
Longitudinal Trajectories of Alcohol Consumption with All-Cause Mortality, Hypertension, and Blood Pressure Change: Results from CHNS Cohort, 1993–2015

Abstract
:
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Alcohol-Consumption Measurement
2.3. Outcome Identification
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
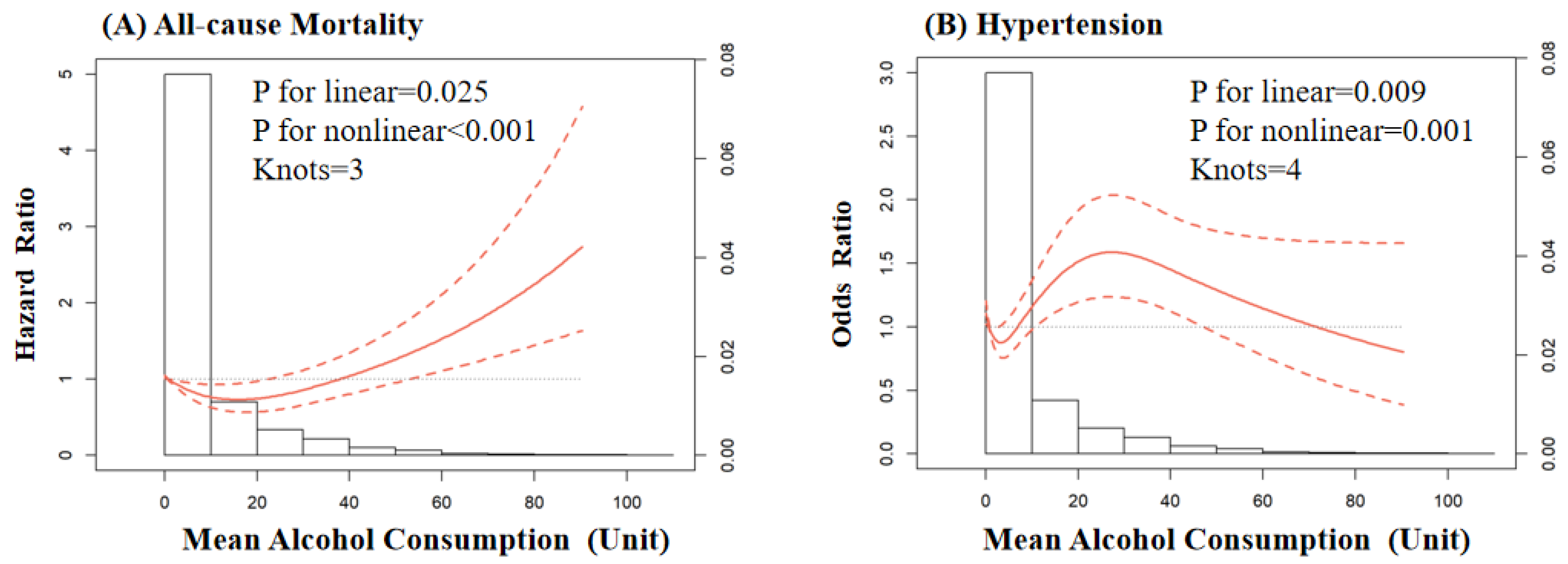
3.2. Alcohol Consumption and All-Cause Mortality
3.3. Alcohol Consumption and Newly Onset Hypertension
3.4. Alcohol Consumption and Change in Blood Pressure
4. Discussion
5. Conclusions
6. Novelty and Relevance
6.1. What Is New?
6.2. What Is Relevant?
7. Clinical/Pathophysiological Implications?
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rehm, J.; Gmel, G.; Gmel, G.; Hasan, O.; Imtiaz, S.; Popova, S.; Probst, C.; Roerecke, M.; Room, R.; Samokhvalov, A.; et al. The relationship between different dimensions of alcohol use and the burden of disease-an update. Addiction 2017, 112, 968–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2020 Alcohol Collaborators. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: A systematic analysis for the global burden of disease study. Lancet 2022, 400, 185–235. [Google Scholar] [CrossRef] [PubMed]
- Smyth, A.; Teo, K.K.; Rangarajan, S.; O’Donnell, M.; Zhang, X.; Rana, P.; Leong, D.P.; Dagenais, G.; Seron, P.; Rosengren, A.; et al. Alcohol consumption and cardiovascular disease, cancer, injury, admission to hospital, and mortality: A prospective cohort study. Lancet 2015, 386, 1945–1954. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- World Health Orgnization. Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Whelton, P.; Carey, R.; Aronow, W.; Casey, D.; Collins, K.; Dennison Himmelfarb, C.; DePalma, S.; Gidding, S.; Jamerson, K.; Jones, D.; et al. 2017 acc/aha/aapa/abc/acpm/ags/apha/ash/aspc/nma/pcna guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the global burden of disease study. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okubo, Y.; Sairenchi, T.; Irie, F.; Yamagishi, K.; Iso, H.; Watanabe, H.; Muto, T.; Tanaka, K.; Ota, H. Association of alcohol consumption with incident hypertension among middle-aged and older japanese population: The ibarakai prefectural health study (iphs). Hypertension 2014, 63, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Stewart, D.; Han, L.; Doran, T.; McCambridge, J. Alcohol consumption and all-cause mortality: An analysis of general practice database records for patients with long-term conditions. J. Epidemiol. Community Health 2017, 71, 729–735. [Google Scholar] [CrossRef]
- O’Neill, D.; Britton, A.; Hannah, M.; Goldberg, M.; Kuh, D.; Khaw, K.; Bell, S. Association of longitudinal alcohol consumption trajectories with coronary heart disease: A meta-analysis of six cohort studies using individual participant data. BMC Med. 2018, 16, 124. [Google Scholar] [CrossRef]
- Popkin, B.; Du, S.; Zhai, F.; Zhang, B. Cohort profile: The china health and nutrition survey--monitoring and understanding socio-economic and health change in china, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Zhai, F.; Du, S.; Popkin, B. The china health and nutrition survey, 1989–2011. In Obesity Reviews: An Official Journal of the International Association for the Study of Obesity; Wiley Online Library: New York, NY, USA, 2014; pp. 2–7. [Google Scholar]
- Liu, M.; Zhou, C.; Zhang, Z.; Li, Q.; He, P.; Zhang, Y.; Li, H.; Liu, C.; Qin, X. Inverse association between riboflavin intake and new-onset hypertension: A nationwide cohort study in china. Hypertension 2020, 76, 1709–1716. [Google Scholar] [CrossRef]
- Chinese Center for Disease Control and Prevention. Surveillance Report on Chronic Diseases and Its Risk Factors in China; Military Medical Science Press: Beijing, China, 2010. [Google Scholar]
- Britton, A.; O’Neill, D.; Bell, S. Underestimating the alcohol content of a glass of wine: The implications for estimates of mortality risk. Alcohol Alcohol. 2016, 51, 609–614. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.L.; Nagin, D.S. A note on a stata plugin for estimating group-based trajectory models. Sociol. Methods Res. 2013, 42, 608–613. [Google Scholar] [CrossRef]
- Nagin, D.S. Group-Based Modeling of Development; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Nagin, D.; Odgers, C. Group-based trajectory modeling in clinical research. Annu. Rev. Clin. Psychol. 2010, 6, 109–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croxford, R. Restricted Cubic Spline Regression: A Brief Introduction; Institute for Clinical Evaluative Sciences: Toronto, ON, Canada, 2016; pp. 1–5. [Google Scholar]
- Xi, B.; Veeranki, S.; Zhao, M.; Ma, C.; Yan, Y.; Mi, J. Relationship of alcohol consumption to all-cause, cardiovascular, and cancer-related mortality in u.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.; Kaptoge, S.; Butterworth, A.; Willeit, P.; Warnakula, S.; Bolton, T.; Paige, E.; Paul, D.; Sweeting, M.; Burgess, S.; et al. Risk thresholds for alcohol consumption: Combined analysis of individual-participant data for 599,912 current drinkers in 83 prospective studies. Lancet 2018, 391, 1513–1523. [Google Scholar] [CrossRef] [Green Version]
- Pai, J.; Mukamal, K.; Rimm, E. Long-term alcohol consumption in relation to all-cause and cardiovascular mortality among survivors of myocardial infarction: The health professionals follow-up study. Eur. Heart J. 2012, 33, 1598–1605. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.; Lee, S.-R.; Choi, E.-k.; Park, S.-H.; Lee, H.; Choi, J.; Han, M.; Lee, S.-w.; Han, K.-D.; Kim, S.; et al. Abstract 13797: Does alcohol consumption have a cumulative effect on the risk of stroke in young adults? Circulation 2021, 144, A13797. [Google Scholar]
- Stockwell, T.; Zhao, J.; Panwar, S.; Roemer, A.; Naimi, T.; Chikritzhs, T. Do “moderate” drinkers have reduced mortality risk? A systematic review and meta-analysis of alcohol consumption and all-cause mortality. J. Stud. Alcohol Drugs 2016, 77, 185–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knott, C.S.; Coombs, N.; Stamatakis, E.; Biddulph, J.P. All cause mortality and the case for age specific alcohol consumption guidelines: Pooled analyses of up to 10 population based cohorts. BMJ (Clin. Res. Ed.) 2015, 350, h384. [Google Scholar] [CrossRef]
- Millwood, I.; Walters, R.; Mei, X.; Guo, Y.; Yang, L.; Bian, Z.; Bennett, D.; Chen, Y.; Dong, C.; Hu, R.; et al. Conventional and genetic evidence on alcohol and vascular disease aetiology: A prospective study of 500,000 men and women in china. Lancet 2019, 393, 1831–1842. [Google Scholar] [CrossRef] [Green Version]
- Holmes, M.V.; Dale, C.E.; Zuccolo, L.; Silverwood, R.J.; Guo, Y.; Ye, Z.; Prieto-Merino, D.; Dehghan, A.; Trompet, S.; Wong, A.; et al. Association between alcohol and cardiovascular disease: Mendelian randomisation analysis based on individual participant data. BMJ (Clin. Res. Ed.) 2014, 349, g4164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rumgay, H.; Shield, K.; Charvat, H.; Ferrari, P.; Sornpaisarn, B.; Obot, I.; Islami, F.; Lemmens, V.; Rehm, J.; Soerjomataram, I. Global burden of cancer in 2020 attributable to alcohol consumption: A population-based study. Lancet Oncol. 2021, 22, 1071–1080. [Google Scholar] [CrossRef]
- Tomiyama, H.; Matsumoto, C.; Yamada, J.; Yoshida, M.; Shiina, K.; Yamashina, A. Abstract 2931: Raised blood pressure modifies the association between alcohol intake and the progression of arterial stiffness: An 6 years’ observational study. Circulation 2007, 116, II_654. [Google Scholar] [CrossRef]
- Lassaletta, A.; Elmadhun, N.; Liu, Y.; Feng, J.; Burgess, T.; Karlson, N.; Laham, R.; Sellke, F. Ethanol promotes arteriogenesis and restores perfusion to chronically ischemic myocardium. Circulation 2013, 128, S136–S143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, L.; Lassaletta, A.; Robich, M.; Liu, Y.; Burgess, T.; Laham, R.; Sweeney, J.; Shen, T.; Sellke, F. Effects of red wine and vodka on collateral-dependent perfusion and cardiovascular function in hypercholesterolemic swine. Circulation 2012, 126, S65–S72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Femia, R.; Natali, A.; L’Abbate, A.; Ferrannini, E. Coronary atherosclerosis and alcohol consumption: Angiographic and mortality data. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 1607–1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, S. Alcohol consumption, hypertension, and cardiovascular health across the life course: There is no such thing as a one-size-fits-all approach. J. Am. Heart Assoc. 2018, 7, e009698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Byrd, J.; Rodriguez, C. Use of physician-recommended non-pharmacological strategies for hypertension control among hypertensive patients. J. Clin. Hypertens. 2018, 20, 518–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, E. To drink or not to drink: That is the question. Alcohol. Clin. Exp. Res. 2014, 38, 2889–2892. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M.; Kaczorowski, J.; Tobe, S.; Gmel, G.; Hasan, O.; Rehm, J. The effect of a reduction in alcohol consumption on blood pressure: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e108–e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, S.; Lee, H.; Han, K.; Jeon, K.; Kim, D.; Yoo, J.; Cho, M.; Chun, S.; Lee, S.; Nam, K.; et al. Association of change in alcohol consumption with risk of ischemic stroke. Stroke 2022, 53, 2488–2496. [Google Scholar] [CrossRef] [PubMed]
- Salottolo, K.; McGuire, E.; Mains, C.; van Doorn, E.; Bar-Or, D. Occurrence, predictors, and prognosis of alcohol withdrawal syndrome and delirium tremens following traumatic injury. Crit. Care Med. 2017, 45, 867–874. [Google Scholar] [CrossRef]
- Northcote, J.; Livingston, M. Accuracy of self-reported drinking: Observational verification of ‘last occasion’ drink estimates of young adults. Alcohol Alcohol. 2011, 46, 709–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimm, E.; Klatsky, A.; Grobbee, D.; Stampfer, M. Review of moderate alcohol consumption and reduced risk of coronary heart disease: Is the effect due to beer, wine, or spirits. BMJ (Clin. Res. Ed.) 1996, 312, 731–736. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall (N = 5298) | Non-Drinker (N = 2238) | Light Drinker (N = 1712) | Moderate Drinker (N = 1169) | Heavy Drinker (N = 179) | p-Value |
|---|---|---|---|---|---|---|
| Demographics | ||||||
| Age (years) | 62.6 ± 12.7 | 64.1 ± 13.0 | 62.4 ± 13.0 | 60.1 ± 11.4 | 63.3 ± 9.8 | <0.001 |
| Male, (n%) | 2564 (48.4) | 277 (12.4) | 994 (58.1) | 1115 (95.4) | 178 (99.4) | <0.001 |
| Married, n (%) | 4310 (81.4) | 1695 (75.7) | 1399 (81.7) | 1055 (90.3) | 161 (89.9) | <0.001 |
| Urban, n (%) | 1396 (26.4) | 550 (24.6) | 488 (28.5) | 321 (27.5) | 37 (20.7) | 0.010 |
| Education | ||||||
| Less than high school, n (%) | 4369 (82.5) | 1942 (86.8) | 1383 (80.8) | 899 (76.9) | 145 (81.0) | <0.001 |
| High school or equivalent, n (%) | 782 (14.8) | 259 (11.6) | 270 (15.8) | 223 (19.1) | 30 (16.8) | |
| College or above, n (%) | 147 (2.8) | 37 (1.7) | s59 (3.5) | 47 (4.0) | 4 (2.2) | |
| Physical examination * | ||||||
| Mean SBP (mmHg) | 121.9 ± 13.3 | 121.7 ± 14.2 | 121.4 ± 13.2 | 122.7 ± 11.8 | 125.2 ± 12.6 | <0.001 |
| Mean DBP (mmHg) | 78.3 ± 7.5 | 77.4 ± 7.6 | 78.0 ± 7.4 | 79.8 ± 7.2 | 80.4 ± 7.8 | <0.001 |
| Mean PP (mmHg) | 43.7 ± 8.7 | 44.3 ± 9.4 | 43.4 ± 8.6 | 42.9 ± 7.5 | 44.8 ± 8.5 | <0.001 |
| Mean BMI (kg/m2) † | 22.5 (20.7–24.5) | 22.5 (20.7–24.8) | 22.4 (20.8–24.4) | 22.4 (20.8–24.5) | 21.9 (20.6–23.3) | 0.047 |
| Mean waist circumference (cm) † | 79.3 (74.3–85.0) | 78.7 (73.4–84.4) | 79.3 (74.5–85.2) | 80.5 (75.5–86.3) | 79.8 (75.1–84.8) | <0.001 |
| Smoking status | ||||||
| Never, n (%) | 2800 (84.9) | 1900 (84.9) | 767 (44.8) | 121 (10.4) | 12 (6.7) | <0.001 |
| Former, n (%) | 459 (8.7) | 82 (3.7) | 204 (11.9) | 146 (12.5) | 27 (15.1) | |
| Current, n (%) | 2039 (38.5) | 256 (11.4) | 741 (43.3) | 902 (77.2) | 140 (78.2) | |
| Alcohol consumption * | ||||||
| Mean alcohol consumption unit † | 0.75 (0–8.8) | 0 | 2.2 (0.8–4.9) | 17.2 (11.5–25.6) | 51.8 (42.7–61.3) | <0.001 |
| Self-reported comorbidities | ||||||
| Hypertension, n (%) | 1284 (24.2) | 581 (26.0) | 378 (22.1) | 282 (24.1) | 43 (24.0) | 0.047 |
| Diabetes mellitus, n (%) | 301 (5.7) | 147 (6.6) | 102 (6.0) | 46 (3.9) | 6 (3.4) | 0.007 |
| Myocardial infraction, n (%) | 124 (2.3) | 53 (2.4) | 50 (2.9) | 17 (1.5) | 4 (2.2) | 0.077 |
| Stroke, n (%) | 182 (3.4) | 71 (3.2) | 69 (4.0) | 39 (3.3) | 3 (1.7) | 0.262 |
| Malignant tumor, n (%) | 40 (0.8) | 14 (0.6) | 16 (0.9) | 8 (0.7) | 2 (1.1) | 0.543 |
| Events/Total (%) | Person-Years | Crude HR (95% CI) | p-Value | Adjusted HR * (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| All participants | 568/5298 (10.7%) | 97,742 | - | - | - | - |
| Non-drinker | 241/2238 (10.8) | 40,728 | Ref | Ref | Ref | Ref |
| Light drinker | 185/1712 (10.8) | 31,800 | 0.97 (0.80–1.18) | 0.771 | 0.76 (0.61–0.95) | 0.014 |
| Moderate drinker | 111/1169 (9.5) | 21,878 | 0.84 (0.67–1.06) | 0.136 | 0.61 (0.46–0.81) | 0.001 |
| Heavy drinker | 31/179 (17.3) | 3337 | 1.55 (1.07–2.25) | 0.022 | 0.95 (0.63–1.43) | 0.792 |
| Events/Total (%) | Crude OR (95% CI) | p-Value | Adjusted OR * (95% CI) | p-Value | |
|---|---|---|---|---|---|
| All participants | 1284/5298 (24.2) | - | - | - | - |
| Non-drinker | 581/2238 (26.0) | Ref | Ref | Ref | Ref |
| Light drinker | 378/1712 (22.1) | 0.81 (0.70–0.94) | 0.771 | 0.84 (0.72–0.99) | 0.038 |
| Moderate drinker | 282/1169 (24.1) | 0.91 (0.77–1.07) | 0.242 | 1.13 (0.94–1.35) | 0.187 |
| Heavy drinker | 43/179 (24.0) | 0.90 (0.63–1.29) | 0.569 | 1.08 (0.74–1.57) | 0.692 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, W.; Cai, A.; Li, L.; Feng, Y. Longitudinal Trajectories of Alcohol Consumption with All-Cause Mortality, Hypertension, and Blood Pressure Change: Results from CHNS Cohort, 1993–2015. Nutrients 2022, 14, 5073. https://doi.org/10.3390/nu14235073
Qiu W, Cai A, Li L, Feng Y. Longitudinal Trajectories of Alcohol Consumption with All-Cause Mortality, Hypertension, and Blood Pressure Change: Results from CHNS Cohort, 1993–2015. Nutrients. 2022; 14(23):5073. https://doi.org/10.3390/nu14235073
Chicago/Turabian StyleQiu, Weida, Anping Cai, Liwen Li, and Yingqing Feng. 2022. "Longitudinal Trajectories of Alcohol Consumption with All-Cause Mortality, Hypertension, and Blood Pressure Change: Results from CHNS Cohort, 1993–2015" Nutrients 14, no. 23: 5073. https://doi.org/10.3390/nu14235073