
Anthropometric Cut-Off Values for Detecting the Presence of Metabolic Syndrome and Its Multiple Components among Adults in Vietnam: The Role of Novel Indices

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Sample Size and Sampling Technique
2.3. Measurements and Instruments
2.3.1. Anthropometric Measurements and Biochemical Test
- We used a SECA scale with an accuracy of 0.1 kilograms (kg) to assess body weight. The body weight was reported in kg with a decimal. Participants’ scale was measured in the morning without eating anything and after urinating. Participants stood in the middle of the scale; their eyes looked straight, and their weight was evenly distributed on both legs. The scale was placed in a stable and flat position.
- A microtoise gauge height was utilized to estimate vertical height with an accuracy of 1 millimeter (mm). Height was recorded in centimeters (cm) with a decimal. Participants took off their shoes and stood with his/her back to the ruler. Heels, legs, buttocks, shoulders, and head stayed in a straight line against the vertical ruler, while eyes looked straight in a horizontal line. Two hands hung along his/her sides. A researcher pulled the top of the ruler from the top-down and read the result when the ruler’s top touched close to the crown of the head.
- An elastic band estimated waist and hip circumstances (WC and HC), and the results were reported in centimeters (cm) with a decimal. In this study, to measure the WC, we determined the lowest point of the lower rib and the upper edge of the iliac crest and then took the midpoint of these two positions. In addition, the fullest part of the buttock got the measure of the HC.
- Body fat percentage was calculated by a Japanese OMRON bio-electrometer, which was recommended if there was a presence of technical error, such as using a 3-site skinfold [22].
- We applied a mercury sphygmomanometer to assess the blood pressure of respondents two times for two minutes apart. The final result was calculated as the average of the two measurements. If the parameters between the two times differed by more than ten millimeters of mercury (mmHg), the third measurement must be repeated.
- Total cholesterol was quantified by the CHOD-PAP method, which used an enzyme (enzymatic colorimetric), cholesterol oxidase phenazon amino peroxidase.
- Serum triglycerides were measured using the colorimetric GPO-PAP method (Glycerol phosphate oxidase phenazon amino oxidase).
- Serum HDL-C was assessed by the method of precipitation of LDL-C, very-low-density lipoprotein (VLDL) cholesterol, and chylomicrons.
2.3.2. Anthropometric Indices and Metabolic Syndrome Definition
- Body mass index (BMI) = Weight (kg)/Height2 (m)
- Waist-height ratio [WHtR] = WC (cm)/Height (cm)
- Waist-hip ratio [WHR] = WC (cm)/HC (cm)
- Abdominal volume index [AVI] = (2 × WC2 (cm) + 0.7 × (WC-HC)2 (cm))/1000
- Body roundness index [BRI] = 364.2 − 365.5 ×
- A body shape index [ABSI] = WC (m)/(BMI2/3 × Height1/2 (m))
- Conicity index [CI] = WC (m)/(0.109 ×)
- Body adiposity index [BAI] = (HC (cm)/Height1.5(m)) − 18
- Abdominal fat in which waist circumference was ≥90 cm for males and ≥80 cm for females
- High triglycerides (≥1.7 mmol/L or ≥150 mg/dL)
- Low HDL-C (<40 mg/dL (<1.03 mmol/L) for males, <50 mg/dL (<1.29 mmol/L) for females)
- Elevated blood pressure which was presented as systolic hypertension (SBP ≥ 130 mmHg) or diastolic hypertension (DBP ≥ 85mmHg)
- High fasting blood glucose (≥5.6 mmol/l or ≥100 mg/dL)
2.4. Data Analysis
2.5. Ethical Statement
3. Results
3.1. General Information of Participants
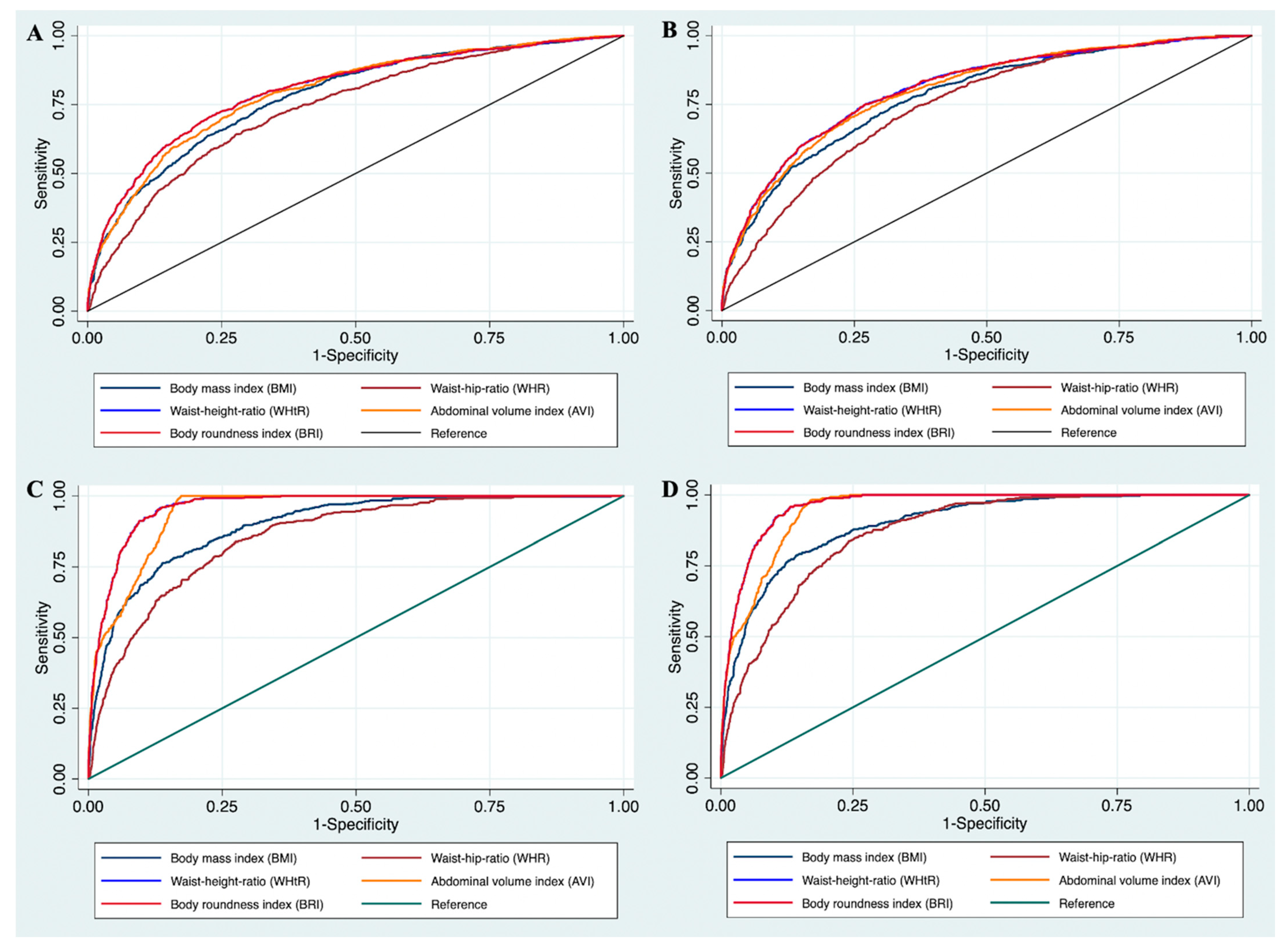
3.2. ROC Curve Analysis and Cut-Off Points Estimation
4. Discussion
4.1. Implications
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Han, T.S.; Lean, M.E. A clinical perspective of obesity, metabolic syndrome and cardiovascular disease. JRSM Cardiovasc. Dis. 2016, 5, 2048004016633371. [Google Scholar] [CrossRef]
- Zhang, J.; Zhu, W.; Qiu, L.; Huang, L.; Fang, L. Sex- and Age-Specific Optimal Anthropometric Indices as Screening Tools for Metabolic Syndrome in Chinese Adults. Int. J. Endocrinol. 2018, 2018, 1067603. [Google Scholar] [CrossRef]
- Ngoc, N.B.; Lin, Z.L.; Ahmed, W. Diabetes: What Challenges Lie Ahead for Vietnam? Ann. Glob. Health 2020, 86, 1. [Google Scholar] [CrossRef]
- Benmohammed, K.; Valensi, P.; Benlatreche, M.; Nguyen, M.T.; Benmohammed, F.; Paries, J.; Khensal, S.; Benlatreche, C.; Lezzar, A. Anthropometric markers for detection of the metabolic syndrome in adolescents. Diabetes Metab. 2015, 41, 138–144. [Google Scholar] [CrossRef]
- Gluszek, S.; Ciesla, E.; Gluszek-Osuch, M.; Koziel, D.; Kiebzak, W.; Wypchlo, L.; Suliga, E. Anthropometric indices and cut-off points in the diagnosis of metabolic disorders. PLoS ONE 2020, 15, e0235121. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.S.; Gibson, R.S. Principles of Nutritional Assessment; Oxford University Press: New York, NY, USA, 2005. [Google Scholar]
- Daniels, S.R. The use of BMI in the clinical setting. Pediatrics 2009, 124 (Suppl. 1), S35–S41. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Ashwell, M.; Gibson, S. Waist-to-height ratio as an indicator of ‘early health risk’: Simpler and more predictive than using a ‘matrix’ based on BMI and waist circumference. BMJ Open 2016, 6, e010159. [Google Scholar] [CrossRef]
- Bener, A.; Yousafzai, M.T.; Darwish, S.; Al-Hamaq, A.O.; Nasralla, E.A.; Abdul-Ghani, M. Obesity index that better predict metabolic syndrome: Body mass index, waist circumference, waist hip ratio, or waist height ratio. J. Obes. 2013, 2013, 269038. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.M.; Bredlau, C.; Bosy-Westphal, A.; Mueller, M.; Shen, W.; Gallagher, D.; Maeda, Y.; McDougall, A.; Peterson, C.M.; Ravussin, E.; et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity 2013, 21, 2264–2271. [Google Scholar] [CrossRef] [PubMed]
- Rico-Martin, S.; Calderon-Garcia, J.F.; Sanchez-Rey, P.; Franco-Antonio, C.; Martinez Alvarez, M.; Sanchez Munoz-Torrero, J.F. Effectiveness of body roundness index in predicting metabolic syndrome: A systematic review and meta-analysis. Obes. Rev. 2020, 21, e13023. [Google Scholar] [CrossRef] [PubMed]
- Valdez, R.; Seidell, J.C.; Ahn, Y.I.; Weiss, K.M. A new index of abdominal adiposity as an indicator of risk for cardiovascular disease. A cross-population study. Int. J. Obes. Relat. Metab. Disord. 1993, 17, 77–82. [Google Scholar]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A better index of body adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef]
- Bergman, R.N. A Better Index of Body Adiposity. Obesity 2012, 20, 1135. [Google Scholar] [CrossRef]
- Sinaga, M.; Worku, M.; Yemane, T.; Tegene, E.; Wakayo, T.; Girma, T.; Lindstrom, D.; Belachew, T. Optimal cut-off for obesity and markers of metabolic syndrome for Ethiopian adults. Nutr. J. 2018, 17, 109. [Google Scholar] [CrossRef]
- Liu, Y.; Tong, G.; Tong, W.; Lu, L.; Qin, X. Can body mass index, waist circumference, waist-hip ratio and waist-height ratio predict the presence of multiple metabolic risk factors in Chinese subjects? BMC Public Health 2011, 11, 35. [Google Scholar] [CrossRef]
- Liu, L.; Liu, Y.; Sun, X.; Yin, Z.; Li, H.; Deng, K.; Chen, X.; Cheng, C.; Luo, X.; Zhang, M.; et al. Identification of an obesity index for predicting metabolic syndrome by gender: The rural Chinese cohort study. BMC Endocr. Disord. 2018, 18, 54. [Google Scholar] [CrossRef]
- Hop, L.T.; Mai, L.B.; Khan, N.C. Obesity and metabolic syndrome among adults aged 25–64 in Vietnam. J. Food Nutr. Sci. 2008, 4, 4. [Google Scholar]
- Pham, D.T.; Le, M.B. Metabolic syndrome and some risk factors among adults in a ward of the inner city of Hanoi. J. Pract. Med. 2007, 263, 25–33. [Google Scholar]
- Loenneke, J.P.; Barnes, J.T.; Wilson, J.M.; Lowery, R.P.; Isaacs, M.N.; Pujol, T.J. Reliability of field methods for estimating body fat. Clin. Physiol. Funct. Imaging 2013, 33, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Moy, F.M.; Bulgiba, A. The modified NCEP ATP III criteria maybe better than the IDF criteria in diagnosing Metabolic Syndrome among Malays in Kuala Lumpur. BMC Public Health 2010, 10, 678. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C.; et al. Diagnosis and Management of the Metabolic Syndrome. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [Green Version]
- Hajian-Tilaki, K. Receiver Operating Characteristic (ROC) Curve Analysis for Medical Diagnostic Test Evaluation. Caspian J. Intern. Med. 2013, 4, 627–635. [Google Scholar]
- Zou, K.H.; O’Malley, A.J.; Mauri, L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Cleves, M.A. From the Help Desk: Comparing Areas under Receiver Operating Characteristic Curves from Two or more Probit or Logit Models. Stata J. 2002, 2, 301–313. [Google Scholar] [CrossRef]
- Moosaie, F.; Fatemi Abhari, S.M.; Deravi, N.; Karimi Behnagh, A.; Esteghamati, S.; Dehghani Firouzabadi, F.; Rabizadeh, S.; Nakhjavani, M.; Esteghamati, A. Waist-To-Height Ratio Is a More Accurate Tool for Predicting Hypertension Than Waist-To-Hip Circumference and BMI in Patients With Type 2 Diabetes: A Prospective Study. Front. Public Health 2021, 9, 726288. [Google Scholar] [CrossRef]
- Quaye, L.; Owiredu, W.; Amidu, N.; Dapare, P.P.M.; Adams, Y. Comparative Abilities of Body Mass Index, Waist Circumference, Abdominal Volume Index, Body Adiposity Index, and Conicity Index as Predictive Screening Tools for Metabolic Syndrome among Apparently Healthy Ghanaian Adults. J. Obes. 2019, 2019, 8143179. [Google Scholar] [CrossRef]
- Xu, J.; Zhang, L.; Wu, Q.; Zhou, Y.; Jin, Z.; Li, Z.; Zhu, Y. Body roundness index is a superior indicator to associate with the cardio-metabolic risk: Evidence from a cross-sectional study with 17,000 Eastern-China adults. BMC Cardiovasc. Disord. 2021, 21, 97. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.; Yu, L.; Shen, X.; Li, D.; Wang, K. Waist-to-height ratio, an optimal predictor for obesity and metabolic syndrome in Chinese adults. J. Nutr. Health Aging 2010, 14, 782–785. [Google Scholar] [CrossRef]
- Savva, S.C.; Lamnisos, D.; Kafatos, A.G. Predicting cardiometabolic risk: Waist-to-height ratio or BMI. A meta-analysis. Diabetes Metab. Syndr. Obes. 2013, 6, 403–419. [Google Scholar] [CrossRef]
- Gu, J.J.; Rafalson, L.; Zhao, G.M.; Wu, H.Y.; Zhou, Y.; Jiang, Q.W.; Bai, Y.; Zhu, Q.L.; Fu, X.J.; Zhang, H.; et al. Anthropometric measurements for prediction of metabolic risk among Chinese adults in Pudong new area of Shanghai. Exp. Clin. Endocrinol. Diabetes 2011, 119, 387–394. [Google Scholar] [CrossRef]
- Ashwell, M.; Hsieh, S.D. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int. J. Food Sci. Nutr. 2005, 56, 303–307. [Google Scholar] [CrossRef]
- Perona, J.S.; Schmidt Rio-Valle, J.; Ramirez-Velez, R.; Correa-Rodriguez, M.; Fernandez-Aparicio, A.; Gonzalez-Jimenez, E. Waist circumference and abdominal volume index are the strongest anthropometric discriminators of metabolic syndrome in Spanish adolescents. Eur. J. Clin. Investig. 2019, 49, e13060. [Google Scholar] [CrossRef]
- Tran, N.T.T.; Blizzard, C.L.; Luong, K.N.; Truong, N.L.V.; Tran, B.Q.; Otahal, P.; Nelson, M.; Magnussen, C.; Gall, S.; Bui, T.V.; et al. The importance of waist circumference and body mass index in cross-sectional relationships with risk of cardiovascular disease in Vietnam. PLoS ONE 2018, 13, e0198202. [Google Scholar] [CrossRef]
- Perona, J.S.; Schmidt-RioValle, J.; Fernandez-Aparicio, A.; Correa-Rodriguez, M.; Ramirez-Velez, R.; Gonzalez-Jimenez, E. Waist Circumference and Abdominal Volume Index Can Predict Metabolic Syndrome in Adolescents, but only When the Criteria of the International Diabetes Federation are Employed for the Diagnosis. Nutrients 2019, 11, 1370. [Google Scholar] [CrossRef]
- Zhu, L.; Spence, C.; Yang, J.W.; Ma, G.X. The IDF Definition Is Better Suited for Screening Metabolic Syndrome and Estimating Risks of Diabetes in Asian American Adults: Evidence from NHANES 2011–2016. J. Clin. Med. 2020, 9, 3871. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for the Western, P. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000.
- Nguyen, T.T.; Adair, L.S.; Suchindran, C.M.; He, K.; Popkin, B.M. The association between body mass index and hypertension is different between East and Southeast Asians. Am. J. Clin. Nutr. 2009, 89, 1905–1912. [Google Scholar] [CrossRef]
- Choi, J.-W.; Yu, J. Cut-off Values of Waist Circumference and Body Mass Index for Metabolic Syndrome according to Sasang Constitution. J. Sasang Const. Med. 2014, 26, 365–378. [Google Scholar] [CrossRef]
- Kim, H.I.; Kim, J.T.; Yu, S.H.; Kwak, S.H.; Jang, H.C.; Park, K.S.; Kim, S.Y.; Lee, H.K.; Cho, Y.M. Gender Differences in Diagnostic Values of Visceral Fat Area and Waist Circumference for Predicting Metabolic Syndrome in Koreans. J. Korean Med. Sci. 2011, 26, 906–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Regions of Vietnam | City and Areas |
|---|---|
| Urban areas | Hanoi city and Ho Chi Minh city |
| Rural areas | Northern delta and Mekong River delta |
| Mountainous areas | Northern mountainous region and Central Highlands |
| Coastal areas | Coastal areas in North Central and South Central |
| Having MetS | Without MetS | Total | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| MetS by NCEP ATP III (n, %) | 1056 | 22.5 | 3645 | 77.5 | |||
| MetS by IDF (n, %) | 468 | 10.0 | 4233 | 90.0 | |||
| Weight (kg) | 57.5 | 10.4 | 51.3 | 8.5 | 52.7 | 9.3 | <0.01 * |
| Height (cm) | 156.0 | 8.1 | 157.0 | 7.7 | 156.8 | 7.8 | <0.01 * |
| Waist circumference (WC, cm) | 81.4 | 9.8 | 71.8 | 7.8 | 73.9 | 9.2 | <0.01 * |
| Hip circumference (cm) | 92.2 | 7.0 | 87.2 | 5.9 | 88.3 | 6.5 | <0.01 * |
| Body mass index (kg/m2) | 23.6 | 3.4 | 20.8 | 2.6 | 21.4 | 3.1 | <0.01 * |
| Waist–hip ratio (WHR) | 0.9 | 0.1 | 0.8 | 0.1 | 0.8 | 0.1 | <0.01 * |
| Waist–height ratio (WHtR) | 0.5 | 0.1 | 0.5 | 0.1 | 0.5 | 0.1 | 0.50 * |
| Body fat percentage (%) | 29.8 | 6.5 | 23.6 | 6.5 | 25.0 | 7.0 | <0.01 * |
| Systolic blood pressure (mmhg) | 142.3 | 21.7 | 121.6 | 20.2 | 126.3 | 22.3 | <0.01 * |
| Diastolic blood pressure (mmhg) | 86.4 | 12.4 | 75.5 | 12.1 | 78.0 | 13.0 | <0.01 * |
| Total cholesterol (mg/dL) | 5.4 | 1.2 | 4.7 | 1.0 | 4.9 | 1.1 | <0.01 * |
| HDL cholesterol (mg/dL) | 1.0 | 0.2 | 1.3 | 0.3 | 1.2 | 0.3 | <0.01 * |
| LDL cholesterol (mg/dL) | 3.3 | 1.1 | 2.7 | 0.9 | 2.9 | 0.9 | <0.01 * |
| Triglycerides (mg/dL) | 2.7 | 1.6 | 1.4 | 0.9 | 1.7 | 1.2 | <0.01 * |
| Fasting blood glucose (mg/dL) | 6.0 | 2.0 | 4.9 | 0.9 | 5.2 | 1.3 | <0.01 * |
| Abdominal Volume Index (AVI) | 13.5 | 3.2 | 10.6 | 2.2 | 11.3 | 2.8 | <0.01 * |
| Body roundness index (BRI) | 3.9 | 1.2 | 2.6 | 0.8 | 2.9 | 1.1 | <0.01 * |
| A body shape index (ABSI) | 0.08 | 0.01 | 0.08 | 0.01 | 0.08 | 0.01 | 0.05 * |
| Body adiposity index (BAI) | 29.5 | 4.5 | 26.4 | 3.6 | 27.1 | 4.0 | <0.01 * |
| Conicity index (CI) | 1.2 | 0.1 | 1.2 | 0.1 | 1.2 | 0.1 | 0.05 * |
| MetS Components | Indices | AUC | Sensitivity | Specificity | Youden Index | Cut-Off Points |
|---|---|---|---|---|---|---|
| High triglycerides | BMI | 0.69 | 0.63 | 0.68 | 0.31 | 21.3 |
| %BF | 0.69 | 0.64 | 0.64 | 0.27 | 22.5 | |
| WHR | 0.68 | 0.63 | 0.65 | 0.28 | 0.85 | |
| WHtR | 0.70 | 0.56 | 0.75 | 0.31 | 0.48 | |
| AVI | 0.70 | 0.60 | 0.71 | 0.32 | 11.7 | |
| BRI | 0.70 | 0.56 | 0.75 | 0.31 | 3.00 | |
| ABSI | 0.60 | 0.65 | 0.51 | 0.17 | 0.08 | |
| BAI | 0.63 | 0.65 | 0.55 | 0.20 | 24.6 | |
| CI | 0.65 | 0.58 | 0.67 | 0.25 | 1.19 | |
| Low HDL-C | BMI | 0.59 | 0.55 | 0.61 | 0.16 | 21.3 |
| %BF | 0.59 | 0.37 | 0.78 | 0.15 | 25.80 | |
| WHR | 0.57 | 0.42 | 0.70 | 0.12 | 0.88 | |
| WHtR | 0.58 | 0.49 | 0.65 | 0.14 | 0.48 | |
| AVI | 0.59 | 0.37 | 0.78 | 0.15 | 13.2 | |
| BRI | 0.58 | 0.49 | 0.65 | 0.14 | 2.90 | |
| ABSI | 0.53 | 0.45 | 0.62 | 0.07 | 0.08 | |
| BAI | 0.57 | 0.60 | 0.52 | 0.12 | 24.70 | |
| CI | 0.55 | 0.47 | 0.64 | 0.11 | 1.20 | |
| Increased blood glucose | BMI | 0.61 | 0.50 | 0.63 | 0.14 | 21.7 |
| %BF | 0.62 | 0.56 | 0.63 | 0.19 | 23.6 | |
| WHR | 0.63 | 0.54 | 0.66 | 0.20 | 0.87 | |
| WHtR | 0.64 | 0.46 | 0.75 | 0.21 | 0.49 | |
| AVI | 0.64 | 0.52 | 0.69 | 0.21 | 12.3 | |
| BRI | 0.64 | 0.46 | 0.75 | 0.21 | 3.26 | |
| ABSI | 0.63 | 0.62 | 0.59 | 0.21 | 0.08 | |
| BAI | 0.60 | 0.61 | 0.52 | 0.13 | 24.82 | |
| CI | 0.64 | 0.61 | 0.60 | 0.21 | 1.19 | |
| Elevated blood pressure | BMI | 0.72 | 0.57 | 0.60 | 0.16 | 21.1 |
| %BF | 0.72 | 0.58 | 0.69 | 0.27 | 23.0 | |
| WHR | 0.71 | 0.60 | 0.60 | 0.20 | 0.85 | |
| WHtR | 0.71 | 0.52 | 0.68 | 0.20 | 0.47 | |
| AVI | 0.72 | 0.69 | 0.50 | 0.19 | 10.45 | |
| BRI | 0.72 | 0.52 | 0.68 | 0.20 | 2.82 | |
| ABSI | 0.68 | 0.64 | 0.51 | 0.15 | 0.08 | |
| BAI | 0.70 | 0.68 | 0.47 | 0.15 | 24.00 | |
| CI | 0.70 | 0.48 | 0.71 | 0.19 | 1.20 | |
| MetS by ATP | BMI | 0.74 | 0.74 | 0.61 | 0.35 | 21.30 |
| %BF | 0.74 | 0.74 | 0.63 | 0.37 | 23.10 | |
| WHR | 0.73 | 0.68 | 0.71 | 0.39 | 0.87 | |
| WHtR | 0.76 | 0.60 | 0.82 | 0.42 | 0.50 | |
| AVI | 0.77 | 0.63 | 0.78 | 0.40 | 12.94 | |
| BRI | 0.76 | 0.60 | 0.82 | 0.42 | 3.37 | |
| ABSI | 0.67 | 0.64 | 0.65 | 0.29 | 0.08 | |
| BAI | 0.68 | 0.73 | 0.55 | 0.28 | 24.82 | |
| CI | 0.72 | 0.64 | 0.74 | 0.37 | 1.21 | |
| MetS by IDF | BMI | 0.93 | 0.94 | 0.73 | 0.67 | 22.40 |
| %BF | 0.87 | 0.86 | 0.73 | 0.60 | 25.30 | |
| WHR | 0.94 | 0.95 | 0.82 | 0.77 | 0.90 | |
| WHtR | 0.97 | 0.99 | 0.89 | 0.88 | 0.53 | |
| AVI | 0.99 | 1.00 | 0.98 | 0.98 | 16.20 | |
| BRI | 0.97 | 0.99 | 0.89 | 0.88 | 3.86 | |
| ABSI | 0.80 | 0.84 | 0.66 | 0.50 | 0.08 | |
| BAI | 0.82 | 0.72 | 0.78 | 0.50 | 27.00 | |
| CI | 0.91 | 0.98 | 0.73 | 0.71 | 1.22 |
| MetS Components | Indices | AUC | Sensitivity | Specificity | Youden Index | Cut-Off Points |
|---|---|---|---|---|---|---|
| High triglycerides | BMI | 0.72 | 0.76 | 0.51 | 0.27 | 20.73 |
| %BF | 0.72 | 0.77 | 0.54 | 0.31 | 27.50 | |
| WHR | 0.69 | 0.75 | 0.52 | 0.27 | 0.80 | |
| WHtR | 0.72 | 0.68 | 0.64 | 0.32 | 0.48 | |
| AVI | 0.72 | 0.68 | 0.64 | 0.32 | 10.71 | |
| BRI | 0.72 | 0.68 | 0.64 | 0.32 | 2.94 | |
| ABSI | 0.64 | 0.63 | 0.55 | 0.17 | 0.08 | |
| BAI | 0.68 | 0.66 | 0.55 | 0.21 | 28.81 | |
| CI | 0.67 | 0.72 | 0.53 | 0.25 | 1.15 | |
| Low HDL-C | BMI | 0.58 | 0.62 | 0.51 | 0.13 | 20.66 |
| %BF | 0.57 | 0.48 | 0.63 | 0.11 | 29.30 | |
| WHR | 0.55 | 0.64 | 0.45 | 0.09 | 0.80 | |
| WHtR | 0.56 | 0.51 | 0.60 | 0.11 | 0.48 | |
| AVI | 0.56 | 0.72 | 0.38 | 0.10 | 9.39 | |
| BRI | 0.56 | 0.51 | 0.60 | 0.11 | 2.91 | |
| ABSI | 0.53 | 0.44 | 0.62 | 0.06 | 0.08 | |
| BAI | 0.54 | 0.48 | 0.58 | 0.06 | 29.29 | |
| CI | 0.53 | 0.58 | 0.50 | 0.08 | 1.14 | |
| Increased blood glucose | BMI | 0.68 | 0.39 | 0.79 | 0.18 | 23.56 |
| %BF | 0.68 | 0.57 | 0.69 | 0.26 | 30.90 | |
| WHR | 0.68 | 0.53 | 0.71 | 0.25 | 0.84 | |
| WHtR | 0.70 | 0.62 | 0.65 | 0.27 | 0.49 | |
| AVI | 0.70 | 0.46 | 0.81 | 0.27 | 12.39 | |
| BRI | 0.70 | 0.62 | 0.65 | 0.27 | 3.13 | |
| ABSI | 0.65 | 0.46 | 0.75 | 0.21 | 0.08 | |
| BAI | 0.67 | 0.57 | 0.62 | 0.19 | 29.70 | |
| CI | 0.67 | 0.52 | 0.73 | 0.25 | 1.20 | |
| Elevated blood pressure | BMI | 0.79 | 0.49 | 0.72 | 0.21 | 22.27 |
| %BF | 0.77 | 0.61 | 0.68 | 0.29 | 29.50 | |
| WHR | 0.77 | 0.61 | 0.61 | 0.22 | 0.82 | |
| WHtR | 0.78 | 0.66 | 0.64 | 0.30 | 0.47 | |
| AVI | 0.78 | 0.61 | 0.65 | 0.26 | 10.81 | |
| BRI | 0.78 | 0.66 | 0.64 | 0.30 | 2.90 | |
| ABSI | 0.76 | 0.61 | 0.54 | 0.15 | 0.08 | |
| BAI | 0.78 | 0.50 | 0.73 | 0.24 | 30.35 | |
| CI | 0.76 | 0.60 | 0.61 | 0.21 | 1.16 | |
| MetS by ATP | BMI | 0.83 | 0.64 | 0.74 | 0.38 | 22.31 |
| %BF | 0.81 | 0.68 | 0.77 | 0.45 | 30.90 | |
| WHR | 0.80 | 0.74 | 0.68 | 0.42 | 0.82 | |
| WHtR | 0.84 | 0.76 | 0.75 | 0.51 | 0.49 | |
| AVI | 0.85 | 0.59 | 0.89 | 0.48 | 12.37 | |
| BRI | 0.84 | 0.76 | 0.75 | 0.51 | 3.14 | |
| ABSI | 0.74 | 0.67 | 0.61 | 0.28 | 0.08 | |
| BAI | 0.79 | 0.67 | 0.66 | 0.34 | 29.61 | |
| CI | 0.79 | 0.60 | 0.80 | 0.40 | 1.21 | |
| MetS by IDF | BMI | 0.90 | 0.73 | 0.84 | 0.58 | 23.58 |
| %BF | 0.88 | 0.80 | 0.79 | 0.59 | 31.90 | |
| WHR | 0.90 | 0.87 | 0.80 | 0.67 | 0.85 | |
| WHtR | 0.96 | 0.95 | 0.87 | 0.82 | 0.51 | |
| AVI | 0.97 | 1.00 | 0.93 | 0.93 | 12.80 | |
| BRI | 0.96 | 0.95 | 0.87 | 0.82 | 3.60 | |
| ABSI | 0.81 | 0.78 | 0.69 | 0.47 | 0.08 | |
| BAI | 0.82 | 0.73 | 0.72 | 0.45 | 30.42 | |
| CI | 0.90 | 0.87 | 0.80 | 0.67 | 1.21 |
| Index | Men * | Women ** | ||
|---|---|---|---|---|
| OR + | 95%CI | OR + | 95%CI | |
| Body mass index (BMI) | 4.10 | 3.18; 5.29 | 4.67 | 3.73; 5.84 |
| Body fat percentage (%) | 4.12 | 3.15; 5.38 | 4.31 | 3.45; 5.39 |
| Waist–hip ratio (WHR) | 3.80 | 2.97; 4.87 | 3.79 | 3.02; 4.75 |
| Waist–height ratio (WHtR) | 5.04 | 3.94; 6.45 | 6.14 | 4.87; 7.74 |
| Abdominal Volume Index (AVI) | 4.62 | 3.60; 5.93 | 6.82 | 4.15; 7.97 |
| Body roundness index (BRI) | 5.27 | 4.11; 6.75 | 6.25 | 4.95; 7.89 |
| A body shape index (ABSI) | 2.12 | 1.66; 2.70 | 2.05 | 1.63; 2.58 |
| Body adiposity index (BAI) | 2.76 | 2.15; 3.53 | 3.08 | 2.48; 3.83 |
| Conicity index (CI) | 3.57 | 2.79; 4.58 | 3.52 | 2.82; 4.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dang, A.K.; Truong, M.T.; Le, H.T.; Nguyen, K.C.; Le, M.B.; Nguyen, L.T.; Do, K.N.; Nguyen, L.H.T.; Mamun, A.A.; Phung, D.; et al. Anthropometric Cut-Off Values for Detecting the Presence of Metabolic Syndrome and Its Multiple Components among Adults in Vietnam: The Role of Novel Indices. Nutrients 2022, 14, 4024. https://doi.org/10.3390/nu14194024
Dang AK, Truong MT, Le HT, Nguyen KC, Le MB, Nguyen LT, Do KN, Nguyen LHT, Mamun AA, Phung D, et al. Anthropometric Cut-Off Values for Detecting the Presence of Metabolic Syndrome and Its Multiple Components among Adults in Vietnam: The Role of Novel Indices. Nutrients. 2022; 14(19):4024. https://doi.org/10.3390/nu14194024
Chicago/Turabian StyleDang, Anh Kim, Mai Tuyet Truong, Huong Thi Le, Khan Cong Nguyen, Mai Bach Le, Lam Thi Nguyen, Khanh Nam Do, Lan Huong Thi Nguyen, Abdullah A. Mamun, Dung Phung, and et al. 2022. "Anthropometric Cut-Off Values for Detecting the Presence of Metabolic Syndrome and Its Multiple Components among Adults in Vietnam: The Role of Novel Indices" Nutrients 14, no. 19: 4024. https://doi.org/10.3390/nu14194024
APA StyleDang, A. K., Truong, M. T., Le, H. T., Nguyen, K. C., Le, M. B., Nguyen, L. T., Do, K. N., Nguyen, L. H. T., Mamun, A. A., Phung, D., & Thai, P. K. (2022). Anthropometric Cut-Off Values for Detecting the Presence of Metabolic Syndrome and Its Multiple Components among Adults in Vietnam: The Role of Novel Indices. Nutrients, 14(19), 4024. https://doi.org/10.3390/nu14194024