
Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey

 ,
,  , , , , , , , , ,
, , , , , , , , ,
Abstract
1. Introduction
2. Materials and Method
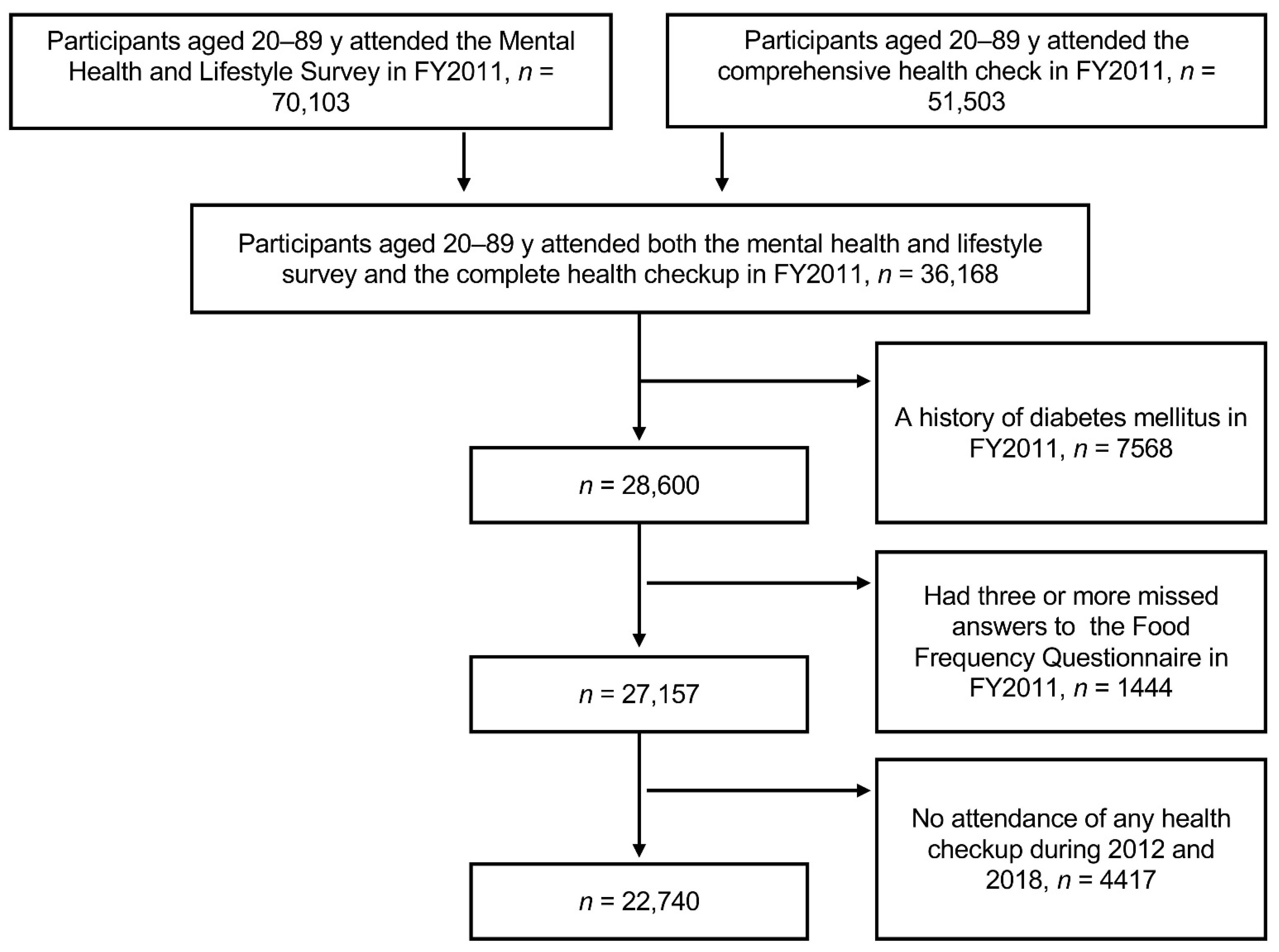
2.1. Study Design and Study Participants
2.2. Dietary Intake Assessment
2.3. Diabetes- and Disaster-Related Variables
2.4. Statistical Analysis
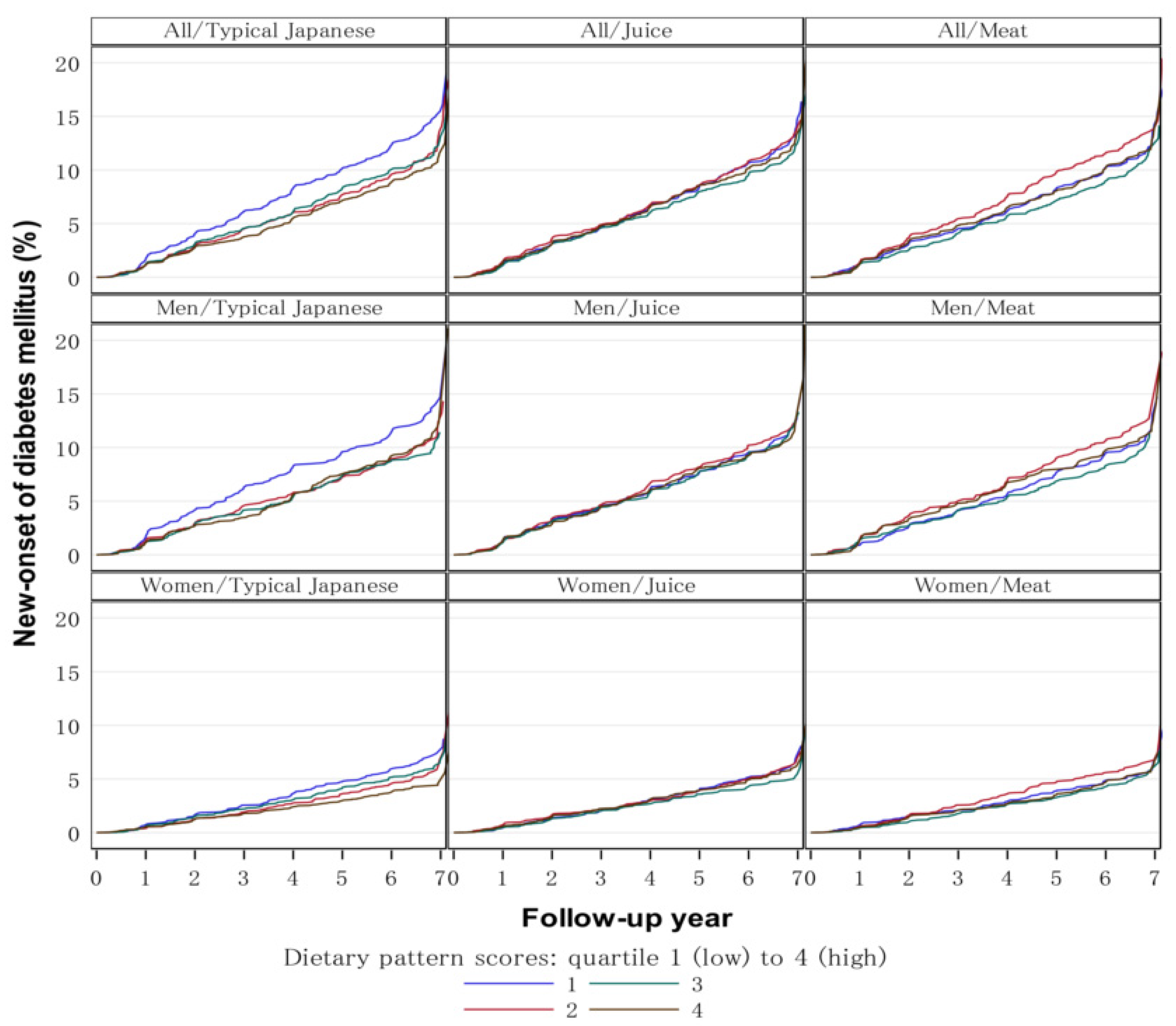
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [PubMed]
- Neuenschwander, M.; Ballon, A.; Weber, K.S.; Norat, T.; Aune, D.; Schwingshackl, L.; Schlesinger, S. Role of diet in type 2 diabetes incidence: Umbrella review of meta-analyses of prospective observational studies. BMJ 2019, 366, l2368. [Google Scholar] [CrossRef]
- Churuangsuk, C.; Hall, J.; Reynolds, A.; Griffin, S.J.; Combet, E.; Lean, M.E.J. Diets for weight management in adults with type 2 diabetes: An umbrella review of published meta-analyses and systematic review of trials of diets for diabetes remission. Diabetologia 2022, 65, 14–36. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G.; Lampousi, A.M.; Knüppel, S.; Iqbal, K.; Schwedhelm, C.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Boushey, C.; Ard, J.; Bazzano, L.; Heymsfield, S.; Mayer-Davis, E.; Sabaté, J.; Snetselaar, L.; Van Horn, L.; Schneeman, B.; English, L.K.; et al. USDA nutrition evidence systematic reviews. In Dietary Patterns and Risk of Type 2 Diabetes: A Systematic Review; USDA Nutrition Evidence Systematic Review: Alexandria, VA, USA, 2020. [Google Scholar]
- Sasaki, S. What is the scientific definition of the Japanese diet from the viewpoint of nutrition and health? Nutr. Rev. 2020, 78, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Mizoue, T.; Yamaji, T.; Tabata, S.; Yamaguchi, K.; Ogawa, S.; Mineshita, M.; Kono, S. Dietary patterns and glucose tolerance abnormalities in Japanese men. J. Nutr. 2006, 136, 1352–1358. [Google Scholar] [CrossRef] [PubMed]
- Okada, E.; Takahashi, K.; Nakamura, K.; Ukawa, S.; Takabayashi, S.; Nakamura, M.; Sasaki, S.; Tamakoshi, A.; Takimoto, H. Dietary patterns and abnormal glucose tolerance among Japanese: Findings from the National Health and Nutrition Survey, 2012. Public Health Nutr. 2019, 22, 2460–2468. [Google Scholar] [CrossRef]
- Yasumura, S.; Abe, M. Fukushima Health Management Survey and Related Issues. Asia Pac. J. Public Health 2017, 29, 29S–35S. [Google Scholar] [CrossRef]
- Nagai, M.; Ohira, T.; Takahashi, H.; Nakano, H.; Sakai, A.; Hashimoto, S.; Yasumura, S.; Abe, M. Impact of evacuation on trends in the prevalence, treatment, and control of hypertension before and after a disaster. J. Hypertens. 2018, 36, 924–932. [Google Scholar] [CrossRef]
- Ohira, T.; Nakano, H.; Nagai, M.; Yumiya, Y.; Zhang, W.; Uemura, M.; Sakai, A.; Hashimoto, S.; Fukushima Health Management Survey Group. Changes in Cardiovascular Risk Factors After the Great East Japan Earthquake. Asia Pac. J. Public Health 2017, 29, 47S–55S. [Google Scholar] [CrossRef]
- Takahashi, S.; Nakamura, M.; Yonekura, Y.; Tanno, K.; Sakata, K.; Ogawa, A.; Kobayashi, S. Association between relocation and changes in cardiometabolic risk factors: A longitudinal study in tsunami survivors of the 2011 Great East Japan Earthquake. BMJ Open 2016, 6, e011291. [Google Scholar] [CrossRef] [PubMed]
- Hirai, H.; Nagao, M.; Ohira, T.; Maeda, M.; Okazaki, K.; Nakano, H.; Hayashi, F.; Harigane, M.; Suzuki, Y.; Takahashi, A.; et al. Psychological burden predicts new-onset diabetes in men: A longitudinal observational study in the Fukushima Health Management Survey after the Great East Japan Earthquake. Front. Endocrinol. 2022, 13, 2840. [Google Scholar]
- Gohardehi, F.; Seyedin, H.; Moslehi, S. Prevalence rate of diabetes and hypertension in disaster-exposed populations: A systematic review and meta-analysis. Ethiop. J. Health Sci. 2020, 30, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Ma, E.; Ohira, T.; Sakai, A.; Yasumura, S.; Takahashi, A.; Kazama, J.; Shimabukuro, M.; Nakano, H.; Okazaki, K.; Maeda, M.; et al. Associations between dietary patterns and cardiometabolic risks in Japan: A cross-sectional study from the Fukushima Health Management Survey, 2011–2015. Nutrients 2020, 12, 129. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Ohira, T.; Abe, M.; Kamiya, K.; Yamashita, S.; Yasumura, S.; Ohtsuru, A.; Maeda, M.; Harigane, M.; Horikoshi, N.; et al. Evacuation after the Great East Japan Earthquake was associated with poor dietary intake: The Fukushima Health Management Survey. J. Epidemiol. 2017, 27, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Sauvaget, C.; Allen, N.; Hayashi, M.; Spencer, E.; Nagano, J. Validation of a food frequency questionnaire in the Hiroshima/Nagasaki Life Span Study. J. Epidemiol. 2002, 12, 394–401. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.L.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Uemura, M.; Ohira, T.; Yasumura, S.; Otsuru, A.; Maeda, M.; Harigane, M.; Horikoshi, N.; Suzuki, Y.; Yabe, H.; Takahashi, H.; et al. Association between psychological distress and dietary intake among evacuees after the Great East Japan Earthquake in a cross-sectional study: The Fukushima Health Management Survey. BMJ Open 2016, 6, e011534. [Google Scholar] [CrossRef]
- Luger, E.; Aspalter, R.; Luger, M.; Longin, R.; Rieder, A.; Dorner, T.E. Changes of dietary patterns during participation in a web-based weight-reduction programme. Public Health Nutr. 2016, 19, 1211–1221. [Google Scholar] [CrossRef]
- Lin, J.; Fung, T.T.; Hu, F.B.; Curhan, G.C. Association of dietary patterns with albuminuria and kidney function decline in older white women: A subgroup analysis from the Nurses’ Health Study. Am. J. Kidney Dis. 2011, 57, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Htun, N.C.; Suga, H.; Imai, S.; Shimizu, W.; Takimoto, H. Food intake patterns and cardiovascular risk factors in Japanese adults: Analyses from the 2012 National Health and nutrition survey, Japan. Nutr. J. 2017, 16, 61. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B.E.; Sasaki, S. Thirteen-Year Trends in Dietary Patterns among Japanese Adults in the National Health and Nutrition Survey 2003(-)2015: Continuous Westernization of the Japanese Diet. Nutrients 2018, 10, 994. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Montero, C.; Fraile-Martinez, O.; Gomez-Lahoz, A.M.; Pekarek, L.; Castellanos, A.J.; Noguerales-Fraguas, F.; Coca, S.; Guijarro, L.G.; Garcia-Honduvilla, N.; Asunsolo, A.; et al. Nutritional Components in Western Diet Versus Mediterranean Diet at the Gut Microbiota-Immune System Interplay. Implications for Health and Disease. Nutrients 2021, 13, 699. [Google Scholar] [CrossRef] [PubMed]
- Boushey, C.J.; Abed, B.; Corpuz, G.G.; Spoden, M. Dietary patterns: What’s in a name? Nutr. Today 2017, 52, 137–142. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef]
- Muraki, I.; Imamura, F.; Manson, J.E.; Hu, F.B.; Willett, W.C.; van Dam, R.M.; Sun, Q. Fruit consumption and risk of type 2 diabetes: Results from three prospective longitudinal cohort studies. BMJ 2013, 347, f5001. [Google Scholar] [CrossRef]
- Ito, T.; Kawakami, R.; Tanisawa, K.; Miyawaki, R.; Ishii, K.; Torii, S.; Suzuki, K.; Sakamoto, S.; Muraoka, I.; Oka, K.; et al. Dietary patterns and abdominal obesity in middle-aged and elderly Japanese adults: Waseda Alumni’s Sports, Exercise, Daily Activity, Sedentariness and Health Study (WASEDA’S Health Study). Nutrition 2019, 58, 149–155. [Google Scholar] [CrossRef]
- Shimabukuro, M. Cardiac adiposity and global cardiometabolic risk: New concept and clinical implication. Circ. J. 2009, 73, 27–34. [Google Scholar] [CrossRef]
- Tanabe, H.; Masuzaki, H.; Shimabukuro, M. Novel strategies for glycaemic control and preventing diabetic complications applying the clustering-based classification of adult-onset diabetes mellitus: A perspective. Diabetes Res. Clin. Pract. 2021, 180, 109067. [Google Scholar] [CrossRef]
- Bertoia, M.L.; Mukamal, K.J.; Cahill, L.E.; Hou, T.; Ludwig, D.S.; Mozaffarian, D.; Willett, W.C.; Hu, F.B.; Rimm, E.B. Changes in Intake of Fruits and Vegetables and Weight Change in United States Men and Women Followed for Up to 24 Years: Analysis from Three Prospective Cohort Studies. PLoS Med. 2015, 12, e1001878. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, R.E.; Elvestad, M.; Molin, M.; Aune, D. Fruit and vegetable consumption and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis of prospective studies. BMJ Nutr. Prev. Health 2021, 4, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Woo, H.D.; Cho, M.J.; Park, J.K.; Kim, S.S. Identification of Dietary Patterns Associated with Incidence of Hyperglycemia in Middle-Aged and Older Korean Adults. Nutrients 2019, 11, 1801. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Shi, Z. Dietary Pattern during 1991–2011 and Its Association with Cardio Metabolic Risks in Chinese Adults: The China Health and Nutrition Survey. Nutrients 2017, 9, 1218. [Google Scholar] [CrossRef]
- Hermansen, K.; Sondergaard, M.; Hoie, L.; Carstensen, M.; Brock, B. Beneficial effects of a soy-based dietary supplement on lipid levels and cardiovascular risk markers in type 2 diabetic subjects. Diabetes Care 2001, 24, 228–233. [Google Scholar] [CrossRef]
- Wakita Asano, A.; Hayashi, F.; Miyoshi, M.; Arai, Y.; Yoshita, K.; Yamamoto, S.; Yoshiike, N. Demographics, health-related behaviors, eating habits and knowledge associated with vegetable intake in Japanese adults. Eur. J. Clin. Nutr. 2009, 63, 1335–1344. [Google Scholar] [CrossRef]
- Northstone, K. Dietary patterns: The importance of sex differences. Br. J. Nutr. 2012, 108, 393–394. [Google Scholar] [CrossRef]
- Xu, S.H.; Qiao, N.; Huang, J.J.; Sun, C.M.; Cui, Y.; Tian, S.S.; Wang, C.; Liu, X.M.; Zhang, H.X.; Wang, H.; et al. Gender Differences in Dietary Patterns and Their Association with the Prevalence of Metabolic Syndrome among Chinese: A Cross-Sectional Study. Nutrients 2016, 8, 180. [Google Scholar] [CrossRef]
- Sharkey, T.; Whatnall, M.C.; Hutchesson, M.J.; Haslam, R.L.; Bezzina, A.; Collins, C.E.; Ashton, L.M. Effectiveness of gender-targeted versus gender-neutral interventions aimed at improving dietary intake, physical activity and/or overweight/obesity in young adults (aged 17–35 years): A systematic review and meta-analysis. Nutr. J. 2020, 19, 78. [Google Scholar] [CrossRef]
- Eshak, E.S.; Iso, H.; Mizoue, T.; Inoue, M.; Noda, M.; Tsugane, S. Soft drink, 100% fruit juice, and vegetable juice intakes and risk of diabetes mellitus. Clin. Nutr. 2013, 32, 300–308. [Google Scholar] [CrossRef]
- Ulven, S.M.; Holven, K.B.; Gil, A.; Rangel-Huerta, O.D. Milk and Dairy Product Consumption and Inflammatory Biomarkers: An Updated Systematic Review of Randomized Clinical Trials. Adv. Nutr. 2019, 10, S239–S250. [Google Scholar] [CrossRef] [PubMed]
- Savaiano, D.A.; Hutkins, R.W. Yogurt, cultured fermented milk, and health: A systematic review. Nutr. Rev. 2021, 79, 599–614. [Google Scholar] [CrossRef] [PubMed]
- Companys, J.; Pla-Paga, L.; Calderon-Perez, L.; Llaurado, E.; Sola, R.; Pedret, A.; Valls, R.M. Fermented Dairy Products, Probiotic Supplementation, and Cardiometabolic Diseases: A Systematic Review and Meta-analysis. Adv. Nutr. 2020, 11, 834–863. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Red meat consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1088–1096. [Google Scholar] [CrossRef]
- den Braver, N.R.; Lakerveld, J.; Rutters, F.; Schoonmade, L.J.; Brug, J.; Beulens, J.W.J. Built environmental characteristics and diabetes: A systematic review and meta-analysis. BMC Med. 2018, 16, 12. [Google Scholar] [CrossRef]
- Greenwood, D.C.; Threapleton, D.E.; Evans, C.E.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Burley, V.J. Association between sugar-sweetened and artificially sweetened soft drinks and type 2 diabetes: Systematic review and dose-response meta-analysis of prospective studies. Br. J. Nutr. 2014, 112, 725–734. [Google Scholar] [CrossRef]
- Guess, N.D. Dietary Interventions for the Prevention of Type 2 Diabetes in High-Risk Groups: Current State of Evidence and Future Research Needs. Nutrients 2018, 10, 1245. [Google Scholar] [CrossRef]
- Goto, A.; Goto, M.; Noda, M.; Tsugane, S. Incidence of type 2 diabetes in Japan: A systematic review and meta-analysis. PLoS ONE 2013, 8, e74699. [Google Scholar] [CrossRef]
- Iwasaki, Y.; Arisawa, K.; Katsuura-Kamano, S.; Uemura, H.; Tsukamoto, M.; Kadomatsu, Y.; Okada, R.; Hishida, A.; Tanaka, K.; Hara, M.; et al. Associations of Nutrient Patterns with the Prevalence of Metabolic Syndrome: Results from the Baseline Data of the Japan Multi-Institutional Collaborative Cohort Study. Nutrients 2019, 11, 990. [Google Scholar] [CrossRef]
- Tomata, Y.; Sugiyama, K.; Kaiho, Y.; Honkura, K.; Watanabe, T.; Zhang, S.; Sugawara, Y.; Tsuji, I. Dietary Patterns and Incident Dementia in Elderly Japanese: The Ohsaki Cohort 2006 Study. J. Gerontol. Ser. A 2016, 71, 1322–1328. [Google Scholar] [CrossRef]
- Fung, T.T.; Schulze, M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Dietary patterns, meat intake, and the risk of type 2 diabetes in women. Arch. Intern. Med. 2004, 164, 2235–2240. [Google Scholar] [CrossRef] [PubMed]
- Ahlqvist, E.; Storm, P.; Käräjämäki, A.; Martinell, M.; Dorkhan, M.; Carlsson, A.; Vikman, P.; Prasad, R.B.; Aly, D.M.; Almgren, P.; et al. Novel subgroups of adult-onset diabetes and their association with outcomes: A data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. 2018, 6, 361–369. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All (n = 22,740) | Men (n = 8465) | Women (n = 14,275) | p Value | |
|---|---|---|---|---|
| Age (years) | 55.9 (15.7) | 58.2 (15.4) | 54.6 (15.8) | <0.001 |
| Education ≥ vocational university | 25.8 | 22.6 | 27.7 | <0.001 |
| Current smoker | 16.4 | 29.4 | 8.7 | <0.001 |
| Current alcohol drinking | 45.0 | 69.8 | 30.3 | <0.001 |
| Physical activity ≥ 2 times/week | 34.6 | 39.0 | 32.0 | <0.001 |
| K6 ≥ 13 | 13.7 | 10.6 | 15.5 | <0.001 |
| Live at shelter/temporary house | 43.6 | 43.9 | 43.5 | 0.193 |
| BMI (kg/m2) | 23.4 (3.6) | 24.2 (3.3) | 22.9 (3.7) | <0.001 |
| BMI ≥ 25 kg/m2 | 29.8 | 37.6 | 25.1 | <0.001 |
| Hypertension | 39.8 | 49.3 | 34.1 | <0.001 |
| SBP (mmHg) | 127.0 (16.9) | 130.9 (15.8) | 124.7 (17.1) | <0.001 |
| DBP (mmHg) | 76.7 (10.9) | 79.8 (10.4) | 74.8 (10.7) | <0.001 |
| Fasting blood glucose (mg/dL) | 93 [88, 100] | 96 [90, 103] | 92 [87, 98] | <0.001 |
| LDL-C (mg/dL) | 124.3 (32.4) | 122.8 (32.0) | 125.1 (32.6) | <0.001 |
| LDL-C ≥ 140 mg/dL | 30.2 | 29.2 | 30.8 | 0.008 |
| HDL-C (mg/dL) | 61.3 (15.3) | 55.7 (14.4) | 64.6 (14.9) | <0.001 |
| HDL-C < 40 mg/dL | 5.6 | 10.3 | 2.8 | <0.001 |
| Triglycerides (mg/dL) | 91 [64, 130] | 105 [74, 151] | 83 [60, 118] | <0.001 |
| Triglycerides ≥ 150 mg/dL | 17.8 | 25.8 | 13.1 | <0.001 |
| Typical Japanese pattern score | −0.02 [−0.71, 0.71] | −0.02 [−0.69, 0.70] | −0.02 [−0.71, 0.71] | 0.817 |
| Juice pattern score | −0.18 [−0.69, 0.46] | −0.17 [−0.69, 0.45] | −0.19 [−0.69, 0.46] | 0.657 |
| Meat pattern score | −0.21 [−0.67, 0.50] | −0.23 [−0.66, 0.46] | −0.20 [−0.68, 0.53] | 0.383 |
| 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Total | Person -Year | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | New onset T2DM | 142 | (19.4) | 136 | (18.6) | 92 | (12.6) | 114 | (15.6) | 104 | (14.2) | 83 | (11.4) | 60 | (8.2) | 731 | 40,688 |
| Fasting blood glucose, ≥126 mg/dL | 84 | (19.2) | 66 | (15.1) | 51 | (11.7) | 60 | (13.7) | 65 | (14.9) | 52 | (11.9) | 59 | (13.5) | 437 | 41,450 | |
| HbA1c, >6.5% | 64 | (16.0) | 81 | (20.3) | 42 | (10.5) | 59 | (14.8) | 50 | (12.5) | 56 | (14.0) | 48 | (12) | 400 | 41,558 | |
| Women | New onset T2DM | 113 | (15.8) | 132 | (18.4) | 87 | (12.1) | 114 | (15.9) | 106 | (14.8) | 99 | (13.8) | 66 | (9.2) | 717 | 73,082 |
| Fasting blood glucose, ≥126 mg/dL | 59 | (15.6) | 57 | (15.1) | 55 | (14.6) | 52 | (13.8) | 56 | (14.9) | 47 | (12.5) | 51 | (13.5) | 377 | 73,946 | |
| HbA1c, >6.5% | 52 | (12.1) | 86 | (20.0) | 47 | (11.0) | 61 | (14.2) | 63 | (14.7) | 66 | (15.4) | 54 | (12.6) | 429 | 73,854 | |
| Dietary Pattern Scores | All (n = 22,740) | Men (n = 8465) | Women (n = 14,275) | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | HR | 95% CI | HR | 95% CI | ||
| Typical Japanese | |||||||
| Model 1 a | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 0.79 | (0.68, 0.92) | 0.78 | (0.63, 0.97) | 0.80 | (0.64, 1.00) | |
| Q3 | 0.79 | (0.68, 0.92) | 0.73 | (0.58, 0.90) | 0.86 | (0.70, 1.07) | |
| Q4 | 0.71 | (0.60, 0.83) | 0.78 | (0.63, 0.97) | 0.64 | (0.51, 0.80) | |
| P for trend | <0.001 | 0.048 | <0.001 | ||||
| Model 2 b | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 0.81 | (0.69, 0.94) | 0.79 | (0.64, 0.98) | 0.82 | (0.66, 1.03) | |
| Q3 | 0.80 | (0.69, 0.93) | 0.72 | (0.58, 0.90) | 0.89 | (0.72, 1.10) | |
| Q4 | 0.74 | (0.63, 0.86) | 0.78 | (0.63, 0.97) | 0.70 | (0.56, 0.88) | |
| P for trend | 0.011 | 0.042 | 0.005 | ||||
| Model 3 c | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 0.82 | (0.70, 0.96) | 0.81 | (0.65, 1.01) | 0.84 | (0.67, 1.05) | |
| Q3 | 0.83 | (0.71, 0.97) | 0.74 | (0.60, 0.92) | 0.93 | (0.75, 1.15) | |
| Q4 | 0.80 | (0.68, 0.94) | 0.85 | (0.68, 1.06) | 0.76 | (0.60, 0.95) | |
| P for trend | 0.015 | 0.181 | 0.04 | ||||
| Juice | |||||||
| Model 1 a | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.01 | (0.88, 1.17) | 1.03 | (0.84, 1.27) | 1.00 | (0.82, 1.23) | |
| Q3 | 0.90 | (0.78, 1.05) | 0.97 | (0.79, 1.20) | 0.85 | (0.68, 1.05) | |
| Q4 | 0.96 | (0.83, 1.11) | 0.97 | (0.79, 1.20) | 0.96 | (0.78, 1.18) | |
| P for trend | 0.427 | 0.690 | 0.563 | ||||
| Model 2 b | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.00 | (0.86, 1.16) | 1.01 | (0.82, 1.24) | 1.00 | (0.82, 1.23) | |
| Q3 | 0.89 | (0.76, 1.03) | 0.95 | (0.77, 1.16) | 0.84 | (0.68, 1.04) | |
| Q4 | 0.95 | (0.83, 1.11) | 0.94 | (0.77, 1.16) | 0.99 | (0.80, 1.21) | |
| P for trend | 0385 | 0.503 | 0.728 | ||||
| Model 3 c | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.01 | (0.87, 1.17) | 1.02 | (0.83, 1.26) | 0.99 | (0.81, 1.22) | |
| Q3 | 0.90 | (0.78, 1.05) | 0.97 | (0.79, 1.20) | 0.83 | (0.67, 1.03) | |
| Q4 | 0.99 | (0.86, 1.15) | 0.99 | (0.80, 1.23) | 1.01 | (0.82, 1.24) | |
| P for trend | 0.773 | 0.832 | 0.912 | ||||
| Meat | |||||||
| Model 1 a | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.14 | (0.99, 1.30) | 1.13 | (0.94, 1.37) | 1.15 | (0.95, 1.39) | |
| Q3 | 0.89 | (0.76, 1.03) | 0.89 | (0.72, 1.10) | 0.89 | (0.73, 1.10) | |
| Q4 | 1.01 | (0.87, 1.17) | 1.04 | (0.84, 1.29) | 0.97 | (0.79, 1.20) | |
| P for trend | 0.455 | 0.846 | 0.415 | ||||
| Model 2 b | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.13 | (0.99, 1.29) | 1.12 | (0.92, 1.35) | 1.15 | (0.95, 1.39) | |
| Q3 | 0.90 | (0.78, 1.05) | 0.91 | (0.74, 1.13) | 0.89 | (0.73, 1.10) | |
| Q4 | 1.03 | (0.88, 1.19) | 1.07 | (0.87, 1.33) | 0.98 | (0.80, 1.21) | |
| P for trend | 0.694 | 0.898 | 0.465 | ||||
| Model 3 c | Q1 (lowest) | Ref. | - | Ref. | - | Ref. | - |
| Q2 | 1.13 | (0.99, 1.29) | 1.11 | (0.91, 1.34) | 1.17 | (0.96, 1.41) | |
| Q3 | 0.91 | (0.78, 1.06) | 0.90 | (0.72, 1.11) | 0.92 | (0.74, 1.13) | |
| Q4 | 1.05 | (0.90, 1.22) | 1.06 | (0.86, 1.32) | 1.03 | (0.83, 1.27) | |
| P for trend | 0.883 | 0.959 | 0.747 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, E.; Ohira, T.; Hirai, H.; Okazaki, K.; Nagao, M.; Hayashi, F.; Nakano, H.; Suzuki, Y.; Sakai, A.; Takahashi, A.; et al. Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey. Nutrients 2022, 14, 4872. https://doi.org/10.3390/nu14224872
Ma E, Ohira T, Hirai H, Okazaki K, Nagao M, Hayashi F, Nakano H, Suzuki Y, Sakai A, Takahashi A, et al. Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey. Nutrients. 2022; 14(22):4872. https://doi.org/10.3390/nu14224872
Chicago/Turabian StyleMa, Enbo, Tetsuya Ohira, Hiroyuki Hirai, Kanako Okazaki, Masanori Nagao, Fumikazu Hayashi, Hironori Nakano, Yuriko Suzuki, Akira Sakai, Atsushi Takahashi, and et al. 2022. "Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey" Nutrients 14, no. 22: 4872. https://doi.org/10.3390/nu14224872
APA StyleMa, E., Ohira, T., Hirai, H., Okazaki, K., Nagao, M., Hayashi, F., Nakano, H., Suzuki, Y., Sakai, A., Takahashi, A., Kazama, J. J., Yabe, H., Maeda, M., Yasumura, S., Ohto, H., Kamiya, K., & Shimabukuro, M. (2022). Dietary Patterns and New-Onset Type 2 Diabetes Mellitus in Evacuees after the Great East Japan Earthquake: A 7-Year Longitudinal Analysis in the Fukushima Health Management Survey. Nutrients, 14(22), 4872. https://doi.org/10.3390/nu14224872