Abstract
Obesity is a risk factor for NAFLD. However, not all people with obesity have an excessive intrahepatic fat content. Adherence to a high-quality dietary pattern may also promote liver health in obesity. A cross-sectional study of 2967 women with overweight and obesity was carried out to assess the association between a Mediterranean diet and fatty liver. All women underwent clinical examination, anthropometric measurements, blood sampling, ultrasound measurements of abdominal visceral and subcutaneous fat, and assessment of adherence to the Mediterranean diet using the 14-item MEDAS questionnaire. Fatty liver index (FLI), NAFLD fatty liver steatosis (NAFLD-FLS) and hepatic steatosis index (HSI) were calculated. In women with obesity, the MEDAS score was inversely associated with FLI (β = −0.60, 95% CI: −1.04, −0.16, p = 0.008), NAFLD-FLS (β = −0.092, 95% CI: −0.134, −0.049, p < 0.001) and HSI (β = −0.17, 95% CI: −0.30, −0.04, p = 0.011). Stronger associations were observed in premenopausal women with obesity. Mediterranean diet was inversely associated with NAFLD-FLS in women with overweight, independently of menopausal status. In conclusion, Mediterranean diet is associated with a better liver status in women with overweight and obesity. This may have a public health impact and be useful in drafting nutritional guidelines for NAFLD.
1. Introduction
Non-alcoholic fatty liver disease (NAFLD) is a condition resulting from excessive lipid accumulation in the liver (triglyceride content >5% of organ weight) in individuals with low alcohol consumption (<20 g/day in women and <30 g/day in men) [1]. NAFLD encompasses a spectrum of conditions, including simple steatosis, non-alcoholic steatohepatitis (NASH) and cirrhosis, which can sometimes progress to hepatocarcinoma [1]. The reference method for diagnosing NAFLD is liver biopsy [2]. However, this is an expensive and invasive procedure that can lead to clinical complications in 1% of patients and death in 0.01% of them [3]. Non-invasive fatty liver indices are easy-to-use diagnostic tools with good accuracy in detecting NAFLD, and because of this fact, several European scientific societies recommend their use for the diagnosis and management of NAFLD, especially when imaging techniques are not available or not feasible [4]. In Western countries, NAFLD affects 20–30% of the adult general population [5], with a prevalence higher in men than in women in the reproductive age. However, after menopause, NAFLD occurs more frequently in women [6].
Obesity is an established risk factor for the development of NAFLD, and 50% to 75% of people with obesity also have NAFLD [7]. Excess body weight is associated with excess visceral fat accumulation and insulin resistance, which are the two main actors in the pathogenesis of NAFLD. However, NAFLD is not inextricably linked to obesity; some individuals with obesity have normal liver fat, while others with normal weight have NAFLD [8]. Environmental factors, such as adherence to a high-quality dietary pattern, may favorably influence the metabolic profile of individuals with overweight and obesity, preventing or delaying the development of NAFLD.
The Mediterranean diet is a high-quality dietary pattern characterized by high consumption of fruits and vegetables, cereals, especially whole grains, nuts and legumes, with olive oil as the main source of added fats, along with high to moderate intake of fishery products, moderate consumption of dairy products, white meat and eggs, low consumption of red or processed meat and moderate intake of alcohol (especially wine at meals) [9]. The Mediterranean diet is inversely associated with obesity, metabolic syndrome, cardiovascular disease (CVD) and type 2 diabetes [10]. Some cohort studies suggest that Mediterranean diet may be beneficial for the primary prevention of NAFLD in the general population [11,12]. An inverse association between adherence to the Mediterranean diet and risk of NAFLD has also been reported by a number of case–control [13,14] and cross-sectional [15,16,17] studies of healthy subjects and convenience samples of subjects with selected metabolic disease. However, we are not aware of studies performed in patients with excess body weight. Studies investigating the association between Mediterranean diet and non-invasive indices of fatty liver in these patients are, therefore, required. Knowledge of the relationship between diet and fatty liver is necessary to develop effective strategies for the prevention and treatment of NAFLD associated with obesity [18]. Previously, several randomized controlled trials have shown the potential benefits of the Mediterranean diet against the progression of hepatic steatosis in individuals with obesity [19,20,21,22]. Moreover, it has been reported that the Mediterranean diet is associated with lower visceral fat accumulation [23], greater insulin sensitivity [24] and fewer metabolic alterations in individuals with obesity [25]. In light of this evidence, it is presumable that the Mediterranean diet is also associated with lower indices of fatty liver in individuals with excess body weight. In women, however, the association between diet and liver health could be influenced by menopausal status. With the advent of menopause, in fact, a redistribution of adipose tissue from the gluteo-femoral to the abdominal region occurs, increasing cardiometabolic risk. To verify these assumptions, the aim of this study was to evaluate the association between Mediterranean diet and non-invasive indices of fatty liver in a large sample of women with overweight and obesity.
2. Materials and Methods
2.1. Study Design and Protocol
We performed a cross-sectional study of 2967 consecutive women with overweight and obesity referring to the International Center for Nutritional Status Assessment (ICANS, University of Milan, Milan, Italy) from September 2010 to February 2020, to devise a nutritional assessment and obtain a personalized dietary intervention to lose weight. The study was conducted following the guidelines established by the Declaration of Helsinki. The Ethics Committee of the University of Milan approved the study procedures (study protocol No. 23/2016). Patients gave written informed consent for the use of their data for research purposes.
The inclusion criteria were: women, age ≥ 18 years, BMI ≥ 25 kg/m2 and alcohol intake ≤ 20 g/day. The exclusion criteria were: diabetes, cardiovascular disease, cancer within the past 5 years, hepatitis C virus infection, hepatitis B virus infection, liver cirrhosis, neurological disease, gastrointestinal disease, cardiac failure, renal failure, pulmonary insufficiency and use of drugs known to cause lipodystrophy.
The patients underwent a clinical history and a physical examination. An appointed physician collected the data on the personal and family occurrence of CVD, diabetes and other chronic disease, previous and current pharmacological treatment, menopausal status, blood pressure and lifestyle habits, such as smoking and structured physical activity. Blood pressure was measured using international guidelines. Such guidelines changed during the study period but not with regard to the method of measurement of blood pressure. Women reporting absence of menstrual cycle for at least 12 months were defined as postmenopausal.
A fasting blood sample was drawn between 08:30 and 09:00 AM for the measurement of blood glucose, insulin, triglycerides, total-, low-density-lipoprotein (LDL)-, high-density-lipoprotein (HDL)-cholesterol and alanine transaminase (ALT), aspartate transaminase (AST) and gamma-glutamyl-transferase (GGT).
Thereafter, an experienced physician measured the thicknesses of visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) at the abdominal level using ultrasonography (Logiq 3 Pro, GE Healthcare, Boston, MA, USA) with a 7.5 MHz linear probe and a 3.5 MHz convex-array probe. The measurements, recorded at the end of expiration, were taken 1 cm above the umbilicus. VAT was defined as the distance between the posterior surface of the rectus abdominis muscle and the anterior wall of the aorta. SAT was defined as the distance between the external face of the rectus abdominis muscle and the epidermis [26,27].
Lastly, a registered dietitian took anthropometric measurements following international guidelines [28]. Weight was measured with an electronic scale with an accuracy of 100 g (Seca 700, Seca Corporation, Hamburg, Germany). Height was measured with a vertical stadiometer with an accuracy of 0.1 cm. Waist circumference (WC) was measured with an accuracy of 0.5 cm using a nonelastic tape placed at the midpoint between the last rib and the iliac crest. The thicknesses of four skinfolds (biceps, triceps, subscapular and suprailiac) were measured using a skinfold caliper (Holtan Ltd., Crymych, Wales). Fat mass was estimated from the Durnin–Womersley equation [29]. Percent fat mass (%FM) was calculated as (fat mass (kg)/body weight (kg)) × 100.
Metabolic syndrome was diagnosed according to the harmonized definition [30].
2.2. Outcome Assessment
Fatty liver status was evaluated using the following non-invasive indices:
- Fatty liver index (FLI) [31] = eLP/(1 + eLP) × 100 where LP (linear predictor) = 0.953 × ln(triglycerides (mg/dL)) + 0.139 × BMI (kg/m2) + 0.718 × ln (GGT (U/L)) + 0.053 × WC (cm) − 15.745;
- Non-alcoholic fatty liver disease–fatty liver steatosis (NAFLD-FLS) [32] = −2.89 + 1.18 × Metabolic syndrome (0 = No; 1 = Yes) + 0.45 × type 2 diabetes mellitus (2 = Yes; 0 = No) + 0.15 × insulin (mU/L) + 0.04 × AST (U/L) − 0.94 × AST (U/L)/ALT (U/L);
- Hepatic steatosis index (HSI) [33] = 8 × (ALT (U/L)/AST (U/L)) + BMI (kg/m2) + 2 if woman + 2 if diabetes mellitus.
2.3. Mediterranean Diet Adherence
Adherence to the Mediterranean diet was evaluated using the 14-item Mediterranean diet adherence screener (MEDAS), a short questionnaire developed and validated in the PREDIMED trial [34]. Such questionnaire investigates food preferences and the frequency of consumption of foods typical of the Mediterranean diet and of Western diets. For each item, one point is assigned if the Mediterranean criterion is met, as reported in Supplementary Table S1 [35,36,37]. The score of MEDAS ranges from 0 to 14 points.
2.4. Statistical Analysis
As most continuous variables were not normally distributed, all are presented as median and interquartile range. Discrete variables are presented as frequency and percentage. Linear regression models were used to evaluate the association between the MEDAS score (continuous) and fatty liver indices. Age (continuous), BMI class (discrete; 0 = overweight, 1 = obesity), %FM (continuous), VAT (continuous), SAT (continuous), total cholesterol (continuous), HDL (continuous), glucose (continuous), menopausal status (discrete, 0 = premenopausal, 1 = postmenopausal), smoking (discrete; 0 = non-smoker, 1 = ex-smoker, 2 = smoker), physical activity (discrete; 0 = no, 1 = at least 2 h/week), statins (discrete, 0 = no, 1 = yes) were included as potential confounders. To evaluate the association of the Mediterranean diet with fatty liver, a BMI × MEDAS (discrete x continuous) interaction was added to the models; because the BMI × MEDAS interaction was significant for all models, we reported the results separately for each BMI class. No evidence of multicollinearity was found among the predictors. Multivariable fractional polynomials were used to model non-linear associations of continuous predictors with the outcome. Because we found some violations of the homoscedasticity assumption in some regression models, robust confidence intervals were calculated for all models [23]. A p value of <0.05 was considered statistically significant. Statistical analysis was performed using Stata 12.0 (Stata Corporation, College Station, TX, USA).
3. Results
The measurements of the patients stratified by BMI category are reported in Table 1.

Table 1.
Characteristics of patients.
Table 2 reports the association of the Mediterranean diet score with fatty liver indices.
Table 2.
Association of Mediterranean diet with fatty liver indices in women with overweight and obesity.
MEDAS was associated with the indices of fatty liver, but the magnitude of the association differed among the BMI classes. In women with obesity, a 1-point increase in MEDAS was associated with a 0.60 reduction in FLI (95% CI: −1.04; −0.16, p = 0.008), a 0.092 reduction in NAFLD-FLS (95% CI: −0.134; −0.049, p < 0.001) and a 0.17 reduction in HSI (95% CI: −0.30; −0.04, p = 0.011). In women with overweight, a 1-point increase in MEDAS was associated with a 0.034 reduction in NAFLD-FLS (95% CI: −0.057; −0.010, p = 0.005), while no association between the MEDAS score and FLI and HSI was found. Figure 1 shows the marginal mean of indices of fatty liver associated with the MEDAS score in women with overweight and obesity.
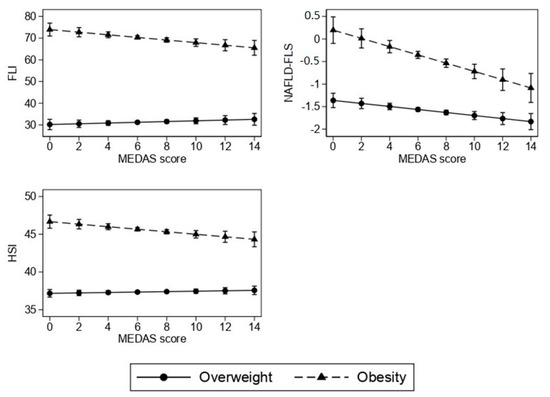
Figure 1.
Association of Mediterranean diet (MEDAS score) with indices of fatty liver according to BMI category. Values are marginal means and 95% confidence intervals estimated from multivariable linear regression.
Given the impact of menopause on body composition and metabolism, we also stratified the analysis for the menopausal status (Table 3).
Table 3.
Association of Mediterranean diet with fatty liver indices in women affected by overweight and obesity according to menopausal status.
In premenopausal women with obesity, MEDAS was inversely associated with all indices of fatty liver, while in postmenopausal women, MEDAS was inversely associated only with NAFLD-FLS (−0.077, 95% CI: −0.148; −0.007, p = 0.032, for 1-unit increase). In women with overweight, MEDAS was stably associated with NAFLD-FLS, independently of menopausal status. Figure 2 shows the marginal means of indices of fatty liver associated with MEDAS in pre- and postmenopausal women with overweight and obesity.
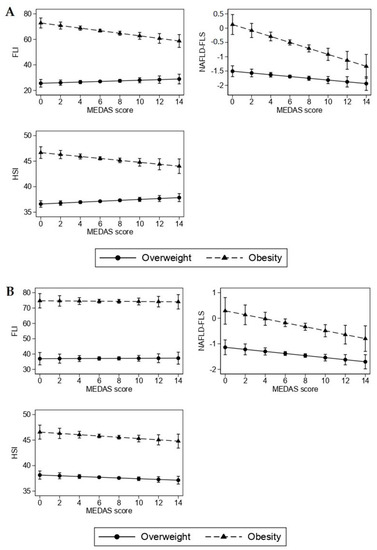
Figure 2.
Association of Mediterranean diet (MEDAS score) with indices of fatty liver according to BMI category in premenopausal (A) and postmenopausal (B) women.
4. Discussion
Non-invasive fatty liver indices are commonly used in clinical practice as simple and accurate tools to screen for NAFLD, especially when imaging techniques are not available. Among them, FLI and NAFLD-FLS have been extensively validated in external populations [4]. Recently, HSI has also been externally validated and has been found to perform similarly to the FLI in predicting NAFLD [38]. In the present study, higher adherence to the Mediterranean diet was associated with lower indices of fatty liver in women with overweight and obesity, suggesting that diet quality, even without energy restriction, might promote liver health despite excess body weight. These findings are consistent with those of trials showing that the Mediterranean diet lowers liver fat in people with obesity, even without energy restriction and weight loss [21]. Therefore, choosing a Mediterranean diet as dietary intervention to achieve weight loss might improve liver health, even if it fails to improve weight status. Taken together, these findings may have relevance for public health and may be useful to draft nutritional guidelines aimed at the prevention and management of NAFLD.
The exact pathophysiological pathway leading to fat accumulation in the liver is not entirely clear [39]. However, the prevailing view is that it occurs as a result of an initial alteration of insulin sensitivity in adipose tissue, which would lead to uninhibited lipolysis, which, in turn, produces increased fatty acid (FA) flow to the liver and other organs (e.g., muscle) [40]. It is estimated that 60% of the triglycerides in the liver come from adipose tissue [41]. VAT is the main source of FA to the liver [42,43]. In subjects with obesity, VAT delivers 20% of total fatty acid intake to the liver, as compared to 5% in lean subjects [44]. Peripheral insulin resistance also enhances hepatic de novo lipogenesis [45,46], increasing hepatic triglyceride accumulation. This pathway accounts for 25% of hepatic triglyceride content [41,47]. This may, in turn, lead to dysregulation of VLDL production and secretion [48,49,50], which would be increased as a compensatory response to intrahepatocyte triglyceride accumulation, although this pathway seems to be insufficient to normalize the elevated hepatic triglyceride content [40]. The mechanisms proposed to explain the impact of Mediterranean diet on hepatic fat deposition involve the ability of diet to regulate general and visceral adiposity, as well as the specific biochemical processes occurring in the liver. In fact, it has been previously reported that there is an inverse association between adherence to the Mediterranean diet and the amount of abdominal visceral fat [23,51]. Moreover, as a result of higher consumption of fruits and vegetables and olive oil, individuals following the Mediterranean diet have higher intakes of dietary polyphenols and monounsaturated fatty acids, which have been shown to inhibit de novo lipogenesis and improve peripheral insulin sensitivity, mainly through their antioxidant, anti-inflammatory and antifibrotic effects [52,53,54,55]. The Mediterranean diet is also characterized by high consumption of fish and seafood, which contributes to increased intake of omega-3 PUFAs, which have been shown to reduce hepatic lipid accumulation and improve liver enzymes and insulin sensitivity, as well as having anti-inflammatory effects. In contrast, low omega-3 PUFAs intake has been correlated with the development of NAFLD and progression to NASH and cirrhosis [56,57,58]. In addition, the high fiber content of the Mediterranean diet may positively influence body weight and the composition of the gut microbiota [59] by increasing the levels of bacteria that produce short-chain fatty acids, such as butyrate and propionate, which have been shown to have insulin-sensitizing effects [60,61]. The Mediterranean diet is also low in saturated fats, which have been shown to enhance de novo lipogenesis, insulin resistance and increased hepatic triglyceride content [62,63,64]. On the other hand, women not following the Mediterranean diet may have a higher consumption of ultra-processed foods [65], whose consumption has been associated with overweight and obesity [66], visceral fat accumulation [67], insulin resistance, diabetes [68,69] and NAFLD [70].
Our results also show a stronger inverse association between Mediterranean diet and fatty liver indices in women with obesity than in women with overweight. Women with obesity had higher fatty liver indices than overweight women who had a medium–low risk of NAFLD, i.e., a median FLI < 30. Clinical trials have shown that the Mediterranean diet, in addition to reducing liver fat, improves insulin sensitivity and helps the reversion of metabolic syndrome, even without weight loss [21,71]. It follows that women at high risk of NAFLD may benefit more from increased adherence to the Mediterranean diet. Unlike the other fatty liver indices studied here, NAFLD-FLS does not include body weight and considers metabolic parameters, including insulin and metabolic syndrome. It is therefore possible that this index is more sensitive to the effect of diet quality, especially without weight loss. This may explain why NAFLD-FLS was inversely associated with Mediterranean diet adherence in both women with overweight and obesity, while such association was detected for FLI and HSI only in women with obesity. The same fact could explain the lack of association between FLI, HSI and Mediterranean diet in postmenopausal women. Menopause is accompanied by a physiological redistribution of adipose tissue, which tends to accumulate preferentially at the abdominal level. Therefore, the inclusion of parameters such as BMI and waist circumference could mitigate the association between fatty liver indices and adherence to the Mediterranean diet in postmenopausal women.
To the best of our knowledge, no study has assessed the association between adherence to the Mediterranean diet and fatty liver indices in women with overweight and obesity. In addition to its novelty, the present work has some strengths. First, the data are from a large population. Second, we used indices of fatty liver that have been externally validated and shown to have good and similar predictive abilities. Third, we controlled for a wide range of covariates, body composition and abdominal fat distribution, metabolic status and lifestyle, all variables that may impact metabolic status and risk of fatty liver. However, our study is not without limitations. First, a cross-sectional study design cannot prove a cause–effect relationship. Second, although we chose externally validated fatty liver indices, the use of such indices does not allow for the exact separation of individuals with NAFLD from those without. However, compared to liver biopsy, these indices are non-invasive, simple to use in clinical practice and cost effective. In addition, some of them, such as the FLI and NAFLD-FLS, are recommended by several European scientific societies for liver health screening in large epidemiological studies and when imaging techniques are not available [4]. Third, body composition was assessed using surrogate techniques, such as skinfold thickness measurement and ultrasonography. Body skinfolds are largely used in clinical practice but provide only an estimation of total body fat. Ultrasonography provides the thickness, not the area, of abdominal fat compartments. However, some studies show a good association between ultrasound measurements and areas measured by reference methods, such as computed tomography and magnetic resonance imaging [26,72]. Fourth, although it is valuable for its designed aim, the MEDAS questionnaire is a short dietary screener and therefore considers only the consumption of few specific foods [34]. Fifth, our sample included only Caucasian individuals, so these results need confirmation in individuals of other ethnicities.
5. Conclusions
In conclusion, the Mediterranean diet is inversely associated with indices of fatty liver in women with overweight and obesity. Women with obesity, especially during the premenopausal period, may benefit more from following a Mediterranean-style diet. Nevertheless, the Mediterranean diet could also improve liver health in overweight and postmenopausal women. These findings should be confirmed by randomized clinical trials using, at the very least, imaging techniques to diagnose NAFLD.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu14183771/s1, Table S1: Questions and criteria for assessing the adherence to the Mediterranean diet.
Author Contributions
Conceptualization, A.L. and A.B.; methodology, A.L., S.B. and A.B.; formal analysis, A.L.; investigation, A.L., S.B. and L.V.; data curation, A.L.; intellectual support, G.B.; writing—original draft preparation, A.L.; writing—review and editing, A.L., M.P., G.B. and A.B.; visualization, A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The Department of Food, Environmental and Nutritional Sciences, Università degli Studi di Milano, partially covered the open access APC. The remaining was funded by ICANS internal grant.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of University of Milan (protocol code 23/2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author.
Acknowledgments
We are deeply grateful to dietitians Chiara Lessa, Lidia Lewandowski and Diana Osio, and laboratory technicians Stefano Ravasenghi, Giovanni Fiorillo and Franca Criscuoli for their work that made this study possible.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Arab, J.P.; Arrese, M.; Trauner, M. Recent Insights into the Pathogenesis of Nonalcoholic Fatty Liver Disease. Annu. Rev. Pathol. 2018, 13, 321–350. [Google Scholar] [CrossRef] [PubMed]
- Carr, R.M.; Oranu, A.; Khungar, V. Nonalcoholic Fatty Liver Disease: Pathophysiology and Management. Gastroenterol. Clin. N. Am. 2016, 45, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Bravo, A.A.; Sheth, S.G.; Chopra, S. Liver biopsy. N. Engl. J. Med. 2001, 344, 495–500. [Google Scholar] [CrossRef] [PubMed]
- EASL; EASD; EASO. EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Bellentani, S.; Scaglioni, F.; Marino, M.; Bedogni, G. Epidemiology of non-alcoholic fatty liver disease. Dig. Dis. 2010, 28, 155–161. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Ballestri, S.; Fairweather, D.; Win, S.; Than, T.A.; Abdelmalek, M.F.; Suzuki, A. Sex Differences in Nonalcoholic Fatty Liver Disease: State of the Art and Identification of Research Gaps. Hepatology 2019, 70, 1457–1469. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism 2019, 92, 82–97. [Google Scholar] [CrossRef]
- DiStefano, J.K.; Gerhard, G.S. NAFLD in normal weight individuals. Diabetol. Metab. Syndr. 2022, 14, 45. [Google Scholar] [CrossRef]
- Leone, A.; Battezzati, A.; De Amicis, R.; De Carlo, G.; Bertoli, S. Trends of Adherence to the Mediterranean Dietary Pattern in Northern Italy from 2010 to 2016. Nutrients 2017, 9, 734. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Willett, W.C. The Mediterranean diet and health: A comprehensive overview. J. Intern. Med. 2021, 290, 549–566. [Google Scholar] [CrossRef]
- Khalatbari-Soltani, S.; Marques-Vidal, P.; Imamura, F.; Forouhi, N.G. Prospective association between adherence to the Mediterranean diet and hepatic steatosis: The Swiss CoLaus cohort study. BMJ Open 2020, 10, e040959. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Hennein, R.; Liu, C.; Long, M.T.; Hoffmann, U.; Jacques, P.F.; Lichtenstein, A.H.; Hu, F.B.; Levy, D. Improved Diet Quality Associates With Reduction in Liver Fat, Particularly in Individuals With High Genetic Risk Scores for Nonalcoholic Fatty Liver Disease. Gastroenterology 2018, 155, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Giraldi, L.; Miele, L.; Aleksovska, K.; Manca, F.; Leoncini, E.; Biolato, M.; Arzani, D.; Pirro, M.A.; Marrone, G.; Cefalo, C.; et al. Mediterranean diet and the prevention of non-alcoholic fatty liver disease: Results from a case-control study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7391–7398. [Google Scholar] [CrossRef] [PubMed]
- Entezari, M.R.; Talenezhad, N.; Mirzavandi, F.; Rahimpour, S.; Mozaffari-Khosravi, H.; Fallahzadeh, H.; Hosseinzadeh, M. Mediterranean dietary pattern and non-alcoholic fatty liver diseases: A case-control study. J. Nutr. Sci. 2021, 10, e55. [Google Scholar] [CrossRef]
- Kouvari, M.; Boutari, C.; Chrysohoou, C.; Fragkopoulou, E.; Antonopoulou, S.; Tousoulis, D.; Pitsavos, C.; Panagiotakos, D.B.; Mantzoros, C.S. Mediterranean diet is inversely associated with steatosis and fibrosis and decreases ten-year diabetes and cardiovascular risk in NAFLD subjects: Results from the ATTICA prospective cohort study. Clin. Nutr. 2021, 40, 3314–3324. [Google Scholar] [CrossRef]
- Baratta, F.; Pastori, D.; Polimeni, L.; Bucci, T.; Ceci, F.; Calabrese, C.; Ernesti, I.; Pannitteri, G.; Violi, F.; Angelico, F.; et al. Adherence to Mediterranean Diet and Non-Alcoholic Fatty Liver Disease: Effect on Insulin Resistance. Am. J. Gastroenterol. 2017, 112, 1832–1839. [Google Scholar] [CrossRef]
- Doustmohammadian, A.; Clark, C.C.T.; Maadi, M.; Motamed, N.; Sobhrakhshankhah, E.; Ajdarkosh, H.; Mansourian, M.R.; Esfandyari, S.; Hanjani, N.A.; Nikkhoo, M.; et al. Favorable association between Mediterranean diet (MeD) and DASH with NAFLD among Iranian adults of the Amol Cohort Study (AmolCS). Sci. Rep. 2022, 12, 2131. [Google Scholar] [CrossRef]
- Cantero, I.; Abete, I.; Babio, N.; Arós, F.; Corella, D.; Estruch, R.; Fitó, M.; Hebert, J.R.; Martínez-González, M.; Pintó, X.; et al. Dietary Inflammatory Index and liver status in subjects with different adiposity levels within the PREDIMED trial. Clin. Nutr. 2018, 37, 1736–1743. [Google Scholar] [CrossRef]
- Gepner, Y.; Shelef, I.; Komy, O.; Cohen, N.; Schwarzfuchs, D.; Bril, N.; Rein, M.; Serfaty, D.; Kenigsbuch, S.; Zelicha, H.; et al. The beneficial effects of Mediterranean diet over low-fat diet may be mediated by decreasing hepatic fat content. J. Hepatol. 2019, 71, 379–388. [Google Scholar] [CrossRef]
- Ristic-Medic, D.; Kovacic, M.; Takic, M.; Arsic, A.; Petrovic, S.; Paunovic, M.; Jovicic, M.; Vucic, V. Calorie-Restricted Mediterranean and Low-Fat Diets Affect Fatty Acid Status in Individuals with Nonalcoholic Fatty Liver Disease. Nutrients 2020, 13, 15. [Google Scholar] [CrossRef]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’Dea, K.; Desmond, P.V.; Johnson, N.A.; Wilson, A.M. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Yaskolka Meir, A.; Rinott, E.; Tsaban, G.; Zelicha, H.; Kaplan, A.; Rosen, P.; Shelef, I.; Youngster, I.; Shalev, A.; Blüher, M.; et al. Effect of green-Mediterranean diet on intrahepatic fat: The DIRECT PLUS randomised controlled trial. Gut 2021, 70, 2085. [Google Scholar] [CrossRef] [PubMed]
- Bertoli, S.; Leone, A.; Vignati, L.; Bedogni, G.; Martínez-González, M.A.; Bes-Rastrollo, M.; Spadafranca, A.; Vanzulli, A.; Battezzati, A. Adherence to the Mediterranean diet is inversely associated with visceral abdominal tissue in Caucasian subjects. Clin. Nutr. 2015, 34, 1266–1272. [Google Scholar] [CrossRef] [PubMed]
- Tzima, N.; Pitsavos, C.; Panagiotakos, D.B.; Skoumas, J.; Zampelas, A.; Chrysohoou, C.; Stefanadis, C. Mediterranean diet and insulin sensitivity, lipid profile and blood pressure levels, in overweight and obese people; the Attica study. Lipids Heal. Dis. 2007, 6, 22. [Google Scholar] [CrossRef]
- Leone, A.; De Amicis, R.; Battezzati, A.; Bertoli, S. Adherence to the Mediterranean Diet and Risk of Metabolically Unhealthy Obesity in Women: A Cross-Sectional Study. Front. Nutr. 2022, 9, 858206. [Google Scholar] [CrossRef]
- Armellini, F.; Zamboni, M.; Rigo, L.; Todesco, T.; Bergamo-Andreis, I.A.; Procacci, C.; Bosello, O. The contribution of sonography to the measurement of intra-abdominal fat. J. Clin. Ultrasound 1990, 18, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Bertoli, S.; Leone, A.; Vignati, L.; Spadafranca, A.; Bedogni, G.; Vanzulli, A.; Rodeschini, E.; Battezzati, A. Metabolic correlates of subcutaneous and visceral abdominal fat measured by ultrasonography: A comparison with waist circumference. Nutr. J. 2016, 15, 2. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- Durnin, J.V.; Womersley, J. Body fat assessed from total body density and its estimation from skinfold thickness: Measurements on 481 men and women aged from 16 to 72 years. Br. J. Nutr. 1974, 32, 77–97. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef]
- Kotronen, A.; Peltonen, M.; Hakkarainen, A.; Sevastianova, K.; Bergholm, R.; Johansson, L.M.; Lundbom, N.; Rissanen, A.; Ridderstråle, M.; Groop, L.; et al. Prediction of non-alcoholic fatty liver disease and liver fat using metabolic and genetic factors. Gastroenterology 2009, 137, 865–872. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Soldati, L.; Bertoli, S.; Terranegra, A.; Brasacchio, C.; Mingione, A.; Dogliotti, E.; Raspini, B.; Leone, A.; Frau, F.; Vignati, L.; et al. Relevance of Mediterranean diet and glucose metabolism for nephrolithiasis in obese subjects. J. Transl. Med. 2014, 12, 34. [Google Scholar] [CrossRef]
- Bertoli, S.; Spadafranca, A.; Bes-Rastrollo, M.; Martinez-Gonzalez, M.A.; Ponissi, V.; Beggio, V.; Leone, A.; Battezzati, A. Adherence to the Mediterranean diet is inversely related to binge eating disorder in patients seeking a weight loss program. Clin. Nutr. 2015, 34, 107–114. [Google Scholar] [CrossRef]
- Amicis, R.D.; Leone, A.; Foppiani, A.; Osio, D.; Lewandowski, L.; Giustizieri, V.; Cornelio, P.; Cornelio, F.; Imperatori, S.F.; Cappa, S.F.; et al. Mediterranean Diet and Cognitive Status in Free-Living Elderly: A Cross-Sectional Study in Northern Italy. J. Am. Coll. Nutr. 2018, 37, 494–500. [Google Scholar] [CrossRef]
- Foschi, F.G.; Conti, F.; Domenicali, M.; Giacomoni, P.; Borghi, A.; Bevilacqua, V.; Napoli, L.; Berardinelli, D.; Altini, M.; Cucchetti, A.; et al. External Validation of Surrogate Indices of Fatty Liver in the General Population: The Bagnacavallo Study. J. Clin. Med. 2021, 10, 520. [Google Scholar] [CrossRef]
- Cohen, J.C.; Horton, J.D.; Hobbs, H.H. Human fatty liver disease: Old questions and new insights. Science 2011, 332, 1519–1523. [Google Scholar] [CrossRef]
- Arguello, G.; Balboa, E.; Arrese, M.; Zanlungo, S. Recent insights on the role of cholesterol in non-alcoholic fatty liver disease. Biochim. Et Biophys. Acta (BBA) Mol. Basis Dis. 2015, 1852, 1765–1778. [Google Scholar] [CrossRef]
- Donnelly, K.L.; Smith, C.I.; Schwarzenberg, S.J.; Jessurun, J.; Boldt, M.D.; Parks, E.J. Sources of fatty acids stored in liver and secreted via lipoproteins in patients with nonalcoholic fatty liver disease. J. Clin. Investig. 2005, 115, 1343–1351. [Google Scholar] [CrossRef]
- Speliotes, E.K.; Massaro, J.M.; Hoffmann, U.; Vasan, R.S.; Meigs, J.B.; Sahani, D.V.; Hirschhorn, J.N.; O’Donnell, C.J.; Fox, C.S. Fatty liver is associated with dyslipidemia and dysglycemia independent of visceral fat: The Framingham Heart Study. Hepatology 2010, 51, 1979–1987. [Google Scholar] [CrossRef] [PubMed]
- Duwaerts, C.C.; Maher, J.J. Mechanisms of Liver Injury in Non-Alcoholic Steatohepatitis. Curr. Hepatol. Rep. 2014, 13, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.; Guo, Z.; Johnson, C.M.; Hensrud, D.D.; Jensen, M.D. Splanchnic lipolysis in human obesity. J. Clin. Investig. 2004, 113, 1582–1588. [Google Scholar] [CrossRef]
- Sanders, F.W.; Griffin, J.L. De novo lipogenesis in the liver in health and disease: More than just a shunting yard for glucose. Biol. Rev. Camb. Philos. Soc. 2016, 91, 452–468. [Google Scholar] [CrossRef]
- Smith, G.I.; Shankaran, M.; Yoshino, M.; Schweitzer, G.G.; Chondronikola, M.; Beals, J.W.; Okunade, A.L.; Patterson, B.W.; Nyangau, E.; Field, T.; et al. Insulin resistance drives hepatic de novo lipogenesis in nonalcoholic fatty liver disease. J. Clin. Investig. 2020, 130, 1453–1460. [Google Scholar] [CrossRef]
- Tamura, S.; Shimomura, I. Contribution of adipose tissue and de novo lipogenesis to nonalcoholic fatty liver disease. J. Clin. Investig. 2005, 115, 1139–1142. [Google Scholar] [CrossRef]
- Lewis, G.F.; Carpentier, A.; Adeli, K.; Giacca, A. Disordered fat storage and mobilization in the pathogenesis of insulin resistance and type 2 diabetes. Endocr. Rev. 2002, 23, 201–229. [Google Scholar] [CrossRef]
- Gibbons, G.F.; Islam, K.; Pease, R.J. Mobilisation of triacylglycerol stores. Biochim. Biophys. Acta 2000, 1483, 37–57. [Google Scholar] [CrossRef]
- Fabbrini, E.; Mohammed, B.S.; Magkos, F.; Korenblat, K.M.; Patterson, B.W.; Klein, S. Alterations in adipose tissue and hepatic lipid kinetics in obese men and women with nonalcoholic fatty liver disease. Gastroenterology 2008, 134, 424–431. [Google Scholar] [CrossRef]
- Hennein, R.; Liu, C.; McKeown, N.M.; Hoffmann, U.; Long, M.T.; Levy, D.; Ma, J. Increased Diet Quality is Associated with Long-Term Reduction of Abdominal and Pericardial Fat. Obesity 2019, 27, 670–677. [Google Scholar] [CrossRef]
- Salomone, F.; Godos, J.; Zelber-Sagi, S. Natural antioxidants for non-alcoholic fatty liver disease: Molecular targets and clinical perspectives. Liver Int. 2016, 36, 5–20. [Google Scholar] [CrossRef]
- Abenavoli, L.; Milic, N.; Luzza, F.; Boccuto, L.; De Lorenzo, A. Polyphenols Treatment in Patients with Nonalcoholic Fatty Liver Disease. J. Transl. Int. Med. 2017, 5, 144–147. [Google Scholar] [CrossRef]
- Yang, J.; Fernández-Galilea, M.; Martínez-Fernández, L.; González-Muniesa, P.; Pérez-Chávez, A.; Martínez, J.A.; Moreno-Aliaga, M.J. Oxidative Stress and Non-Alcoholic Fatty Liver Disease: Effects of Omega-3 Fatty Acid Supplementation. Nutrients 2019, 11, 872. [Google Scholar] [CrossRef]
- Salomone, F.; Ivancovsky-Wajcman, D.; Fliss-Isakov, N.; Webb, M.; Grosso, G.; Godos, J.; Galvano, F.; Shibolet, O.; Kariv, R.; Zelber-Sagi, S. Higher phenolic acid intake independently associates with lower prevalence of insulin resistance and non-alcoholic fatty liver disease. JHEP Rep. 2020, 2, 100069. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Salomone, F.; Mlynarsky, L. The Mediterranean dietary pattern as the diet of choice for non-alcoholic fatty liver disease: Evidence and plausible mechanisms. Liver Int. 2017, 37, 936–949. [Google Scholar] [CrossRef]
- Bouzianas, D.G.; Bouziana, S.D.; Hatzitolios, A.I. Potential treatment of human nonalcoholic fatty liver disease with long-chain omega-3 polyunsaturated fatty acids. Nutr. Rev. 2013, 71, 753–771. [Google Scholar] [CrossRef]
- Masterton, G.S.; Plevris, J.N.; Hayes, P.C. Review article: Omega-3 fatty acids-a promising novel therapy for non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2010, 31, 679–692. [Google Scholar] [CrossRef]
- Rose, D.J. Impact of whole grains on the gut microbiota: The next frontier for oats? Br. J. Nutr. 2014, 112, S44–S49. [Google Scholar] [CrossRef]
- Guilloteau, P.; Martin, L.; Eeckhaut, V.; Ducatelle, R.; Zabielski, R.; Van Immerseel, F. From the gut to the peripheral tissues: The multiple effects of butyrate. Nutr. Res. Rev. 2010, 23, 366–384. [Google Scholar] [CrossRef]
- Al-Lahham, S.H.; Peppelenbosch, M.P.; Roelofsen, H.; Vonk, R.J.; Venema, K. Biological effects of propionic acid in humans; metabolism, potential applications and underlying mechanisms. Biochim. Biophys. Acta 2010, 1801, 1175–1183. [Google Scholar] [CrossRef]
- Hernández, E.; Kahl, S.; Seelig, A.; Begovatz, P.; Irmler, M.; Kupriyanova, Y.; Nowotny, B.; Nowotny, P.; Herder, C.; Barosa, C.; et al. Acute dietary fat intake initiates alterations in energy metabolism and insulin resistance. J. Clin. Investig. 2017, 127, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Bjermo, H.; Iggman, D.; Kullberg, J.; Dahlman, I.; Johansson, L.; Persson, L.; Berglund, J.; Pulkki, K.; Basu, S.; Uusitupa, M.; et al. Effects of n-6 PUFAs compared with SFAs on liver fat, lipoproteins, and inflammation in abdominal obesity: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 95, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Roumans, K.H.M.; Lindeboom, L.; Veeraiah, P.; Remie, C.M.E.; Phielix, E.; Havekes, B.; Bruls, Y.M.H.; Brouwers, M.; Ståhlman, M.; Alssema, M.; et al. Hepatic saturated fatty acid fraction is associated with de novo lipogenesis and hepatic insulin resistance. Nat. Commun. 2020, 11, 1891. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Tristan Asensi, M.; Pagliai, G.; Lotti, S.; Martini, D.; Colombini, B.; Sofi, F. Consumption of Ultra-Processed Foods Is Inversely Associated with Adherence to the Mediterranean Diet: A Cross-Sectional Study. Nutrients 2022, 14, 2073. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, R.D.; Pimenta, A.M.; Gea, A.; de la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Lopes, A.C.; Bes-Rastrollo, M. Ultraprocessed food consumption and risk of overweight and obesity: The University of Navarra Follow-Up (SUN) cohort study. Am. J. Clin. Nutr. 2016, 104, 1433–1440. [Google Scholar] [CrossRef]
- Konieczna, J.; Morey, M.; Abete, I.; Bes-Rastrollo, M.; Ruiz-Canela, M.; Vioque, J.; Gonzalez-Palacios, S.; Daimiel, L.; Salas-Salvadó, J.; Fiol, M.; et al. Contribution of ultra-processed foods in visceral fat deposition and other adiposity indicators: Prospective analysis nested in the PREDIMED-Plus trial. Clin. Nutr. 2021, 40, 4290–4300. [Google Scholar] [CrossRef]
- Leone, A.; Martínez-González, M.; Craig, W.; Fresán, U.; Gómez-Donoso, C.; Bes-Rastrollo, M. Pre-Gestational Consumption of Ultra-Processed Foods and Risk of Gestational Diabetes in a Mediterranean Cohort. The SUN Project. Nutrients 2021, 13, 2202. [Google Scholar] [CrossRef]
- Llavero-Valero, M.; Escalada-San Martín, J.; Martínez-González, M.A.; Basterra-Gortari, F.J.; de la Fuente-Arrillaga, C.; Bes-Rastrollo, M. Ultra-processed foods and type-2 diabetes risk in the SUN project: A prospective cohort study. Clin. Nutr. 2021, 40, 2817–2824. [Google Scholar] [CrossRef]
- Zhang, S.; Gan, S.; Zhang, Q.; Liu, L.; Meng, G.; Yao, Z.; Wu, H.; Gu, Y.; Wang, Y.; Zhang, T.; et al. Ultra-processed food consumption and the risk of non-alcoholic fatty liver disease in the Tianjin Chronic Low-grade Systemic Inflammation and Health Cohort Study. Int. J. Epidemiol. 2022, 51, 237–249. [Google Scholar] [CrossRef]
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; Martínez-González, M.A.; Castañer, O.; Bulló, M.; Corella, D.; Arós, F.; Gómez-Gracia, E.; et al. Mediterranean diets and metabolic syndrome status in the PREDIMED randomized trial. Can. Med. Assoc. J. 2014, 186, E649–E657. [Google Scholar] [CrossRef]
- Stolk, R.P.; Wink, O.; Zelissen, P.M.; Meijer, R.; van Gils, A.P.; Grobbee, D.E. Validity and reproducibility of ultrasonography for the measurement of intra-abdominal adipose tissue. Int. J. Obes. 2001, 25, 1346–1351. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).