

Description of Ultra-Processed Food Intake in a Swiss Population-Based Sample of Adults Aged 18 to 75 Years

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Dietary Assessment in the Swiss National Nutrition Survey
2.3. Food Classification According to Processing
2.4. Food Grouping
2.5. Sociodemographic Characteristics
2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
3.2. Consumption of UPFs according to Characteristics of Participants
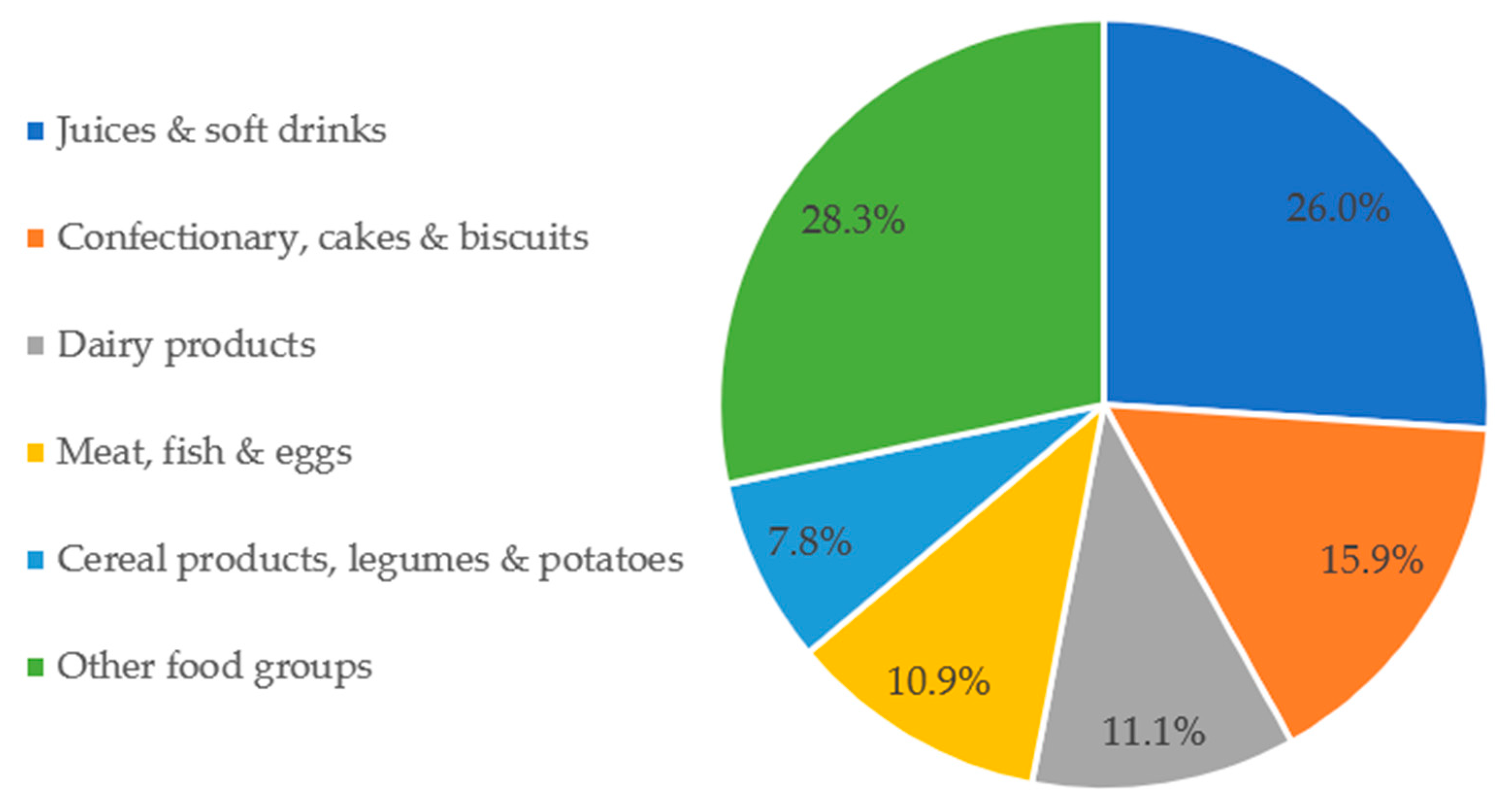
3.3. Distribution of Energy Intake (Kcal) from UPFs by Food Group
3.4. Distribution of Weight of Total Diet (Grams) from UPFs by Food Group
3.5. Contribution of UPFs to Intake of Macro- and Micronutrients
4. Discussion
4.1. Principal Findings
4.2. Consumption of UPFs according to Countries
4.3. Consumption of UPFs according to Characteristics of Participants
4.4. Distribution of Energy Intake from UPFs by Food Group
4.5. Distribution of Intake from UPFs (Grams/Day) by Food Group
4.6. Nutrition Profile of UPFs
4.7. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.C.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-Processed Foods: What They Are and How to Identify Them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Martinez Steele, E.M.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The share of ultra-processed foods and the overall nutritional quality of diets in the US: Evidence from a nationally representative cross-sectional study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- Louzada, M.L.D.C.; Martins, A.P.B.; Canella, D.; Baraldi, L.; Levy, R.B.; Claro, R.; Moubarac, J.-C.; Cannon, G.; Monteiro, C.A. Impact of ultra-processed foods on micronutrient content in the Brazilian diet. Rev. Saúde Pública 2015, 49, 1–8. [Google Scholar] [CrossRef]
- Gupta, S.; Hawk, T.; Aggarwal, A.; Drewnowski, A. Characterizing Ultra-Processed Foods by Energy Density, Nutrient Density, and Cost. Front. Nutr. 2019, 6, 70. [Google Scholar] [CrossRef] [Green Version]
- Fardet, A.; Rock, E. Chronic diseases are first associated with the degradation and artificialization of food matrices rather than with food composition: Calorie quality matters more than calorie quantity. Eur. J. Nutr. 2022, 61, 2239–2253. [Google Scholar] [CrossRef]
- Thorning, T.K.; Bertram, H.C.; Bonjour, J.-P.; De Groot, L.; Dupont, D.; Feeney, E.; Ipsen, R.; Lecerf, J.M.; Mackie, A.; McKinley, M.C.; et al. Whole dairy matrix or single nutrients in assessment of health effects: Current evidence and knowledge gaps. Am. J. Clin. Nutr. 2017, 105, 1033–1045. [Google Scholar] [CrossRef] [Green Version]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of ultra-processed foods and health status: A systematic review and meta-analysis. Br. J. Nutr. 2020, 125, 308–318. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, Z.; Yang, H.; Qiu, P.; Wang, H.; Wang, F.; Zhao, Q.; Fang, J.; Nie, J. Consumption of ultra-processed foods and health outcomes: A systematic review of epidemiological studies. Nutr. J. 2020, 19, 86. [Google Scholar] [CrossRef]
- Askari, M.; Heshmati, J.; Shahinfar, H.; Tripathi, N.; Daneshzad, E. Ultra-processed food and the risk of overweight and obesity: A systematic review and meta-analysis of observational studies. Int. J. Obes. 2020, 44, 2080–2091. [Google Scholar] [CrossRef]
- Moradi, S.; Entezari, M.H.; Mohammadi, H.; Jayedi, A.; Lazaridi, A.-V.; Kermani, M.A.H.; Miraghajani, M. Ultra-processed food consumption and adult obesity risk: A systematic review and dose-response meta-analysis. Crit. Rev. Food Sci. Nutr. 2021, 1–12. [Google Scholar] [CrossRef]
- Pestoni, G.; Habib, L.; Reber, E.; Rohrmann, S.; Staub, K.; Stanga, Z.; Faeh, D. Ultraprocessed Food Consumption is Strongly and Dose-Dependently Associated with Excess Body Weight in Swiss Women. Obesity 2021, 29, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Marino, M.; Puppo, F.; Del Bo’, C.; Vinelli, V.; Riso, P.; Porrini, M.; Martini, D. A Systematic Review of Worldwide Consumption of Ultra-Processed Foods: Findings and Criticisms. Nutrients 2021, 13, 2778. [Google Scholar] [CrossRef] [PubMed]
- Chatelan, A.; Beer-Borst, S.; Randriamiharisoa, A.; Pasquier, J.; Blanco, J.M.; Siegenthaler, S.; Paccaud, F.; Slimani, N.; Nicolas, G.; Camenzind-Frey, E.; et al. Major Differences in Diet across Three Linguistic Regions of Switzerland: Results from the First National Nutrition Survey menuCH. Nutrients 2017, 9, 1163. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, L.G.; Martinez Steele, E.; Canella, D.S.; Monteiro, C.A. Consumption of Ultra-Processed Foods and Associated Sociodemographic Factors in the USA between 2007 and 2012: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2018, 8, e020574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, G.C.; Julia, C.; Deschamps, V.; Srour, B.; Hercberg, S.; Kesse-Guyot, E.; Allès, B.; Chazelas, E.; Deschasaux, M.; Touvier, M.; et al. Consumption of Ultra-Processed Food and Its Association with Sociodemographic Characteristics and Diet Quality in a Representative Sample of French Adults. Nutrients 2021, 13, 682. [Google Scholar] [CrossRef] [PubMed]
- Nardocci, M.; Leclerc, B.-S.; Louzada, M.-L.; Monteiro, C.A.; Batal, M.; Moubarac, J.-C. Consumption of ultra-processed foods and obesity in Canada. Can. J. Public Health 2019, 110, 4–14. [Google Scholar] [CrossRef]
- Marchese, L.; Livingstone, K.M.; Woods, J.L.; Wingrove, K.; Machado, P. Ultra-processed food consumption, socio-demographics and diet quality in Australian adults. Public Health Nutr. 2021, 25, 94–104. [Google Scholar] [CrossRef]
- Moubarac, J.-C.; Batal, M.; Louzada, M.L.; Steele, E.M.; Monteiro, C.A. Consumption of Ultra-Processed Foods Predicts Diet Quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef]
- Vandevijvere, S.; De Ridder, K.; Fiolet, T.; Bel, S.; Tafforeau, J. Consumption of ultra-processed food products and diet quality among children, adolescents and adults in Belgium. Eur. J. Nutr. 2018, 58, 3267–3278. [Google Scholar] [CrossRef]
- Chatelan, A.; Gaillard, P.; Kruseman, M.; Keller, A. Total, Added, and Free Sugar Consumption and Adherence to Guidelines in Switzerland: Results from the First National Nutrition Survey menuCH. Nutrients 2019, 11, 1117. [Google Scholar] [CrossRef]
- Chatelan, A.; Marques-Vidal, P.; Bucher, S.; Siegenthaler, S.; Metzger, N.; Zuberbühler, C.A.; Camenzind-Frey, E.; Reggli, A.; Bochud, M.; Beer-Borst, S. Lessons Learnt About Conducting a Multilingual Nutrition Survey in Switzerland: Results from menuCH Pilot Survey. Int. J. Vitam. Nutr. Res. 2017, 87, 25–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slimani, N.; Casagrande, C.; Nicolas, G.; Freisling, H.; Huybrechts, I.; Ocké, M.C.; Niekerk, E.M.; Van Rossum, C.; Bellemans, M.; De Maeyer, M.; et al. The standardized computerized 24-h dietary recall method EPIC-Soft adapted for pan-European dietary monitoring. Eur. J. Clin. Nutr. 2011, 65, S5–S15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crispim, S.P.; De Vries, J.H.M.; Geelen, A.; Souverein, O.W.; Hulshof, P.J.M.; Lafay, L.; Rousseau, A.-S.; Lillegaard, I.T.L.; Andersen, L.F.; Huybrechts, I.; et al. Two non-consecutive 24 h recalls using EPIC-Soft software are sufficiently valid for comparing protein and potassium intake between five European centres—Results from the European Food Consumption Validation (EFCOVAL) study. Br. J. Nutr. 2010, 105, 447–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camenzind-Frey, E.; Zuberbühler, C. menuCH—Schweizerisches Fotobuch/Livre Photo Suisse/Manuale Fotografico Svizzero (menuCH Picture Book); Federal Office of Public Health & Federal Food Safety and Veterinary Office: Bern, Switzerland, 2014. [Google Scholar]
- Federal Food Safety and Veterinary Office FSVO. The Swiss Food Composition Database. Available online: https://www.valeursnutritives.ch/fr/ (accessed on 5 October 2020).
- Juul, F.; Martinez-Steele, E.; Parekh, N.; Monteiro, C.A.; Chang, V.W. Ultra-processed food consumption and excess weight among US adults. Br. J. Nutr. 2018, 120, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Martínez Steele, E.; Baraldi, L.G.; da Costa Louzada, M.L.; Moubarac, J.-C.; Mozaffarian, D.; Monteiro, C.A. Ultra-Processed Foods and Added Sugars in the US Diet: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [Green Version]
- Open Food Facts—Suisse. Available online: https://ch-fr.openfoodfacts.org (accessed on 20 April 2022).
- Swiss Society for Nutrition; Federal Food Safety and Veterinary Office. Pyramide Alimentaire Suisse 2011 (Swiss Food Pyramid). Available online: https://www.sge-ssn.ch/fr/toi-et-moi/boire-et-manger/equilibre-alimentaire/pyramide-alimentaire-suisse/ (accessed on 9 June 2022).
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.B.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the healthy eating index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djupegot, I.L.; Nenseth, C.B.; Bere, E.; Bjørnarå, H.B.T.; Helland, S.H.; Øverby, N.C.; Torstveit, M.K.; Stea, T.H. The association between time scarcity, sociodemographic correlates and consumption of ultra-processed foods among parents in Norway: A cross-sectional study. BMC Public Health 2017, 17, 447. [Google Scholar] [CrossRef]
- Monsivais, P.; Aggarwal, A.; Drewnowski, A. Time Spent on Home Food Preparation and Indicators of Healthy Eating. Am. J. Prev. Med. 2014, 47, 796–802. [Google Scholar] [CrossRef] [Green Version]
- Qutteina, Y.; Hallez, L.; Mennes, N.; De Backer, C.; Smits, T. What Do Adolescents See on Social Media? A Diary Study of Food Marketing Images on Social Media. Front. Psychol. 2019, 10, 2637. [Google Scholar] [CrossRef]
- Bochud, M.; Chatelan, A.; Blanco, J.M.; Beer-Borst, S.M. Anthropometric Characteristics and Indicators of Eating and Physical Activity Behaviors in the Swiss Adult Population: Results from menuCH 2014–2015; The Federal Office of Public Health and the Food Safety and Veterinary Office: Bern, Switzerland, 2017. [Google Scholar] [CrossRef]
- Federal Statistical Office. Foreign Population. Available online: https://www.bfs.admin.ch/bfs/en/home/statistiken/bevoelkerung/migration-integration/auslaendische-bevoelkerung.html (accessed on 6 May 2022).
- Dinu, M.; Asensi, M.T.; Pagliai, G.; Lotti, S.; Martini, D.; Colombini, B.; Sofi, F. Consumption of Ultra-Processed Foods Is Inversely Associated with Adherence to the Mediterranean Diet: A Cross-Sectional Study. Nutrients 2022, 14, 2073. [Google Scholar] [CrossRef]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; Da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2018, 72, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Moubarac, J.-C.; Levy, R.B.; Canella, D.S.; da Costa Louzada, M.L.; Cannon, G. Household Availability of Ultra-Processed Foods and Obesity in Nineteen European Countries. Public Health Nutr. 2018, 21, 18–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Mestral, C.; Khalatbari-Soltani, S.; Stringhini, S.; Marques-Vidal, P. Perceived barriers to healthy eating and adherence to dietary guidelines: Nationwide study. Clin. Nutr. 2019, 39, 2580–2585. [Google Scholar] [CrossRef]
- Lawrence, E.M. Why Do College Graduates Behave More Healthfully Than Those Who Are Less Educated? J. Health Soc. Behav. 2017, 58, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Powdthavee, N. Does more education lead to better health habits? Evidence from the school reforms in Australia. Soc. Sci. Med. 2015, 127, 83–91. [Google Scholar] [CrossRef]
- Raghupathi, V.; Raghupathi, W. The influence of education on health: An empirical assessment of OECD countries for the period 1995–2015. Arch. Public Health 2020, 78, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mertens, E.; Colizzi, C.; Peñalvo, J.L. Ultra-processed food consumption in adults across Europe. Eur. J. Nutr. 2021, 61, 1521–1539. [Google Scholar] [CrossRef]
- Chocosuisse. Available online: https://www.chocosuisse.ch/en/services/facts-figures (accessed on 7 May 2022).
- Julia, C.; Martinez, L.; Allès, B.; Touvier, M.; Hercberg, S.; Méjean, C.; Kesse-Guyot, E. Contribution of ultra-processed foods in the diet of adults from the French NutriNet-Santé study. Public Health Nutr. 2018, 21, 27–37. [Google Scholar] [CrossRef] [Green Version]
- de Deus Mendonça, R.; Pimenta, A.M.; Gea, A.; De La Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Lopes, A.C.S.; Bes-Rastrollo, M. Ultraprocessed food consumption and risk of overweight and obesity: The University of Navarra Follow-Up (SUN) cohort study. Am. J. Clin. Nutr. 2016, 104, 1433–1440. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a WHO Study Group; Technical report series; World Health Organization: Geneva, Switzerland, 1995; ISBN 978-92-4-120797-3. [Google Scholar]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [Green Version]
- Leyvraz, M.; Chatelan, A.; Da Costa, B.R.; Taffé, P.; Paradis, G.; Bovet, P.; Bochud, M.; Chiolero, A. Sodium intake and blood pressure in children and adolescents: A systematic review and meta-analysis of experimental and observational studies. Int. J. Epidemiol. 2018, 47, 1796–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauber, F.; Louzada, M.L.D.C.; Steele, E.M.; Rezende, L.; Millett, C.; A Monteiro, C.; Levy, R.B. Ultra-processed foods and excessive free sugar intake in the UK: A nationally representative cross-sectional study. BMJ Open 2019, 9, e027546. [Google Scholar] [CrossRef] [PubMed]
- Rauber, F.; da Costa Louzada, M.L.; Steele, E.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008–2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef] [Green Version]
- Gentry, M. World Cancer Research Fund International (WCRF). Impact 2017, 2017, 32–33. [Google Scholar] [CrossRef]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef]
- GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.; Hofman, K.; Moubarac, J.-C.; Thow, A.M. Public health response to ultra-processed food and drinks. BMJ 2020, 369, m2391. [Google Scholar] [CrossRef]
- DAPA Measurement2 Toolkit. Available online: https://dapa-toolkit.mrc.ac.uk/diet/subjective-methods/24-hour-dietary-recall (accessed on 7 October 2020).
- FAO. Guidelines on the Collection of Information on Food Processing through Food Consumption Surveys; FAO: Rome, Italy, 2015. [Google Scholar]
- Popkin, B.M.; Barquera, S.; Corvalan, C.; Hofman, K.J.; Monteiro, C.; Ng, S.W.; Swart, E.C.; Taillie, L.S. Towards unified and impactful policies to reduce ultra-processed food consumption and promote healthier eating. Lancet Diabetes Endocrinol. 2021, 9, 462–470. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N (%) | TEI (kcal/Day) | UPF Consumption (kcal/Day) 1 | UPF Consumption (%TEI) 2 | p-Value 3 | p-Value 4 | |||
|---|---|---|---|---|---|---|---|---|---|
| Medians | P25–P75 | Medians | P25–P75 | Medians | P25–P75 | ||||
| All participants | 2085 (100.0) | 2089 | 1665–2552 | 587 | 364–885 | 28.7 | 19.9–38.9 | ||
| Sex | 0.125 | 0.012 * | |||||||
| Women | 1139 (54.6) | 1842 | 1527–2216 | 517 | 325–746 | 28.4 | 19.4–38.5 | ||
| Men | 946 (45.4) | 2417 | 1987–2993 | 703 | 445–1056 | 29.2 | 20.8–39.9 | ||
| Age groups, years | 0.001 * | 0.001 * | |||||||
| 18–29 | 407 (19.5) | 2221 | 1709–2731 | 727 | 478–1060 | 34.8 | 24.5–45.0 | ||
| 30–39 | 327 (15.7) | 2126 | 1700–2669 | 646 | 418–963 | 31.8 | 22.3–42.0 | ||
| 40–49 | 450 (21.6) | 2110 | 1702–2583 | 599 | 380–883 | 28.2 | 20.3–37.8 | ||
| 50–64 | 562 (27.0) | 2021 | 1640–2507 | 519 | 308–811 | 25.5 | 16.9–36.6 | ||
| 65–75 | 339 (16.3) | 1978 | 1641–2331 | 495 | 314–714 | 26.3 | 17.1–35.0 | ||
| Linguistic region | 0.003 * | 0.002 * | |||||||
| German | 1359 (65.2) | 2153 | 1721–2612 | 617 | 399–915 | 29.6 | 20.9–39.6 | ||
| French | 510 (24.5) | 1991 | 1647–2467 | 526 | 323–789 | 27.2 | 17.7–37.1 | ||
| Italian | 216 (10.4) | 1930 | 1515–2319 | 509 | 298–820 | 28.0 | 16.9–39.4 | ||
| 1st nationality 5 | 0.009 * | 0.002 * | |||||||
| Swiss | 1751 (84.0) | 2078 | 1665–2550 | 595 | 379–894 | 29.2 | 20.3–39.0 | ||
| Non-Swiss | 330 (15.8) | 2124 | 1654–2571 | 557 | 318–839 | 26.1 | 17.5–37.1 | ||
| Household size 5 | 0.060 | 0.400 | |||||||
| One person | 338 (16.2) | 1996 | 1621–2446 | 573 | 330–892 | 29.0 | 18.5–40.6 | ||
| Two people | 825 (39.6) | 2070 | 1669–2514 | 565 | 353–835 | 28.1 | 19.7–37.3 | ||
| Three people | 336 (16.1) | 2103 | 1728–2522 | 591 | 371–901 | 28.8 | 19.5–39.7 | ||
| Four people and more | 582 (27.9) | 2132 | 1688–2678 | 626 | 407–945 | 30.2 | 21.5–40.1 | ||
| Education 5 | 0.073 | 0.060 | |||||||
| Primary & secondary | 1069 (51.3) | 1993 | 1588–2495 | 574 | 355–894 | 29.1 | 20.2–39.7 | ||
| Tertiary | 1012 (48.5) | 2160 | 1762–2617 | 604 | 373–870 | 28.4 | 19.6–38.4 | ||
| Food Groups | Total Intake (kcal/Day) | Contribution to TEI (%TEI) | UPF intake (kcal/Day) | UPF intake from Total Intake (%) 1 | UPF Intake from TEI (%TEI) 2 |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Confectionary, cakes & biscuits | 204 (216) | 9.0 (8.3) | 204 (214) | 99.6 (4.6) | 29.5 (23.9) |
| Meat, fish & eggs | 272 (218) | 12.6 (8.8) | 105 (150) | 35.3 (34.1) | 14.9 (18.6) |
| Cereal products, legumes & potatoes | 564 (310) | 25.6 (10.4) | 78 (109) | 14.8 (19.3) | 12.5 (16.8) |
| Juices & soft drinks | 97 (150) | 4.1 (5.5) | 65 (136) | 53.9 (44.4) | 8.0 (13.3) |
| Dairy products | 269 (208) | 12.4 (8.3) | 50 (86) | 16.6 (25.0) | 7.9 (13.9) |
| Seasoning, spices, yeast & herbs | 95 (100) | 4.4 (4.2) | 33 (62) | 32.2 (37.5) | 5.5 (10.1) |
| Added fats | 182 (152) | 8.3 (6.0) | 30 (75) | 15.8 (25.6) | 4.9 (10.0) |
| Salty snacks | 22 (75) | 1.0 (2.8) | 22 (75) | 100.0 (0.0) | 3.0 (8.5) |
| Sugar, honey, jam, sweet sauces & syrups | 60 (75) | 2.7 (3.2) | 18 (46) | 26.4 (38.0) | 2.9 (7.0) |
| Breakfast cereals | 29 (72) | 1.2 (3.1) | 19 (58) | 65.9 (44.9) | 2.7 (8.1) |
| Other foods | 14 (58) | 0. 7 (2.7) | 13 (58) | 94.1 (23.0) | 2.4 (9.3) |
| Ice-creams & milk-based desserts | 22 (54) | 1.0 (2.3) | 14 (38) | 74.4 (42.0) | 2.3 (6.5) |
| Alcoholic beverages substitutes | 107 (159) | 4.7 (6.5) | 13 (47) | 14.4 (29.6) | 1.9 (6.4) |
| Soups & broth | 21 (55) | 1.0 (2.8) | 5 (29) | 40.5 (48.3) | 0.7 (4.3) |
| Industrial dishes | 13 (65) | 0.6 (2.6) | 6 (45) | 40.2 (48.3) | 0.6 (4.4) |
| Other non-alcoholic beverages | 15 (33) | 0.8 (1.5) | 2 (12) | 2.26 (13.3) | 0.2 (2.3) |
| Nuts & seeds | 39 (84) | 1.7 (3.6) | 0 (0) | 0.0 (0.0) | 0.0 (0.0) |
| Fruit & vegetables | 159 (120) | 7.8 (6.1) | 0 (0) | 0.0 (0.0) | 0.0 (0.0) |
| Total | 2184 (750) | 100.0 | 676.3 (440.1) | - | 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertoni Maluf, V.A.; Bucher Della Torre, S.; Jotterand Chaparro, C.; Belle, F.N.; Khalatbari-Soltani, S.; Kruseman, M.; Marques-Vidal, P.; Chatelan, A. Description of Ultra-Processed Food Intake in a Swiss Population-Based Sample of Adults Aged 18 to 75 Years. Nutrients 2022, 14, 4486. https://doi.org/10.3390/nu14214486
Bertoni Maluf VA, Bucher Della Torre S, Jotterand Chaparro C, Belle FN, Khalatbari-Soltani S, Kruseman M, Marques-Vidal P, Chatelan A. Description of Ultra-Processed Food Intake in a Swiss Population-Based Sample of Adults Aged 18 to 75 Years. Nutrients. 2022; 14(21):4486. https://doi.org/10.3390/nu14214486
Chicago/Turabian StyleBertoni Maluf, Valeria A., Sophie Bucher Della Torre, Corinne Jotterand Chaparro, Fabiën N. Belle, Saman Khalatbari-Soltani, Maaike Kruseman, Pedro Marques-Vidal, and Angeline Chatelan. 2022. "Description of Ultra-Processed Food Intake in a Swiss Population-Based Sample of Adults Aged 18 to 75 Years" Nutrients 14, no. 21: 4486. https://doi.org/10.3390/nu14214486
APA StyleBertoni Maluf, V. A., Bucher Della Torre, S., Jotterand Chaparro, C., Belle, F. N., Khalatbari-Soltani, S., Kruseman, M., Marques-Vidal, P., & Chatelan, A. (2022). Description of Ultra-Processed Food Intake in a Swiss Population-Based Sample of Adults Aged 18 to 75 Years. Nutrients, 14(21), 4486. https://doi.org/10.3390/nu14214486