
How Do the Different Types of Maternal Diabetes during Pregnancy Influence Offspring Outcomes?


Abstract
1. Introduction
2. Methods and Materials:
2.1. Literature Search and Data Extraction
2.2. Study Selection
- (1)
- Studies evaluating fetal exposure to at least two types of maternal diabetes, including GDM, pre-pregnancy T1D and T2D. Studies with unclear diabetes status were excluded.
- (2)
- At least one of the following offspring outcomes was used as primary or secondary endpoint: obesity, overweight, adiposity, glucose intolerance, diabetes, cardiovascular outcomes, metabolic syndrome, neurodevelopmental outcomes, autism, or attention deficit disorder.
- (3)
- Only randomized controlled trials and prospective or retrospective cohort studies were considered.
- (1)
- Studies with unclear diabetes status (i.e., when the term pregestational diabetes mellitus is used without specifying the type of diabetes).
- (2)
- Narrative reviews.
- (3)
- Systematic reviews and meta-analyses.
- (4)
- Studies evaluating pathophysiology rather than clinical outcomes.
2.3. Analysis
3. Results
3.1. Flow Chart
3.2. Risk of Overweight and Obesity in Offspring of Diabetic Mothers
3.3. Risk of Type 2 Diabetes or Abnormal Glucose Level
3.4. Risk of Type 1 Diabetes
3.5. Risk of Cardiovascular Disease and Metabolic Syndrome in Offspring from Diabetic Mothers

{kind=link}
{kind=link}
| Author, Year | Countries | Type of Study | Types of Diabetes (Sample Size) | Age at Follow Up | Outcomes | Outcomes with Adjustment |
|---|---|---|---|---|---|---|
| Clausen et al., 2009 [14] | Denmark | Prospective cohort | GDM (168) T1D (160) | 18–27 years | Risk for metabolic syndrome (OR 95%CI) GDM: 5.35 (2.31–12.42) T1D: 2.73 (1.12–6.64) | Adjusted risk for metabolic syndrome (OR 95%CI) a GDM: 4.12 (1.69–10.06) T1D: 2.59 (1.04–6.45) |
| Yu et al., 2019 [30] | Denmark | Population based cohort | GDM (26 272) T1D (22 055) T2D (6537) | Birth- 40 years | Risk for overall CVD (HR 95%CI) b GDM: 1.51 (1.36–1.67) T1D: 1.46 (1.34–1.59) T2D: 1.44 (1.27–1.62) Risk for Heart failure (HR 95%CI) GDM: 1.61 (0.72–3.60) T1D: 0.95 (0.40–2.29) T2D: 2.41 (1.08–5.38) Risk for hypertension (HR 95%CI) GDM: 2.50 (1.79–3.48) T1D: 1.81 (1.40–2.35) T2D: 2.29 (1.69–3.10) | Fully adjusted (HR 95%CI) c Risk for overall CVD GDM: 1.19 (1.07–1.32) T1D: 1.31 (1.20–1.43) T2D: 1.39 (1.23–1.57) Risk for Heart failure GDM: 1.54 (0.68–3.47) T1D: 0.95 (0.39–2.28) T2D: 2.32 (1.04–5.19) Risk for hypertension GDM: 1.77 (1.27–2.48) T1D: 1.57 (1.22–2.04) T2D: 2.18 (1.61–2.95) |
| Guillemette et al., 2020 [32] | Canada | Retrospective cohort | GDM (8210) T2D (3217) | 10–35 years | Adjusted risk for CVD (HR 95%CI) d GDM: 1.42 (1.12–1.79) T2D: 1.40 (0.98–2.01). Adjusted risk for CVD risk factors (HR 95%CI) GDM: 1.92 (1.75–2.11) T2D: 3.44 (2.89–4.11) |
3.6. Risk of Neurodevelopmental Disorders in Offspring from Diabetic Mothers
4. Discussion
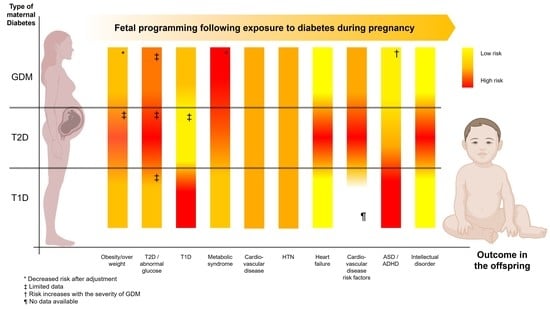
4.1. Summary of the Results (Table 6)
| Outcomes | Risk for the Offspring According to the Type of Maternal Diabetes |
|---|---|
| Overweight/obesity | Increased risk for all types of maternal diabetes No increased risk for O-GDM after adjustment for maternal BMI Limited data for O-T2D |
| T2D/abnormal glucose | Increased risk for all types of diabetes, limited data Risk for O-GDM > O-T1D Risk for O-T2D > O-GDM |
| T1D | Risk mainly increased for O-T1D |
| Metabolic syndrome | Risk X 2 for O-GDM versus O-T1D, limited data Moderate decrease in risk for O-GDM after adjustment for maternal BMI |
| Cardiovascular diseases | Similar increase in risk for all types of maternal diabetes |
| Hypertension | Similar increase in risk for all types of maternal diabetes |
| Heart failure | Risk X 2 only for O-T2D |
| Cardiovascular risk factors | Risk X 1.5 for O-T2D versus O-GDM |
| ASD/ADHD | Risk mainly increased for O-T1D and O-T2D Risk for O-T1D > O-T2D |
| Intellectual disorders | Increased risk for all types of maternal diabetes Risk X 2 for O-T2D versus O-GDM or O-T1D |
4.2. What This Study Adds Compared to Meta-Analyses?
4.2.1. Risk for Overweight and Obesity
4.2.2. Risk for Abnormal Glucose Levels and T2D
4.2.3. Risk for T1D in Offspring
4.2.4. Risk for Cardiovascular Diseases and Hypertension
4.2.5. Risk for Neurodevelopmental Disorders: Intellectual Disorders, ASD, and ADHD
4.3. Strengths and Limitations of the Method
4.4. What Information to Provide to Pregnant Women?
4.5. Are There Potential Identified Mechanisms?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADHD | attention deficit/hyperactivity disorders |
| ASD | autism spectrum disorders |
| BMI | body mass index |
| CVD | cardiovascular disease |
| DOHaD | Developmental Origins of Health and Disease |
| GDM | gestational diabetes mellitus |
| HbA1c | glycosylated hemoglobin |
| HR | hazards ratio |
| ICD | international classification of diseases |
| O-GDM | offspring of mothers with gestational diabetes mellitus |
| OGTT | oral glucose tolerance test |
| OR | odds ratio |
| O-T1D | offspring of mothers with type 1 diabetes |
| O-T2D | offspring of mothers with type 2 diabetes |
| RR | risk ratio |
| T1D | type 1 diabetes |
| T2D | type 2 diabetes |
References
- Gluckman, P.D.; Hanson, M.A.; Bateson, P.; Beedle, A.S.; Law, C.M.; Bhutta, Z.A.; Anokhin, K.V.; Bougnères, P.; Chandak, G.R.; Dasgupta, P.; et al. Towards a new developmental synthesis: Adaptive developmental plasticity and human disease. Lancet 2009, 373, 1654–1657. [Google Scholar] [CrossRef]
- Barker, D.J.; Gluckman, P.D.; Godfrey, K.M.; Harding, J.E.; Owens, J.A.; Robinson, J.S. Fetal nutrition and cardiovascular disease in adult life. Lancet 1993, 341, 938–941. [Google Scholar] [CrossRef]
- Hales, C.N.; Barker, D.J. The thrifty phenotype hypothesis. Br. Med. Bull. 2001, 60, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D.J.; Powell, T.L.; Barrett, E.S.; Hardy, D.B. Developmental origins of metabolic diseases. Physiol. Rev. 2021, 101, 739–795. [Google Scholar] [CrossRef]
- Dabelea, D.; Hanson, R.L.; Lindsay, R.S.; Pettitt, D.J.; Imperatore, G.; Gabir, M.M.; Roumain, J.; Bennett, P.H.; Knowler, W.C. Intrauterine exposure to diabetes conveys risks for type 2 diabetes and obesity: A study of discordant sibships. Diabetes 2000, 49, 2208–2211. [Google Scholar] [CrossRef]
- McGrath, R.T.; Glastras, S.J.; Hocking, S.L.; Fulcher, G.R. Large-for-gestational-age neonates in type 1 diabetes and pregnancy: Contribution of factors beyond hyperglycemia. Diabetes Care 2018, 41, 1821–1828. [Google Scholar] [CrossRef]
- Chu, A.H.Y.; Godfrey, K.M. Gestational diabetes mellitus and developmental programming. Ann. Nutr. Metab. 2020, 76, 4–15. [Google Scholar] [CrossRef]
- Agarwal, P.; Morriseau, T.S.; Kereliuk, S.M.; Doucette, C.A.; Wicklow, B.A.; Dolinsky, V.W. Maternal obesity, diabetes during pregnancy and epigenetic mechanisms that influence the developmental origins of cardiometabolic disease in the offspring. Crit. Rev. Clin. Lab. Sci. 2018, 55, 71–101. [Google Scholar] [CrossRef]
- Ornoy, A.; Reece, E.A.; Pavlinkova, G.; Kappen, C.; Miller, R.K. Effect of maternal diabetes on the embryo, fetus, and children: Congenital anomalies, genetic and epigenetic changes and developmental outcomes. Birth Defects Research. Part C Embryo Today Rev. 2015, 105, 53–72. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Fraser, A.; Lindsay, R.S.; Ness, A.; Dabelea, D.; Catalano, P.; Davey Smith, G.; Sattar, N.; Nelson, S.M. Association of existing diabetes, gestational diabetes and glycosuria in pregnancy with macrosomia and offspring body mass index, waist and fat mass in later childhood: Findings from a prospective pregnancy cohort. Diabetologia 2010, 53, 89–97. [Google Scholar] [CrossRef]
- Patel, S.; Fraser, A.; Davey Smith, G.; Lindsay, R.S.; Sattar, N.; Nelson, S.M.; Lawlor, D.A. Associations of gestational diabetes, existing diabetes, and glycosuria with offspring obesity and cardiometabolic outcomes. Diabetes Care 2012, 35, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Morgan, K.; Rahman, M.; Atkinson, M.; Zhou, S.M.; Hill, R.; Khanom, A.; Paranjothy, S.; Brophy, S. Association of diabetes in pregnancy with child weight at birth, age 12 months and 5 years--a population-based electronic cohort study. PLoS ONE 2013, 8, e79803. [Google Scholar] [CrossRef] [PubMed]
- Chivese, T.; Haynes, M.C.; van Zyl, H.; Kyriacos, U.; Levitt, N.S.; Norris, S.A. The influence of maternal blood glucose during pregnancy on weight outcomes at birth and preschool age in offspring exposed to hyperglycemia first detected during pregnancy, in a south african cohort. PLoS ONE 2021, 16, e0258894. [Google Scholar] [CrossRef] [PubMed]
- Clausen, T.D.; Mathiesen, E.R.; Hansen, T.; Pedersen, O.; Jensen, D.M.; Lauenborg, J.; Schmidt, L.; Damm, P. Overweight and the metabolic syndrome in adult offspring of women with diet-treated gestational diabetes mellitus or type 1 diabetes. J. Clin. Endocrinol. Metab. 2009, 94, 2464–2470. [Google Scholar] [CrossRef] [PubMed]
- Boerschmann, H.; Pflüger, M.; Henneberger, L.; Ziegler, A.G.; Hummel, S. Prevalence and predictors of overweight and insulin resistance in offspring of mothers with gestational diabetes mellitus. Diabetes Care 2010, 33, 1845–1849. [Google Scholar] [CrossRef]
- Pitchika, A.; Vehik, K.; Hummel, S.; Norris, J.M.; Uusitalo, U.M.; Yang, J.; Virtanen, S.M.; Koletzko, S.; Andrén Aronsson, C.; Ziegler, A.G.; et al. Associations of maternal diabetes during pregnancy with overweight in offspring: Results from the prospective teddy study. Obesity 2018, 26, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Sidell, M.; Martinez, M.P.; Chow, T.; Xiang, A.H. Types of diabetes during pregnancy and longitudinal bmi in offspring from birth to age 10 years. Pediatric Obes. 2021, 16, e12776. [Google Scholar] [CrossRef]
- Clausen, T.D.; Mathiesen, E.R.; Hansen, T.; Pedersen, O.; Jensen, D.M.; Lauenborg, J.; Damm, P. High prevalence of type 2 diabetes and pre-diabetes in adult offspring of women with gestational diabetes mellitus or type 1 diabetes: The role of intrauterine hyperglycemia. Diabetes Care 2008, 31, 340–346. [Google Scholar] [CrossRef]
- Kelstrup, L.; Damm, P.; Mathiesen, E.R.; Hansen, T.; Vaag, A.A.; Pedersen, O.; Clausen, T.D. Insulin resistance and impaired pancreatic β-cell function in adult offspring of women with diabetes in pregnancy. J. Clin. Endocrinol. Metab. 2013, 98, 3793–3801. [Google Scholar] [CrossRef]
- Nielsen, G.L.; Welinder, L.; Berg Johansen, M. Mortality and morbidity in offspring of mothers with diabetes compared with a population group: A danish cohort study with 8-35 years of follow-up. Diabet. Med. A J. Br. Diabet. Assoc. 2017, 34, 938–945. [Google Scholar] [CrossRef]
- Wicklow, B.A.; Sellers, E.A.C.; Sharma, A.K.; Kroeker, K.; Nickel, N.C.; Philips-Beck, W.; Shen, G.X. Association of gestational diabetes and type 2 diabetes exposure in utero with the development of type 2 diabetes in first nations and non-first nations offspring. JAMA Pediatrics 2018, 172, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Algert, C.S.; McElduff, A.; Morris, J.M.; Roberts, C.L. Perinatal risk factors for early onset of type 1 diabetes in a 2000-2005 birth cohort. Diabet. Med. A J. Br. Diabet. Assoc. 2009, 26, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Hussen, H.I.; Persson, M.; Moradi, T. Maternal overweight and obesity are associated with increased risk of type 1 diabetes in offspring of parents without diabetes regardless of ethnicity. Diabetologia 2015, 58, 1464–1473. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Lu, C.L.; Chen, H.F.; Su, H.F.; Li, C.Y. Perinatal and childhood risk factors for early-onset type 1 diabetes: A population-based case-control study in taiwan. Eur. J. Public Health 2015, 25, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Goldacre, R.R. Associations between birthweight, gestational age at birth and subsequent type 1 diabetes in children under 12: A retrospective cohort study in england, 1998-2012. Diabetologia 2018, 61, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Lindell, N.; Carlsson, A.; Josefsson, A.; Samuelsson, U. Maternal obesity as a risk factor for early childhood type 1 diabetes: A nationwide, prospective, population-based case-control study. Diabetologia 2018, 61, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Kvehaugen, A.S.; Andersen, L.F.; Staff, A.C. Anthropometry and cardiovascular risk factors in women and offspring after pregnancies complicated by preeclampsia or diabetes mellitus. Acta Obstet. Gynecol. Scand. 2010, 89, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.Q.; Collins, C.E.; Gordon, A.; Rae, K.M.; Pringle, K.G. The relationship between maternal obesity and diabetes during pregnancy on offspring kidney structure and function in humans: A systematic review. J. Dev. Orig. Health Dis. 2019, 10, 406–419. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome--a new world-wide definition. A consensus statement from the international diabetes federation. Diabet. Med. J. Br. Diabet. Assoc. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Yu, Y.; Arah, O.A.; Liew, Z.; Cnattingius, S.; Olsen, J.; Sørensen, H.T.; Qin, G.; Li, J. Maternal diabetes during pregnancy and early onset of cardiovascular disease in offspring: Population based cohort study with 40 years of follow-up. BMJ 2019, 367, l6398. [Google Scholar] [CrossRef]
- Guillemette, L.; Wicklow, B.; Sellers, E.A.C.; Dart, A.; Shen, G.X.; Dolinsky, V.W.; Gordon, J.W.; Jassal, D.S.; Nickel, N.; Duhamel, T.A.; et al. Intrauterine exposure to diabetes and risk of cardiovascular disease in adolescence and early adulthood: A population-based birth cohort study. CMAJ 2020, 192, E1104–E1113. [Google Scholar] [CrossRef] [PubMed]
- Guillemette, L.; Durksen, A.; Rabbani, R.; Zarychanski, R.; Abou-Setta, A.M.; Duhamel, T.A.; McGavock, J.M.; Wicklow, B. Intensive gestational glycemic management and childhood obesity: A systematic review and meta-analysis. Int. J. Obes. 2017, 41, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Norstedt, G.; Schalling, M.; Gissler, M.; Lavebratt, C. The risk of offspring psychiatric disorders in the setting of maternal obesity and diabetes. Pediatrics 2018, 142, e20180776. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Fallin, M.D.; Riley, A.; Landa, R.; Walker, S.O.; Silverstein, M.; Caruso, D.; Pearson, C.; Kiang, S.; Dahm, J.L.; et al. The association of maternal obesity and diabetes with autism and other developmental disabilities. Pediatrics 2016, 137, e20152206. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Nilsson, I.A.K.; Brismar, K.; Gissler, M.; Lavebratt, C. Associations of different types of maternal diabetes and body mass index with offspring psychiatric disorders. JAMA Netw. Open 2020, 3, e1920787. [Google Scholar] [CrossRef]
- Xiang, A.H.; Wang, X.; Martinez, M.P.; Walthall, J.C.; Curry, E.S.; Page, K.; Buchanan, T.A.; Coleman, K.J.; Getahun, D. Association of maternal diabetes with autism in offspring. Jama 2015, 313, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Xiang, A.H.; Wang, X.; Martinez, M.P.; Page, K.; Buchanan, T.A.; Feldman, R.K. Maternal type 1 diabetes and risk of autism in offspring. Jama 2018, 320, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Xiang, A.H.; Wang, X.; Martinez, M.P.; Getahun, D.; Page, K.A.; Buchanan, T.A.; Feldman, K. Maternal gestational diabetes mellitus, type 1 diabetes, and type 2 diabetes during pregnancy and risk of adhd in offspring. Diabetes Care 2018, 41, 2502–2508. [Google Scholar] [CrossRef]
- Chen, S.; Zhao, S.; Dalman, C.; Karlsson, H.; Gardner, R. Association of maternal diabetes with neurodevelopmental disorders: Autism spectrum disorders, attention-deficit/hyperactivity disorder and intellectual disability. Int. J. Epidemiol. 2021, 50, 459–474. [Google Scholar] [CrossRef]
- Philipps, L.H.; Santhakumaran, S.; Gale, C.; Prior, E.; Logan, K.M.; Hyde, M.J.; Modi, N. The diabetic pregnancy and offspring bmi in childhood: A systematic review and meta-analysis. Diabetologia 2011, 54, 1957–1966. [Google Scholar] [CrossRef]
- Kawasaki, M.; Arata, N.; Miyazaki, C.; Mori, R.; Kikuchi, T.; Ogawa, Y.; Ota, E. Obesity and abnormal glucose tolerance in offspring of diabetic mothers: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0190676. [Google Scholar]
- Hidayat, K.; Zou, S.Y.; Shi, B.M. The influence of maternal body mass index, maternal diabetes mellitus, and maternal smoking during pregnancy on the risk of childhood-onset type 1 diabetes mellitus in the offspring: Systematic review and meta-analysis of observational studies. Obes. Rev. 2019, 20, 1106–1120. [Google Scholar] [CrossRef] [PubMed]
- Aceti, A.; Santhakumaran, S.; Logan, K.M.; Philipps, L.H.; Prior, E.; Gale, C.; Hyde, M.J.; Modi, N. The diabetic pregnancy and offspring blood pressure in childhood: A systematic review and meta-analysis. Diabetologia 2012, 55, 3114–3127. [Google Scholar] [CrossRef] [PubMed]
- Hoodbhoy, Z.; Mohammed, N.; Nathani, K.R.; Sattar, S.; Chowdhury, D.; Maskatia, S.; Tierney, S.; Hasan, B.; Das, J.K. The impact of maternal preeclampsia and hyperglycemia on the cardiovascular health of the offspring: A systematic review and meta-analysis. Am. J. Perinatol. 2021; Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.; Ju, R.; Zhou, Q.; Mao, J.; Tao, H.; Jing, H.; Zhu, C.; Dai, J. Association of maternal diabetes with attention deficit/hyperactivity disorder (adhd) in offspring: A meta-analysis and review. Diabetes Res. Clin. Pract. 2020, 165, 108269. [Google Scholar] [CrossRef]
- Yamamoto, J.M.; Benham, J.L.; Dewey, D.; Sanchez, J.J.; Murphy, H.R.; Feig, D.S.; Donovan, L.E. Neurocognitive and behavioural outcomes in offspring exposed to maternal pre-existing diabetes: A systematic review and meta-analysis. Diabetologia 2019, 62, 1561–1574. [Google Scholar] [CrossRef]
- Xu, G.; Jing, J.; Bowers, K.; Liu, B.; Bao, W. Maternal diabetes and the risk of autism spectrum disorders in the offspring: A systematic review and meta-analysis. J. Autism Dev. Disord. 2014, 44, 766–775. [Google Scholar] [CrossRef]
- Zhao, L.; Li, X.; Liu, G.; Han, B.; Wang, J.; Jiang, X. The association of maternal diabetes with attention deficit and hyperactivity disorder in offspring: A meta-analysis. Neuropsychiatr. Dis. Treat. 2019, 15, 675–684. [Google Scholar] [CrossRef]
- Wan, H.; Zhang, C.; Li, H.; Luan, S.; Liu, C. Association of maternal diabetes with autism spectrum disorders in offspring: A systemic review and meta-analysis. Medicine 2018, 97, e9438. [Google Scholar] [CrossRef]
- Donovan, L.E.; Cundy, T. Does exposure to hyperglycaemia in utero increase the risk of obesity and diabetes in the offspring? A critical reappraisal. Diabet. Med. 2015, 32, 295–304. [Google Scholar] [CrossRef]
- Hillier, T.A.; Pedula, K.L.; Schmidt, M.M.; Mullen, J.A.; Charles, M.A.; Pettitt, D.J. Childhood obesity and metabolic imprinting: The ongoing effects of maternal hyperglycemia. Diabetes Care 2007, 30, 2287–2292. [Google Scholar] [CrossRef] [PubMed]
- Quaresima, P.; Visconti, F.; Interlandi, F.; Puccio, L.; Caroleo, P.; Amendola, G.; Morelli, M.; Venturella, R.; Di Carlo, C. Awareness of gestational diabetes mellitus foetal-maternal risks: An italian cohort study on pregnant women. BMC Pregnancy Childbirth 2021, 21, 692. [Google Scholar] [CrossRef] [PubMed]
- Armengaud, J.B.; Ma, R.C.W.; Siddeek, B.; Visser, G.H.A.; Simeoni, U. Offspring of mothers with hyperglycaemia in pregnancy: The short term and long-term impact. What is new? Diabetes Res. Clin. Pract. 2018, 145, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Petropoulos, S.; Guillemin, C.; Ergaz, Z.; Dimov, S.; Suderman, M.; Weinstein-Fudim, L.; Ornoy, A.; Szyf, M. Gestational diabetes alters offspring DNA methylation profiles in human and rat: Identification of key pathways involved in endocrine system disorders, insulin signaling, diabetes signaling, and ilk signaling. Endocrinology 2015, 156, 2222–2238. [Google Scholar] [CrossRef] [PubMed]
- Lamadrid-Romero, M.; Solís, K.H.; Cruz-Reséndiz, M.S.; Pérez, J.E.; Díaz, N.F.; Flores-Herrera, H.; García-López, G.; Perichart, O.; Reyes-Muñoz, E.; Arenas-Huertero, F.; et al. Central nervous system development-related micrornas levels increase in the serum of gestational diabetic women during the first trimester of pregnancy. Neurosci. Res. 2018, 130, 8–22. [Google Scholar] [CrossRef]

| Author, Years | Countries | Type of Study | Type of Diabetes (Sample Size) | Age at Follow-Up | Outcomes | Outcomes with Adjustments | |
|---|---|---|---|---|---|---|---|
| Clausen et al., 2009 [14] | Denmark | Prospective cohort | GDM (168) T1D (160) | 18–27 years | Risk for overweight (OR 95%CI) GDM: 2.09 (1.25–3.50) T1D: 2.15 (1.27–3.62) | Fully adjusted (OR 95%CI)a GDM: 1.79 (1.00–3.24) T1D: 2.27 (1.30–3.98) | |
| Boerschmann et al., 2010 [15] | Germany | Prospective cohort | GDM (231) T1D (757) | From 2 years to 11 years | Prevalence overweight GDM/T1D 2 years: 17.2%/15.8% 8 years: 20.2%/11.0% 11 years: 31.1%/15.8% | Prevalence overweight GDM obese/GDM non obese 2 years: 24.6%/9.2% 8 years: 36.4%/11.3% 11 years: 45.8%/11.9% | |
| Pitchika et al., 2018 [16] | US Germany Finland Sweden | Prospective cohort | GDM (326) T1D (225) T2D (14) | 0.25 to 6 years Median age at follow-up: 5.5 years | Risk for overweight (OR 95%CI) b GDM: 1.48 (1.14–1.92) T1D: 1.60 (1.16–2.20) T2D: 7.39 (2.46–22.23) Risk for obesity (OR) b GDM: 1.98 (1.34–2.93) T1D: 1.84 (1.09–3.10) T2D: 2.93 (0.65–13.22) | Adjusted for maternal pre-pregnancy BMI and GWG (OR 95%CI) c Risk for overweight GDM: 1.14 (0.86–1.51) T1D: 1.50 (1.08–2.09) T2D: 3.68 (1.14–11.81) Risk for obesity GDM: 1.33 (0.87–2.04) T1D: 1.75 (1.02–3.00) T2D: 0.94 (0.19–4.60) | Adjusted for maternal pre-pregnancy BMI, GWG and BW z-score (OR 95%CI) d Risk for overweight GDM: 1.10 (0.82–1.46) T1D: 1.15 (0.81–1.62) T2D: 4.92 (1.40–17.30) Risk for obesity GDM: 1.31 (0.85–2.01) T1D: 1.48 (0.85–2.59) T2D: 1.02 (0.20–5.09) |
| Sidell et al., 2021 [17] | USA (California) | Prospective cohort | Unmedicated GDM (12576) Medicated GDM (6982) T1D (537) T2D (7836) | From birth to 10 years Median age at follow-up: 5 years | Age (year) with BMI SD > 1 from reference category e Unmedicated GDM: 7 Medicated GDM: 4 T1D: 2 T2D: 2.5 | Fully adjusted age (year) for maternal pre-pregnancy BMI and GWG Unmedicated GDM: 9.5 Medicated GDM: 5 T1D: 4.5 TD2: 4.5 | |
| Author, Year | Countries | Type of Study | Type of Diabetes (Sample Size) | Age at Follow-Up | Outcomes | Outcomes with Adjustments |
|---|---|---|---|---|---|---|
| Clausen et al., 2008 [18] | Denmark Nordic Caucasian | Prospective cohort | GDM (168) T1D (160) | 18–27 years | Risk for abnormal glucose/T2D (OR 95%CI) GDM: 8.18 (2.83–23.67) T1D: 3.86 (1.27–11.81) | Risk for abnormal glucose/T2D (OR 95%CI) a GDM: 7.76 (2.58–23.39) T1D: 4.46 (1.38–14.46) |
| Nielsen et al., 2017 [20] | Denmark | Retrospective cohort | GDM (136) T1D (521) T2D (34) | 8 days–35 years Mean age at follow-up 21.5 years | Cumulative incidence of all types of diabetesn (95%CI) No diabetes: <20 years 0.51(0.47–0.55) <35 years 1.14 (1.04–1.26) T1D: <20 years 3.10 (1.62–5.36) <35 years 6.33 (3.97–9.98) GDM and T2D: <20 years 1.93 (0.52–5.12) <35 years 4.04 (1.45–8.79) | |
| Wicklow et al., 2018 [21] | Canada | Retrospective cohort | GDM: 4031 T2D: 3788 | >7 years up to 30 years Mean age at follow-up 17.7 years | Incidence rate/1000 persons/years for T2D GDM: 0.80 T2D: 3.19 Accelerated failure time * for T2D 95%CI GDM: 0.72 (0.65–0.61) T2D: 0.47 (0.44–0.57) |
| Author, Year | Countries | Type of Study | Rate of Type 1 Diabetes (Numbers/‰) or Number of Cases | Length of Follow-Up | Risk for DT1 in Early Childhood | Risk for DT1 in Early Childhood with Adjustments |
|---|---|---|---|---|---|---|
| Algert et al., 2009 [22] | Australia New South Wales | Retrospective cohort | 272/502,040 0.54‰ | Birth to 6 years | RR (95%CI) GDM: 1.2 (0.73–1.96) T1D: 6.33 (2.62–15.3) T2D: 0.0 (0.0–8.4) | |
| Hussen et al., 2015 [23] | Sweden | Retrospective cohort | 5771/1,176,155 4.9‰ | Birth to 18 years | Fully adjusted a (IRR (95%CI)) Both parents Nordic * GDM + T2D: 1.85 (1.53–2.23) T1D: 6.19 (5.30–7.23) Both parents non-Nordic GDM + T2D: 1.13 (0.67–1.92) T1D: 5.80 (2.57–13.08) | |
| Lee et al., 2015 [24] | Taiwan | Retrospective case-control study | Number of T1D: 632 Number of controls: 6320 | 3–8 years | OR (95%CI) GDM: 5.4 (3.62–8.50) T1D: 10.71 (0.67–171.86) T2D: 0.48 (0.21–1.01) | |
| Goldacre, 2018 [25] | England | Retrospective cohort | 2969/3,834,405 7.7‰ | Nine months to 12 years Median: 5.7 years | HR (95%CI) GDM: 1.3 (1.00–1.68) T1D: 7.55 (6.12–9.33) | |
| Lindell et al., 2018 [26] | Sweden | Retrospective case-control study | Number of T1D: 3231 Number of controls: 12,948 | 0–19 years | OR (95%CI) GDM: 1.78 (1.07–2.98) T1D: 5.13 (3.16–8.33) | Fully adjusted OR (95%CI) b GDM: 1.81 (1.08–3.04) T1D: 4.75 (2.19–7.75) |
| Author, Year | Country | Study Type | Type of Diabetes (Sample Size) | Follow Up | Outcomes | Outcomes with Adjustment |
|---|---|---|---|---|---|---|
| Xiang et al., 2015 [36] | USA (California) | Retrospective longitudinal cohort | GDM ≤ 26 weeks (7456) GDM > 26 weeks (17 579) T2D (6496) | 3–17 years median age at follow-up 5.5 years | ASD (HR 95%CI) (Adjusted for birth year) GDM at any age: 1.18 (1.04–1.33) GDM ≤ 26 weeks: 1.63 (1.35–1.97) GDM > 26 weeks: 0.98 (0.84–1.15) DT2: 1.59 (1.29–1.95) | Fully adjusted a (HR 95%CI) GDM at any age: 1.03 (0.90–1.17) GDM ≤ 26 weeks: 1.40 (1.14–1.72) GDM > 26 weeks: 0.86 (0.73–1.02) T2D: 1.30 (1.04–1.62) |
| Xiang et al., 2018 [37] | USA (California) | Retrospective longitudinal cohort | GDM ≤ 26 weeks (11 922) GDM > 26 weeks (24 505) T2D (9453) T1D (621) | 1–22 years median age at follow-up 6.9 years | ASD (HR 95%CI) b GDM ≤ 26 weeks: 1.30 (1.12–1.51) GDM > 26 weeks: 0.99 (0.88–1.12) T2D: 1.45 (1.24–1.70) T1D: 2.36 (1.36–4.12) | Fully adjusted c (HR 95%CI) GDM≤ 26 weeks: 1.26 (1.08–1.47) GDM > 26 weeks: 0.98 (0.87–1.10) T2D: 1.39 (1.18–1.62) T1D: 2.33 (1.29–4.21) |
| Xiang et al., 2018 [38] | USA (California) | Retrospective birth cohort | GDM (29 534) T2D (7822) T1D (522) | 4–18 years | ADHD (HR 95%CI) (Adjusted for birth year and random siblings) GDM: 0.94 (0.88–1.00) T2D: 1.40 (1.26–1.56) T1D: 1.97 (1.39–2.79) | Fully adjusted d (HR 95%CI) GDM: 1.02 (0.96–1.09) T2D: 1.43 (1.28–1.59) T1D: 1.56 (1.09 –2.25) |
| Chen et al., 2021 [39] | Sweden | Retrospective cohort | GDM (21 325) T1D (17 444) T2D (1679) | 6–29 years | OR 95%CI (Adjusted for birth year and sex) Any intellectual disorder: GDM: 1.68 (1.50–1.89) T2D: 3.57 (2.59–4.92) T1D: 1.91 (1.69–2.16) Any ADHD: GDM: 1.17 (1.10–1.25) T2D: 1.78 (1.44–2.19) T1D: 1.42 (1.33–1.53) Any ASD: GDM: 1.43 (1.32–1.56) T2D: 1.85 (1.39–2.48) T1D: 1.48 (1.35–1.63) | Fully adjusted e (OR 95%CI) Any intellectual disorder: GDM: 1.30 (1.15–1.46) T2D: 2.09 (1.53–2.87) T1D: 1.58 (1.40–1.79) Any ADHD: GDM: 1.16 (1.08–1.23) T2D: 1.43 (1.16–1.77) T1D: 1.21 (1.13–1.29) Any ASD: GDM: 1.30 (1.20–1.42) T2D: 1.37 (1.03–1.84) T1D: 1.29 (1.17–1.42) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eletri, L.; Mitanchez, D. How Do the Different Types of Maternal Diabetes during Pregnancy Influence Offspring Outcomes? Nutrients 2022, 14, 3870. https://doi.org/10.3390/nu14183870
Eletri L, Mitanchez D. How Do the Different Types of Maternal Diabetes during Pregnancy Influence Offspring Outcomes? Nutrients. 2022; 14(18):3870. https://doi.org/10.3390/nu14183870
Chicago/Turabian StyleEletri, Lina, and Delphine Mitanchez. 2022. "How Do the Different Types of Maternal Diabetes during Pregnancy Influence Offspring Outcomes?" Nutrients 14, no. 18: 3870. https://doi.org/10.3390/nu14183870
APA StyleEletri, L., & Mitanchez, D. (2022). How Do the Different Types of Maternal Diabetes during Pregnancy Influence Offspring Outcomes? Nutrients, 14(18), 3870. https://doi.org/10.3390/nu14183870