The Effects of Enteral Nutrition in Critically Ill Patients with COVID-19: A Systematic Review and Meta-Analysis

 ,
, 
 , and
, and 
Abstract
:1. Introduction
1.1. Description of the Intervention
1.2. Implementation of the Intervention
1.3. Why It Is Important to Do This Review
1.4. Aim
2. Method
2.1. Types of Studies
2.2. Types of Participants
2.3. Types of Interventions
2.4. The Inclusion Criteria
2.5. The Exclusion Criteria
2.6. Types of Outcome Measures
- Mortality.
- Length of hospital stay (days).
- Length of ICU stay (days).
- Days on mechanical ventilation (days).
- The Sequential Organ Failure Assessment Score.
2.7. Search Methods for Identification of Studies
2.8. Data Collection and Analysis
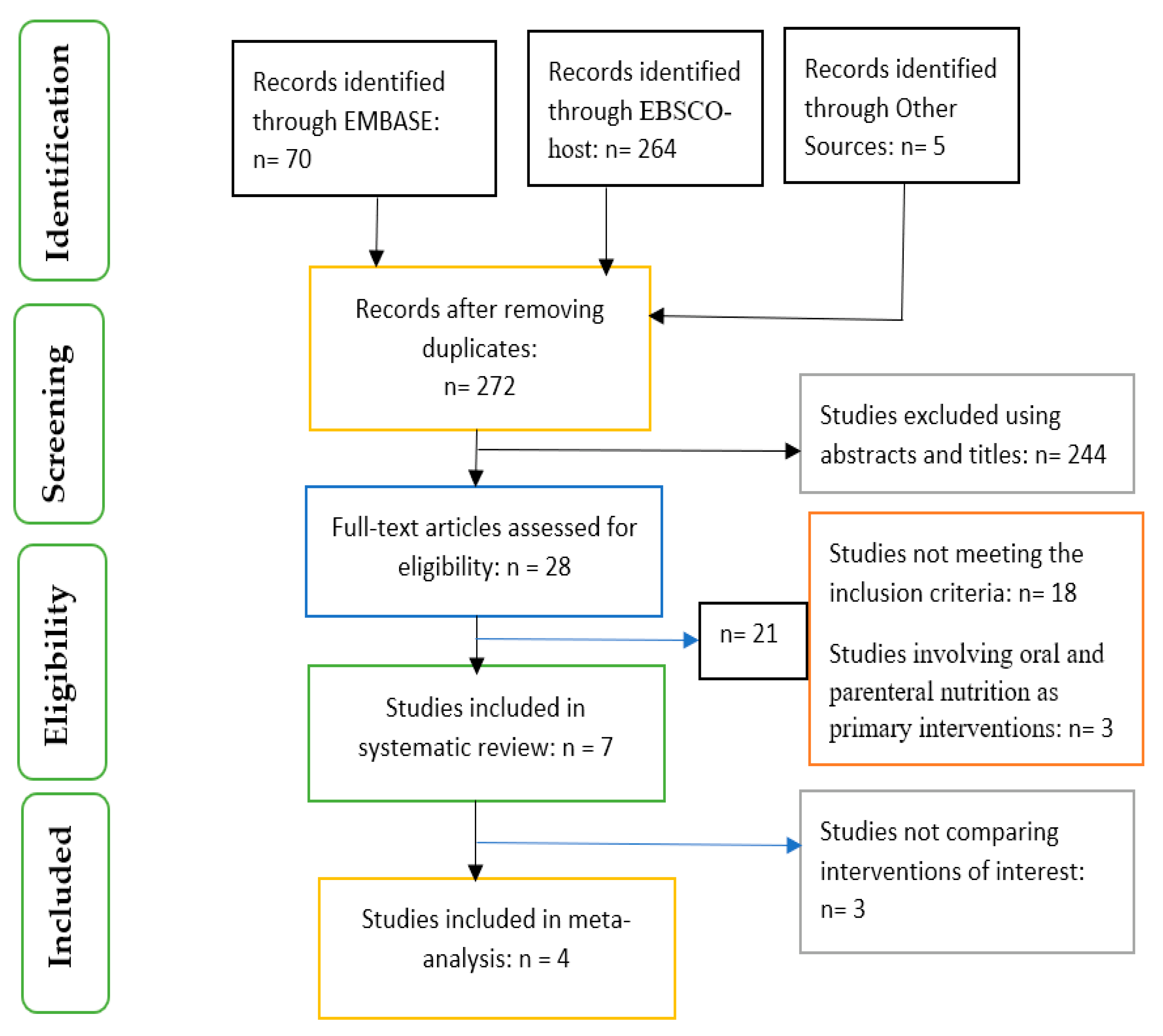
2.8.1. Selection of Studies
2.8.2. Data Extraction and Management
2.9. Data Analysis
3. Results
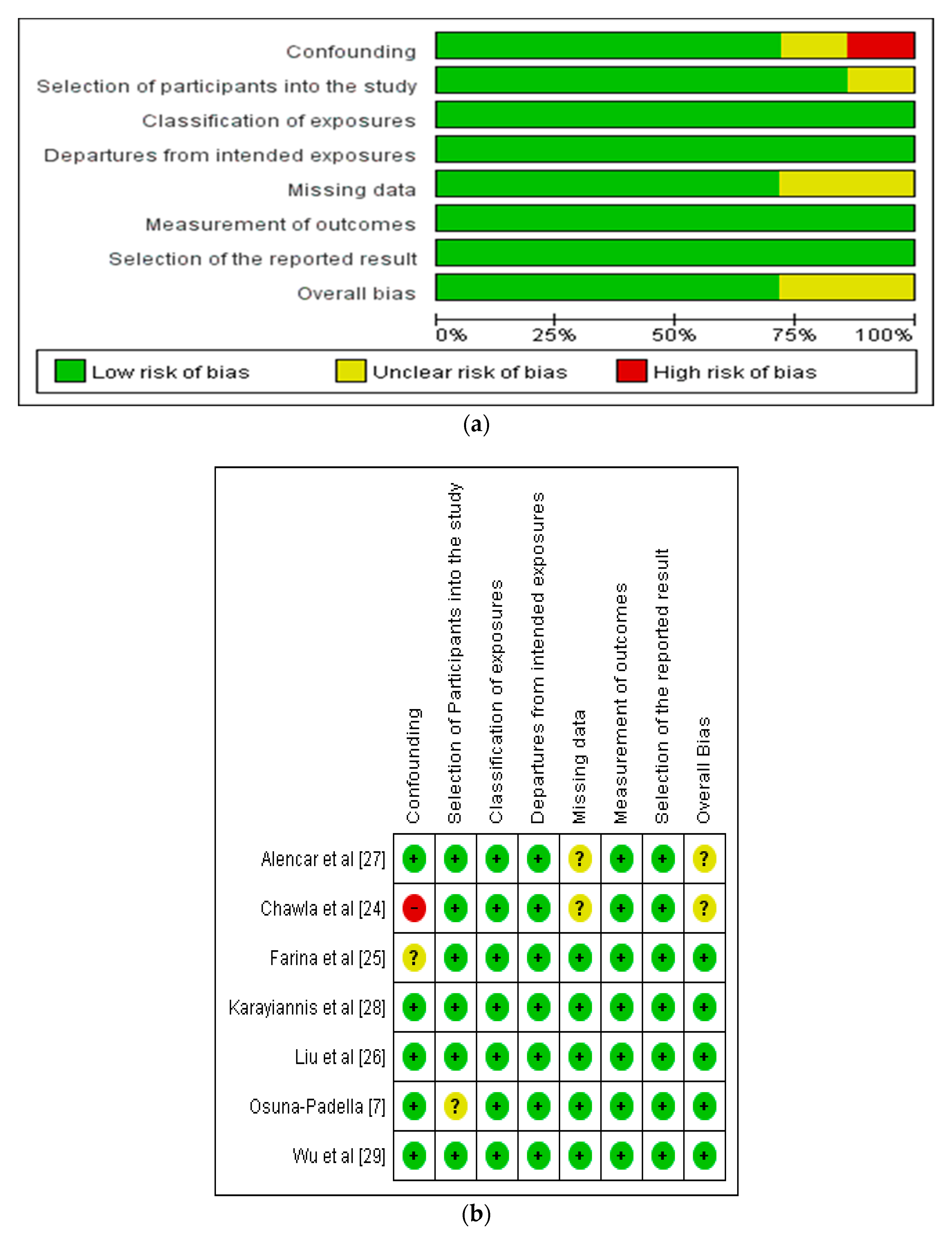
3.1. Assessment of Risk of Bias in Included Studies
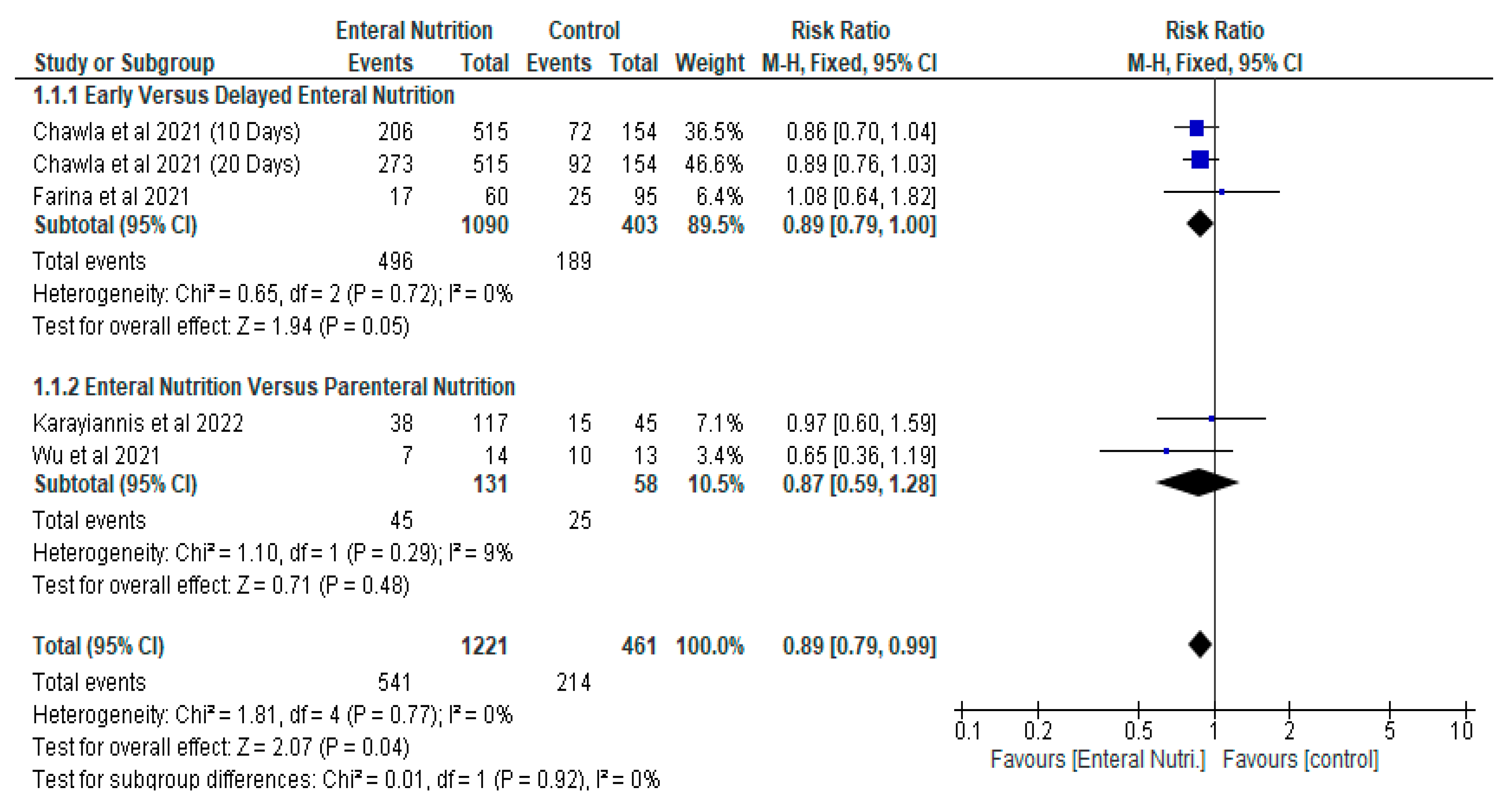
3.2. The Impact of Enteral Nutrition
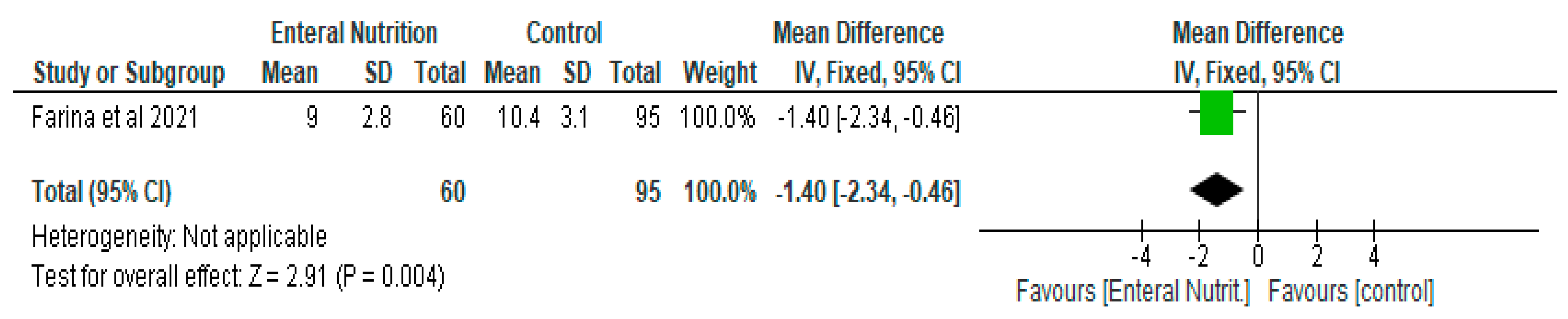
3.2.1. Early Enteral Nutrition versus Delayed Enteral Nutrition
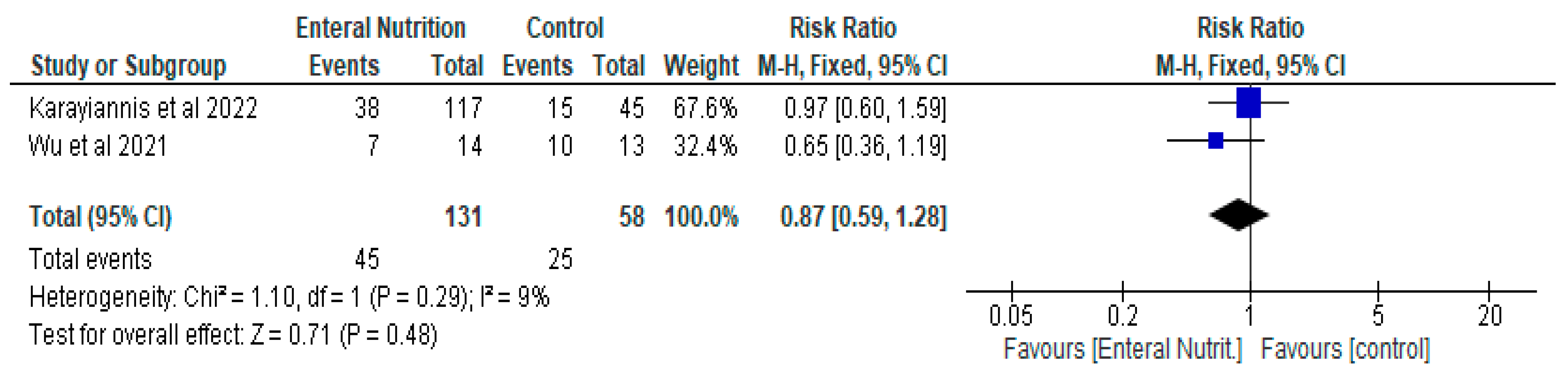
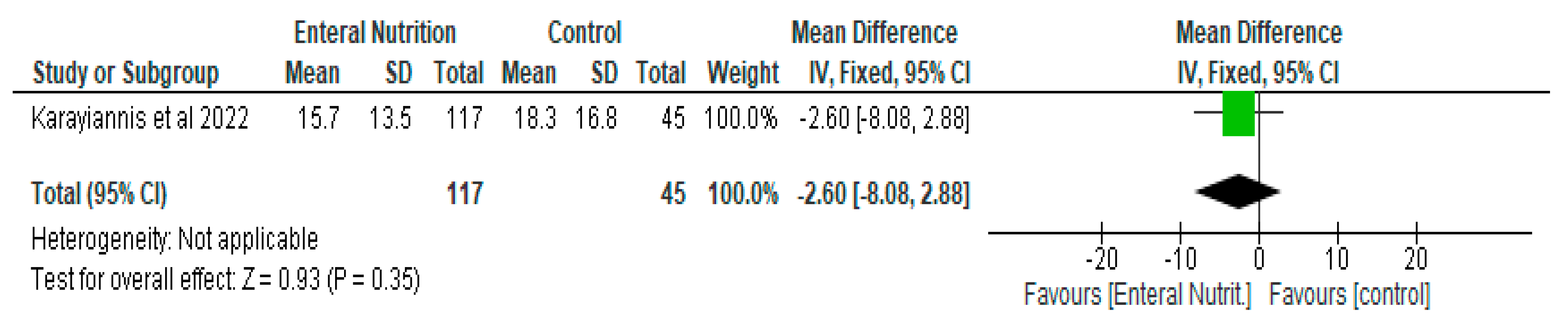
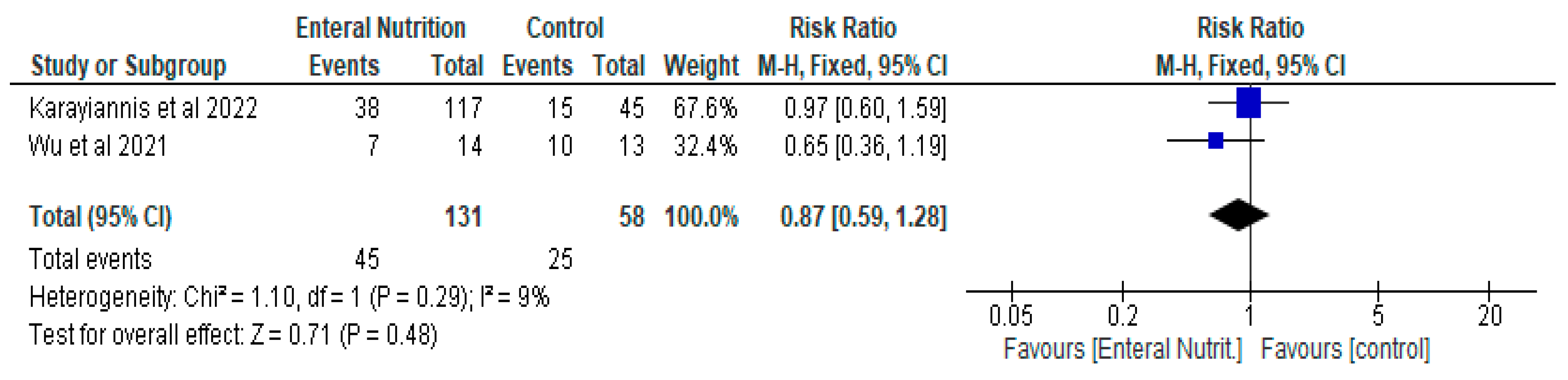
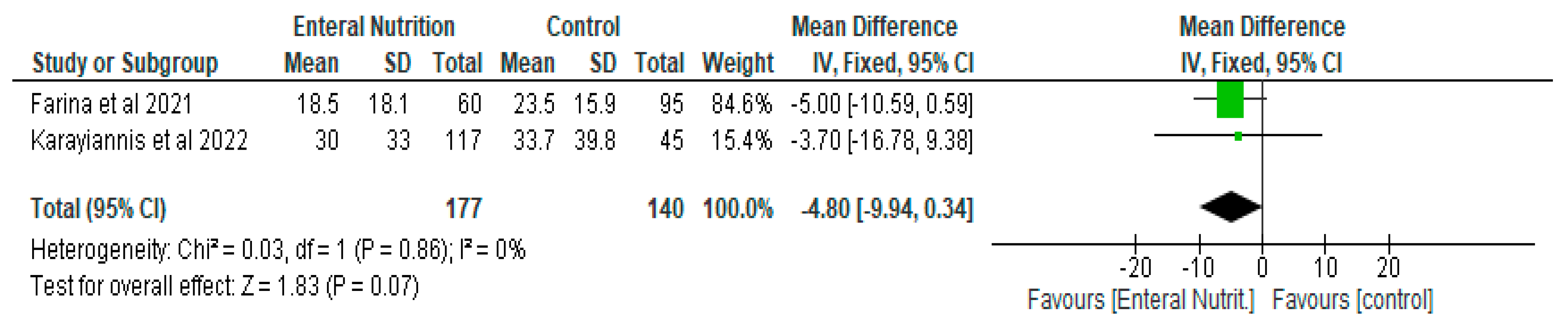
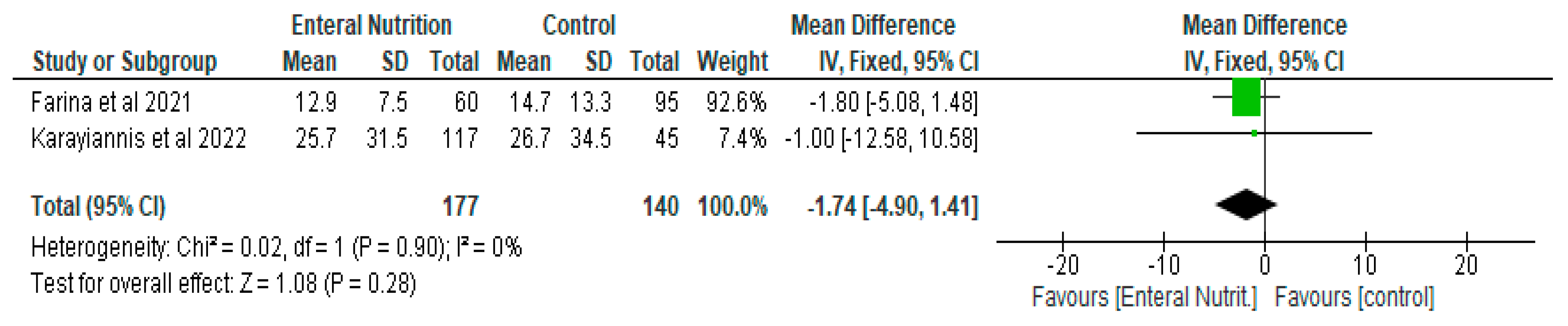
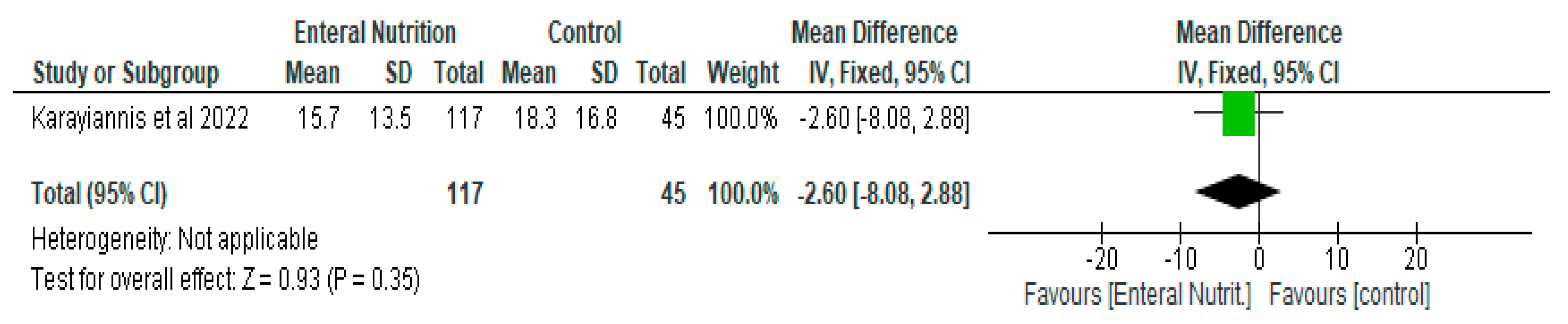
3.2.2. Enteral Nutrition versus Parenteral Nutrition
3.3. Gastrointestinal Intolerance Associated with Enteral Nutrition
4. Discussion
Limitation of the Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ojo, O.; Keaveney, E.; Wang, X.-H.; Feng, P. The Effect of Enteral Tube Feeding on Patients’ Health-Related Quality of Life: A Systematic Review. Nutrients 2019, 11, 1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguila, E.J.T.; Cua, I.H.Y.; Fontanilla, J.A.C.; Yabut, V.L.M.; Causing, M.F.P. Gastrointestinal Manifestations of COVID-19: Impact on Nutrition Practices. Nutrition in Clinical Practice: Official Publication of the American Society for Parenteral and Enteral Nutrition. Nutr. Clin. Pract. 2020, 35, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Ojo, O. Enteral feeding for nutritional support in critically ill patients. Br. J. Nurs. 2017, 26, 666–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thibault, R.; Coëffier, M.; Joly, F.; Bohé, J.; Schneider, S.M.; Déchelotte, P. How the COVID-19 epidemic is challenging our practice in clinical nutrition—Feedback from the field. Eur. J. Clin. Nutr. 2020, 75, 407–416. [Google Scholar] [CrossRef]
- Li, T.; Zhang, Y.; Gong, C.; Wang, J.; Liu, B.; Shi, L.; Duan, J. Prevalence of malnutrition and analysis of related factors in elderly patients with COVID-19 in Wuhan, China. Eur. J. Clin. Nutr. 2020, 74, 871–875. [Google Scholar] [CrossRef] [Green Version]
- Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Krznaric, Z.; Nitzan, D.; Pirlich, M.; Singer, P. ESPEN expert statements and practical guidance for nutritional management of individuals with SARS-CoV-2 infection. Clin. Nutr. 2020, 39, 1631–1638. [Google Scholar] [CrossRef]
- Osuna-Padilla, I.; Rodríguez-Moguel, N.C.; Aguilar-Vargas, A.; Rodríguez-Llamazares, S. Safety and tolerance of enteral nutrition in COVID-19 critically ill patients, a retrospective study. Clin. Nutr. ESPEN 2021, 43, 495–500. [Google Scholar] [CrossRef]
- National Nurses Nutrition Group. Practical Advice and Guidance for Management of Nutritional Support during COVID-19. 2020. Available online: https://www.bapen.org.uk/pdfs/covid-19/covid-nnng-document-updated-12-04-20.pdf (accessed on 23 December 2021).
- Department of Health and Social Care. COVID 19—Resilience of High Protein Enteral Tube Feeds and Giving Sets. 2020. Available online: https://www.bda.uk.com/uploads/assets/ff0396c0-386e-4674-88330c5db70849cd/Communication-brief-Enteral-resilience-arrangements-December-2020.pdf (accessed on 23 December 2021).
- Goyal, H.; Ali, A.; Bansal, P. Percutaneous Endoscopic Gastrostomy Tube Placement in COVID-19 Patients. Front. Nutr. 2021, 8, 603276. [Google Scholar] [CrossRef]
- Ojo, O.; Brooke, J. The Use of Enteral Nutrition in the Management of Stroke. Nutrients 2016, 8, 827. [Google Scholar] [CrossRef] [Green Version]
- Martindale, R.; Patel, J.J.; Taylor, B.; Arabi, Y.M.; Warren, M.; McClave, S.A. Nutrition Therapy in Critically Ill Patients With Coronavirus Disease 2019. JPEN J. Parenter. Enter. Nutr. 2020, 44, 1174–1184. [Google Scholar] [CrossRef]
- Mulherin, D.W.; Walker, R.; Holcombe, B.; Guenter, P. ASPEN Report on Nutrition Support Practice Processes with COVID-19: The First Response. Nutr. Clin. Pract. 2020, 35, 783–791. [Google Scholar] [CrossRef]
- Hu, Y.; Li, X.; Gong, W. Nutritional support for critically ill patients with COVID-19. J. Zhejiang Univ. Med. Sci. 2020, 49, 347–355. [Google Scholar] [CrossRef]
- Delaney, E. Nutritional Care in Relation to COVID-19. Br. J. Nurs. 2020, 29, 1096–1103. [Google Scholar] [CrossRef]
- Holdoway, A. Nutritional management of patients during and after COVID-19 illness. Br. J. Community Nurs. 2020, 25, S6–S10. [Google Scholar] [CrossRef]
- Ferrara, F.; De Rosa, F.; Vitiello, A. The Central Role of Clinical Nutrition in COVID-19 Patients during and after Hospitalization in Intensive Care Unit. SN Compr. Clin. Med. 2020, 2, 1064–1068. [Google Scholar] [CrossRef]
- Suliman, S.; McClave, S.A.; Taylor, B.E.; Patel, J.; Omer, E.; Martindale, R.G. Barriers to nutrition therapy in the critically ill patient with COVID-19. J. Parenter. Enter. Nutr. 2021. [Google Scholar] [CrossRef]
- Minnelli, N.; Gibbs, L.; Larrivee, J.; Sahu, K.K. Challenges of Maintaining Optimal Nutrition Status in COVID-19 Patients in Intensive Care Settings. J. Parenter. Enter. Nutr. 2020, 44, 1439–1446. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2009; p. 31. [Google Scholar]
- The Nordic Cochrane Centre. Review Manager, Version 5.3; The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- Chawla, G.S.; Fazzari, M.J.; Baron, S.W.; Assa, A.; Mohrmann, L.; Chekuri, S.; Katz, J. S1430 Early Enteral Nutrition Reduces In-Hospital Mortality of Critically Ill COVID-19 Patients. Am. J. Gastroenterol. 2021, 116, S657. [Google Scholar] [CrossRef]
- Farina, N.; Nordbeck, S.; Rdn, M.M.; Cordwin, L.; Blair, F.; Cherry-Bukowiec, J.; Kraft, M.D.; Pleva, M.R.; Raymond, E. Early Enteral Nutrition in Mechanically Ventilated Patients with COVID-19 Infection. Nutr. Clin. Pract. 2021, 36, 440–448. [Google Scholar] [CrossRef]
- Liu, R.; Paz, M.; Siraj, L.; Boyd, T.; Salamone, S.; Lite, T.-L.V.; Leung, K.M.; Chirinos, J.D.; Shang, H.H.; Townsend, M.J.; et al. Feeding intolerance in critically ill patients with COVID-19. Clin. Nutr. 2021. [Google Scholar] [CrossRef]
- de Alencar, E.S.; Muniz, L.S.d.S.; Holanda, J.L.G.; Oliveira, B.D.D.; de Carvalho, M.C.F.; Leitão, A.M.M.; Cavalcante, M.I.d.A.; de Oliveira, R.C.P.; da Silva, C.A.B.; Carioca, A.A.F. Enteral nutritional support for patients hospitalized with COVID-19: Results from the first wave in a public hospital. Nutrition 2021, 94, 111512. [Google Scholar] [CrossRef]
- Karayiannis, D.; Kakavas, S.; Sarri, A.; Giannopoulou, V.; Liakopoulou, C.; Jahaj, E.; Kanavou, A.; Pitsolis, T.; Malachias, S.; Adamos, G.; et al. Does Route of Full Feeding Affect Outcome among Ventilated Critically Ill COVID-19 Patients: A Prospective Observational Study. Nutrients 2021, 14, 153. [Google Scholar] [CrossRef]
- Wu, S.; Lou, J.; Xu, P.; Luo, R.; Li, L. Early enteral nutrition improves the outcome of critically ill patients with COVID-19: A retrospective study. Asia Pac. J. Clin. Nutr. 2021, 30, 192–198. [Google Scholar]
- Bristol.ac.uk. Preliminary Tool for Risk of Bias in Exposure Studies. 2021. Available online: https://www.bristol.ac.uk/media-library/sites/social-community-medicine/images/centres/cresyda/Risk_of_bias_preliminary_for_exposures_template_Jul2017.pdf (accessed on 7 January 2021).
- Tian, F.; Heighes, P.T.; Allingstrup, M.J.; Doig, G.S. Early Enteral Nutrition Provided within 24 hours of ICU Admission. Crit. Care Med. 2018, 46, 1049–1056. [Google Scholar] [CrossRef]
- Yu, A.; Xie, Y.; Zhong, M.; Wang, F.; Huang, H.; Nie, L.; Liu, X.; Xiao, M.; Zhu, H. Comparison of the Initiation Time of Enteral Nutrition for Critically Ill Patients: At Admission vs. 24 to 48 Hours after Admission. Emerg. Med. Int. 2021, 2021, 3047732. [Google Scholar] [CrossRef]
- Vila, B.G.; Grau, T. Early enteral nutrition in the critically-ill patient. Nutr. Hosp. 2005, 20, 93–100. [Google Scholar]
- Thomas, S.; Alexander, C.; Cassady, B.A. Nutrition risk prevalence and nutrition care recommendations for hospitalized and critically-ill patients with COVID-19. Clin. Nutr. ESPEN 2021, 44, 38–49. [Google Scholar] [CrossRef]
- Patel, J.J.; Martindale, R.G.; McClave, S.A. Relevant Nutrition Therapy in COVID-19 and the Constraints on Its Delivery by a Unique Disease Process. Nutr. Clin. Pract. 2020, 35, 792–799. [Google Scholar] [CrossRef]
- Seres, D.S.; Valcarcel, M.; Guillaume, A. Advantages of enteral nutrition over parenteral nutrition. Ther. Adv. Gastroenterol. 2012, 6, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.J.; Kozeniecki, M.; Peppard, W.J.; Peppard, S.R.; Zellner-Jones, S.; Graf, J.; Szabo, A.; Heyland, D.K. Phase 3 Pilot Randomized Controlled Trial Comparing Early Trophic Enteral Nutrition with “No Enteral Nutrition” in Mechanically Ventilated Patients with Septic Shock. J. Parenter. Enter. Nutr. 2019, 44, 866–873. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient/Population | Intervention | Comparator | Combining Search Terms |
|---|---|---|---|
| Patients with Corona-virus | Enteral nutrition | Control | |
| Patients with corona virus OR COVID-19 OR COVID-19 testing OR SARS-CoV-2 | Nutrition, Enteral OR Enteral feeding OR Feeding, Enteral OR Tube feeding OR Feeding, Tube OR Gastric feeding tubes OR Feeding tube, Gastric OR Feeding tubes, Gastric OR Gastric feeding tube OR Tube, Gastric feeding OR Tubes, Gastric feeding | Column 1 AND Column 2 |
| Citation/Country of Study | Type of Study | Sample Size | Mean Age (Years) | Aim | Interventions | Results |
|---|---|---|---|---|---|---|
| Alencar et al. [27] Brazil | Retrospective study | n = 112 | <60 (n = 24) ≥60 (n = 88) | To evaluate the association between enteral nutrition support and clinical outcomes in patients with COVID-19 | Enteral nutrition | The authors found an association between deficit in protein and energy supply and mortality and recommended that nutrition support should be promoted in such conditions. |
| Chawla et al. [24] USA | Retrospective study | n = 515 | Not Available | To examine if early enteral nutrition reduced morbidity and mortality in patients with COVID-19 | Early enteral nutrition versus delayed enteral nutrition | There was a lower risk of in-hospital death in the Early enteral nutrition group compared with the Delayed enteral nutrition group. The times to extubate and discharge patients from the hospital were not associated with early enteral nutrition administration. |
| Farina et al. [25] USA | Retrospective study | n = 155 | 60.3 ± 13.8 | To assess the effect of early enteral nutrition on outcomes in mechanically ventilated patients with COVID-19 | Early enteral nutrition versus delayed enteral nutrition | The commencement of early enteral nutrition within 24 h did not improve the outcomes in mechanically ventilated patients with COVID-19 |
| Karayiannis et al. [28] Greece | Prospective observational study | n = 162 | EN group (63.2 ± 11.9) PN group (62.7 ± 10.7) | To describe the feeding practices of intubated patients with COVID-19 and their association with mortality, length of hospital stay and mechanical ventilation. | Enteral nutrition compared with parenteral nutrition. | During the second week of ICU hospitalization, enteral feeding may be associated with a shorter duration of hospitalization and use of mechanical ventilation support in COVID-19 patients who are critically ill and intubated. |
| Liu et al. [26] USA | Retrospective study | Received enteral nutrition (n = 323) Did not receive enteral nutrition (n = 79) | 59.6 ± 14.9 among 323 patients on enteral nutrition | To evaluate the prevalence and clinical outcomes of feeding intolerance among COVID-19 patients | Enteral nutrition versus ‘No enteral nutrition’ | There were 56% incident cases of feeding intolerance among the 323 patients on enteral nutrition. The length of intubation, ICU admission and mortality were (16 versus 2 days), (18 versus 2 days) and (84 versus 18) among patients that received enteral tube feeding compared with no tube feeds, respectively. |
| Osuna-Padella et al. [7] Mexico | Retrospective study | (n = 52) | 55.7 ± 14.3 | To examine the incidence of gastrointestinal intolerance associated with enteral nutrition | Enteral nutrition during the first week of administration | Enteral nutrition was well tolerated in patients with COVID-19 within the first week of intubation and who are on mechanical ventilation. |
| Wu et al. [29] China | Retrospective study | enteral nutrition (n = 14) parental nutrition(n = 13) | 74.9 ± 10.5 | To evaluate the nutritional status of critically ill patients with COVID-19 and to determine, which route of nutrition support is advantageous | Enteral nutrition versus parenteral nutrition | The incidence of nutritional risk in critically ill patients with COVID-19 was very high. Early EN may be beneficial to patient outcomes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojo, O.; Ojo, O.O.; Feng, Q.; Boateng, J.; Wang, X.; Brooke, J.; Adegboye, A.R.A. The Effects of Enteral Nutrition in Critically Ill Patients with COVID-19: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 1120. https://doi.org/10.3390/nu14051120
Ojo O, Ojo OO, Feng Q, Boateng J, Wang X, Brooke J, Adegboye ARA. The Effects of Enteral Nutrition in Critically Ill Patients with COVID-19: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(5):1120. https://doi.org/10.3390/nu14051120
Chicago/Turabian StyleOjo, Omorogieva, Osarhumwese Osaretin Ojo, Qianqian Feng, Joshua Boateng, Xiaohua Wang, Joanne Brooke, and Amanda Rodrigues Amorim Adegboye. 2022. "The Effects of Enteral Nutrition in Critically Ill Patients with COVID-19: A Systematic Review and Meta-Analysis" Nutrients 14, no. 5: 1120. https://doi.org/10.3390/nu14051120
APA StyleOjo, O., Ojo, O. O., Feng, Q., Boateng, J., Wang, X., Brooke, J., & Adegboye, A. R. A. (2022). The Effects of Enteral Nutrition in Critically Ill Patients with COVID-19: A Systematic Review and Meta-Analysis. Nutrients, 14(5), 1120. https://doi.org/10.3390/nu14051120