Abstract
Very preterm infants are at high risk for suboptimal nutrition in the first weeks of life leading to insufficient weight gain and complications arising from metabolic imbalances such as insufficient bone mineral accretion. We investigated the use of a novel set of standardized parenteral nutrition (PN; MUC PREPARE) solutions regarding improving nutritional intake, accelerating termination of parenteral feeding, and positively affecting growth in comparison to individually prescribed and compounded PN solutions. We studied the effect of MUC PREPARE on macro- and micronutrient intake, metabolism, and growth in 58 very preterm infants and compared results to a historic reference group of 58 very preterm infants matched for clinical characteristics. Infants receiving MUC PREPARE demonstrated improved macro- and micronutrient intake resulting in balanced electrolyte levels and stable metabolomic profiles. Subsequently, improved energy supply was associated with up to 1.5 weeks earlier termination of parenteral feeding, while simultaneously reaching up to 1.9 times higher weight gain at day 28 in extremely immature infants (<27 GA weeks) as well as overall improved growth at 2 years of age for all infants. The use of the new standardized PN solution MUC PREPARE improved nutritional supply and short- and long-term growth and reduced PN duration in very preterm infants and is considered a superior therapeutic strategy.
1. Introduction
About 1% of infants are born very preterm, i.e., before 32 week gestational age (GA) [1]. Despite significant advances in perinatal medicine that led to survival rates of up to 70% in the most immature infants [2], management of nutrition and postnatal growth remains a challenge in this high-risk patient population even for experienced perinatal centers.
Adequate nutritional support strategies for preterm infants are important for meeting their macro- and micronutrient needs for health growth and development and are related to the time to regain birth weight and prevalence of postnatal complications including the rate of necrotizing enterocolitis (NEC), nosocomial sepsis, and bronchopulmonary dysplasia (BPD) [3,4,5]. Importantly, substrate—in particular, higher protein—and energy intake during the first 7 days of life is associated with improved neurodevelopmental outcomes at 18 months of age [6,7]. In line with this, weight gain velocity during neonatal intensive care is associated with a significant positive effect on neurodevelopmental outcome and growth in the first years of life [8], with adequate nutrition and somatic growth revealing favorable effects on brain growth and white matter maturation [9]. Furthermore, early and aggressive introduction of enteral feeding was associated with improved growth developmental outcomes [6], even though the transition period of parenteral to enteral feeding is precarious and nutrient deficits can occur [10].
As a result, optimization of nutritional intake while compensating for immaturity-associated complications has become one of the most important goals in neonatal care [4,11,12,13,14,15,16,17,18,19] which requires the use of parenteral nutrition (PN) from day 1 of life in very preterm infants until sufficient enteral nutrition can be established [5]. Given the vulnerability of very preterm infants, the highest hygiene standards for both production and application of PN solutions must be met in this high-risk population [15].
Recommendations for PN in the very preterm infant changed significantly over the past years, requiring perinatal centers to adapt their PN regimen [20,21]. Next to training programs addressing composition and application of PN, standardized solutions emerged to meet nutritional needs and hygiene standards more broadly in the preterm population by reducing both delays and errors or inconsistencies when prescribing PN [22,23]. Standardized PN solutions for infants marketed by commercial companies, however, are not specifically designed to meet the needs of very preterm infants but are mostly designed to approximately meet the needs of a broader group of infants.
We therefore developed and evaluated standardized PN solutions (MUniCh PREterm PAREnteral solution (MUC PREPARE)), meeting the specific nutritional needs of very preterm infants in line with established recommendations [18,22,24]. We assessed the effect of our newly developed PN solutions on macro- and micronutrient intake, plasma electrolyte levels and metabolites, as well as somatic growth until discharge and at two years of age in very preterm infants in comparison to a historic reference group with matched pairs that had received individually designed PN solutions.
2. Materials and Methods
2.1. Study Population
The cohort comprises 116 very preterm infants ≤ 32 weeks GA born at the Perinatal Center of the University Hospital of Ludwig-Maximilians-Universität (LMU), Campus Grosshadern. Exclusion criteria were severe congenital malformations, chromosomal abnormalities, and metabolic diseases. Written informed parental consent was obtained for all study infants (AIRR study cohort: Munich #195-07, Munich # 492-15). The study was registered at the German Registry for Clinical Studies (DRKS00004600). Of the 116 infants, 58 preterm infants born between 24 January 2012 and 30 April 2014 were prospectively enrolled and received the standardized PN regimen (study cohort: median birth weight 989.3 g (interquartile range [IQR]: 722.5–1275 g)). A retrospectively recruited second cohort of 58 infants born between 17 January 2007 and 5 December 2009 was established based on pairs matched for gestational age, birth weight, birth weight percentile, gender, multiples, presence of infection at birth, grade of respiratory distress syndrome, intraventricular hemorrhage, and persistent ductus arteriosus (reference cohort: median birth weight 990.9 g (IQR: 745–1222.5 g)). Table 1 presents the demographic characteristics of the two patient cohorts and the respective subgroups divided by age. The two cohorts were similar for clinical characteristics and complications except for a higher BPD incidence in the study cohort (Fisher’s exact test p-value = 1.04 × 10−7).

Table 1.
Patient characteristics.
2.2. Development of the Standardized Parenteral Nutrition Solution MUC PREPARE
The standardized PN solution (Munich Preterm Parenteral feeding solution (MUC PREPARE)) was designed in cooperation with the Pharmacy of the University Hospital to fulfil the ESPGHAN (European Society for Paediatric Gastroenterology Hepatology and Nutrition) and ESPEN (European Society for Clinical Nutrition and Metabolic Care) guidelines [24] while achieving long-lived chemical and physical stability of its contents. The PN solutions are tailored to (i) meet the different stages of intake and fluid balance after birth [13,24] by the means of three different ranges of macro- and micronutrient concentrations and (ii) enable both peripheral and central venous application. Composition of the PN solutions furthermore addressed the rapidly changing nutritional needs including adaptations necessary due to expected complications in the first weeks of life. These prerequisites resulted in a total of nine standardized PN solutions MUC PREPARE (Table 2 and Table 3) together with three solutions containing commercial fat emulsions and vitamins (Table 4 and Table 5). Solution 1 is designed for the first day of life allowing for a reduced supply of macro- and micronutrients and overall fluid intake as recommended. Solution 2 is designed for increased parenteral supply of macro- and micronutrients in infants exhibiting significant intra- and interindividual variability in the parenteral supply needed due to fluid and metabolic imbalance and clinically critical conditions. Solution 3 is designed to meet stabilized conditions that allow for the transition to enteral feeding. In order to allow for optimal protein supply in infants with slightly restricted carbohydrate supply due to hyperglycemia, the solutions for central venous application were divided into “G(+)” and “G(−)” referring to different glucose concentrations. Each infusion is composed of one main infusion bag that can be combined with different bypass solutions for additional amino acid, glucose, or water supply. Trace element solutions are delivered in a syringe and added to the main infusion bag right before application. The standardized PN solutions furthermore fulfil the requirements of the updated ESPGHAN guidelines [18,22], that recommend a lower calorie intake (45–55 kcal/kg bw/day) in the first days of life, followed by an increase to 90–120 kcal/kg bw/day in the intermediate phase based on a presumed lower energy consumption due to low amounts of enteral feeding.
Table 2.
‘NeoPeri’ and ‘NeoZent’ solutions containing amino acids, glucose, electrolytes, and trace elements, supply per kg bodyweight per day.
Table 3.
‘NeoPeri’ and ‘NeoZent’ solutions containing amino acids, glucose, electrolytes, and trace elements, supply per 100 mL solution.
Table 4.
‘NeoFett’ solutions, containing fat and vitamins, supply per kg bodyweight per day.
Table 5.
‘NeoFett’ solutions, containing fat and vitamins, supply per 100 mL.
2.3. Parenteral Nutrition
Application of PN for both study groups followed the ESPGHAN guidelines for pediatric PN published in 2005 supported by a structured recommendation plan displayed at the desk of the prescribing physician. All prescriptions were carried out with the software ‘Visite2000′ [25]. Every prescribing physician received a 2-week training prior to the first prescription, followed by update training twice a year and continuous supervision through a senior attending neonatologist. PN was prescribed every morning and prepared by the Pharmacy of the University Hospital according to Annex 1, EUGMP (Good Manufacturing Practice) guidelines. All PN nutrition regimens contained the solutions outlined above including fat emulsion (Table 2 and Table 3) until enteral feeding contained the macronutrient intake recommended. While the study cohort (n = 58) received standardized PN solutions as outlined above (Table 2, Table 3, Table 4 and Table 5), the reference cohort (n = 58) received individually designed and compounded PN solutions. Both standardized and individual PN solutions were adapted with respect to volume and electrolyte content as clinically indicated.
2.4. Enteral Feeding
Enteral feeding was initiated on the first day of life along with PN in all study infants and based on fortified own mothers’ milk or donor milk (fortifier FM 85 (Nestlé, Frankfurt M, Germany) or, in case human milk was not available, preterm formula (study cohort: Aptamil Prematil [Milupa, Friedrichsdorf, Germany], reference cohort: Beba FG [Nestlé, Frankfurt M, Germany])). Enteral feeding was adjusted according to ESPGHAN recommendations as available at the time (study cohort [26], reference cohort [27], Supplementary Table S1, overview of differences between cohorts, Supplementary Table S2, Summary table of provided nutrients). Iron supplementation was initiated when enteral feeding exceeded 75% of recommended energy intake.
2.5. Clinical Monitoring
Data collection was performed at 8 timepoints (days of life 1, 3, 7, 14, 21, and 28 and respective age of 32- and 36-weeks GA) and comprised the following variables: intake of total fluids, calories, carbohydrates, proteins, lipids, and electrolytes via parenteral (and enteral) feeding. Nutritional supply composition was expressed with respect to the ratio enteral/parenteral (% of total mL). Serum parameters monitored included glucose, sodium, potassium, lactate, calcium, phosphate, and magnesium, all of which were determined by blood gas analysis (ABL-Radiometer, Copenhagen, Denmark) every day to twice a week. Organ function and infections were assessed by weekly analysis of differential blood count, C-reactive protein, liver parameters, and creatinine. Blood triglycerides were measured once or twice a month depending on routine blood work and signs of metabolic imbalance. In addition, acute and chronic complications were monitored: early onset and late onset neonatal infection, respiratory distress syndrome (RDS), intraventricular hemorrhage (IVH), and persistent ductus arteriosus (PDA) (Table 1). Growth parameters were assessed by the attending intensive care nurse using standardized procedures and calibrated scales; relative growth was calculated using standardized growth percentile charts, i.e., weight-for-age z-score charts [28]. Weight gain [g], growth of head circumference (HC (cm)) and body length (BL (cm)) were calculated as a percentage of the observed parameters at day 28 to birth. Somatic growth, i.e., weight gain, growth of head circumference, and body length was reassessed at 24 months and corrected for degree of prematurity.
2.6. Metabolomics
Levels of 397 metabolites (amino acids, biogenic amines, lipids, and acylcarnitines) in blood plasma samples of 22 infants (study cohort: median: 2.5 days of life, range: 0–30) were measured by ultra-high-performance LC tandem mass spectrometry (UPLC-MS/MS; BioMedical Metabolomics Facility Leiden at the Leiden University). Relative abundances of the metabolites were reported and log2 transformed prior to statistical analysis. After exclusion of metabolites (n = 138) and/or samples (n = 3) with >20% missingness, a total of 259 metabolites and 19 samples were analyzed. Remaining missing values were imputed using kNN-based imputation [29], and one outlier detected in the PCA analysis was removed. Association of metabolite levels with changes in nutritional intake (macronutrients including total fluid and total calorie intake, percentage of carbohydrate, fat and protein to overall calorie consumption, concentration of added micronutrients (natrium, potassium, calcium, magnesium, chloride, and phosphate)) was analyzed by linear regression correcting for gender and GA. All p-values were corrected for multiple testing using the Benjamini–Hochberg procedure [30].
2.7. Statistical Analyses
Nutritional intakes, serum, and urinary excretion levels for electrolytes over the first two weeks of life were calculated for parenteral and enteral nutrition regimen per (i) individual patient, (ii) cohort, and (iii) GA subgroups (< or >27 weeks GA). Parenteral and enteral nutrition was expressed as the mean percentage of total supply at each time point. A sample was labelled as belonging to either the parenteral or enteral nutrition regimen when the respective nutritional supply exceeded 50% of the total fluid intake. Group differences were calculated using the Wilcoxon rank sum test. Feature selection of nutritional and clinical variables for growth parameters was performed using lasso regression with the primary outcome ‘growth’ (in relation to birth values). Pearson correlations were used to compare percentile values. Analysis was performed in all infants with further stratification for GA, i.e., < or >27 weeks GA. Standard infusion solutions and SOPs are detailed in the supplementary material and summarized in Table 2, Table 3, Table 4 and Table 5 (composition of the MUC PREPARE solutions).
3. Results
Preterm infants in the study and the reference cohort were well matched for clinical characteristics such as GA, birth weight, gender, and presence of infection. No significant difference between the two cohorts was observed for critical perinatal variables.
3.1. Improved Early Postnatal Energy and Nutrient Supply with the Standardized PN Solution MUC PREPARE in Very Premature Infants
Application of the standardized PN solution MUC PREPARE based on the ESPGHAN guidelines resulted in overall comparable fluid intake that only differed at day 1 (10% higher in the study cohort, p = 1.03 × 10−6, Figure 1a). Infants who received the standardized PN solution MUC PREPARE received more than 1.5-fold higher amino acid and up to 1.5 times more energy intakes on day 1 (FC 1.5, p < 2.2 × 10−16) and day 3 of life (FC 1.2, p = 8.26 × 10−10, Figure 1b), in line with a 5-fold increase in the number of infants meeting the recommended nutrient intake in this group (n = 17 of 55 (study cohort, 2012–14) vs. n = 3 of 53 (reference cohort, 2007–09); day 3 of life). The updated ESPGHAN guidelines differing in recommended calorie intake in the first days of life are met in the study cohort received with an average intake of 46.06 ± 8.22, 81.93 ± 9.00, and 97.36 ± 13 on days 1, 3, and 7 of life, respectively.
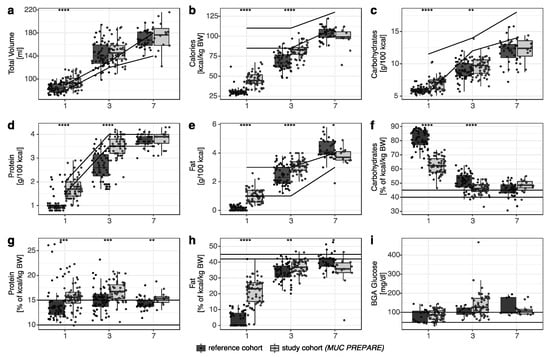
Figure 1.
Comparison between the reference cohort (dark grey) and the study cohort (light grey; MUC PREPARE) for (a) total volume (mL), (b) calories (kcal/kg BW), supply shown in g/100 kcal for (c) carbohydrates, (d) protein, and (e) fat, (f–h) supply expressed as percentage of total calorie intake supply. (i) BGA glucose levels (mg/dL). Recommendations are shown as horizontal lines (ESPGHAN 2005 [24]). * p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001. Study cohort (MUC PREPARE): 2012–2014, reference cohort: 2007–2009.
The amino acid and higher energy intake in the first 3 days of life (Figure 1b) resulted from a balanced increase in all three macronutrients with significantly increased amino acid, lipid, and glucose intake in the MUC PREPARE study group until day 3 of life when compared to the reference cohort (Figure 1c–e, Supplementary Table S3).
Balanced energy supply was furthermore reflected by the significantly increased number of infants that reached the recommended relation of carbohydrate to total calorie intake (40–45% of kcal/kg BW) in the study group as early as day 3 of life (30% (study cohort) vs. 9% (reference cohort), p-value = 6.52 × 10−7, Figure 1f). The number of infants that reached the recommended protein supply was higher in infants receiving the standardized PN solution (day 1: 15.63% (study cohort) vs. 14.41% (reference cohort); day 3: 16.72% (study cohort) vs. 15.13% (reference cohort), Figure 1g). The number of infants that reached the recommended lipid supply was up to 5-fold higher when infants received the standardized PN solution at day 1 and day 3 of life (day 1: 21.3% (study cohort (MUC PREPARE)) vs. 4.1% (reference cohort); day 3: 36.9% (study cohort) vs. 33.7% (reference cohort), Figure 1h).
Regarding the electrolytes sodium, potassium, and phosphate, intake was increased in the first three days of life when standardized PN solutions were received, while magnesium and calcium intake were marginally reduced at day 1 of life (Figure 2a–f, Supplementary Table S4).
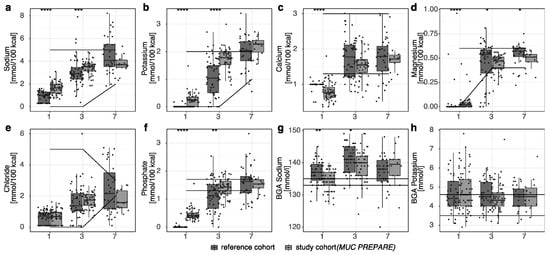
Figure 2.
(a–f) Electrolyte supply in the parenteral diet regimens. (g,h) Serum levels of sodium and potassium. Recommendations shown as horizontal lines (ESPGHAN 2005 [24]). * p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001. Study cohort (MUC PREPARE): 2012–2014, reference cohort: 2007–2009.
3.2. Balanced Indicators of Metabolism with Standardized PN Solution
Despite the increased intake of carbohydrates, blood glucose concentrations did not differ (Figure 1i) significantly between the study and the reference cohort. Likewise, pH levels did not differ significantly between the two cohorts. As a critical readout for bone metabolism, calcium and phosphate supply and excretion levels were monitored and demonstrated a reduced variability of the relative calcium to phosphate intake in the standardized PN solution cohort (study cohort (MUC PREPARE): 1.30 ± 0.17 vs. reference cohort: 1.89 ± 0.67; mean ± SD; Leven test p-value: 5.81 × 10−6). Serum sodium levels were decreased in the first three days of life in the study cohort (Figure 2g), while potassium (Figure 2h), and phosphate (not shown) were comparable between the study and the reference cohort.
Metabolomic profiles in the study cohort were not altered by the prevalence of infection, both early and late onset, RDS, BPD, or nutritional intake, i.e., total volume (mL), calories, macronutrient supply, i.e., lipid, protein, and carbohydrate supply all expressed as either g/kg or % of total calorie intake, and micronutrient supply, i.e., natrium, magnesium, and chloride supply. We did show, however, significant inverse correlations of phenylalanine and alpha-aminobutyric acid levels with calcium, potassium, and phosphate intake after correcting for multiple testing using FDR. In addition, phenylalanine was inversely correlated with total carbohydrate intake (g/kg) (Figure 3). There was no correlation of phenylalanine to protein intake and total volume; negative associations with lipid intake (β = 2.19, p = 0.00088, FDR adjusted p = 0.23) and calorie intake (β = −39.28, p = 0.0005, FDR adjusted p = 0.13) did not remain significant after multiple testing.
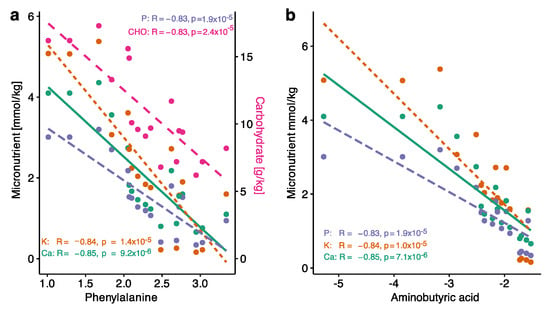
Figure 3.
Scatterplots of Pearson correlations of (a) phenylalanine with calcium, potassium, phosphate, and carbohydrate (g/kg) intake levels and (b) of ABA with calcium, potassium, and phosphate levels. All p-values were significant after FDR.
3.3. Improved Rate of Enteral Feeding and Postnatal Growth with Standardized PN Solutions
All infants in the standardized PN cohort achieved earlier enteral feeding (75% of total fluid intake; study cohort (MUC PREPARE): 10.6 ± 3.6 days; reference cohort: 17.2 ± 6.6 days; mean ± SD, p = 1 × 10−8, Supplementary Figure S1A) and earlier termination of any PN (study cohort: 17.4 ± 11.7 days; reference cohort: 22.4 ± 12.7 days (mean ± SD), p = 0.038, Supplementary Figure S1B). Infants receiving the MUC PREPARE achieved 75% enteral feeding on average 4 days (27–32 weeks GA) and 1.5 weeks (<27 weeks GA) earlier when compared to the infants that received individual PN (<27 weeks GA: study cohort: 11.3 ± 3.5 days; reference cohort: 20.6 ± 7.1 days; p = 9.5 × 10−6, 27–32 weeks GA: study cohort: 10.4 ± 3.6 days; reference cohort: 14.9 ± 5.1 days; p = 9.5 × 10−5; all values mean and SD; Figure 4a).
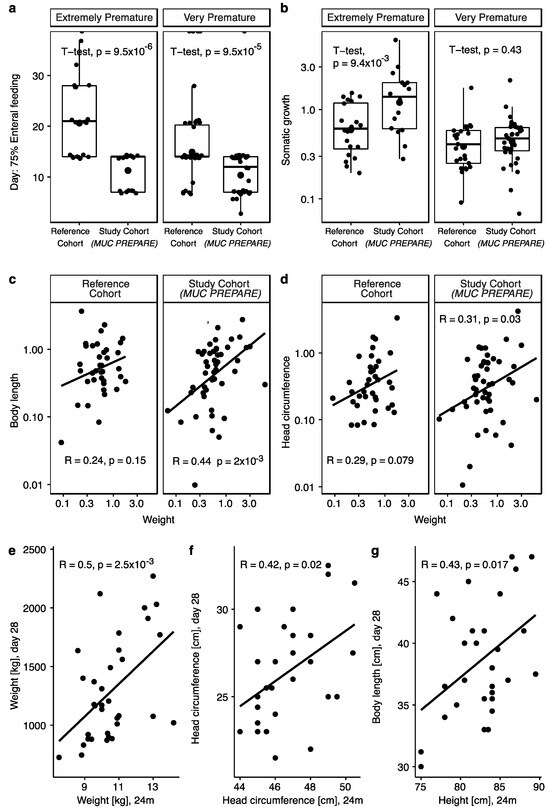
Figure 4.
(a) Days of life by when infants achieved 75% enteral feeding in percentage of total volume (mL) given separated by immaturity. (b) Somatic growth calculated as change in percentiles at day of birth and day 28 of life separated by immaturity. (c,d) Scatterplots showing Pearson correlations of weight with (c) body length and (d) head circumference separated by cohort. (e–g) Scatterplots showing Pearson correlations over both cohorts in available data showing that the (e) body weight (kg), (f) head circumference (cm), and (g) height/body length (cm) correlate with the respective values at 24 months. Extremely immature: <27 GA weeks, very premature: 27–32 GA weeks. Study cohort (MUC PREPARE): 2012–2014, reference cohort: 2007–2009.
Regarding somatic growth, infants that received standardized PN solutions (MUC PREPARE) showed significantly improved weight gain when compared to the reference cohort, with most significant effects in the most premature infants (study cohort: 1.63 ± 1.42; reference cohort: 0.72 ± 0.45 (difference in percentiles at day of birth and day 3 of life; mean ± SD), p = 0.0094; Figure 4b). There was no significant difference in initial weight loss between the two cohorts independent of immaturity at birth. Feature selection showed that—regardless of cohort—the main factor influencing weight gain and body length growth was gestational age, while prematurity was a factor for body length where the younger infants grew more (Supplementary Table S5).
In the study cohort with standardized PN (MUC PREPARE), weight gain was correlated with an increase in body length (R = 0.44, p = 0.002, Figure 4c) and head circumference (R = 0.31, p = 0.03; Figure 4d), in contrast to the lack of correlation in the reference cohort.
Growth parameters at 28 days of life in the study cohort correlated significantly with the respective growth parameter at 24 months corrected age (weight (R = 0.5, p = 0.0025), body length/height (R = 0.43, p = 0.017), head circumference (R = 0.42, p = 0.02)) (Figure 4e–g). Supplementary Table S5 summarizes the results.
4. Discussion
The aim of standardizing PN is to increase patient safety and to optimize resource efficiency by minimizing procedural incidents when providing PN to meet recommendations and individual patient needs [31]. To address these vital issues, guidelines, and recommendations for PN of preterm infants have continued to change and evolve over the past decades, requiring perinatal centers to adapt their infusion regimens accordingly [18,20,21,22,32] while meeting increasingly higher hygiene standards.
In a representative cohort of preterm infants, we demonstrated that our standardized PN solutions for preterm infants MUC PREPARE resulted in an improved energy and macro- as well as micronutrient intake meeting international recommendations [24]. Optimized PN resulted in a balanced metabolic profile, earlier enteral nutrition, and improved somatic growth.
While commercially available PN solutions for infants generally cover the needs of a broader range of age groups and diseases and are not adapted to the different postnatal growth phases, we have developed standardized PN solutions especially for the growing, high-risk cohort of patients after premature birth (Munich Preterm Parenteral feeding solution (MUC PREPARE)). The ‘one-fits-all’ policy of commercial products often requires either an increase in fluid intake or a restriction of energy or micronutrient intake when conditions are critical after preterm birth. Most of these commercial solutions are designed for administration via central infusion lines [33] or require individual dilution of the solution, thereby risking calculation errors and/or non-optimal macro- and micronutrient intake. The need for adding vitamins and micronutrients to the commercial solutions also increases the likelihood of calculation errors and hygienic risks [34]. The MUC PREPARE solutions enable standardized, but individually adaptable nutrition in the first weeks of life through nine different formulations and meet the highest quality criteria regarding nutrient content and application safety. In contrast to commercially available nutrition solutions, our PN solutions are adapted to the higher macro- and micronutrient requirements with the simultaneous restriction of fluid intake, characteristic for infants with significant immaturity.
4.1. Improved Early Postnatal Energy and Nutrient Supply with the Standardized PN Solution MUC PREPARE in Very Preterm Infants
Postnatal nutrient intake is crucial for somatic growth [35]. Improved nutrient intake not only leads to a faster regain of birth weight but was shown to improve somatic growth including body weight and head circumference until term in infants with a birth weight of less than 1500 g [36]. Even small differences in the supply of macro- and micronutrients were shown to have significant effects on growth and metabolism [37,38] best exemplified by studies demonstrating that protein intake the first week of life determines insulin sensitivity through epigenetic changes [39] and significantly affects cognitive performance at 18 months of age [40].
Without increasing overall fluid intake, MUC PREPARE was able to improve nutritional intake according to the ESPGHAN recommendations [24] when compared to the group of infants receiving individually prescribed PN. This included a higher calorie intake and a balanced increase in macronutrient supply leading to significantly increased carbohydrate, protein, and lipid intakes (g/kg) as early as day three of life. Here, especially improved amino acid intake critically impacts on somatic and organ growth but requires improved levels of overall macronutrient intake to balance energy consumption and to ensure adequate growth in preterm infants at the same time. This is in line with previous publications favoring a standardized PN regimen [34,37,41,42]. In contrast to these studies, however, MUC PREPARE resulted in a higher calorie intake [43] and improved growth shown across a large set of study time points [41,42] and even meets updated ESPGHAN recommendations [18]. In addition, micronutrient intake was increased, and serum levels showed less fluctuations under MUC PREPARE PN in comparison to the reference cohort. Stabilization of micronutrient intake as achieved when receiving MUC PREPARE is important when considering publications demonstrating deranged electrolyte levels and later disease development, specifically when considering sodium intake in preterm infants and the later development of arterial hypertension [44]. When considering critical goals for bone growth and mineral density in preterm infants [45,46,47,48], calcium and phosphate intake and excretion were stabilized and more likely within the recommended calcium/phosphate ratio of 1.3–1.7 [43] when receiving MUC PREPARE, in line with recommendations from ESPGHAN and the American Academy of Pediatrics, despite the actual supply being still lower than currently recommended.
4.2. Balanced Metabolomic Profile with the Use of a Standardized PN Solution
Despite increased macronutrient intake, blood glucose concentrations and pH levels did not differ significantly between the study and reference cohorts, indicating a balanced metabolism, reflecting previous studies [49,50]. The metabolic profile, including amino acids, biogenic amines, lipids, and acylcarnitines, was unaffected by the remaining variability of nutrient intake within MUC PREPARE study infants. In contrast to other studies, postnatal complications or degree of immaturity did not alter the metabolomic profiles [51]. The only exception were differentially co-regulated levels of the amino acids alpha-aminobutyric acid and phenylalanine with macro- and micronutrient intake, in line with previous studies indicating negative correlations with energy supplementation [52] but indicating lower risk profiles for morbidity and mortality [53,54,55] in infants with optimized PN at the same time.
4.3. Improved Rate of Enteral Nutrition and Postnatal Growth with Standardized PN Solutions
Referring to the two most important outcome measures, we demonstrated a reduced time until full enteral feeding as well as improved weight gain in infants receiving optimized PN with MUC PREPARE. Early enteral feeding is known to reduce complications caused by parenteral infusion therapy [21] and to increase postnatal energy intake and weight gain [56]. The beneficial effects of adequate weight gain related to expected growth in utero include lower rates of complications of necrotizing enterocolitis (NEC), bronchopulmonary dysplasia (BPD), and nosocomial sepsis [3,4], as well as improved neurological outcome until preschool age [8,57,58] and a reduced rate of metabolic diseases in adulthood [59,60]. Notably, the beneficial effects on weight gain were most pronounced in the most immature infants and, in addition, were long lasting when growth parameters were followed up to 2 years of age. The correlations of body length and head circumference to weight gain reflects balanced somatic growth and underlines the lasting effects of nutrition in this group.
The limited number of patients studied is due to the character of the cohort including only very preterm infants. The limitation was counteracted by the homogeneity of each cohort due to pairwise matching as shown by the significant comparability for perinatal complications between the study and the reference cohort. Despite possible differences in postnatal care in general and changes in mechanical ventilation duration in the study cohort, this difference must be considered when interpreting study results (study cohort (MUC PREPARE), reference cohort). A second limitation is the changes in the number of parenterally fed infants over time, with an increasing number of infants achieving full enteral feeding as expected, particularly in the study cohort. This must be considered when interpreting the results from day 7 onwards, but at the same time reflects a significant advantage of the standardized PN regimen.
5. Conclusions
In summary, the standardized infusion regimen MUC PREPARE appears to be safe and beneficial for meeting nutrient needs and supporting growth, when compared to individually prescribed and compounded PN. We demonstrated a significant increase in energy and macro- and micronutrient supply together with a balanced metabolic profile, earlier achievement of full enteral nutrition, and improved short- and long-term growth. The standardized infusion concept is thus recommended for clinical use as a superior PN strategy in very preterm infants [61]. Broad application of standardized PN concepts may also facilitate comparability between perinatal centers and thereby improve outcome assessment in multicentric clinical trials.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu14193912/s1, Table S1: Overview of recommendations per reference cohort and feeding mode; Table S2: Summary table of provided nutrients; Overview of all macro- and micronutrients measurements available over all timepoints and infants that are below, within, and above the excretion guidelines per age group and birth cohort. The recommendations are outlined against the birth cohorts and values investigated, as they increased over the years; Table S3: Overview of fold changes, means, SD and n for each variable shown in Figure 1; Table S4: Overview of fold changes, means, SD and n for each variable shown in Figure 2; Table S5: Overview of feature selection. Figure S1A: Day of 75% enteral feeding, Figure S1B: Day of 100% enteral feeding.
Author Contributions
Conceptualization, Y.K., J.B. and A.H.; data acquisition, Y.K., F.H., A.W.F., S.H.-J. and H.W.; methodology, Y.K., A.K., L.D.R. and K.M.F.; formal analysis, A.K.; investigation, Y.K., A.K. and A.H.; resources, A.H.; data curation, Y.K.; writing–original draft preparation, A.H.; writing—review and editing, Y.K., A.K., L.D.R., B.K., T.H., N.A., J.K. and A.H.; visualization, A.K., L.D.R., and A.H.; supervision, A.H.; project administration, A.H. All authors have read and agreed to the published version of the manuscript. A.K. carried out the analyses, reviewed and revised the manuscript; Y.K. conceptualized and designed the study, designed the data collection instruments, collected data, and reviewed and revised the manuscript; F.H. H.W. acquired data; L.D.R. performed the metabolomic data analysis, reviewed and revised the manuscript; K.M.F. coordinated and supervised data collection, and critically reviewed the manuscript for important intellectual content; A.W.F. and S.H.-J. collected data, and reviewed and revised the manuscript; J.B. conceptualised and designed the study, reviewed and revised the manuscript; B.K., T.H., N.A. and J.K. contributed to the drafting of the manuscript for important intellectual content. A.H. conceptualized and designed the study, coordinated, and supervised data collection, drafted the initial manuscript, and critically reviewed the manuscript for important intellectual content.
Funding
Funded by the Helmholtz Association, grant number NWG VH-NG-829, German Center for Lung Research (Federal Ministry of Science). BK is the Else Kröner Seniorprofessor of Paediatrics at LMU—University of Munich, financially supported by Else Kröner-Fresenius-Foundation, LMU Medical Faculty and LMU University Hospitals.
Institutional Review Board Statement
Approval by the local Ethics Committee and written informed parental consent for the study infant was obtained (Munich cohort #195-07; German Registry for Clinical Studies DRKS00004600). All methods were performed in accordance with the relevant guidelines and regulations of the local Ethics Committee and the declaration of Helsinki.
Informed Consent Statement
Written informed parental consent was obtained for all study infants (AIRR study cohort: Munich #195-07, Munich #492-15).
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy reasons.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Blondel, B.; Papiernik, E.; Delmas, D.; Künzel, W.; Weber, T.; Maier, R.; Kollée, L.; Zeitlin, J.; Mosaic Research Group. Organisation of Obstetric Services for Very Preterm Births in Europe: Results from the MOSAIC Project: Models of Regionalisation in Europe for Very Preterm Births. BJOG Int. J. Obstet. Gynaecol. 2009, 116, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Lawn, J.E.; Davidge, R.; Paul, V.K.; von Xylander, S.; de Graft Johnson, J.; Costello, A.; Kinney, M.V.; Segre, J.; Molyneux, L. Born Too Soon: Care for the Preterm Baby. Reprod. Health 2013, 10, S5. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.; Sosenko, I.R.S. Undernutrition as a Major Contributing Factor in the Pathogenesis of Bronchopulmonary Dysplasia. Am. Rev. Respir. Dis. 1988, 138, 725–729. [Google Scholar] [CrossRef]
- Ehrenkranz, R.A.; Dusick, A.M.; Vohr, B.R.; Wright, L.L.; Wrage, L.A.; Poole, W.K.; National Institutes of Child Health and Human Development Neonatal Research Network. Growth in the Neonatal Intensive Care Unit Influences Neurodevelopmental and Growth Outcomes of Extremely Low Birth Weight Infants. Pediatrics 2006, 117, 1253–1261. [Google Scholar] [CrossRef]
- Koletzko, B.; Cheah, F.-C.; Domellöf, M.; van Goudoever, J.B.; Poindexter, B.B.; Vain, N. Scientific Basis and Practical Application of Nutritional Care for Preterm Infants. In World Review of Nutrition and Dietetics; Koletzko, B., Cheah, F.-C., Domellöf, M., Poindexter, B.B., Vain, N., van Goudoever, J.B., Eds.; S. Karger: Basel, Switzerland, 2021; Volume 122, pp. 13–14. [Google Scholar]
- Kumar, R.K.; Singhal, A.; Vaidya, U.; Banerjee, S.; Anwar, F.; Rao, S. Optimizing Nutrition in Preterm Low Birth Weight Infants—Consensus Summary. Front. Nutr. 2017, 4, 20. [Google Scholar] [CrossRef]
- Hiltunen, H.; Löyttyniemi, E.; Isolauri, E.; Rautava, S. Early Nutrition and Growth until the Corrected Age of 2 Years in Extremely Preterm Infants. Neonatology 2018, 113, 100–107. [Google Scholar] [CrossRef]
- Leppänen, M.; Lapinleimu, H.; Lind, A.; Matomäki, J.; Lehtonen, L.; Haataja, L.; Rautava, P. Antenatal and Postnatal Growth and 5-Year Cognitive Outcome in Very Preterm Infants. Pediatrics 2014, 133, 63–70. [Google Scholar] [CrossRef]
- Schneider, J.; Fischer Fumeaux, C.J.; Duerden, E.G.; Guo, T.; Foong, J.; Graz, M.B.; Hagmann, P.; Chakravarty, M.M.; Hüppi, P.S.; Beauport, L.; et al. Nutrient Intake in the First Two Weeks of Life and Brain Growth in Preterm Neonates. Pediatrics 2018, 141, e20172169. [Google Scholar] [CrossRef]
- Brennan, A.-M.; Fenton, S.; Murphy, B.P.; Kiely, M.E. Transition Phase Nutrition Recommendations: A Missing Link in the Nutrition Management of Preterm Infants. JPEN J. Parenter. Enteral. Nutr. 2017, 42, 343–351. [Google Scholar] [CrossRef]
- Bronsky, J.; Campoy, C.; Braegger, C.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Decsi, T.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Vitamins. Clin. Nutr. 2018, 37, 2366–2378. [Google Scholar] [CrossRef]
- Domellöf, M.; Szitanyi, P.; Simchowitz, V.; Franz, A.; Mimouni, F.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Iron and Trace Minerals. Clin. Nutr. 2018, 37, 2354–2359. [Google Scholar] [CrossRef] [PubMed]
- Jochum, F.; Moltu, S.J.; Senterre, T.; Nomayo, A.; Goulet, O.; Iacobelli, S.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Fluid and Electrolytes. Clin. Nutr. 2018, 37, 2344–2353. [Google Scholar] [CrossRef] [PubMed]
- Joosten, K.; Embleton, N.; Yan, W.; Senterre, T.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Energy. Clin. Nutr. 2018, 37, 2309–2314. [Google Scholar] [CrossRef] [PubMed]
- Kolaček, S.; Puntis, J.W.L.; Hojsak, I.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Decsi, T.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Venous Access. Clin. Nutr. 2018, 37, 2379–2391. [Google Scholar] [CrossRef] [PubMed]
- Lapillonne, A.; Fidler Mis, N.; Goulet, O.; van den Akker, C.H.P.; Wu, J.; Koletzko, B.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Lipids. Clin. Nutr. 2018, 37, 2324–2336. [Google Scholar] [CrossRef]
- Mesotten, D.; Joosten, K.; van Kempen, A.; Verbruggen, S.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Carbohydrates. Clin. Nutr. 2018, 37, 2337–2343. [Google Scholar] [CrossRef]
- Mihatsch, W.; Shamir, R.; van Goudoever, J.B.; Fewtrell, M.; Lapillonne, A.; Lohner, S.; Mihályi, K.; Decsi, T.; Braegger, C.; Bronsky, J.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Guideline Development Process for the Updated Guidelines. Clin. Nutr. 2018, 37, 2306–2308. [Google Scholar] [CrossRef]
- van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; Sainz de Pipaon, M.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Amino Acids. Clin. Nutr. 2018, 37, 2315–2323. [Google Scholar] [CrossRef]
- Early Nutrition Programming Project; Koletzko, B.; Brands, B.; Demmelmair, H. The Early Nutrition Programming Project (EARNEST): 5 y of Successful Multidisciplinary Collaborative Research. Am. J. Clin. Nutr. 2011, 94, 1749S–1753S. [Google Scholar] [CrossRef]
- Koletzko, B.; Poindexter, B.; Uauy, R. Recommended Nutrient Intake Levels for Stable, Fully Enterally Fed Very Low Birth Weight Infants. In World Review of Nutrition and Dietetics; Koletzko, B., Poindexter, B., Uauy, R., Eds.; S. Karger: Basel, Switzerland, 2014; Volume 110, pp. 297–299. ISBN 978-3-318-02640-5. [Google Scholar]
- Carnielli, V.P.; Correani, A.; Giretti, I.; Apos Ascenzo, R.D.; Bellagamba, M.P.; Burattini, I.; Biagetti, C. Practice of Parenteral Nutrition in Preterm Infants. In World Review of Nutrition and Dietetics; Koletzko, B., Cheah, F.-C., Domellöf, M., Poindexter, B.B., Vain, N., van Goudoever, J.B., Eds.; S. Karger: Basel, Switzerland, 2021; Volume 122, pp. 198–211. ISBN 978-3-318-06646-3. [Google Scholar]
- Mustapha, M.; Wilson, K.A.; Barr, S. Optimising Nutrition of Preterm and Term Infants in the Neonatal Intensive Care Unit. Paediatr. Child Health 2021, 31, 38–45. [Google Scholar] [CrossRef]
- ESPGHAN and ESPEN Guidelines Paediatric Parenteral Nutrition—Annex: List of Products. J. Pediatric Gastroenterol. Nutr. 2005, 41, S85–S87. [CrossRef] [PubMed]
- Maier, H. Visite2000. Available online: www.Visite2000.de (accessed on 9 September 2022).
- Agostoni, C.; Buonocore, G.; Carnielli, V.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral Nutrient Supply for Preterm Infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatric Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef]
- Nutrition and Feeding of Preterm Infants. Committee on Nutrition of the Preterm Infant, European Society of Paediatric Gastroenterology and Nutrition. Acta Paediatr. Scand. Suppl. 1987, 336, 1–14. [Google Scholar]
- Voigt, M.; Fusch, C.; Olbertz, D.; Hartmann, K.; Rochow, N.; Renken, C.; Schneider, K. Analyse des Neugeborenenkollektivs der Bundesrepublik Deutschland. Geburtsh. Frauenheilk. 2006, 66, 956–970. [Google Scholar] [CrossRef]
- Do, K.T.; Wahl, S.; Raffler, J.; Molnos, S.; Laimighofer, M.; Adamski, J.; Suhre, K.; Strauch, K.; Peters, A.; Gieger, C.; et al. Characterization of Missing Values in Untargeted MS-Based Metabolomics Data and Evaluation of Missing Data Handling Strategies. Metabolomics 2018, 14, 128. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodological) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- A.S.P.E.N. Board of Directors and Task Force on Parenteral Nutrition Standardization; Kochevar, M.; Guenter, P.; Holcombe, B.; Malone, A.; Mirtallo, J. A.S.P.E.N. Statement on Parenteral Nutrition Standardization. JPEN J. Parenter. Enteral. Nutr. 2007, 31, 441–448. [Google Scholar] [CrossRef]
- Georgieff, M.K. Nutrition and the Developing Brain: Nutrient Priorities and Measurement. Am. J. Clin. Nutr. 2007, 85, 614S–620S. [Google Scholar] [CrossRef]
- Kreissl, A.; Repa, A.; Binder, C.; Thanhaeuser, M.; Jilma, B.; Berger, A.; Haiden, N. Clinical Experience with Numeta in Preterm Infants: Impact on Nutrient Intake and Costs. JPEN J. Parenter. Enteral. Nutr. 2016, 40, 536–542. [Google Scholar] [CrossRef]
- Simmer, K.; Rakshasbhuvankar, A.; Deshpande, G. Standardised Parenteral Nutrition. Nutrients 2013, 5, 1058–1070. [Google Scholar] [CrossRef]
- Morisaki, N.; Belfort, M.B.; McCormick, M.C.; Mori, R.; Noma, H.; Kusuda, S.; Fujimura, M.; The Neonatal Research Network of Japan. Brief Parenteral Nutrition Accelerates Weight Gain, Head Growth Even in Healthy VLBWs. PLoS ONE 2014, 9, e88392. [Google Scholar] [CrossRef] [PubMed]
- Dinerstein, A.; Nieto, R.M.; Solana, C.L.; Perez, G.P.; Otheguy, L.E.; Larguia, A.M. Early and Aggressive Nutritional Strategy (Parenteral and Enteral) Decreases Postnatal Growth Failure in Very Low Birth Weight Infants. J. Perinatol. 2006, 26, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Iacobelli, S.; Bonsante, F.; Vintéjoux, A.; Gouyon, J.-B. Standardized Parenteral Nutrition in Preterm Infants: Early Impact on Fluid and Electrolyte Balance. Neonatology 2010, 98, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Osborn, D.A.; Schindler, T.; Jones, L.J.; Sinn, J.K.; Bolisetty, S. Higher versus Lower Amino Acid Intake in Parenteral Nutrition for Newborn Infants. Cochrane Database Syst. Rev. 2018, 2018, 3. [Google Scholar] [CrossRef] [PubMed]
- Regan, F.M.; Cutfield, W.S.; Jefferies, C.; Robinson, E.; Hofman, P.L. The Impact of Early Nutrition in Premature Infants on Later Childhood Insulin Sensitivity and Growth. Pediatrics 2006, 118, 1943–1949. [Google Scholar] [CrossRef]
- Stephens, B.E.; Walden, R.V.; Gargus, R.A.; Tucker, R.; McKinley, L.; Mance, M.; Nye, J.; Vohr, B.R. First-Week Protein and Energy Intakes Are Associated with 18-Month Developmental Outcomes in Extremely Low Birth Weight Infants. Pediatrics 2009, 123, 1337–1343. [Google Scholar] [CrossRef]
- Yeung, M.; Smyth, J.; Maheshwari, R.; Shah, S. Evaluation of Standardized versus Individualized Total Parenteral Nutrition Regime for Neonates Less than 33 Weeks Gestation. J. Paediatr. Child Health 2003, 39, 613–617. [Google Scholar] [CrossRef]
- Skouroliakou, M.; Koutri, K.; Stathopoulou, M.; Vourvouhaki, E.; Giannopoulou, I.; Gounaris, A. Comparison of Two Types of TPN Prescription Methods in Preterm Neonates. Pharm. World Sci. 2009, 31, 202–208. [Google Scholar] [CrossRef]
- Bolisetty, S.; Osborn, D.; Schindler, T.; Sinn, J.; Deshpande, G.; Wong, C.S.; Jacobs, S.E.; Phad, N.; Pharande, P.; Tobiansky, R.; et al. Standardised Neonatal Parenteral Nutrition Formulations—Australasian Neonatal Parenteral Nutrition Consensus Update 2017. BMC Pediatr. 2020, 20, 59. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. Neonatal Salt Intake and Blood Pressure. Lancet 2001, 357, 1880. [Google Scholar] [CrossRef]
- Posner, A.S. Crystal Chemistry of Bone Mineral. Physiol. Rev. 1969, 49, 760–792. [Google Scholar] [CrossRef] [PubMed]
- Pohlandt, F. Prevention of Postnatal Bone Demineralization in Very Low-Birth-Weight Infants by Individually Monitored Supplementation with Calcium and Phosphorus. Pediatr. Res. 1994, 35, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Pohlandt, F. Bone Mineral Deficiency as the Main Factor of Dolichocephalic Head Flattening in Very-Low-Birth-Weight Infants. Pediatr. Res. 1994, 35, 701–703. [Google Scholar] [CrossRef] [PubMed]
- Trotter, A.; Pohlandt, F. Calcium and Phosphorus Retention in Extremely Preterm Infants Supplemented Individually. Acta Paediatr. 2002, 91, 680–683. [Google Scholar] [CrossRef]
- Wilson, D.C.; Cairns, P.; Halliday, H.L.; Reid, M.; McClure, G.; Dodge, J.A. Randomised Controlled Trial of an Aggressive Nutritional Regimen in Sick Very Low Birthweight Infants. Arch. Dis. Child. Fetal Neonatal. Ed. 1997, 77, F4–F11. [Google Scholar] [CrossRef]
- Singhal, A.; Fewtrell, M.; Cole, T.J.; Lucas, A. Low Nutrient Intake and Early Growth for Later Insulin Resistance in Adolescents Born Preterm. Lancet 2003, 361, 1089–1097. [Google Scholar] [CrossRef]
- Clark, R.H.; Kelleher, A.S.; Chace, D.H.; Spitzer, A.R. Gestational Age and Age at Sampling Influence Metabolic Profiles in Premature Infants. Pediatrics 2014, 134, e37–e46. [Google Scholar] [CrossRef]
- Nilsson, A.K.; Tebani, A.; Malmodin, D.; Pedersen, A.; Hellgren, G.; Löfqvist, C.; Hansen-Pupp, I.; Uhlén, M.; Hellström, A. Longitudinal Serum Metabolomics in Extremely Premature Infants: Relationships with Gestational Age, Nutrition, and Morbidities. Front. Neurosci. 2022, 16, 830884. [Google Scholar] [CrossRef]
- Druml, W.; Heinzel, G.; Kleinberger, G. Amino Acid Kinetics in Patients with Sepsis. Am. J. Clin. Nutr. 2001, 73, 908–913. [Google Scholar] [CrossRef]
- Chiarla, C.; Giovannini, I.; Siegel, J.H. Characterization of Alpha-Amino-n-Butyric Acid Correlations in Sepsis. Transl. Res. 2011, 158, 328–333. [Google Scholar] [CrossRef]
- Oltman, S.P.; Rogers, E.E.; Baer, R.J.; Jasper, E.A.; Anderson, J.G.; Steurer, M.A.; Pantell, M.S.; Petersen, M.A.; Partridge, J.C.; Karasek, D.; et al. Newborn Metabolic Vulnerability Profile Identifies Preterm Infants at Risk for Mortality and Morbidity. Pediatr. Res. 2021, 89, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Schanler, R.J.; Shulman, R.J.; Lau, C.; Smith, E.O.; Heitkemper, M.M. Feeding Strategies for Premature Infants: Randomized Trial of Gastrointestinal Priming and Tube-Feeding Method. Pediatrics 1999, 103, 434–439. [Google Scholar] [CrossRef]
- EPIPAGE 2 Writing Group; Ancel, P.-Y.; Goffinet, F. EPIPAGE 2: A Preterm Birth Cohort in France in 2011. BMC Pediatr. 2014, 14, 97. [Google Scholar] [CrossRef] [PubMed]
- Dusick, A.M.; Poindexter, B.B.; Ehrenkranz, R.A.; Lemons, J.A. Growth Failure in the Preterm Infant: Can We Catch Up? Semin. Perinatol. 2003, 27, 302–310. [Google Scholar] [CrossRef]
- Wiedmeier, J.E.; Joss-Moore, L.A.; Lane, R.H.; Neu, J. Early Postnatal Nutrition and Programming of the Preterm Neonate: Nutrition Reviews©. Nutr. Rev. 2011, 69, 76–82. [Google Scholar] [CrossRef]
- Johnson, M.J.; Wiskin, A.E.; Pearson, F.; Beattie, R.M.; Leaf, A.A. How to Use: Nutritional Assessment in Neonates. Arch. Dis. Child. Educ. Pract. Ed. 2015, 100, 147–154. [Google Scholar] [CrossRef]
- Riskin, A.; Picaud, J.-C.; Shamir, R.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Decsi, T.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Standard versus Individualized Parenteral Nutrition. Clin. Nutr. 2018, 37, 2409–2417. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).