deficiency is associated with adverse outcomes for mother and child if untreated. Early detection of maternal vitamin B12 deficiency already in pregnancy would be desirable but is complex and currently not sufficiently performed. Maternal blood counts alone do not allow for the differentiation of vitamin B12 deficiency and other, possibly combined, nutritional deficiencies. NBS for vitamin B12 deficiency is feasible and allows early treatment in children and further work-up and treatment for mothers. After detection of vitamin B12 deficiency in NBS, a systematic multidisciplinary evaluation and therapy of both children and mothers should be performed. This is of benefit for both children and mothers and can also prevent affected subsequent pregnancies.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/nu14183767/s1, Table S1: Maternal characteristics; Table S2: Child characteristics.
Author Contributions
Conceptualization, G.G., A.T.R.-H., K.H.W. and G.F.H.; methodology, G.G., A.T.R.-H. and S.F.G.; formal analysis, A.T.R.-H. and S.F.G.; investigation, G.G., A.T.R.-H. and K.H.W.; resources, G.F.H.; data curation, P.F.; writing—original draft preparation, G.G. and A.T.R.-H.; writing—review and editing, S.F.G., K.H.W., P.F., U.M., S.K. and G.F.H.; visualization, A.T.R.-H. and S.F.G.; supervision, G.G.; funding acquisition, S.K. and G.F.H. All authors have read and agreed to the published version of the manuscript.
Funding
The newborn screening pilot study (“Extension of Newborn Screening by 26 additional Metabolic Disorders”) is generously supported by the Dietmar Hopp Foundation, St. Leon-Rot, Germany (grant numbers 2311221, DH2011117 and 2311220 to S.K. and G.F.H.).
Institutional Review Board Statement
The study NBS 2020 was conducted in accordance with the Declaration of Helsinki, and approved by the ethics committee of the University Hospital Heidelberg (Number S-533/2015).
Informed Consent Statement
Written informed consent was obtained from a legal guardian before participation in the study.
Acknowledgments
The newborn screening pilot study (“Extension of Newborn Screening by 26 additional Metabolic Disorders”) is generously supported by the Dietmar Hopp Foundation, St. Leon-Rot, Germany (grant numbers 2311221, DH2011117 and 2311220 to S.K. and G.F.H.). The authors confirm independence from the sponsor; the content of the article has not been influenced by the sponsor.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lyon, P.; Strippoli, V.; Fang, B.; Cimmino, L. B vitamins and one-carbon metabolism: Implications in human health and disease. Nutrients 2020, 12, 2867. [Google Scholar] [CrossRef] [PubMed]
- Stabler, S.P. Vitamin B12 deficiency. N. Engl. J. Med. 2013, 368, 149–160. [Google Scholar] [CrossRef]
- Nielsen, M.J.; Rasmussen, M.R.; Andersen, C.B.F.; Nexø, E.; Moestrup, S.K. Vitamin B12 transport from food to the body’s cells—A sophisticated, multistep pathway. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 345–354. [Google Scholar] [CrossRef]
- Stabler, S.P.; Allen, R.H. Vitamin B12 deficiency as a worldwide problem. Annu. Rev. Nutr. 2004, 24, 299–326. [Google Scholar] [CrossRef] [PubMed]
- Green, R.; Allen, L.H.; Bjørke-Monsen, A.-L.; Brito, A.; Guéant, J.-L.; Miller, J.W.; Molloy, A.M.; Nexo, E.; Stabler, S.; Toh, B.-H.; et al. Vitamin B 12 deficiency. Nat. Rev. Dis. Primers 2017, 3, 17040. [Google Scholar] [CrossRef]
- McLean, E.; de Benoist, B.; Allen, L.H. Review of the magnitude of folate and vitamin B12 deficiencies worldwide. Food Nutr. Bull. 2008, 29 (Suppl. 2), S38–S51. [Google Scholar] [CrossRef]
- Allen, L.H. How common is vitamin B-12 deficiency? Am. J. Clin. Nutr. 2009, 89, 693S–696S. [Google Scholar] [CrossRef]
- Sukumar, N.; Adaikalakoteswari, A.; Venkataraman, H.; Maheswaran, H.; Saravanan, P. Vitamin B12 status in women of childbearing age in the UK and its relationship with national nutrient intake guidelines: Results from two National Diet and Nutrition Surveys. BMJ Open 2016, 6, e011247. [Google Scholar] [CrossRef] [PubMed]
- Obeid, R.; Murphy, M.; Solé-Navais, P.; Yajnik, C. Cobalamin status from pregnancy to early childhood: Lessons from global experience. Adv. Nutr. 2017, 8, 971–979. [Google Scholar] [CrossRef]
- Murphy, M.M.; Molloy, A.M.; Ueland, P.M.; Fernandez-Ballart, J.D.; Schneede, J.; Arija, V.; Scott, J.M. Longitudinal study of the effect of pregnancy on maternal and fetal cobalamin status in healthy women and their offspring. J. Nutr. 2007, 137, 1863–1867. [Google Scholar] [CrossRef] [Green Version]
- Gramer, G.; Hoffmann, G.F. Vitamin B12 deficiency in newborns and their mothers. Curr. Med. Sci. 2020, 40, 801–809. [Google Scholar] [CrossRef]
- Scolamiero, E.; Villani, G.R.D.; Ingenito, L.; Pecce, R.; Albano, L.; Caterino, M.; di Girolamo, M.G.; Di Stefano, C.; Franzese, I.; Gallo, G.; et al. Maternal vitamin B12 deficiency detected in expanded newborn screening. Clin. Biochem. 2014, 47, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Sukumar, N.; Rafnsson, S.B.; Kandala, N.-B.; Bhopal, R.; Yajnik, C.S.; Saravanan, P. Prevalence of vitamin B-12 insufficiency during pregnancy and its effect on offspring birth weight: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 103, 1232–1251. [Google Scholar] [CrossRef]
- Schroder, T.H.; Sinclair, G.; Mattman, A.; Jung, B.; Barr, S.I.; Vallance, H.D.; Lamers, Y. Pregnant women of South Asian ethnicity in Canada have substantially lower vitamin B12 status compared with pregnant women of European ethnicity. Br. J. Nutr. 2017, 118, 454–462. [Google Scholar] [CrossRef]
- Finkelstein, J.L.; Layden, A.J.; Stover, P.J. Vitamin B-12 and perinatal health. Adv. Nutr. 2015, 6, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Varsi, K.; Ueland, P.M.; Torsvik, I.K.; Bjørke-Monsen, A.-L. Maternal serum cobalamin at 18 weeks of pregnancy predicts infant cobalamin status at 6 months—A prospective, observational study. J. Nutr. 2018, 148, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Graham, S.M.; Arvela, O.M.; Wise, G.A. Long-term neurologic consequences of nutritional vitamin B12 deficiency in infants. J. Pediatrics 1992, 121, 710–714. [Google Scholar] [CrossRef]
- Jain, R.; Singh, A.; Mittal, M.; Talukdar, B. Vitamin B12 deficiency in children: A treatable cause of neurodevelopmental delay. J. Child Neurol. 2015, 30, 641–643. [Google Scholar] [CrossRef]
- Singh, G.; Le, D.; Schnabl, K.; Leaker, M.T.; Steele, M.; Sparkes, R.L. Vitamin B12 deficiency in infancy: The case for screening. Pediatric Blood Cancer 2016, 63, 740–742. [Google Scholar] [CrossRef]
- Röschinger, W.; Sonnenschein, S.; Schuhmann, E.; Nennstiel-Ratzel, U.; Roscher, A.; Olgemöller, B. Neue zielerkrankungen im neugeborenenscreening. Mon. Kinderheilkd. 2015, 163, 142–149. [Google Scholar] [CrossRef]
- Mütze, U.; Walter, M.; Keller, M.; Gramer, G.; Garbade, S.F.; Gleich, F.; Haas, D.; Posset, R.; Grünert, S.C.; Hennermann, J.B.; et al. Health outcomes of infants with Vitamin B12 deficiency identified by newborn screening and early treated. J. Pediatrics 2021, 235, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Gramer, G.; Fang-Hoffmann, J.; Feyh, P.; Klinke, G.; Monostori, P.; Mütze, U.; Posset, R.; Weiss, K.H.; Hoffmann, G.F.; Okun, J.G.; et al. Newborn screening for Vitamin B(12) deficiency in Germany—Strategies, results, and public health implications. J. Pediatr. 2020, 216, 165–172.e4. [Google Scholar] [CrossRef] [PubMed]
- Reinson, K.; Künnapas, K.; Kriisa, A.; Vals, M.-A.; Muru, K.; Õunap, K. High incidence of low vitamin B12 levels in Estonian newborns. Mol. Genet. Metab. Rep. 2018, 15, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Sarafoglou, K.; Rodgers, J.; Hietala, A.; Matern, D.; Bentler, K. Expanded newborn screening for detection of vitamin B12 deficiency. JAMA 2011, 305, 1198–1200. [Google Scholar] [CrossRef] [PubMed]
- Richtlinie des Gemeinsamen Bundesausschusses über die Früherkennung von Krankheiten bei Kindern (Kinder-Richtlinie); Gemeinsamer Bundesausschuss: Berlin/Heidelberg, Germany, 2022; Volume 18.
- Monostori, P.; Klinke, G.; Richter, S.; Baráth, A.; Fingerhut, R.; Baumgartner, M.R.; Kölker, S.; Hoffmann, G.F.; Gramer, G.; Okun, J.G. Simultaneous determination of 3-hydroxypropionic acid, methylmalonic acid and methylcitric acid in dried blood spots: Second-tier LC-MS/MS assay for newborn screening of propionic acidemia, methylmalonic acidemias and combined remethylation disorders. PLoS ONE 2017, 12, e0184897. [Google Scholar] [CrossRef] [PubMed]
- Gan-Schreier, H.; Kebbewar, M.; Fang-Hoffmann, J.; Wilrich, J.; Abdoh, G.; Ben-Omran, T.; Shahbek, N.; Bener, A.; Al Rifai, H.; Al Khal, A.L.; et al. Newborn population screening for classic homocystinuria by determination of total homocysteine from guthrie cards. J. Pediatr. 2010, 156, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Hannibal, L.; Lysne, V.; Bjørke-Monsen, A.-L.; Behringer, S.; Grünert, S.C.; Spiekerkoetter, U.; Jacobsen, D.W.; Blom, H.J. Biomarkers and algorithms for the diagnosis of vitamin B12 deficiency. Front. Mol. Biosci. 2016, 3, 27. [Google Scholar] [CrossRef]
- Bundesamt, S. Bevölkerung Migration und Integration 2022. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Migration-Integration/_inhalt.html (accessed on 20 February 2022).
- Honzik, T.; Adamovicova, M.; Smolka, V.; Magner, M.; Hruba, E.; Zeman, J. Clinical presentation and metabolic consequences in 40 breastfed infants with nutritional vitamin B12 deficiency—What have we learned? Eur. J. Paediatr. Neurol. 2010, 14, 488–495. [Google Scholar] [CrossRef]
- Hinton, C.F.; Ojodu, J.A.; Fernhoff, P.M.; Rasmussen, S.A.; Scanlon, K.S.; Hannon, W.H. Maternal and neonatal vitamin B12 deficiency detected through expanded newborn screening—United States, 2003–2007. J. Pediatr. 2010, 157, 162–163. [Google Scholar] [CrossRef]
- Koletzko, B.; Cremer, M.; Flothkötter, M.; Graf, C.; Hauner, H.; Hellmers, C.; Kersting, M.; Krawinkel, M.; Przyrembel, H.; Röbl-Mathieu, M.; et al. Diet and lifestyle before and during pregnancy–practical recommendations of the Germany-wide healthy start–young family network. Geburtshilfe Frauenheilkd. 2018, 78, 1262–1282. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, H.; Bellach, B. Der bundes-gesundheits-survey 1998—Erfahrungen, ergebnisse, perspektiven. Gesundheitswesen 1999, 61, S55–S56. [Google Scholar]
- Masih, S.P.; Plumptre, L.; Ly, A.; Berger, H.; Lausman, A.Y.; Croxford, R.; Kim, Y.-I.; O’Connor, D.L. Pregnant Canadian women achieve recommended intakes of one-carbon nutrients through prenatal supplementation but the supplement composition, including choline, requires reconsideration. J. Nutr. 2015, 145, 1824–1834. [Google Scholar] [CrossRef] [PubMed]
- Karabiber, H.; Sonmezgoz, E.; Ozerol, E.; Yakinci, C.; Otlu, B.; Yologlu, S. Effects of valproate and carbamazepine on serum levels of homocysteine, vitamin B12, and folic acid. Brain Dev. 2003, 25, 113–115. [Google Scholar] [CrossRef]
- Karaoglu, L.; Pehlivan, E.; Egri, M.; Deprem, C.; Gunes, G.; Genc, M.F.; Temel, I. The prevalence of nutritional anemia in pregnancy in an east Anatolian province, Turkey. BMC Public Health 2010, 10, 329. [Google Scholar] [CrossRef] [PubMed]
- Hartong, S.; Steegers, E.; Visser, W. Hemolysis, elevated liver enzymes and low platelets during pregnancy due to vitamin B12 and folate deficiencies. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 131, 241–242. [Google Scholar] [CrossRef]
- Solé-Navais, P.; Cavallé-Busquets, P.; Fernandez-Ballart, J.D.; Murphy, M.M. Early pregnancy B vitamin status, one carbon metabolism, pregnancy outcome and child development. Biochimie 2016, 126, 91–96. [Google Scholar] [CrossRef]
- Eidgenossenschaft, S. Gesundheit von Müttern und Kindern mit Migrationshintergrund. 2015. Available online: https://www.bfs.admin.ch/bfs/portal/de/index/news/00/06.html (accessed on 28 November 2014).
- Centers for Disease Control and Prevention. Neurologic impairment in children associated with maternal dietary deficiency of cobalamin—Georgia, 2001. MMWR Morb. Mortal. Wkly. Rep. 2003, 52, 61–64. [Google Scholar]
- Mishra, J.; Tomar, A.; Puri, M.; Jain, A.; Saraswathy, K. Trends of folate, vitamin B12, and homocysteine levels in different trimesters of pregnancy and pregnancy outcomes. Am. J. Hum. Biol. 2020, 32, e23388. [Google Scholar] [CrossRef]
- Rogne, T.; Tielemans, M.J.; Chong, M.F.-F.; Yajnik, C.S.; Krishnaveni, G.V.; Poston, L.; Jaddoe, V.W.V.; Steegers, E.A.P.; Joshi, S.; Chong, Y.-S.; et al. Associations of maternal vitamin B12 concentration in pregnancy with the risks of preterm birth and low birth weight: A systematic review and meta-analysis of individual participant data. Am. J. Epidemiol. 2017, 185, 212–223. [Google Scholar] [CrossRef]
- Özturk, Ö.; Keskin, L.; Tafl, E.E.; Akgün, N.; Avflar, F. The effect of vitamin B12 level on fetal birth weight. Perinat. J. 2015, 23, 73–78. [Google Scholar] [CrossRef]
- Hogeveen, M.; Blom, H.J.; van der Heijden, E.H.; Semmekrot, B.A.; Sporken, J.M.; Ueland, P.M.; Heijer, M.D. Maternal homocysteine and related B vitamins as risk factors for low birthweight. Am. J. Obstet. Gynecol. 2010, 202, 572.e1–572.e6. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.; Sinclair, G.; Mattman, A.; Vallance, H.D.; Lamers, Y. Maternal vitamin B12 status in early pregnancy and its association with birth outcomes in Canadian mother–newborn Dyads. Br. J. Nutr. 2021, 126, 1823–1831. [Google Scholar] [CrossRef]
- Verkleij-Hagoort, A.C.; van Driel, L.M.; Lindemans, J.; Isaacs, A.; Steegers, E.A.; Helbing, W.A.; Uitterlinden, A.G.; Steegers-Theunissen, R.P. Genetic and lifestyle factors related to the periconception vitamin B12 status and congenital heart defects: A Dutch case-control study. Mol. Genet. Metab. 2008, 94, 112–119. [Google Scholar] [CrossRef]
- Van Der Linde, D.; Konings, E.E.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef]
- Pfitzer, C.; Helm, P.C.; Ferentzi, H.; Rosenthal, L.-M.; Bauer, U.M.M.; Berger, F.; Schmitt, K.R.L. Changing prevalence of severe congenital heart disease: Results from the National Register for Congenital Heart Defects in Germany. Congenit. Heart Dis. 2017, 12, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Bahadir, A.; Reis, P.G.; Erduran, E. Oral vitamin B 12 treatment is effective for children with nutritional vitamin B 12 deficiency. J. Paediatr. Child Health 2014, 50, 721–725. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).