

How to Decide the Iodine Content in Salt for a Country—China as an Example
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Organizing Cooperating Departments
2.2. Information Collection
2.3. Field Investigation
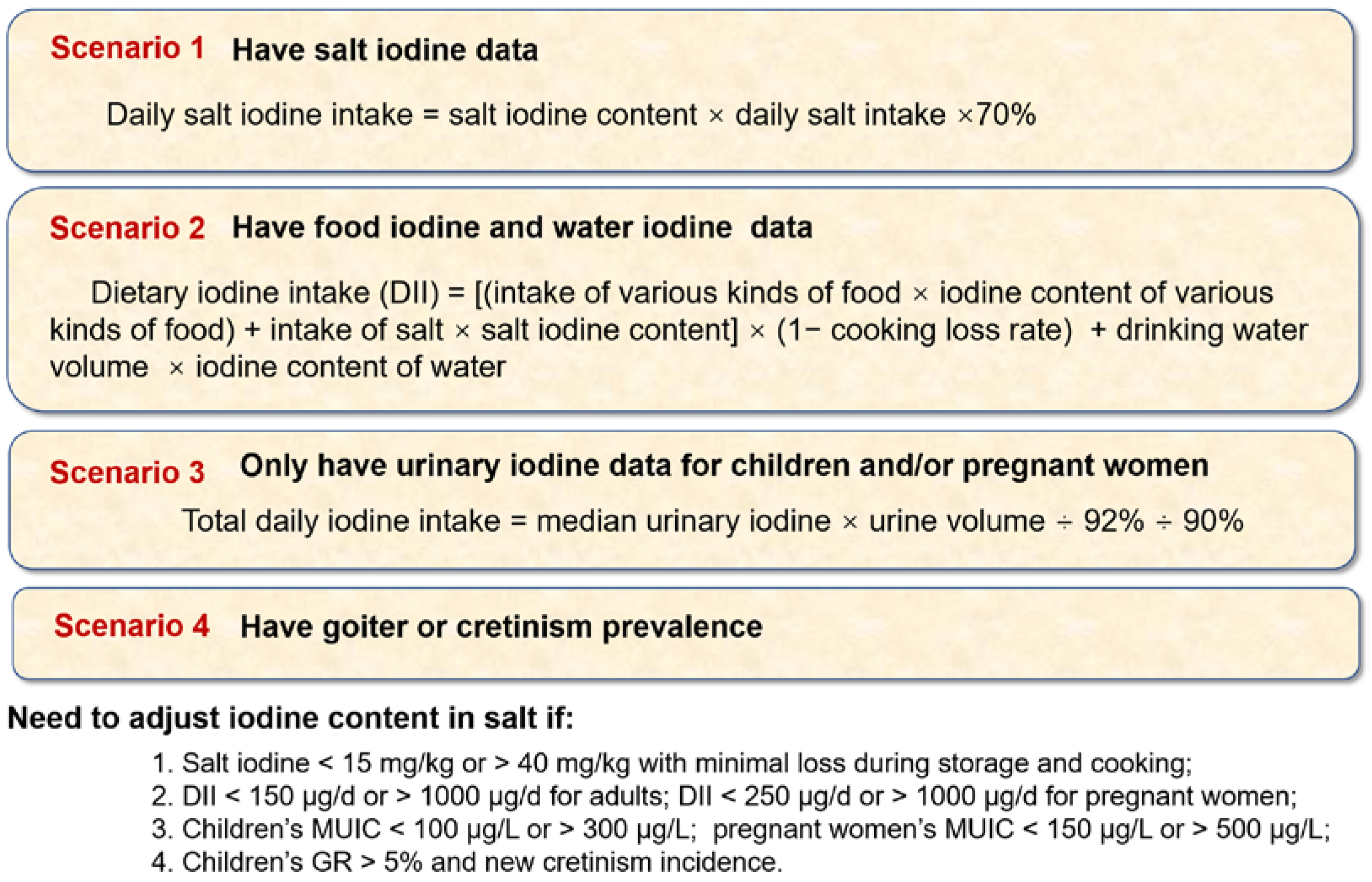
2.4. Calculation
2.5. Decision on the Iodine Content in Salt
2.6. Verification and Evaluation
3. Results
3.1. Information Collection
3.2. Field Investigation
3.3. Determination and Verification
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morreale de Escobar, G.; Obregon, M.J.; Escobar del Rey, F. Role of thyroid hormone during early brain development. Eur. J. Endocrinol. 2004, 151 (Suppl. 3), U25–U37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO/UNICEF/ICCIDD. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination, a Guide for Programme Managers, 3rd ed.; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Zimmermann, M.B.; Boelaert, K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015, 4, 286–295. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Andersson, M. Global endocrinology: Global perspectives in endocrinology: Coverage of iodized salt programs and iodine status in 2020. Eur. J. Endocrinol. 2021, 1, R13–R21. [Google Scholar] [CrossRef]
- WHO. Guideline: Fortification of Food-Grade Salt with Iodine for the Prevention and Control of Iodine Deficiency Disorders; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Leung, A.M.; Braverman, L.E. Consequences of excess iodine. Nat. Rev. Endocrinol. 2014, 3, 136–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farebrother, J.; Zimmermann, M.B.; Andersson, M. Excess iodine intake: Sources, assessment, and effects on thyroid function. Ann. N. Y. Acad. Sci. 2019, 1, 44–65. [Google Scholar] [CrossRef]
- Sun, D.; Codling, K.; Chang, S.; Zhang, S.; Shen, H.; Su, X.; Chen, Z.; Scherpbier, R.W.; Yan, J. Eliminating iodine deficiency in China: Achievements, challenges and global implications. Nutrients 2017, 4, 361. [Google Scholar] [CrossRef]
- WHO/UNICEF/ICCIDD. Indicators for Assessing Iodine Deficiency Disorders and Their Control through Salt Iodization; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- GB 16006-1995; Criteria of Elimination on Iodine Deficiency Disorders. Standards Press of China: Beijing, China, 1996. Available online: https://www.doc88.com/p-90927813100.html (accessed on 1 July 2022).
- Liu, P.; Fan, L.; Meng, F.; Su, X.; Liu, S.; Shen, H.; Sun, D. Prevention and control of iodine deficiency disorders—China, 1995–2020. China CDC Wkly. 2020, 20, 345–349. [Google Scholar] [CrossRef] [PubMed]
- GB5461-2000; Edible Salt. Standards Press of China: Beijing, China, 2000. Available online: https://openstd.samr.gov.cn/bzgk/gb/newGbInfo?hcno=17E41516849AF0F776DDED38C8F8A85C (accessed on 1 July 2022).
- GB26878-2011; National Standard for Food Safety: Iodine Content in Edible Salt. Standards Press of China: Beijing, China, 2011. Available online: http://down.foodmate.net/standard/yulan.php?itemid=28365 (accessed on 1 July 2022).
- Endemic Disease Control Center of Chinese Center for Disease Control and Prevention. Investigation Report on the Assessment of Iodine Deficiency Disorders Elimination; Chinese National Health Report; CDC: Beijing, China, 2020. [Google Scholar]
- Endemic Disease Control Center of Chinese Center for Disease Control and Prevention. The Report of the National Survey on Iodine in Drinking Water; Chinese National Health Report; CDC: Beijing, China, 2019. Available online: http://www.nhc.gov.cn/jkj/s5874/201905/bb1da1f5e47040e8820b9378e6db4bd3.shtml (accessed on 15 June 2022).
- Yang, Y.X. Chinese Food Composition Standard Edition (6th Edition); Peking University Medical Press: Beijing, China, 2019. (in Chinese) [Google Scholar]
- WS/T107.1-2016; Determination of Iodine in Urine—Part 1: As3+-Ce4+ Catalytic Spectrophotometry. Standards Press of China: Beijing, China, 2016. Available online: http://www.nhc.gov.cn/fzs/s7852d/201605/39b5a03b8531403496f0c2f6b4f41f46.shtml (accessed on 1 July 2022).
- GB/T 13026.7-2012; Determination of Iodine of General Test Method in Salt Industry. Standards press of China: Beijing, China, 2006. Available online: https://openstd.samr.gov.cn/bzgk/gb/newGbInfo?hcno=85D289F3BCE6F6A31822CD0BDAAA7579 (accessed on 15 June 2022).
- National Center for Iodine Deficiency Disorders Reference Laboratory of the Chinese Center for Disease Control and Prevention. The Method Suitable for the Detection of Water Iodine in Iodine-Deficient and High-Iodine Areas. 2012. (A Chinese Recommended Method). Available online: https://wenku.baidu.com/view/407b266cbd1e650e52ea551810a6f524ccbfcbf4.html (accessed on 15 June 2022).
- Chinese Nutrition Society. The Chinese Dietary Guidelines (2016); People’s Medical Publishing House: Beijing, China, 2016; (Chinese Dietary Guideline). [Google Scholar]
- WS/T 669-2020; Definition and Demarcation of Iodine Deficient Areas and Iodine Adequate Areas. Standards Press of China: Beijing, China, 2020. Available online: http://www.nhc.gov.cn/fzs/s7852d/202003/bf5ad1fbcde44ef096ca3fb28e731134.shtml (accessed on 1 July 2022).
- GB16006-2008; Criteria of Elimination on Iodine Deficiency Disorders. Standards Press of China: Beijing, China, 2008. Available online: http://www.nhc.gov.cn/wjw/s9500/201410/5405a2af749c4c079e239637937404c1.shtml (accessed on 1 July 2022).
- Endemiology Society of Chinese Medical Association, Chinese Nutrition Society, Endocrinology Society of Chinese Medical Association. Guidelines for Iodine Supplementation for Chinese Residents; People’s Medical Publishing House: Beijing, China, 2019; (Chinese Dietary Guideline). [Google Scholar]
- Tan, M.; He, F.J.; Wang, C.; MacGregor, G.A. Twenty-four-hour urinary sodium and potassium excretion in China: A systematic review and meta-analysis. J. Am. Heart Assoc. 2019, 37, e12. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, H.; Wang, Z.; Du, W.; Su, C.; Huang, F.; Jia, X.; Ouyang, Y.; Li, L.; Wang, Y.; et al. Trends in adult cooking salt intake—China, 1991–2018. China CDC Wkly. 2020, 7, 104–108. [Google Scholar] [CrossRef]
- Xu, J.; Liu, L.; Wang, J.; Ma, W.; Zhang, J.; Wang, H.; Cao, X.; Li, X.; Gu, Y. Stability analysis of iodine content in potassium iodide iodized salt and potassium iodate iodized salt during production. Chin. J. Endem. 2018, 37, 441–445. [Google Scholar] [CrossRef]
- Shawel, D.; Hagos, S.; Lachat, C.K.; Kimanya, M.E.; Kolsteren, P. Post-production losses in iodine concentration of salt hamper the control of iodine deficiency disorders: A case study in northern Ethiopia. J. Health Popul. Nutr. 2010, 3, 238–244. [Google Scholar] [CrossRef] [Green Version]
- WHO. Salt Reduction and Iodine Fortification Strategies in Public Health: Report of a Joint Technical Meeting; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Tan, H.; Luo, X.; Liu, Y.; Liu, X.; Li, L.; Liu, X.; Wang, Z.; Wang, J. Detection and correlation between the content of sodium and iodine in pre-packaged foods. Wei Sheng Yan Jiu 2020, 6, 1002–1007. [Google Scholar] [CrossRef]
- Chen, Z.H.; Zhao, Y.G.; WU, J.N. Analysis of the iodine content of condiment in Fuzhou market. Chin J. Contr. Endem. Dis. 2012, 4, 245–247. [Google Scholar]
- Iodine Global Network. Global Scorecard of Iodine Nutrition in 2020 in the General Population Based on School-Age Children (SAC); IGN: Ottawa, ON, Canada, 2021. [Google Scholar]
- Zimmermann, M.B.; Jooste, P.L.; Pandav, C.S. Iodine-deficiency disorders. Lancet 2008, 4, 1251–1262. [Google Scholar] [CrossRef]
- Koukkou, E.G.; Roupas, N.D.; Markou, K.B. Effect of excess iodine intake on thyroid on human health. Minerva. Med. 2017, 108, 136–146. [Google Scholar] [CrossRef]
- Bülow, P.I.; Laurberg, P.; Knudsen, N.; Jørgensen, T.; Perrild, H.; Ovesen, L.; Rasmussen, L.B. Increase in incidence of hyperthyroidism predominantly occurs in young people after iodine fortifi cation of salt in Denmark. J. Clin. Endocrinol. Metab. 2006, 91, 3830–3834. [Google Scholar] [CrossRef] [Green Version]
- Dumont, J.E.; Ermans, A.M.; Maenhaut, C.; Coppée, F.; Stanbury, J.B. Large goitre as a maladaptation to iodine defi ciency. Clin. Endocrinol. 1995, 43, 1–10. [Google Scholar] [CrossRef]
- Bonglaisin, J.N.; Ngondé, E.; Tsafack, T.; Ngo Nlend, M.; Mbakop, C.D.; Wirsiy, E.; Kimoun, M.K.; Ekambi, M.A.; Lantum, D.N. Monitoring and impact evaluation of iodized salt intervention in Cameroon. Heliyon 2019, 5, e01670. [Google Scholar] [CrossRef] [Green Version]
- Thout, S.R.; Santos, J.A.; McKenzie, B.; Trieu, K.; Johnson, C.; McLean, R.; Arcand, J.; Campbell, N.R.C.; Webster, J. The Science of Salt: Updating the evidence on global estimates of salt intake. J. Clin. Hypertens. 2019, 21, 710–721. [Google Scholar] [CrossRef] [Green Version]
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D. Group (NutriCoDE) on behalf of the GB of DN and CDE. Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Su, X.; Li, M.; Shen, H.; Yu, J.; Kelly, P.J.; Meng, F.; Liu, L.; Fan, L.; Li, M.; et al. Should urinary iodine concentrations of school-aged children continue to be used as proxy for different populations? Analysis of data from Chinese national surveys. Br. J. Nutr. 2016, 6, 1068–1076. [Google Scholar] [CrossRef] [PubMed]
- WHO. Salt Reduction and Iodine Fortification Strategies in Public Health; WHO: Canberra, Australia, 2013. [Google Scholar]
- Chinese State Council. Opinions on the Implementation of Healthy China Action; 2019 (A Chinese Document). Available online: http://www.nhc.gov.cn/guihuaxxs/s3585u/201912/d4e000784b2946588fd28cee95dfbdc8.shtml (accessed on 1 July 2022).
- Blankenship, J.L.; Garrett, G.S.; Khan, N.A.; De-Regil, L.M.; Spohrer, R.; Gorstein, J. Effect of iodized salt on organoleptic properties of processed foods: A systematic review. J. Food Sci. Technol. 2018, 55, 3341–3352. [Google Scholar] [CrossRef] [PubMed]
- Knowles, J.; van der Haar, F.; Shehata, M.; Gerasimov, G.; Bimo, B.; Cavenagh, B. Iodine intake through processed food: Case studies from Egypt, Indonesia, the Philippines, the Russian Federation and Ukraine, 2010–2015. Nutrients 2017, 9, 797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesar, J.A.; Santos, I.S.; Black, R.E.; Chrestani, M.; Duarte, F.A.; Nilson, E. Iodine status of Brazilian school-age children: A national cross-sectional survey. Nutrients 2020, 12, 1077. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | District | N | MUIC (μg/L) Median, P25−P75 | Salt Iodine (mg/kg) ± s | Consumption Rate (%) | Contribution Proportion (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Salt 1 | Iodine Preparations | Iodine−Rich Food | Salt 1 | Food | Water | Iodine Preparations | |||||
| Children | Fujian | 814 | 213.7, 136.0−309.6 | 21.7 ± 7.8 | 86.1 | − | 80.4 | 60.5 | 38.2 | 1.3 | − |
| Shanxi | 819 | 234.5, 129.1−382.5 | 25.2 ± 4.9 | 93.3 | − | 65.5 | 73.9 | 24.0 | 2.1 | − | |
| Yunnan | 400 | 250.6, 179.2−323.4 | 25.4 ± 3.7 | 96.0 | − | − | 56.8 | 40.6 | 2.6 | − | |
| Xinjiang | 804 | 258.0, 179.3−332.0 | 26.9 ± 4.0 | 92.9 | − | 77.9 | 97.3 | 1.2 | 1.4 | − | |
| Total | 2837 | 238.2, 154.1−335.5 | 24.8 ± 8.0 | 91.5 | − | 74.6 | 74.3 | 24.0 | 1.7 | − | |
| Adults | Fujian | 376 | 168.7, 103.6−228.7 | 24.6 ± 2.7 | 89.7 | 0.3 | 53.2 | 57.0 | 41.2 | 1.8 | − |
| Shanxi | 345 | 180.3, 104.1−259.9 | 25.6 ± 4.9 | 92.5 | 2.0 | 23.3 | 67.8 | 27.0 | 5.2 | − | |
| Yunnan | 388 | 186.7, 118.6−253.7 | 25.8 ± 2.8 | 98.5 | 0.7 | 37.0 | 64.5 | 32.7 | 2.8 | − | |
| Xinjiang | 384 | 224.3, 165.6−282.1 | 28.2 ± 5.3 | 94.5 | 0.5 | 7.8 | 42.6 | 56.8 | 0.6 | − | |
| Total | 1493 | 187.3, 122.8−258.1 | 26.1 ± 4.3 | 93.9 | 0.8 | 29.7 | 56.9 | 40.7 | 2.4 | − | |
| Pregnantwomen | Fujian | 338 | 145.4, 100.5−214.7 | 23.8 ± 5.4 | 100.0 | 10.7 | 66.6 | 50.6 | 41.1 | 1.0 | 7.3 |
| Shanxi | 874 | 161.5, 91.2−247.2 | 25.3 ± 5.4 | 96.6 | 2.0 | 32.5 | 53.3 | 43.3 | 2.7 | 0.7 | |
| Yunnan | 413 | 138.7, 91.9−192.8 | 26.0 ± 2.8 | 98.0 | 1.0 | 32.2 | 59.5 | 38.8 | 1.7 | − | |
| Xinjiang 2 | 503 | 216.2, 145.7−288.8 | 27.2 ± 4.1 | 78.4 | 7.6 | 20.8 | 20.6 | 20.2 | 1.5 | 57.7 | |
| Total | 2128 | 164.5, 104.8−243.0 | 25.7 ± 4.8 | 93.4 | 5.2 | 35.5 | 39.3 | 31.7 | 1.4 | 27.6 | |
| Iodine Content in Salt (mg/kg) | Children (μg/d) | Adults (μg/d) | Pregnant Women (μg/d) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Water 1 | Food | Salt 2 | Total | Water | Food | Salt | Total | Water | Food | Salt | Total | |
| Iodine-deficient areas | ||||||||||||
| 15 | 0–40 | 3.7–96.1 | 75.0 | 63.0–192.9 | 0–80 | 60–156 | 127.5 | 150.0–306.8 | 0–80 | 65–112 | 130.5 | 156.4–274.0 |
| 20 | 0–40 | 3.7–96.1 | 100.0 | 83.0–212.9 | 0–80 | 60–156 | 170.0 | 184.0–340.8 | 0–80 | 65–112 | 174.0 | 191.2–308.8 |
| 25 | 0–40 | 3.7–96.1 | 125.0 | 103.0–232.9 | 0–80 | 60–156 | 212.5 | 218.0–374.8 | 0–80 | 65–112 | 217.5 | 226.0–343.6 |
| 30 | 0–40 | 3.7–96.1 | 150.0 | 123.0–252.9 | 0–80 | 60–156 | 255.0 | 252.0–408.8 | 0–80 | 65–112 | 261.0 | 260.8–378.4 |
| 35 | 0–40 | 3.7–96.1 | 175.0 | 143.0–272.9 | 0–80 | 60–156 | 297.5 | 286.0–442.8 | 0–80 | 65–112 | 304.5 | 295.6–413.2 |
| 40 | 0–40 | 3.7–96.1 | 200.0 | 163.0–292.9 | 0–80 | 60–156 | 340.0 | 320.0–476.8 | 0–80 | 65–112 | 348.0 | 330.4–448.0 |
| 45 | 0–40 | 3.7–96.1 | 225.0 | 183.0–312.9 | 0–80 | 60–156 | 382.5 | 354.0–510.8 | 0–80 | 65–112 | 391.5 | 365.2–482.8 |
| Iodine-adequate areas | ||||||||||||
| 15 | 40–100 | 3.7–96.1 | 75.0 | 119.0–276.9 | 80–200 | 60–156 | 127.5 | 230.0–426.8 | 80–200 | 65–112 | 130.5 | 236.4–394.0 |
| 20 | 40–100 | 3.7–96.1 | 100.0 | 139.0–296.9 | 80–200 | 60–156 | 170.0 | 264.0–460.8 | 80–200 | 65–112 | 174.0 | 271.2–428.8 |
| 25 | 40–100 | 3.7–96.1 | 125.0 | 159.0–316.9 | 80–200 | 60–156 | 212.5 | 298.0–494.8 | 80–200 | 65–112 | 217.5 | 306.0–463.6 |
| 30 | 40–100 | 3.7–96.1 | 150.0 | 179.0–336.9 | 80–200 | 60–156 | 255.0 | 332.0–528.8 | 80–200 | 65–112 | 261.0 | 340.8–498.4 |
| 35 | 40–100 | 3.7–96.1 | 175.0 | 199.0–356.9 | 80–200 | 60–156 | 297.5 | 366.0–562.8 | 80–200 | 65–112 | 304.5 | 375.6–533.2 |
| 40 | 40–100 | 3.7–96.1 | 200.0 | 219.0–376.9 | 80–200 | 60–156 | 340.0 | 400.0–596.8 | 80–200 | 65–112 | 348.0 | 410.4–568.0 |
| 45 | 40–100 | 3.7–96.1 | 225.0 | 239.0–396.9 | 80–200 | 60–156 | 382.5 | 434.0–630.8 | 80–200 | 65–112 | 391.5 | 445.2–602.8 |
| Population | Iodine Content in Salt 1 (mg/kg) | P-SII 2 (μg/d) | P-TII 3 (μg/d) | E-MUIC 4 (μg/L) |
|---|---|---|---|---|
| Children | 15 | 60.0 | 173.5 | 179.6 |
| 20 | 80.0 | 193.5 | 200.3 | |
| 25 | 100.0 | 213.5 | 221.0 | |
| 30 | 120.0 | 233.5 | 241.7 | |
| 35 | 140.0 | 253.5 | 262.4 | |
| Adults | 15 | 112.1 | 230.3 | 136.2 |
| 20 | 149.5 | 267.7 | 158.3 | |
| 25 | 186.9 | 305.0 | 180.4 | |
| 30 | 224.2 | 342.4 | 202.5 | |
| 35 | 261.6 | 379.8 | 224.6 | |
| Pregnant women | 25 | 186.9 | 296.8 | 175.5 |
| 30 | 224.2 | 334.1 | 197.6 | |
| 35 | 261.6 | 371.5 | 219.7 | |
| 40 | 299.0 | 408.9 | 241.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, L.; Du, Y.; Meng, F.; Liu, L.; Li, M.; Liu, P.; Sun, D. How to Decide the Iodine Content in Salt for a Country—China as an Example. Nutrients 2022, 14, 4606. https://doi.org/10.3390/nu14214606
Fan L, Du Y, Meng F, Liu L, Li M, Liu P, Sun D. How to Decide the Iodine Content in Salt for a Country—China as an Example. Nutrients. 2022; 14(21):4606. https://doi.org/10.3390/nu14214606
Chicago/Turabian StyleFan, Lijun, Yang Du, Fangang Meng, Lixiang Liu, Ming Li, Peng Liu, and Dianjun Sun. 2022. "How to Decide the Iodine Content in Salt for a Country—China as an Example" Nutrients 14, no. 21: 4606. https://doi.org/10.3390/nu14214606
APA StyleFan, L., Du, Y., Meng, F., Liu, L., Li, M., Liu, P., & Sun, D. (2022). How to Decide the Iodine Content in Salt for a Country—China as an Example. Nutrients, 14(21), 4606. https://doi.org/10.3390/nu14214606