
Temporal Trends in Incidence of Nutritional Deficiency among Older Adults in China: A Secondary Analysis of the Global Burden of Disease Study 1990–2019
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Definitions
2.2. Statistical Analysis
3. Results
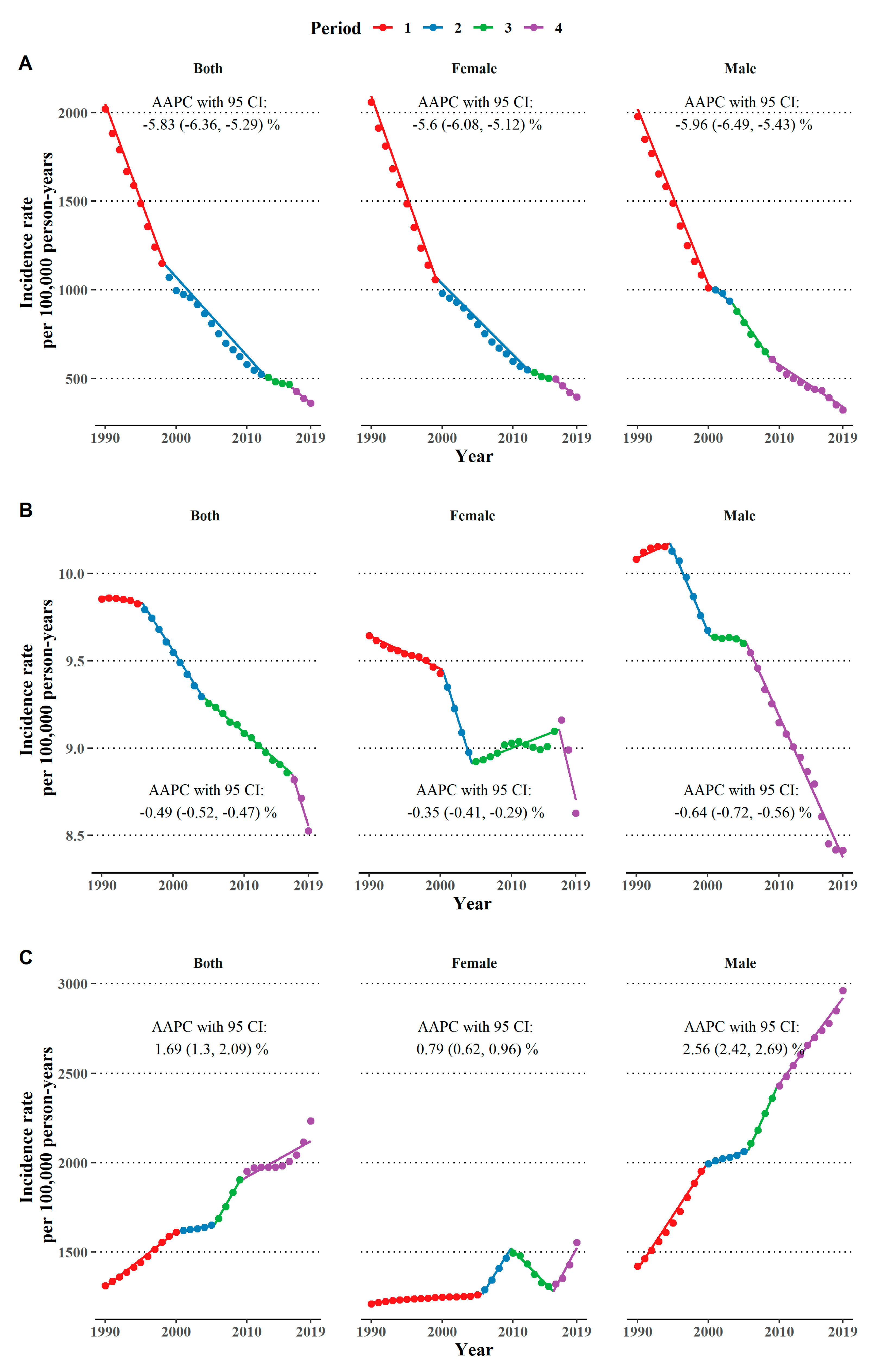
3.1. Temporal Trends in Nutritional Deficiencies
3.2. The Effect of Age, Period, and Cohort
4. Discussion
4.1. Trends in Vitamin A Deficiency
4.2. Trends in Iodine Deficiency
4.3. Trends in Protein-Energy Malnutrition
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- National Bureau of Statistics of China. Main Data of the Seventh National Population Census. Available online: http://www.stats.gov.cn/english/PressRelease/202105/t20210510_1817185.html (accessed on 1 September 2022).
- World Health Organization. Ageing and Health in China. Available online: https://www.who.int/china/health-topics/ageing (accessed on 1 September 2022).
- The Lancet. Ageing in China: A ticking bomb. Lancet 2016, 388, 2058. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.B.; Rosenberg, I. Nutrition and aging: Changes in the regulation of energy metabolism with aging. Physiol. Rev. 2006, 86, 651–667. [Google Scholar] [CrossRef]
- Cox, N.J.; Morrison, L.; Ibrahim, K.; Robinson, S.M.; Sayer, A.A.; Roberts, H.C. New horizons in appetite and the anorexia of ageing. Age Ageing 2020, 49, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Longo, V.D.; Anderson, R.M. Nutrition, longevity and disease: From molecular mechanisms to interventions. Cell 2022, 185, 1455–1470. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Ding, S.; Lu, J.; Li, Y. Global, regional, and national burdens of common micronutrient deficiencies from 1990 to 2019: A secondary trend analysis based on the Global Burden of Disease 2019 study. EClinicalMedicine 2022, 44, 101299. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, L.; Pu, Y.; Sun, M.; Zhao, Y.; Zhang, D.; Wang, X.; Li, Y.; Guo, D.; He, S. Global, Regional, and National Burden of Protein-Energy Malnutrition: A Systematic Analysis for the Global Burden of Disease Study. Nutrients 2022, 14, 2592. [Google Scholar] [CrossRef]
- The Lancet Regional Health—Western Pacific. What to eat for a healthier China? Lancet Reg. Health—West. Pac. 2022, 23, 100525. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.Q.; Yu, J.M.; Li, W.; Fu, Z.M.; Lin, Y.; Shi, Y.Y.; Hu, W.; Ba, Y.; Li, S.Y.; Li, Z.N.; et al. Survey and analysis of the nutritional status in hospitalized patients with malignant gastric tumors and its influence on the quality of life. Support Care Cancer 2020, 28, 373–380. [Google Scholar] [CrossRef] [Green Version]
- Lai, X.; Zhu, H.; Du, H.; Huo, X.; Yu, K. Nutritional status of Chinese oldest-old adults (≥80 years of age): A cross-sectional study in Beijing. Eur. J. Clin. Nutr. 2021, 75, 1040–1046. [Google Scholar] [CrossRef]
- Leung, D.Y.P.; Cheng, H.L.; Tyrovolas, S.; Tang, A.S.K.; Liu, J.Y.W.; Tse, M.M.Y.; Lai, C.K.Y.; Molassiotis, A. Magnitude, Temporal Trends, and Inequalities in the DALYs and YLDs of Nutritional Deficiency among Older Adults in the Western Pacific Region: Findings from the Global Burden of Disease Study 1990–2019. Nutrients 2021, 13, 4421. [Google Scholar] [CrossRef]
- Chen, H.; Lu, J.; Li, Y. Secular Trends in the Prevalence of and Disability-Adjusted Life Years Due to Common Micronutrient Deficiencies in China from 1990 to 2019: An Age-Period-Cohort Study and Joinpoint Analysis. Front. Nutr. 2022, 9, 754351. [Google Scholar] [CrossRef]
- Murray, C.J.; Lopez, A.D.; World Health Organization. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020: Summary; World Health Organization: Geneva, Switzerland, 1996.
- Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [CrossRef]
- Murray, C.J.; Ezzati, M.; Flaxman, A.D.; Lim, S.; Lozano, R.; Michaud, C.; Naghavi, M.; Salomon, J.A.; Shibuya, K.; Vos, T.; et al. GBD 2010: Design, definitions, and metrics. Lancet 2012, 380, 2063–2066. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Available online: https://www.cdc.gov/nchs/icd/icd9cm.htm (accessed on 10 November 2022).
- The 2019 Global Burden of Disease (GBD) Study. GBD Results. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 20 August 2022).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Yue, T.; Zhang, Q.; Li, G.; Qin, H. Global Burden of Nutritional Deficiencies among Children under 5 Years of Age from 2010 to 2019. Nutrients 2022, 14, 2685. [Google Scholar] [CrossRef] [PubMed]
- Commission, N.H. China Health Statistics Yearbook (2018); Peking Union Medical College Press: Beijing, China, 2018. [Google Scholar]
- Ministry of Education of the People’s Republic of China. Major Educational Achievements in China in 2020. Available online: http://en.moe.gov.cn/features/2021TwoSessions/Reports/202103/t20210323_522026.html (accessed on 9 October 2022).
- Zhang, J.; Wang, Z.; Du, W.; Huang, F.; Jiang, H.; Bai, J.; Zhang, X.; Zhang, B.; Wang, H. Twenty-Five-Year Trends in Dietary Patterns among Chinese Adults from 1991 to 2015. Nutrients 2021, 13, 1327. [Google Scholar] [CrossRef]
- Du, W.; Wang, H.; Wang, Z.; Zhang, J.; Su, C.; Jia, X.; Zhang, J.; Jiang, H.; Huang, F.; Ouyang, Y.; et al. Dietary vitamin a intake among Chinese adults: Findings from CNTCS2015. Nutr. J. 2018, 17, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Global Database on National Nutrition Policies and Programmes. Policy—National Plan of Action for Nutrition for China. Available online: https://extranet.who.int/nutrition/gina/en/node/8767 (accessed on 10 October 2022).
- Sun, D.; Codling, K.; Chang, S.; Zhang, S.; Shen, H.; Su, X.; Chen, Z.; Scherpbier, R.W.; Yan, J. Eliminating Iodine Deficiency in China: Achievements, Challenges and Global Implications. Nutrients 2017, 9, 361. [Google Scholar] [CrossRef]
- Sun, D.; Xiao, D.; Liu, S. The Monitoring of Iodine Deficiency Disorders of China in 2011; People’s Medical Publishing House: Beijing, China, 2011. [Google Scholar]
- Lin, Y.; Chen, D.; Wu, J.; Chen, Z. Iodine status five years after the adjustment of universal salt iodization: A cross-sectional study in Fujian Province, China. Nutr. J. 2021, 20, 17. [Google Scholar] [CrossRef] [PubMed]
- Du, S.; Batis, C.; Wang, H.; Zhang, B.; Zhang, J.; Popkin, B.M. Understanding the patterns and trends of sodium intake, potassium intake, and sodium to potassium ratio and their effect on hypertension in China. Am. J. Clin. Nutr. 2014, 99, 334–343. [Google Scholar] [CrossRef]
- Mathewson, S.L.; Azevedo, P.S.; Gordon, A.L.; Phillips, B.E.; Greig, C.A. Overcoming protein-energy malnutrition in older adults in the residential care setting: A narrative review of causes and interventions. Aging Res. Rev. 2021, 70, 101401. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, Y.; Tan, T.; Song, X.; Huang, F.; Zhang, B.; Ding, G.; Wang, H. Dietary protein intake dynamics in elderly Chinese from 1991 to 2018. Nutrients 2021, 13, 3806. [Google Scholar] [CrossRef]
- Chen, H.; Qian, Y.; Dong, Y.; Yang, Z.; Guo, L.; Liu, J.; Shen, Q.; Wang, L. Patterns and changes in life expectancy in China, 1990–2016. PLoS ONE 2020, 15, e0231007. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Zhao, L.; Zhang, J.; Yang, Z.; Yang, L.; Huang, J.; Fang, H.; Guo, Q.; Xu, X.; Ju, L. China Nutrition and Health Surveys (1982−2017). China CDC Wkly. 2021, 3, 193. [Google Scholar] [CrossRef]
- Shahar, D.; Shai, I.; Vardi, H.; Fraser, D. Dietary intake and eating patterns of elderly people in Israel: Who is at nutritional risk? Eur. J. Clin. Nutr. 2003, 57, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Bunn, D.; Hooper, L.; Welch, A. Dehydration and malnutrition in residential care: Recommendations for strategies for improving practice derived from a scoping review of existing policies and guidelines. Geriatrics 2018, 3, 77. [Google Scholar] [CrossRef] [Green Version]
- Fávaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.E.; Duyck, J. Risk Factors for Malnutrition in Older Adults: A Systematic Review of the Literature Based on Longitudinal Data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.; Lee, Y.W. Nutrition knowledge, attitudes and dietary restriction behaviour of Taiwanese elderly. Asia Pac. J. Clin. Nutr. 2005, 14, 221–229. [Google Scholar] [PubMed]
- The State Council Information Office of the People’s Republic of China. Press Conference-Report on Chinese Residents’ Chronic Diseases and Nutrition 2020. Available online: http://www.scio.gov.cn/xwfbh/xwbfbh/wqfbh/42311/44583/wz44585/Document/1695276/1695276.htm (accessed on 18 November 2022).
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Both Sexes Combined | Male | Female | ||
|---|---|---|---|---|
| Vitamin A deficiency | Age effect: Age-specific incidence rate per 100,000 person-years (95% CI) | |||
| 65–69 | 8349.81 (8256.74, 8443.93) | 8632.09 (8473.00, 8794.17) | 8148.16 (8034.02, 8263.93) | |
| 70–74 | 5007.98 (4953.66, 5062.89) | 5143.90 (5051.42, 5238.08) | 5005.56 (4937.32, 5074.73) | |
| 75–79 | 3244.68 (3211.96, 3277.74) | 3164.02 (3111.58, 3217.35) | 3330.35 (3288.16, 3373.09) | |
| 80–84 | 2213.25 (2193.00, 2233.70) | 1961.68 (1931.61, 1992.22) | 2336.82 (2310.09, 2363.85) | |
| 85–89 | 1522.70 (1509.39, 1536.13) | 1216.24 (1198.29, 1234.45) | 1654.28 (1636.34, 1672.41) | |
| Period effect: RR (95% CI) | ||||
| 1994 | 1.06 (1.05, 1.06) | 1.01 (1.00, 1.01) | 1.09 (1.09, 1.09) | |
| 1999 | 0.94 (0.94, 0.94) | 0.95 (0.95, 0.95) | 0.93 (0.93, 0.93) | |
| 2004 | 1.02 (1.02, 1.02) | 1.05 (1.05, 1.06) | 0.99 (0.99, 1.00) | |
| 2009 | 0.99 (0.99, 1.00) | 1.01 (1.01, 1.01) | 0.99 (0.98, 0.99) | |
| 2014 | 0.98 (0.98, 0.98) | 0.98 (0.98, 0.98) | 0.99 (0.99, 0.99) | |
| 2019 | 1.02 (1.01, 1.02) | 1.00 (1.00, 1.00) | 1.02 (1.02, 1.02) | |
| Cohort effect: RR (95% CI) | ||||
| 1905–1909 | 0.64 (0.64, 0.64) | 0.64 (0.63, 0.64) | 0.64 (0.64, 0.65) | |
| 1910–1914 | 0.47 (0.46, 0.47) | 0.46 (0.46, 0.47) | 0.47 (0.47, 0.47) | |
| 1915–1919 | 0.34 (0.34, 0.34) | 0.33 (0.33, 0.34) | 0.34 (0.34, 0.35) | |
| 1920–1924 | 0.25 (0.24, 0.25) | 0.24 (0.24, 0.25) | 0.25 (0.25, 0.25) | |
| 1925–1929 | 0.18 (0.18, 0.18) | 0.18 (0.17, 0.18) | 0.18 (0.18, 0.19) | |
| 1930–1934 | 0.14 (0.13, 0.14) | 0.13 (0.13, 0.13) | 0.14 (0.14, 0.14) | |
| 1935–1939 | 0.10 (0.10, 0.10) | 0.09 (0.09, 0.10) | 0.11 (0.11, 0.11) | |
| 1940–1944 | 0.08 (0.08, 0.08) | 0.07 (0.07, 0.07) | 0.08 (0.08, 0.08) | |
| 1945–1949 | 0.06 (0.06, 0.06) | 0.05 (0.05, 0.05) | 0.06 (0.06, 0.07) | |
| 1950–1954 | 0.04 (0.04, 0.04) | 0.04 (0.04, 0.04) | 0.05 (0.05, 0.05) | |
| Iodine deficiency | Age effect: Age-specific incidence rate per 100,000 person-years (95% CI) | |||
| 65–69 | 11.40 (10.34, 12.56) | 11.75 (10.10, 13.67) | 10.91 (9.49, 12.55) | |
| 70–74 | 8.04 (7.30, 8.85) | 8.31 (7.15, 9.64) | 7.60 (6.62, 8.72) | |
| 75–79 | 6.35 (5.80, 6.96) | 6.45 (5.60, 7.44) | 5.98 (5.23, 6.82) | |
| 80–84 | 5.17 (4.74, 5.64) | 5.13 (4.47, 5.89) | 5.10 (4.50, 5.78) | |
| 85–89 | 4.20 (3.85, 4.59) | 4.08 (3.55, 4.69) | 4.41 (3.89, 5.00) | |
| Period effect: RR (95% CI) | ||||
| 1994 | 0.99 (0.97, 1.02) | 0.99 (0.96, 1.03) | 1.00 (0.97, 1.03) | |
| 1999 | 1.00 (0.99, 1.01) | 1.00 (0.98, 1.02) | 1.00 (0.99, 1.02) | |
| 2004 | 1.01 (0.99, 1.02) | 1.01 (0.98, 1.03) | 1.01 (0.98, 1.03) | |
| 2009 | 1.01 (0.98, 1.03) | 1.01 (0.98, 1.04) | 1.00 (0.97, 1.03) | |
| 2014 | 0.99 (0.97, 1.01) | 0.99 (0.96, 1.01) | 0.99 (0.97, 1.02) | |
| 2019 | 1.00 (0.99, 1.02) | 1.00 (0.98, 1.02) | 1.01 (0.99, 1.02) | |
| Cohort effect: RR (95% CI) | ||||
| 1905–1909 | 0.98 (0.96, 1.01) | 0.97 (0.94, 1.01) | 0.99 (0.96, 1.03) | |
| 1910–1914 | 0.97 (0.93, 1.01) | 0.96 (0.90, 1.02) | 0.99 (0.93, 1.05) | |
| 1915–1919 | 0.95 (0.90, 1.01) | 0.94 (0.86, 1.03) | 0.98 (0.90, 1.08) | |
| 1920–1924 | 0.94 (0.87, 1.02) | 0.92 (0.82, 1.04) | 0.98 (0.87, 1.10) | |
| 1925–1929 | 0.93 (0.85, 1.02) | 0.91 (0.78, 1.05) | 0.97 (0.84, 1.12) | |
| 1930–1934 | 0.91 (0.82, 1.01) | 0.89 (0.76, 1.05) | 0.95 (0.82, 1.10) | |
| 1935–1939 | 0.88 (0.80, 0.98) | 0.87 (0.74, 1.01) | 0.93 (0.81, 1.06) | |
| 1940–1944 | 0.88 (0.80, 0.97) | 0.85 (0.73, 0.99) | 0.94 (0.82, 1.08) | |
| 1945–1949 | 0.86 (0.78, 0.95) | 0.81 (0.70, 0.95) | 0.92 (0.80, 1.06) | |
| 1950–1954 | 0.81 (0.74, 0.90) | 0.77 (0.66, 0.90) | 0.87 (0.76, 1.00) | |
| Protein-energy malnutrition | Age effect: Age-specific incidence rate per 100,000 person-years (95% CI) | |||
| 65–69 | 865.03 (859.87, 870.22) | 819.75 (813.69, 825.85) | 932.61 (924.60, 940.68) | |
| 70–74 | 977.33 (971.54, 983.16) | 959.37 (952.33, 966.46) | 1011.25 (1002.63, 1019.93) | |
| 75–79 | 1103.14 (1096.77, 1109.55) | 1127.64 (1119.54, 1135.80) | 1097.40 (1088.35, 1106.53) | |
| 80–84 | 1212.03 (1205.32, 1218.77) | 1324.00 (1314.84, 1333.23) | 1186.71 (1177.43, 1196.07) | |
| 85–89 | 1322.22 (1314.76, 1329.71) | 1553.67 (1542.48, 1564.93) | 1282.03 (1271.89, 1292.25) | |
| Period effect: RR (95% CI) | ||||
| 1994 | 1.01 (1.01, 1.01) | 1.01 (1.01, 1.01) | 1.05 (1.04, 1.05) | |
| 1999 | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 0.98 (0.98, 0.98) | |
| 2004 | 0.99 (0.99, 0.99) | 0.99 (0.99, 0.99) | 0.96 (0.96, 0.96) | |
| 2009 | 0.99 (0.99, 0.99) | 0.99 (0.99, 1.00) | 1.06 (1.06, 1.06) | |
| 2014 | 1.00 (1.00, 1.00) | 1.01 (1.01, 1.01) | 0.93 (0.93, 0.93) | |
| 2019 | 1.01 (1.01, 1.01) | 1.00 (1.00, 1.00) | 1.03 (1.03, 1.04) | |
| Cohort effect: RR (95% CI) | ||||
| 1905–1909 | 1.13 (1.13, 1.13) | 1.20 (1.20, 1.20) | 1.06 (1.06, 1.06) | |
| 1910–1914 | 1.24 (1.24, 1.24) | 1.36 (1.36, 1.37) | 1.11 (1.10, 1.11) | |
| 1915–1919 | 1.35 (1.35, 1.36) | 1.55 (1.54, 1.56) | 1.15 (1.15, 1.16) | |
| 1920–1924 | 1.48 (1.47, 1.49) | 1.76 (1.75, 1.77) | 1.20 (1.19, 1.21) | |
| 1925–1929 | 1.62 (1.61, 1.63) | 2.00 (1.99, 2.02) | 1.26 (1.24, 1.27) | |
| 1930–1934 | 1.78 (1.77, 1.79) | 2.27 (2.25, 2.29) | 1.32 (1.31, 1.33) | |
| 1935–1939 | 1.97 (1.96, 1.98) | 2.53 (2.51, 2.55) | 1.39 (1.38, 1.40) | |
| 1940–1944 | 2.13 (2.11, 2.14) | 2.82 (2.80, 2.84) | 1.45 (1.43, 1.46) | |
| 1945–1949 | 2.30 (2.29, 2.32) | 3.15 (3.13, 3.17) | 1.51 (1.49, 1.52) | |
| 1950–1954 | 2.51 (2.49, 2.52) | 3.53 (3.50, 3.56) | 1.57 (1.56, 1.59) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, L.; Fu, J.; Lin, L.; Han, Y. Temporal Trends in Incidence of Nutritional Deficiency among Older Adults in China: A Secondary Analysis of the Global Burden of Disease Study 1990–2019. Nutrients 2022, 14, 5008. https://doi.org/10.3390/nu14235008
Xiao L, Fu J, Lin L, Han Y. Temporal Trends in Incidence of Nutritional Deficiency among Older Adults in China: A Secondary Analysis of the Global Burden of Disease Study 1990–2019. Nutrients. 2022; 14(23):5008. https://doi.org/10.3390/nu14235008
Chicago/Turabian StyleXiao, Linqi, Jialin Fu, Likai Lin, and Yong Han. 2022. "Temporal Trends in Incidence of Nutritional Deficiency among Older Adults in China: A Secondary Analysis of the Global Burden of Disease Study 1990–2019" Nutrients 14, no. 23: 5008. https://doi.org/10.3390/nu14235008
APA StyleXiao, L., Fu, J., Lin, L., & Han, Y. (2022). Temporal Trends in Incidence of Nutritional Deficiency among Older Adults in China: A Secondary Analysis of the Global Burden of Disease Study 1990–2019. Nutrients, 14(23), 5008. https://doi.org/10.3390/nu14235008