

Evaluation of a Dietary Supplementation Combining Protein and a Pomegranate Extract in Older People: A Safety Study
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design and Randomization
2.3. Safety Measurements
2.4. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
3.2. Primary Outcomes
3.3. Secondary Outcomes
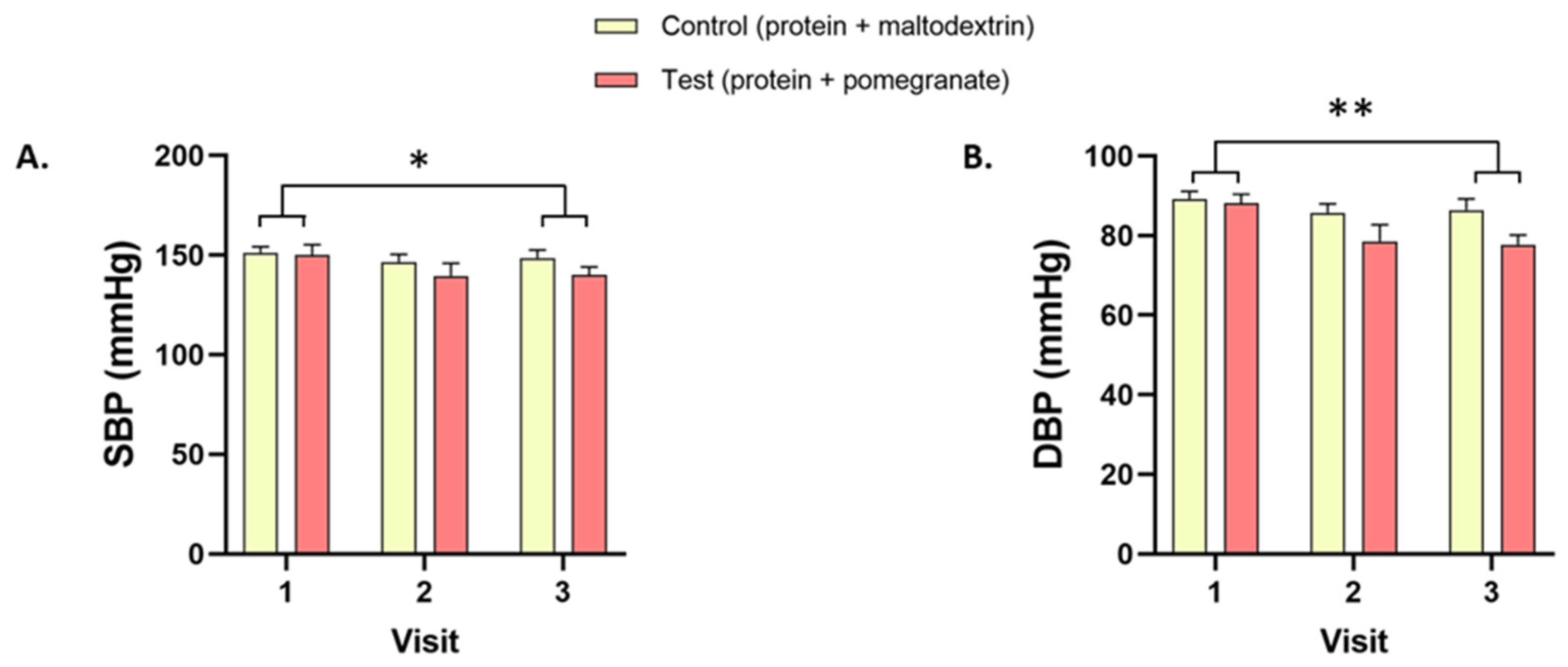
3.3.1. Physical Parameters
3.3.2. Hematological Parameters
3.3.3. Biochemical Parameters
3.3.4. Compliance
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Correia, M.I.; Waitzberg, D.L. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin. Nutr. 2003, 22, 235–239. [Google Scholar] [CrossRef]
- Norman, K.; Hass, U.; Pirlich, M. Malnutrition in Older Adults-Recent Advances and Remaining Challenges. Nutrients 2021, 13, 2764. [Google Scholar] [CrossRef]
- Corish, C.A.; Kennedy, N.P. Protein-energy undernutrition in hospital in-patients. Br. J. Nutr. 2000, 83, 575–591. [Google Scholar] [CrossRef] [Green Version]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef]
- Beaudart, C.; Reginster, J.Y.; Petermans, J.; Bruyere, O. [Quality of life of sarcopenic patients: Contribution of the SarcoPhAge study]. Geriatr. Psychol. Neuropsychiatr. Vieil. 2015, 13, 391–395. [Google Scholar] [CrossRef]
- Baum, J.I.; Kim, I.Y.; Wolfe, R.R. Protein Consumption and the Elderly: What Is the Optimal Level of Intake? Nutrients 2016, 8, 359. [Google Scholar] [CrossRef] [Green Version]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [Green Version]
- Chanet, A.; Verlaan, S.; Salles, J.; Giraudet, C.; Patrac, V.; Pidou, V.; Pouyet, C.; Hafnaoui, N.; Blot, A.; Cano, N.; et al. Supplementing Breakfast with a Vitamin D and Leucine-Enriched Whey Protein Medical Nutrition Drink Enhances Postprandial Muscle Protein Synthesis and Muscle Mass in Healthy Older Men. J. Nutr. 2017, 147, 2262–2271. [Google Scholar] [CrossRef] [Green Version]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B.; et al. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef] [Green Version]
- Volkert, D.; Hubsch, S.; Oster, P.; Schlierf, G. Nutritional support and functional status in undernourished geriatric patients during hospitalization and 6-month follow-up. Aging 1996, 8, 386–395. [Google Scholar] [CrossRef]
- Mathewson, S.L.; Azevedo, P.S.; Gordon, A.L.; Phillips, B.E.; Greig, C.A. Overcoming protein-energy malnutrition in older adults in the residential care setting: A narrative review of causes and interventions. Ageing Res. Rev. 2021, 70, 101401. [Google Scholar] [CrossRef]
- Clegg, M.E.; Williams, E.A. Optimizing nutrition in older people. Maturitas 2018, 112, 34–38. [Google Scholar] [CrossRef]
- Jauhar, S.; Ismail-Fitry, M.R.; Chong, G.H.; NorKhaizura, M.A.R.; Ibadullah, W.Z.W. Polyphenol Compounds from Pomegranate (Punica Granatum) Extracted via Various Methods and its Application on Meat and Meat Products: A Review. J. Adv. Res. Appl. Sci. Eng. Technol. 2018, 12, 1–12. [Google Scholar]
- Trombold, J.R.; Reinfeld, A.S.; Casler, J.R.; Coyle, E.F. The effect of pomegranate juice supplementation on strength and soreness after eccentric exercise. J. Strength Cond. Res. 2011, 25, 1782–1788. [Google Scholar] [CrossRef]
- Torregrosa-Garcia, A.; Avila-Gandia, V.; Luque-Rubia, A.J.; Abellan-Ruiz, M.S.; Querol-Calderon, M.; Lopez-Roman, F.J. Pomegranate Extract Improves Maximal Performance of Trained Cyclists after an Exhausting Endurance Trial: A Randomised Controlled Trial. Nutrients 2019, 11, 721. [Google Scholar] [CrossRef] [Green Version]
- Laurindo, L.F.; Barbalho, S.M.; Marquess, A.R.; Grecco, A.I.S.; Goulart, R.A.; Tofano, R.J.; Bishayee, A. Pomegranate (Punica granatum L.) and Metabolic Syndrome Risk Factors and Outcomes: A Systematic Review of Clinical Studies. Nutrients 2022, 14, 1665. [Google Scholar] [CrossRef]
- Vucic, V.; Grabez, M.; Trchounian, A.; Arsic, A. Composition and Potential Health Benefits of Pomegranate: A Review. Curr. Pharm. Des. 2019, 25, 1817–1827. [Google Scholar] [CrossRef]
- Aviram, M.; Dornfeld, L.; Kaplan, M.; Coleman, R.; Gaitini, D.; Nitecki, S.; Hofman, A.; Rosenblat, M.; Volkova, N.; Presser, D.; et al. Pomegranate juice flavonoids inhibit low-density lipoprotein oxidation and cardiovascular diseases: Studies in atherosclerotic mice and in humans. Drugs Exp. Clin. Res. 2002, 28, 49–62. [Google Scholar]
- Koopman, R.; Wagenmakers, A.J.; Manders, R.J.; Zorenc, A.H.; Senden, J.M.; Gorselink, M.; Keizer, H.A.; van Loon, L.J. Combined ingestion of protein and free leucine with carbohydrate increases postexercise muscle protein synthesis in vivo in male subjects. Am. J. Physiol. Endocrinol. Metab. 2005, 288, E645–E653. [Google Scholar] [CrossRef]
- Colonetti, T.; Grande, A.J.; Milton, K.; Foster, C.; Alexandre, M.C.; Uggioni, M.L.; Rosa, M.I. Effects of whey protein supplement in the elderly submitted to resistance training: Systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2017, 68, 257–264. [Google Scholar] [CrossRef]
- Kuo, Y.Y.; Chang, H.Y.; Huang, Y.C.; Liu, C.W. Effect of Whey Protein Supplementation in Postmenopausal Women: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4210. [Google Scholar] [CrossRef]
- Machin, D.R.; Christmas, K.M.; Chou, T.H.; HIll, S.C.; Van Pelt, D.W.; Trombold, J.R.; Coyle, E.F. Effects of Differing Dosages of Pomegranate Juice Supplementation after Eccentric Exercise. Physiol. J. 2014, 2014, 271959. [Google Scholar] [CrossRef]
- Rivara, M.B.; Mehrotra, R.; Linke, L.; Ruzinski, J.; Ikizler, T.A.; Himmelfarb, J. A pilot randomized crossover trial assessing the safety and short-term effects of pomegranate supplementation in hemodialysis patients. J. Ren. Nutr. 2015, 25, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Heber, D.; Seeram, N.P.; Wyatt, H.; Henning, S.M.; Zhang, Y.; Ogden, L.G.; Dreher, M.; Hill, J.O. Safety and antioxidant activity of a pomegranate ellagitannin-enriched polyphenol dietary supplement in overweight individuals with increased waist size. J. Agric. Food Chem. 2007, 55, 10050–10054. [Google Scholar] [CrossRef]
- Goodarzi, R.; Jafarirad, S.; Mohammadtaghvaei, N.; Dastoorpoor, M.; Alavinejad, P. The effect of pomegranate extract on anthropometric indices, serum lipids, glycemic indicators, and blood pressure in patients with nonalcoholic fatty liver disease: A randomized double-blind clinical trial. Phytother. Res. 2021, 35, 5871–5882. [Google Scholar] [CrossRef]
- Wolfe, R.R.; Miller, S.L.; Miller, K.B. Optimal protein intake in the elderly. Clin. Nutr. 2008, 27, 675–684. [Google Scholar] [CrossRef]
- Kesteloot, H.E.; Joossens, J.V. Relationship between dietary protein intake and serum urea, uric acid and creatinine, and 24-hour urinary creatinine excretion: The BIRNH Study. J. Am. Coll. Nutr. 1993, 12, 42–46. [Google Scholar] [CrossRef]
- Nuttall, F.Q.; Gannon, M.C.; Saeed, A.; Jordan, K.; Hoover, H. The metabolic response of subjects with type 2 diabetes to a high-protein, weight-maintenance diet. J. Clin. Endocrinol. Metab. 2003, 88, 3577–3583. [Google Scholar] [CrossRef] [Green Version]
- Oh, C.; No, J.K. Appropriate protein intake is one strategy in the management of metabolic syndrome in Korean elderly to mitigate changes in body composition. Nutr. Res. 2018, 51, 21–28. [Google Scholar] [CrossRef]
- Huang, X.J.; Choi, Y.K.; Im, H.S.; Yarimaga, O.; Yoon, E.; Kim, H.S. Aspartate aminotransferase (AST/GOT) and alanine aminotransferase (ALT/GPT) detection techniques. Sensors 2006, 6, 756–782. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Description of the Adverse Event | Intensity of the Event | Causal Relation of the Event to the Study Product | |
|---|---|---|---|
| Test | COVID | Moderate | Not related |
| Intestinal problems | Moderate | Maybe related | |
| Intestinal problems | Moderate | Unlikely related | |
| Headache | Mild | Not related | |
| Tendinitis | Moderate | Not related | |
| Control | Lung infection | Moderate | Not related |
| COVID | Mild | Not related | |
| COVID | Moderate | Not related | |
| Eczema | Moderate | Unlikely related | |
| Sciatic nerve inflammation | Moderate | Not related | |
| Painful tooth extraction | Moderate | Not related |
| Test (n = 14) | Control (n = 15) | |||||
|---|---|---|---|---|---|---|
| V1 | V2 | V3 | V1 | V2 | V3 | |
| Physical parameters | ||||||
| Weight (kg) | 70.9 ± 14.7 | 72.8 ± 16.7 | 72.1 ± 16.0 | 72.3 ± 10.6 | 70.2 ± 10.4 | 72.3 ± 11.6 |
| Heart rate (bpm) | 64.9 ± 6.9 | 66.6 ± 11.4 | 71.1 ± 12.0 | 65.3 ± 11.0 | 67.4 ± 17.7 | 65.9 ± 12.3 |
| Body Mass Index (kg/m2) | 25.7 ± 3.2 | 26.8 ± 3.5 | 26.5 ± 3.3 | 24.7 ± 2.2 | 24.3 ± 2.5 | 25.0 ± 3.1 |
| Hematological parameters | ||||||
| White blood cells (103/μL) | 5.89 ± 1.38 | 5.82 ± 1.24 | 5.83 ± 1.13 | 5.57 ± 1.01 | 5.83 ± 1.37 | 5.50 ± 1.21 |
| Red blood cells (106/μL) | 4.62 ± 0.30 | 4.59 ± 0.29 | 4.53 ± 0.26 | 4.68 ± 0.42 | 4.69 ± 0.35 | 4.64 ± 0.35 |
| Hemoglobin (g/dL) | 13.9 ± 1.2 | 13.7 ± 0.9 | 13.6 ± 0.9 * | 14.1 ± 1.1 | 14.0 ± 1.0 | 14.0 ± 1.0 * |
| Hematocrit (%) | 41.0 ± 2.8 | 40.6 ± 2.4 | 40.2 ± 2.4 | 41.3 ± 3.1 | 41.4 ± 2.8 | 41.3 ± 2.7 |
| Platelet count (103/μL) | 267.6 ± 40.6 | 265.1 ± 47.7 | 265.6 ± 36.8 | 241.8 ± 46.6 | 248.3 ± 45.3 | 245.7 ± 42.9 |
| Biochemical parameters | ||||||
| Uric acid (mg/dL) | 5.20 ± 1.26 | 4.76 ± 1.12 *** | 4.59 ± 1.07 *** | 5.52 ± 1.33 | 4.96 ± 1.39 *** | 4.99 ± 1.17 *** |
| Creatinine (mg/dL) | 0.80 ± 0.17 | 0.77 ± 0.12 | 0.74 ± 0.15 | 0.81 ± 0.15 | 0.80 ± 0.16 | 0.80 ± 0.17 |
| Total bilirubin (mg/dL) | 0.77 ± 0.27 | 0.72 ± 0.24 | 0.69 ± 0.26 | 0.84 ± 0.40 | 0.79 ± 0.39 | 0.82 ± 0.41 |
| GOT (U/L) | 23.4 ± 6.6 | 22.6 ± 5.5 | 21.4 ± 4.0 | 22.6 ± 4.2 | 23.6 ± 9.7 | 23.7 ± 5.8 |
| Triglycerides (mg/dL) | 121.9 ± 72.5 | 109.2 ± 45.9 | 106.8 ± 59.9 | 98.2 ± 43.6 | 99.1 ± 48.9 | 94.5 ± 44.2 |
| Sodium (mmol/L) | 139.6 ± 2.3 | 139.7 ± 2.5 | 140.1 ± 2.1 | 139.5 ± 2.0 | 139.5 ± 2.8 | 139.5 ± 2.2 |
| Potassium (mmol/L) | 4.32 ± 0.30 | 4.68 ± 0.37 *** | 4.59 ± 0.37 *** | 4.37 ± 0.21 | 4.78 ± 0.36 *** | 4.53 ± 0.40 *** |
| Total protein (g/L) | 68.4 ± 3.7 | 68.0 ± 3.1 | 66.5 ± 3.7 | 66.9 ± 3.0 | 67.2 ± 2.7 | 66.8 ± 3.3 |
| Urea (mg/dL) | 37.1 ± 10.4 | 42.1 ± 10.0 * | 40.1 ± 6.1 | 35.7 ± 10.2 | 39.7 ± 9.4 * | 37.7 ± 7.8 |
| Blood glucose (mg/dL) | 89.3 ± 9.2 | 87.6 ± 8.1 | 90.1 ± 11.5 | 89.1 ± 8.6 | 88.1 ± 7.3 | 89.9 ± 9.6 |
| Alkaline phosphatase (U/L) | 69.1 ± 22.9 | 68.4 ± 21.4 | 68.5 ± 20.8 | 68.8 ± 15.4 | 68.0 ± 13.8 | 68.3 ± 12.6 |
| GGT (U/L) | 27.4 ± 19.2 | 25.2 ± 16.8 | 24.6 ± 15.2 | 23.3 ± 8.5 | 24.2 ± 11.7 | 24.7 ± 14.4 |
| LDH (U/L) | 168.1 ± 21.1 | 168.9 ± 21.8 | 166.5 ± 26.6 | 175.2 ± 29.6 | 169.5 ± 24.2 | 174.2 ± 23.3 |
| CRP (mg/L) | 2.26 ± 1.75 | 2.71 ± 1.43 | 3.88 ± 6.86 | 1.79 ± 1.12 | 1.55 ± 0.85 | 1.65 ± 1.21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dormal, V.; Pachikian, B.; Debock, E.; Buchet, M.; Copine, S.; Deldicque, L. Evaluation of a Dietary Supplementation Combining Protein and a Pomegranate Extract in Older People: A Safety Study. Nutrients 2022, 14, 5182. https://doi.org/10.3390/nu14235182
Dormal V, Pachikian B, Debock E, Buchet M, Copine S, Deldicque L. Evaluation of a Dietary Supplementation Combining Protein and a Pomegranate Extract in Older People: A Safety Study. Nutrients. 2022; 14(23):5182. https://doi.org/10.3390/nu14235182
Chicago/Turabian StyleDormal, Valérie, Barbara Pachikian, Elena Debock, Marine Buchet, Sylvie Copine, and Louise Deldicque. 2022. "Evaluation of a Dietary Supplementation Combining Protein and a Pomegranate Extract in Older People: A Safety Study" Nutrients 14, no. 23: 5182. https://doi.org/10.3390/nu14235182
APA StyleDormal, V., Pachikian, B., Debock, E., Buchet, M., Copine, S., & Deldicque, L. (2022). Evaluation of a Dietary Supplementation Combining Protein and a Pomegranate Extract in Older People: A Safety Study. Nutrients, 14(23), 5182. https://doi.org/10.3390/nu14235182