1. Introduction
Parkinson’s disease is described as a progressive disorder characterized by degeneration of the dopaminergic neurons of the substantia nigra in the midbrain [
1] and the presence of alpha-synuclein-positive cytoplasmic inclusions called Lewy bodies [
2]. It was first described by British doctor James Parkinson in the “Essay on Shaking Palsy” in 1817. [
3] Patients experience progressing decreases in motor and cognitive functions and higher mortality [
1]. The most common symptoms are bradykinesia, rigidity, postural reflex impairment, and resting tremor [
1,
3]. Some psychiatric symptoms, such as anxiety, dementia and depression, can be noted in patients with Parkinson’s disease [
3], as well as sleep disorders, especially insomnia and REM behavioral disorder [
2]. Other noticeable symptoms are fatigue, constipation, hypotension, cramps, and seborrheic dermatitis [
3].
The diagnosis is especially hard in the early stages of the disease because its symptoms are common to other conditions such as vascular parkinsonism, essential tremor, or progressive supranuclear palsy [
1]. The diagnostics are based on clinical criteria, such as parkinsonism and no history of drugs, toxins, or infections, also excluding the signs of other neurological damage [
3]. Most PD cases are caused sporadically, and only a small number of patients carry disease-causing genetic mutations [
2].
There are two groups of substances that can be used in the treatment of Parkinson’s disease: levodopa and monoamine oxidase-B inhibitors. Levodopa is an agonist of dopamine and is administered with carbidopa. It inhibits the metabolism of levodopa and allows the therapeutic concentration of the drug to enter the brain [
1]. It is the most effective drug used in Parkinson’s disease treatment. Its chemical structure allows it to compete with neutral amino acids for intestinal absorption. Due to that, levodopa should be administered at least 30 min before each meal. This facilitates the avoidance of drug interaction with dietary protein. Side effects of antiparkinsonian drugs are often reported by patients as symptoms contributing to an increased risk of weight loss. Among the most frequently mentioned side effects are: abdominal pain, vomiting, dyspepsia, dry mouth, diarrhea or constipation, and other gastrointestinal disorders [
4,
5,
6].
One of the conditions which leads to an increased risk of malnutrition in PD patients is oropharyngeal dysphagia. It is estimated that around 80% of patients suffer from this kind of issue in the early stages of the disease. The incidence increases to 95% in later stages. Delayed oropharyngeal transition time and reduced muscle strength are most common in this group of patients. Due to dehydration, malnutrition, possible silent penetration, and aspiration of consumed foods to the lungs, the mortality rate increases significantly [
7]. Swallowing dysfunctions in PD patients are diagnosed using the VFSS and FEES tests. A multidisciplinary approach is necessary for the proper management of dysphagia in PD patients [
8].
Patients with Parkinson’s disease are at high risk of weight loss and malnutrition. Weight loss may be present at diagnosis and is associated with increased energy expenditure due to tremors and rigidity. It leads to an increase in the daily dose of levodopa, which results in the worsening of dyskinesias. Weight gain can be noticed as well. It usually occurs because of dopaminergic treatment or deep brain stimulation (DBS). This should be taken into consideration, since it usually results in a fat mass gain, mostly in the abdominal area, and leads to an increased risk of metabolic syndrome [
9].
Due to the many negative aspects of Parkinson’s disease (such as the aforementioned unintentional changes in body weight, swallowing difficulties, drug side effects, and more), there is a need for regular evaluation of nutritional status among this group of patients.
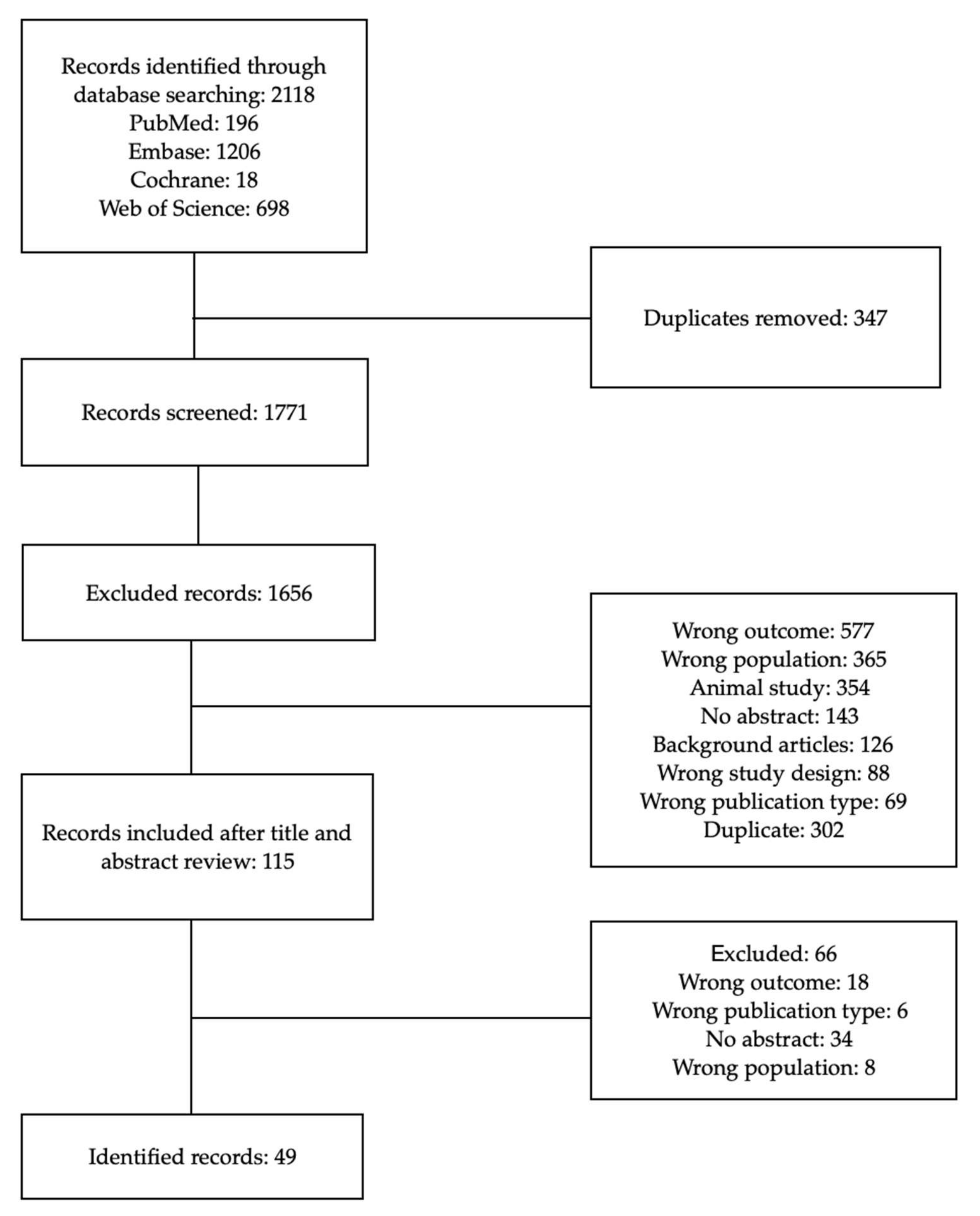
This study aimed to review the nutritional status of patients with Parkinson’s disease and to determine the prevalence of malnutrition in the mentioned group—and to assess the need for nutritional status screening.
4. Discussion
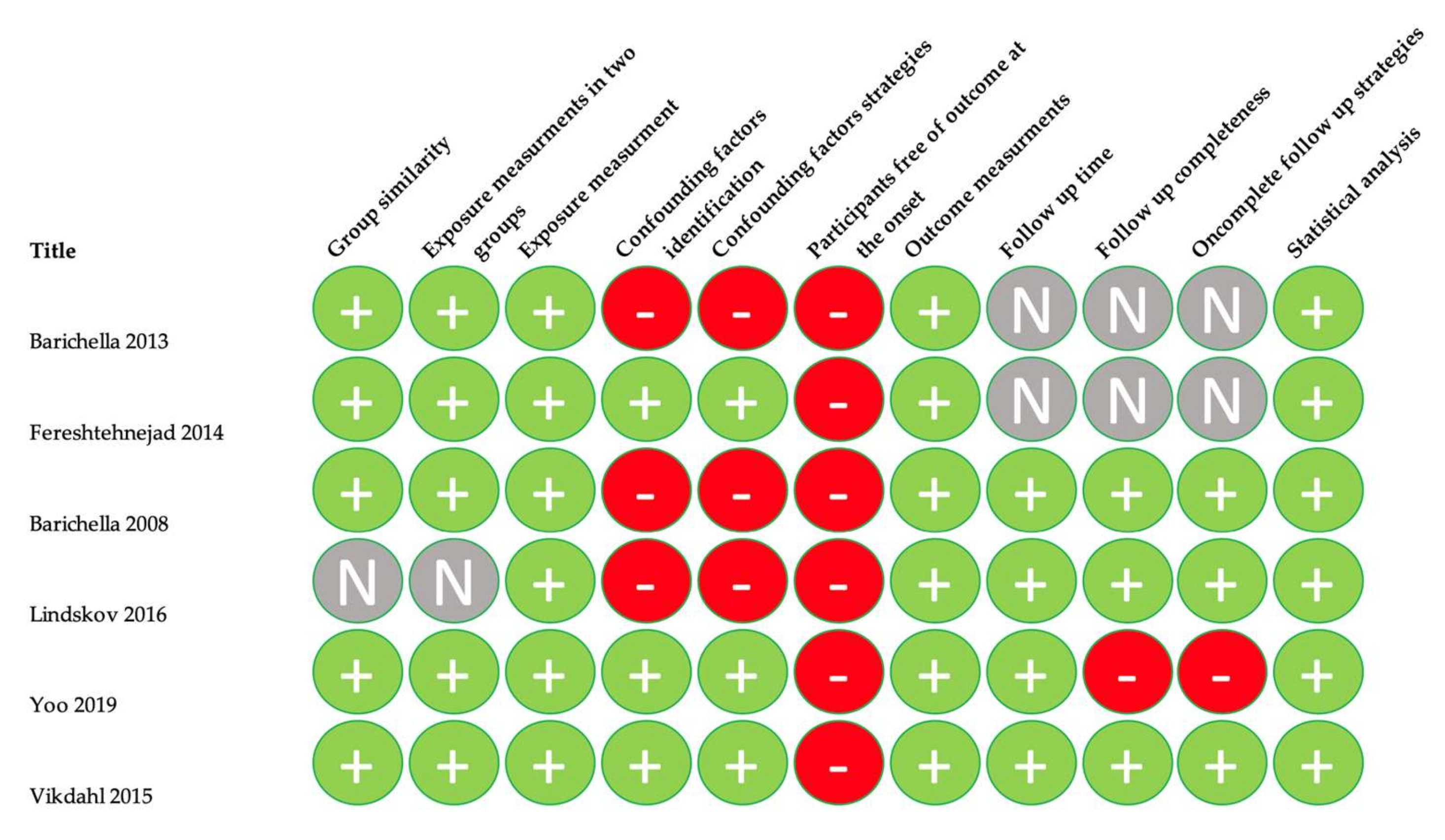
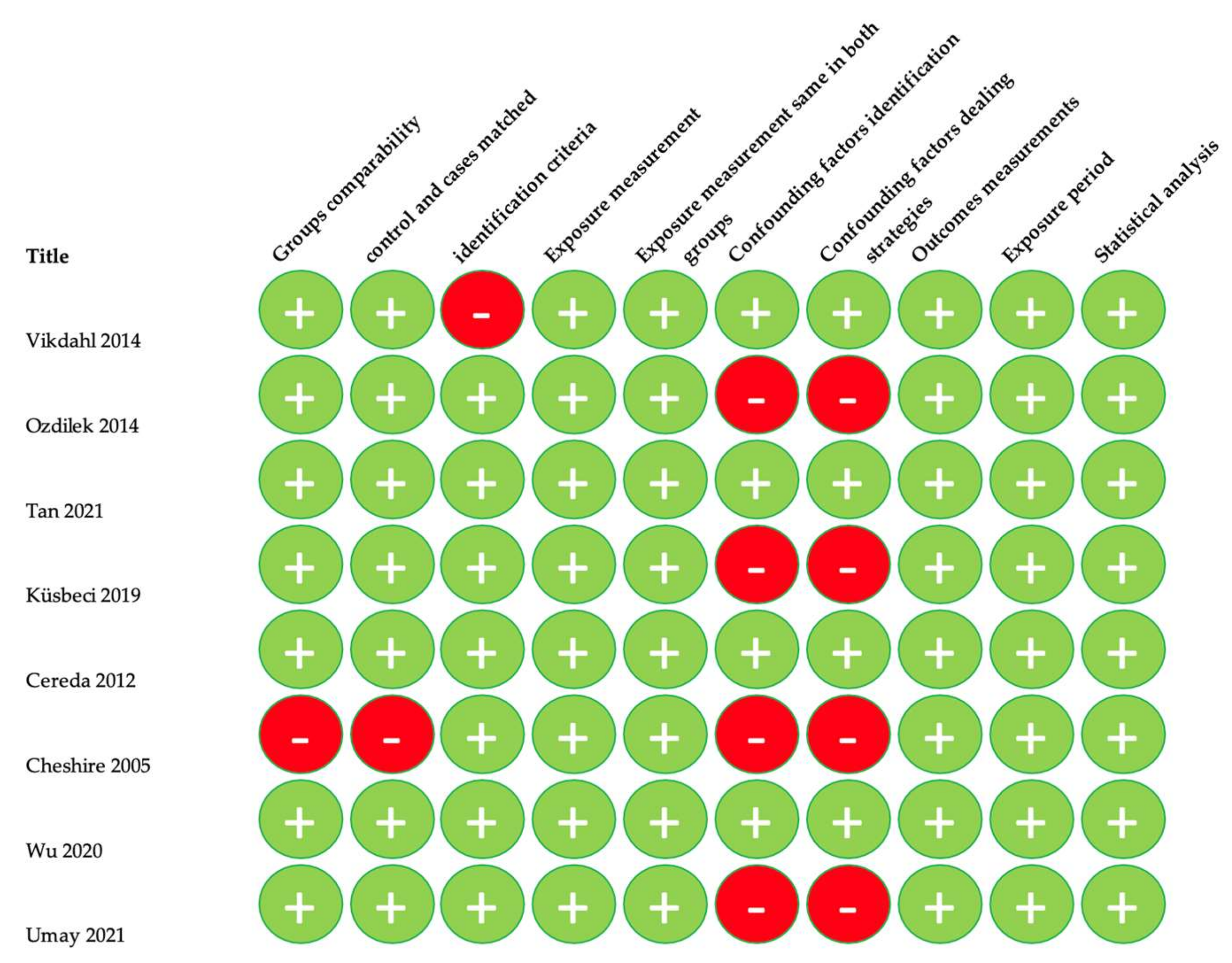
Our systematic review aimed to show the prevalence of malnutrition among patients suffering from Parkinson’s disease. We included 49 studies from 21 countries. We noted that there were disbalances in the results of each questionnaire and method of nutritional status assessment.
Malnutrition is a common issue experienced by patients suffering from Parkinson’s Disease which results in poor health of the patients. Adequate assessment methods and management strategies are needed, as malnutrition affects these groups excessively. There are many coexisting factors that should be taken into consideration at the onset of the disease and during evaluations, such as probable swallowing disorders. Dysphagia affects a significant number of PD patients, and severe dysphagia appears mostly in advanced stages of Parkinson’s disease. Hoehn and Yahr stages 4 and 5, recent weight loss, sialorrhea, and BMI < 20 kg/m
2 have been considered to predict dysphagia in the mentioned group [
8].
Weight loss is another factor strongly associated with malnutrition in PD patients, as it results in cognitive decline, orthostatic hypotension, and dyskinesia. These, in turn, lead to the intake of a higher dosage of levodopa. Both weight loss and malnutrition are a result of negative energy balance, meaning that the intake is lower than the expenditure of energy [
59]. It can also be related to hyposmia, which is a decrease in the capability to sense a smell. Hyposmia is also considered to be one of the earliest non-motor symptoms of PD [
60].
Energy balance is known as homeostasis and is a process in which the human body adjusts food intake and energy expenditure. In healthy individuals, the input of energy equals the output. In PD patients, both disease-related and treatment-related factors can contribute to disturbed energy balance correlated with dopaminergic deficit. In early stages of Parkinson’s disease, symptoms like sensory disfunction or gastrointestinal disfunction are associated with weight loss due to decreased food consumption. In later stages, when motor symptoms are more common, energy expenditure increases. [
59] Resting energy expenditure (REE) is hard to assess. Some authors pointed out that REE was higher in untreated patients than in those treated with L-dopa [
61], while some authors suggested that REE remained unchanged between untreated and treated individuals [
62]. REE is associated with tremor and rigidity. Those two symptoms are strongly associated with Parkinson’s disease and contribute to increased energy expenditure and weight loss.
Another predictor of weight loss and future risk of malnutrition is gastrointestinal dysfunction, which is common in PD patients and can precede motor defects by years. Parkinson’s Disease is associated with intestinal inflammation and other gastrointestinal abnormalities, such as constipation or dysbiosis [
63].
Early detection of weight loss can lead to early notice of malnutrition risk, which makes it possible to improve a patient’s quality of life. Nutritional intervention is meant to improve negative aspects of Parkinson’s disease (e.g., managing swallowing difficulties or maintaining proper body weight), resulting in better quality of life and helping to reduce the progression of the disease. A study by Sheard J. et al. showed that malnourished patients experienced lower life quality than well-nourished patients—and that nutritional intervention helped to improve emotional well-being [
64]. The authors concluded that early detection of weight loss could help to prevent malnutrition and reduction in quality of patients’ lives.
Various tools are used to screen the nutritional status of patients. Aside from biochemical factors or recent weight loss, specific questionnaires are currently in use. One of the most common is the Malnutrition Universal Screening Tool (MUST), which was developed to assess patients in all kinds of ambulatory care [
65]. It includes body mass index value, weight loss for the past 3–6 months, and anorexia associated with an illness in the past 5 days. It also includes two questions about unintentional weight loss and a decrease in food intake [
66].
The Seniors in Community: Risk Evaluation for Eating and Nutrition (SCREEN II) questionnaire consists of seventeen questions and assesses the risk of malnutrition based on the number of eaten meals, difficulties in eating such as dysphagia, changes in body mass, and social aspects of food intake in patients, e.g., living alone in their homes [
66].
Subjective Global Assessment (SGA) is the most commonly used tool for assessing nutritional status. It includes two kinds of information: medical history and physical examination. The first part includes recent weight loss, functional impairment, and changes in dietary intake, whereas the following part brings up loss of subcutaneous fat, oedema, and muscle wasting. Patients are classified as well nourished (SGA A), suspected or moderately malnourished (SGA B), or severely malnourished (SGA C). The downside of this questionnaire is that it does not monitor changes in nutritional status and does not include biochemical values [
28].
The MEONF-II screening tool was designed to determine the risk of undernutrition in hospital inpatients. The score ranges from 0 to 8 points. A score of 0–2 is considered a low risk of undernutrition, 3–4 a moderate risk and ≥5 is a high risk of undernutrition [
67].
The highest sensitivity can be found in the Mini Nutritional Assessment (MNA) questionnaire. It was first introduced to assess the risk of malnutrition in institutionalized geriatric patients and became useful in detecting probable malnutrition in senior patients when other parameters, such as biochemical factors and BMI, are still correct [
65]. It includes diverse components, such as: weight loss and depletion in food access in the past 3 months, changes in physical activity, psychological stress, and acute illness in the mentioned period, as well as anthropometric measurements, altered sense of smell and taste, or frailty. The MNA consists of eighteen questions divided into four domains. On the contrary, a shorter version called the MNA-SF consists of six questions and is considered to be as effective as the full sheet. If the MNA-SF score is 11 points or less, then the full version should be applied for proper assessment, and the patient is considered at risk of malnutrition [
65].
As can be seen from the characteristics of each questionnaire, some assess the risk of malnutrition among patients (MNA, MUST, and SCREEN-II), and others assess nutritional status in general (SGA). MEONF-II, on the other hand, assesses the risk of undernutrition.
One of the included studies, written by Yang T., Zhan Z. et al., showed 39.2% of patients assessed for malnutrition using the MNA questionnaire as malnourished and 30% as at risk of malnutrition, whereas 30.8% had good nutritional status [
10]. On the contrary, a study by Vikdahl M., Carlsson M. et al. showed no patients with malnutrition, and only 14% of the cohort were deemed at risk of malnutrition [
21].
Only one study that used MNA-SF showed the number of patients with malnutrition or at risk. Umay E., Yigman Z. A et al. pointed out that 14.8% of patients were at risk of malnutrition and 5.6% were already malnourished [
22].
Two studies included in our review in which authors used the MUST questionnaire showed comparable results. Barichella M., Cereda E. et al. showed 17.2% of patients at risk of malnutrition and 5% already malnourished [
15], while Jaafar A.F., Gray W.K. et al. showed 8.1% of patients at high risk of malnutrition and 15.4% of patients at moderate risk of malnutrition [
29].
We took into consideration only two studies where authors assessed the patients with SGA and PG-SGA questionnaires. The results showed around 15% of all cohorts, respectively, identified as level B (moderate malnutrition or at risk of malnutrition) and 0% as level C (severely malnourished) [
30,
31].
There was a problem with comparing results using SCREEN-II and MEONF-II due to an insufficient number of studies that used those tools in the assessment of patients [
16].
On the other hand, studies where authors used body mass index as a tool to measure malnutrition did not offer specific data, other than the fact that, in most studies, the mean BMI score showed patients as overweight or obese, with the highest score of 30.17 kg/m
2 [
23] and lowest 17.84 kg/m
2 [
46]. No study that measured only BMI showed the percentage of those malnourished or at risk of malnutrition. The overall results for BMI did not suggest any of the patients to be malnourished or at risk of malnutrition. BMI is used for measuring the weight category, but it is not a reliable way of measuring nutritional status. Thus, BMI is not an adequate assessment tool for assessing patients for malnutrition.
Many authors opted not to provide information on the exact number of patients at risk of malnutrition or malnourished, only the mean score of the questionnaire for the entire cohort studied [
13,
14,
17,
19,
20,
23,
24,
25,
26,
27,
28,
35,
37,
44,
46,
47,
48,
49,
50,
51,
52,
53,
54,
55,
56,
57,
58].
Comorbidities and community could have affected the results, but those were not taken into consideration while preparing this review.
Most studies provided information about disease severity in their cohorts. There were two scales used: Hoehn and Yahr scale and the MDS-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS). Some studies only provided the Hoehn and Yahr scale [
31,
32,
37,
41,
45,
51]. Sometimes authors reported the mean score, sometimes the median [
17,
21,
31,
38,
39,
41], and sometimes the percentage of patients on each level of the scale [
24,
50,
54,
56]. The same issue applied for the UPDRS scale, where various aspects of the scale were reported. A few studies did not provide any information on the disease severity of the cohort included in their research [
11,
16,
18,
19,
26,
27,
30,
34,
42,
46,
47,
49,
52,
55]. The authors showed no correlations between the disease severity and the nutritional status of the patients, leading to the conclusion that no connection existed between disease severity and the prevalence of malnutrition.
Biochemical markers are important factors that could provide more detailed insight into the problem of malnutrition. Albumin, prealbumin, total cholesterol, hemoglobin, and total protein could be useful in screening for malnutrition [
68], but were not included in our study. Screening assessments alone could be inadequate, pointing to a need for more precise markers, such as biochemical markers; however, due to limitations these needs could not be met. Additionally, weight loss may be hard to observe in overweight or obese patients; due to that more in-depth analysis will be needed.
Due to the absence of unified diagnostic criteria for malnutrition, ESPEN, ASPEN, PENSA and FELANPE created the Global Leadership Initiative on Malnutrition (GLIM). The first thing needed for diagnosing malnutrition is a screening tool of choice to determine those at risk of malnutrition. The GLIM authors pointed out criteria to look for in patients marked as at risk. Those are as follows: low body mass index, unintentional weight loss, reduced muscle mass, reduced food intake or assimilation, inflammation, or disease burden. The first three were categorized as phenotypic criteria, and the last two as etiologic criteria. For the diagnosis of malnutrition, the authors recommended that a combination of at least one phenotypic and one etiologic criterion is required [
69]. Weight loss is easy to assess by a doctor or caretaker of a patient. More attention should be paid to this criterion, as fast detection can be crucial in the proper management of malnutrition.
The GLIM diagnostic criteria for malnutrition should be applied to every patient diagnosed with Parkinson’s Disease, as all criteria mentioned by the authors are common in this group of patients. None of the studies reviewed in our study mentioned the GLIM criteria, and hardly any study was based solely on the problem of malnutrition in PD patients.
Another important guideline that mentioned the importance of screening for malnutrition in Parkinson’s Disease patients are the ESPEN guidelines for clinical nutrition in neurology. The authors mentioned that malnutrition was underreported in this group of patients and could be found in at least 15% of community-dwelling patients. The other 24% were at medium or high risk of malnutrition. They also pointed out the importance of screening for oropharyngeal dysphagia and gastrointestinal dysmotility. The first recommendation in this group pointed out the need for regular screening of nutritional status and vitamin levels during the disease, with extra attention paid to recent changes in body weight. The guidelines also recommended screening for dysphagia, as early detection can help in proper intervention and prevention of malnutrition [
70].
The main issue during the writing of this systematic review was the absence of studies investigating the actual problem and prevalence of malnutrition in a group of Parkinson’s disease patients. Most of the data had to be extracted from a variety of studies describing different issues experienced by patients with PD. We also came across a problem when separating the results of only patients with confirmed Parkinson’s Disease. Some studies included larger cohorts with various diseases. We contacted the authors, often with negative results. In the end, studies that lacked necessary information, or in which it was impossible to isolate PD patients from a larger cohort, were excluded from our research.
Currently, only screening tests are available. However, in-depth research is needed to provide adequate, detailed information on the nutritional status of PD patients. Due to the absence of homogeneous studies, it was impossible to conduct results synthesis and meta-analysis.
Our study assessed the prevalence of malnutrition among patients with Parkinson’s Disease by considering 7 questionnaires (MNA, MNA-SF, SGA, PG-SGA, MUST, MEONF-II and SCREEN-II) and BMI. The outcome of this study showed the need for further and more detailed studies on the prevalence of malnutrition in this group of patients. Additionally, it highlighted the lack of adequate assessment tools. Research in this area should be increased, with more care applied to nutritional assessment, as it can determine the quality of life of a patient. A multidisciplinary approach should be applied, and screening for malnutrition should be a routine test, both in the early stages of the disease and throughout the course of the disease, as the prevalence of malnutrition rises with the progression and severity of the disease.




 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}