
What Promotes Acute Kidney Injury in Patients with Myocardial Infarction and Multivessel Coronary Artery Disease—Contrast Media, Hydration Status or Something Else?


Abstract
:1. Introduction
2. Acute Kidney Injury in Patients with Myocardial Infarction
2.1. Definition, Epidemiology and Impact on Prognosis
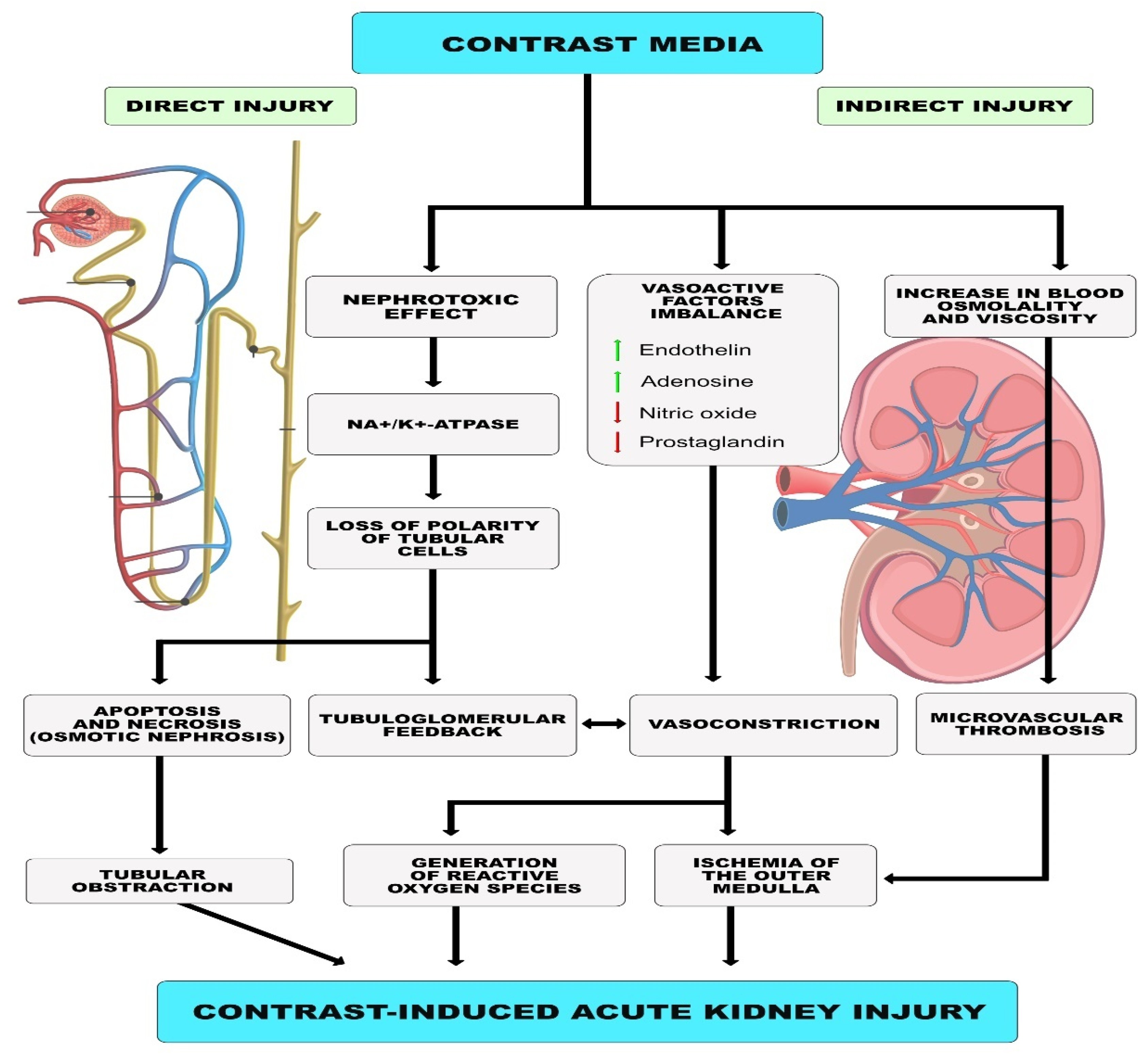
2.2. Etiology, Pathogenesis
2.3. Role of Contrast Agent
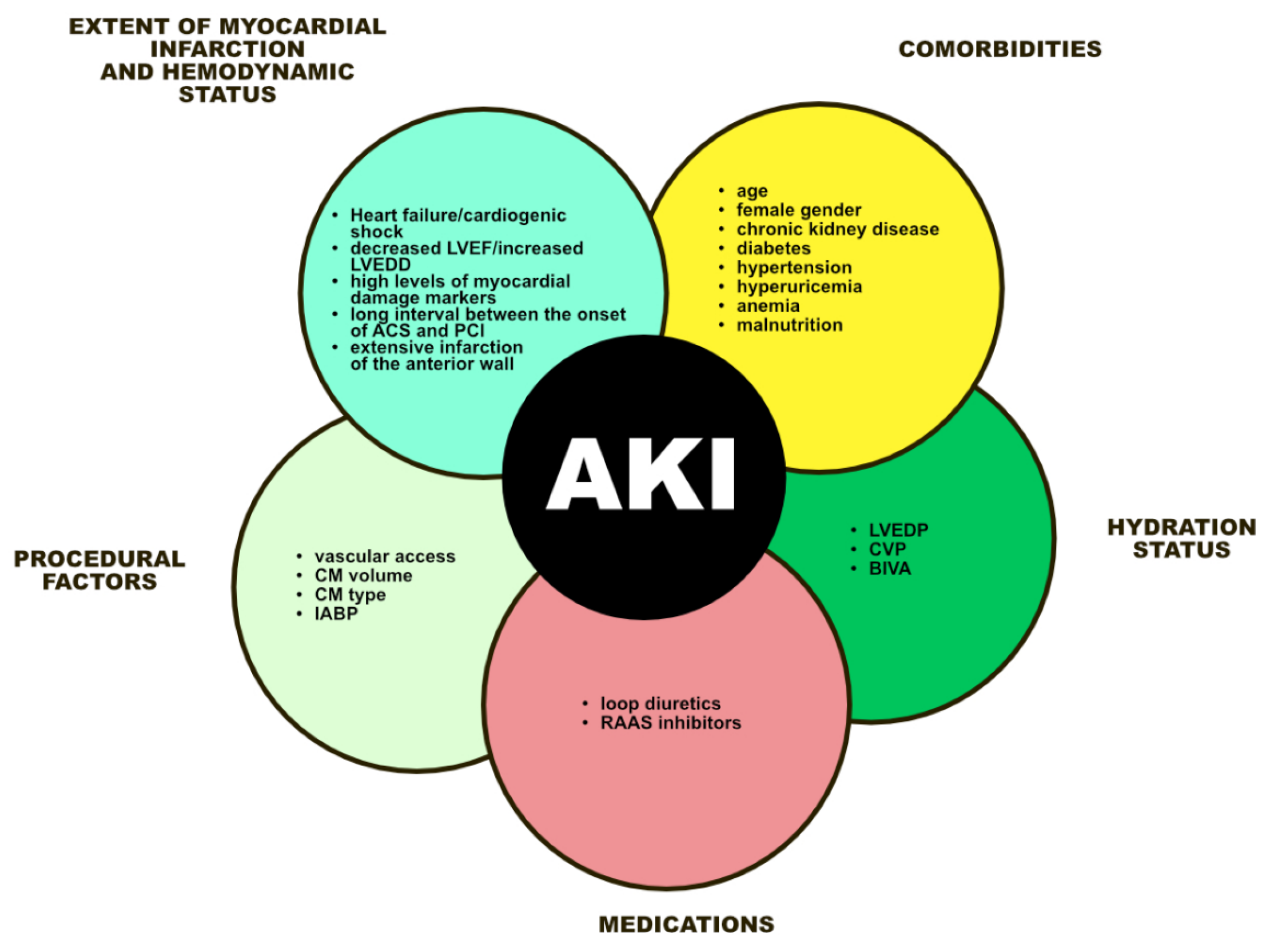
3. Risk Factors for Acute Kidney Injury in Patients with Myocardial Infarction
3.1. Severity of Infarction and Heart Failure
3.2. Comorbidities and Others Factors
3.3. Malnutrition
3.4. Hydration Status
3.5. Medications
3.6. Vascular Access
4. New Markers of Kidney Damage
5. Ways of Prevention
5.1. Hydration
5.2. Medications
5.3. Hemodialysis/Hemofiltration
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sorajja, P.; Gersh, B.J.; Cox, D.A.; McLaughlin, M.G.; Zimetbaum, P.; Costantini, C.; Stuckey, T.; Tcheng, J.E.; Mehran, R.; Lansky, A.J.; et al. Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur. Heart J. 2007, 28, 1709–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Schaaf, R.J.; Timmer, J.R.; Ottervanger, J.P.; Hoorntje, J.C.A.; De Boer, M.-J.; Suryapranata, H.; Zijlstra, F.; Dambrink, J.H. Long-term impact of multivessel disease on cause-specific mortality after ST elevation myocardial infarction treated with reperfusion therapy. Heart 2006, 92, 1760–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.R.; Wood, D.A.; Storey, R.F.; Mehran, R.; Bainey, K.R.; Nguyen, H.; Meeks, B.; Di Pasquale, G.; López-Sendón, J.; Faxon, D.P.; et al. Complete revascularization with multivessel PCI for myocardial infarction. N. Engl. J. Med. 2019, 381, 1411–1421. [Google Scholar] [CrossRef] [Green Version]
- Atti, V.; Gwon, Y.; Narayanan, M.A.; Garcia, S.; Sandoval, Y.; Brilakis, E.S.; Basir, M.B.; Turagam, M.K.; Khandelwal, A.; Mena-Hurtado, C.; et al. Multivessel Versus Culprit-Only Revascularization in STEMI and Multivessel Coronary Artery Disease: Meta-Analysis of Randomized Trials. JACC Cardiovasc. Interv. 2020, 13, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Engstrøm, T.; Kelbæk, H.; Helqvist, S.; Høfsten, D.E.; Kløvgaard, L.; Holmvang, L.; Jørgensen, E.; Pedersen, F.; Saunamäki, K.; Clemmensen, P.; et al. Complete revascularisation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3—PRIMULTI): An open-label, randomised controlled trial. Lancet 2015, 386, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Smits, P.C.; Abdel-Wahab, M.; Neumann, F.J.; Boxma-de Klerk, B.M.; Lunde, K.; Schotborgh, C.E.; Piroth, Z.; Horak, D.; Wlodarczak, A.; Ong, P.J.; et al. Compare-Acute Investigators. Fractional Flow Reserve-Guided Multivessel Angioplasty in Myocardial Infarction. N. Engl. J. Med. 2017, 376, 1234–1244. [Google Scholar] [CrossRef]
- Rathod, K.S.; Koganti, S.; Jain, A.K.; Astroulakis, Z.; Lim, P.; Rakhit, R.; Kalra, S.S.; Dalby, M.C.; O’Mahony, C.; Malik, I.S.; et al. Complete Versus Culprit-Only Lesion Intervention in Patients With Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2018, 72, 1989–1999. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Qarawani, D.; Nahir, M.; Abboud, M.; Hazanov, Y.; Hasin, Y. Culprit only versus complete coronary revascularization during primary PCI. Int. J. Cardiol. 2008, 123, 288–292. [Google Scholar] [CrossRef]
- Stevens, P.E.; Levin, A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellomo, R.; Ronco, C.; Kellum, J.; Mehta, R.L.; Palevsky, P. Acute Dialysis Quality Initiative workgroup. Acute renal failuredefinition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalikias, G.; Serif, L.; Kikas, P.; Thomaidis, A.; Stakos, D.; Makrygiannis, D.; Chatzikyriakou, S.; Papoulidis, N.; Voudris, V.; Lantzouraki, A.; et al. Long-term impact of acute kidney injury on prognosis in patients with acute myocardial infarction. Int. J. Cardiol. 2019, 283, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Dar, M.H.; Khan, A.; Iltaf, K.; Khan, S.; Falah, S.F. Frequency of acute kidney injury and its short-term effects after acute myocardial infarction. J. Pak. Med. Assoc. 2017, 67, 1693–1697. [Google Scholar]
- Schmucker, J.; Fach, A.; Becker, M.; Seide, S.; Bünger, S.; Zabrocki, R.; Fiehn, E.; Würmann-Busch, B.; Pohlabeln, H.; Günther, K.; et al. Predictors of acute kidney injury in patients admitted with ST-elevation myocardial infarction-results from the Bremen STEMI-Registry. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 710–722. [Google Scholar] [CrossRef]
- Wang, C.; Pei, Y.Y.; Ma, Y.H.; Ma, X.L.; Liu, Z.W.; Zhu, J.H.; Li, C.S. Risk factors for acute kidney injury in patients with acute myocardial infarction. Chin. Med. J. 2019, 132, 1660–1665. [Google Scholar] [CrossRef]
- Sun, Y.B.; Liu, B.C.; Zou, Y.; Pan, J.R.; Tao, Y.; Yang, M. Risk factors of acute kidney injury after acute myocardial infarction. Ren. Fail. 2016, 38, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- Tsai, T.T.; Patel, U.D.; Chang, T.I.; Kennedy, K.F.; Masoudi, F.A.; Matheny, M.E.; Kosiborod, M.; Amin, A.P.; Messenger, J.C.; Rumsfeld, J.S.; et al. Contemporary incidence; predictors; and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: Insights from the NCDR Cath-PCI registry. JACC Cardiovasc. Interv. 2014, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Marenzi, G.; Cabiati, A.; Bertoli, S.V.; Assanelli, E.; Marana, I.; De Metrio, M.; Rubino, M.; Moltrasio, M.; Grazi, M.; Campodonico, J.; et al. Incidence and relevance of acute kidney injury in patients hospitalized with acute coronary syndromes. Am. J. Cardiol. 2013, 111, 816–822. [Google Scholar] [CrossRef]
- Mezhonov, E.M.; Vialkina, I.A.; Vakulchik, K.A.; Shalaev, S.V. Acute kidney injury in patients with ST-segment elevation acute myocardial infarction: Predictors and outcomes. Saudi J. Kidney Dis. Transplant. 2021, 32, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.B.; Tao, Y.; Yang, M. Assessing the influence of acute kidney injury on the mortality in patients with acute myocardial infarction: A clinical trail. Ren. Fail. 2018, 40, 75–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanic, V.; Suran, D.; Vollrath, M.; Tapajner, A.; Kompara, G. Influence of minor deterioration of renal function after PCI on outcome in patients with ST-elevation myocardial infarction. J. Interv. Cardiol. 2017, 30, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Shacham, Y.; Steinvil, A.; Arbel, Y. Acute kidney injury among ST elevation myocardial infarction patients treated by primary percutaneous coronary intervention: A multifactorial entity. J. Nephrol. 2016, 29, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.F.; Liu, D.D.; Zhou, Y.; Lou, J.Z. Acute Kidney Injury in Patients with Acute Coronary Syndrome after Percutaneous Coronary Intervention: Pathophysiologies; Risk Factors; and Preventive Measures. Cardiology 2021, 146, 678–689. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Cosentino, N.; Bartorelli, A.L. Acute kidney injury in patients with acute coronary syndromes. Heart 2015, 101, 1778–1785. [Google Scholar] [CrossRef]
- Grisk, O. The sympathetic nervous system in acute kidney injury. Acta Physiol. 2020, 228, e13404. [Google Scholar] [CrossRef]
- Brewster, U.C.; Perazella, M.A. The renin-angiotensin-aldosterone system and the kidney: Effects on kidney disease. Am. J. Med. 2004, 116, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Anzai, A.; Anzai, T.; Naito, K.; Kaneko, H.; Mano, Y.; Jo, Y.; Nagatomo, Y.; Maekawa, Y.; Kawamura, A.; Yoshikawa, T.; et al. Prognostic significance of acute kidney injury after reperfused ST-elevation myocardial infarction: Synergistic acceleration of renal dysfunction and left ventricular remodeling. J. Card. Fail. 2010, 16, 381–389. [Google Scholar] [CrossRef]
- Raso Vasquez, A.O.; Kertai, M.D.; Fontes, M.L. Postoperative thrombocytopenia: Why you should consider antiplatelet therapy? Curr. Opin. Anaesthesiol. 2018, 31, 61–66. [Google Scholar] [CrossRef]
- Baydar, O.; Kilic, A. Acute hyperglycemia and contrast-induced nephropathy in patients with non-ST elevation myocardial infarction. Cardiovasc. Endocrinol. Metab. 2020, 9, 24–29. [Google Scholar] [CrossRef]
- Gohbara, M.; Hayakawa, A.; Akazawa, Y.; Furihata, S.; Kondo, A.; Fukushima, Y.; Tomari, S.; Endo, T.; Kimura, K.; Tamura, K. Association Between Acidosis Soon After Reperfusion and Contrast-Induced Nephropathy in Patients With a First-Time ST-Segment Elevation Myocardial Infarction. J. Am. Heart Assoc. 2017, 6, e006380. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Dangas, G.D.; Weisbord, S.D. Contrast-Associated Acute Kidney Injury. N. Engl. J. Med. 2019, 380, 2146–2155. [Google Scholar] [CrossRef] [PubMed]
- Chalikias, G.; Drosos, I.; Tziakas, D.N. Contrast-Induced Acute Kidney Injury: An Update. Cardiovasc. Drugs Ther. 2016, 30, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Orlacchio, A.; Guastoni, C.; Beretta, G.D.; Cosmai, L.; Galluzzo, M.; Gori, S.; Grassedonio, E.; Incorvaia, L.; Marcantoni, C.; Netti, G.S.; et al. SIRM-SIN-AIOM: Appropriateness criteria for evaluation and prevention of renal damage in the patient undergoing contrast medium examinations-consensus statements from Italian College of Radiology (SIRM). Italian College of Nephrology (SIN) and Italian Association of Medical Oncology (AIOM). Radiol. Med. 2022, 127, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Assanelli, E.; Campodonico, J.; Lauri, G.; Marana, I.; De Metrio, M.; Moltrasio, M.; Grazi, M.; Rubino, M.; Veglia, F.; et al. Contrast volume during primary percutaneous coronary intervention and subsequent contrast-induced nephropathy and mortality. Ann. Intern. Med. 2009, 150, 170–177. [Google Scholar] [CrossRef]
- Narula, A.; Mehran, R.; Weisz, G.; Dangas, G.D.; Yu, J.; Généreux, P.; Nikolsky, E.; Brener, S.J.; Witzenbichler, B.; Guagliumi, G.; et al. Contrast-induced acute kidney injury after primary percutaneous coronary intervention: Results from the HORIZONS-AMI substudy. Eur. Heart J. 2014, 35, 1533–1540. [Google Scholar] [CrossRef] [Green Version]
- Barbieri, L.; Verdoia, M.; Marino, P.; Suryapranata, H.; De Luca, G.; Novara Atherosclerosis Study Group. Contrast volume to creatinine clearance ratio for the prediction of contrast-induced nephropathy in patients undergoing coronary angiography or percutaneous intervention. Eur. J. Prev. Cardiol. 2016, 23, 931–937. [Google Scholar] [CrossRef]
- Caspi, O.; Habib, M.; Cohen, Y.; Kerner, A.; Roguin, A.; Abergel, E.; Boulos, M.; Kapeliovich, M.R.; Beyar, R.; Nikolsky, E.; et al. Acute Kidney Injury After Primary Angioplasty: Is Contrast-Induced Nephropathy the Culprit? J. Am. Heart Assoc. 2017, 6, e005715. [Google Scholar] [CrossRef] [PubMed]
- Sudarski, D.; Naami, R.; Shehadeh, F.; Elias, A.; Kerner, A.; Aronson, D. Risk of Worsening Renal Function Following Repeated Exposures to Contrast Media During Percutaneous Coronary Interventions. J. Am. Heart Assoc. 2021, 10, e021473. [Google Scholar] [CrossRef]
- Lemor, A.; Basir, M.B.; Patel, K.; Kolski, B.; Kaki, A.; Kapur, N.K.; Riley, R.; Finley, J.; Goldsweig, A.; Aronow, H.D.; et al. Multivessel Versus Culprit-Vessel Percutaneous Coronary Intervention in Cardiogenic Shock. JACC Cardiovasc. Interv. 2020, 13, 1171–1178. [Google Scholar] [CrossRef]
- Chatterjee, S.; Kundu, A.; Mukherjee, D.; Sardar, P.; Mehran, R.; Bashir, R.; Giri, J.; Abbott, J.D. Risk of contrast-induced acute kidney injury in ST-elevation myocardial infarction patients undergoing multi-vessel intervention-meta-analysis of randomized trials and risk prediction modeling study using observational data. Catheter. Cardiovasc. Interv. 2017, 90, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Mukete, B.N.; Riehl, R.A.; Alonso, A.; Samson, R.; Jaiswal, A.; Le Jemtel, T.H. Multivessel Revascularization Does Not Increase Contrast-Induced Acute Kidney Injury Incidence in Acute Myocardial Infarction: A Meta-Analysis. Am. J. Cardiovasc. Drugs 2016, 16, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Azzalini, L.; Candilio, L.; McCullough, P.A.; Colombo, A. Current Risk of Contrast-Induced Acute Kidney Injury After Coronary Angiography and Intervention: A Reappraisal of the Literature. Can. J. Cardiol. 2017, 33, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.S.; McDonald, R.J.; Comin, J.; Williamson, E.E.; Katzberg, R.W.; Murad, M.H.; Kallmes, D.F. Frequency of acute kidney injury following intravenous contrast medium administration: A systematic review and meta-analysis. Radiology 2013, 267, 119–128. [Google Scholar] [CrossRef]
- McDonald, R.J.; McDonald, J.S.; Carter, R.E.; Hartman, R.P.; Katzberg, R.W.; Kallmes, D.F.; Williamson, E.E. Intravenous contrast material exposure is not an independent risk factor for dialysis or mortality. Radiology 2014, 273, 714–725. [Google Scholar] [CrossRef]
- Wilhelm-Leen, E.; Montez-Rath, M.E.; Chertow, G. Estimating the Risk of Radiocontrast-Associated Nephropathy. J. Am. Soc. Nephrol. 2017, 28, 653–659. [Google Scholar] [CrossRef] [Green Version]
- Newhouse, J.H.; Kho, D.; Rao, Q.A.; Starren, J. Frequency of serum creatinine changes in the absence of iodinated contrast material: Implications for studies of contrast nephrotoxicity. AJR Am. J. Roentgenol. 2008, 191, 376–382. [Google Scholar] [CrossRef]
- Neves, D.; Belo, A.; Damásio, A.F.; Carvalho, J.; Santos, A.R.; Piçarra, B.; Aguiar, J.; Investigators of the Portuguese Registry on Acute Coronary Syndromes (ProACS). Acute kidney injury in acute coronary syndromes-An important multifactorial consequence. Rev. Port. Cardiol. 2016, 35, 415–421. [Google Scholar] [CrossRef]
- Queiroz, R.E.; de Oliveira, L.S.; de Albuquerque, C.A.; Santana Cde, A.; Brasil, P.M.; Carneiro, L.L.; Libório, A.B. Acute kidney injury risk in patients with ST-segment elevation myocardial infarction at presentation to the ED. Am. J. Emerg. Med. 2012, 30, 1921–1927. [Google Scholar] [CrossRef] [PubMed]
- Di Lullo, L.; Bellasi, A.; Barbera, V.; Russo, D.; Russo, L.; Di Iorio, B.; Cozzolino, M.; Ronco, C. Pathophysiology of the cardio-renal syndromes types 1-5: An uptodate. Indian Heart J. 2017, 69, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Mandurino-Mirizzi, A.; Kajana, V.; Cornara, S.; Somaschini, A.; Demarchi, A.; Galazzi, M.; Crimi, G.; Ferlini, M.; Camporotondo, R.; Gnecchi, M.; et al. Elevated serum uric acid is a predictor of contrast associated acute kidney injury in patient with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2140–2143. [Google Scholar] [CrossRef] [PubMed]
- Shacham, Y.; Gal-Oz, A.; Leshem-Rubinow, E.; Arbel, Y.; Flint, N.; Keren, G.; Roth, A.; Steinvil, A. Association of admission hemoglobin levels and acute kidney injury among myocardial infarction patients treated with primary percutaneous intervention. Can. J. Cardiol. 2015, 31, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Li, D.; Jia, Y.; Li, F.; Jiang, Y.; Zhang, Q.; Gao, Y.; Liao, X.; Zeng, R.; Wan, Z. Nutritional Risk Screening 2002 was associated with acute kidney injury and mortality in patients with acute coronary syndrome: Insight from the REACP study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1121–1128. [Google Scholar] [CrossRef]
- Kurtul, A.; Gok, M.; Esenboga, K. Prognostic Nutritional Index Predicts Contrast-Associated Acute Kidney Injury in Patients with ST-Segment Elevation Myocardial Infarction. Acta Cardiol Sin. 2021, 37, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Murat, S.N.; Kurtul, A.; Yarlioglues, M. Impact of Serum Albumin Levels on Contrast-Induced Acute Kidney Injury in Patients With Acute Coronary Syndromes Treated With Percutaneous Coronary Intervention. Angiology 2015, 66, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Wang, P.; Li, W.; Jiang, L.; Wang, M.; Zhu, B.; Xi, X. Prognostic significance of malnutrition risk in elderly patients with acute kidney injury in the intensive care unit. BMC Nephrol. 2022, 23, 335. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Ruocco, G.; Ronco, C.; McCullough, P.A. Loop diuretics in acute heart failure: Beyond the decongestive relief for the kidney. Crit. Care 2015, 19, 296. [Google Scholar] [CrossRef] [Green Version]
- Andò, G.; Costa, F.; Trio, O.; Oreto, G.; Valgimigli, M. Impact of vascular access on acute kidney injury after percutaneous coronary intervention. Cardiovasc. Revasc. Med. 2016, 17, 333–338. [Google Scholar] [CrossRef]
- Andò, G.; Gragnano, F.; Calabrò, P.; Valgimigli, M. Radial vs femoral access for the prevention of acute kidney injury (AKI) after coronary angiography or intervention: A systematic review and meta-analysis. Catheter. Cardiovasc. Interv. 2018, 92, E518–E526. [Google Scholar] [CrossRef]
- Ohno, Y.; Maekawa, Y.; Miyata, H.; Inoue, S.; Ishikawa, S.; Sueyoshi, K.; Noma, S.; Kawamura, A.; Kohsaka, S.; Fukuda, K. Impact of periprocedural bleeding on incidence of contrast-induced acute kidney injury in patients treated with percutaneous coronary intervention. J. Am. Coll. Cardiol. 2013, 62, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, Y.; Tsutsui, H.; Tsuchihashi, M.; Masumoto, A.; Takeshita, A. Cholesterol Embolism Study(CHEST) Investigators. The incidence and risk factors of cholesterol embolization syndrome; a complication of cardiac catheterization: A prospective study. J. Am. Coll. Cardiol. 2003, 42, 211–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marbach, J.A.; Wells, G.; Santo, P.D.; So, D.; Chong, A.Y.; Russo, J.; Labinaz, M.; Dick, A.; Froeschl, M.; Glover, C.; et al. Acute kidney injury after radial or femoral artery access in ST-segment elevation myocardial infarction: AKI-SAFARI. Am. Heart J. 2021, 234, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Zhen, X.W.; Song, N.P.; Ma, L.H.; Ma, L.N.; Guo, L.; Yang, X.D. Calprotectin and Neutrophil Gelatinase-Associated Lipocalin As Biomarkers of Acute Kidney Injury in Acute Coronary Syndrome. Am. J. Med. Sci. 2021, 361, 736–743. [Google Scholar] [CrossRef]
- Tung, Y.C.; Chang, C.H.; Chen, Y.C.; Chu, P.H. Combined biomarker analysis for risk of acute kidney injury in patients with ST-segment elevation myocardial infarction. PLoS ONE 2015, 10, e0125282. [Google Scholar] [CrossRef]
- Shlipak, M.G.; Matsushita, K.; Ärnlöv, J.; Inker, L.A.; Katz, R.; Polkinghorne, K.R.; Rothenbacher, D.; Sarnak, M.J.; Astor, B.C.; Coresh, J.; et al. CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N. Engl. J. Med. 2013, 369, 932–943. [Google Scholar] [CrossRef] [Green Version]
- Kashani, K.; Al-Khafaji, A.; Ardiles, T.; Artigas, A.; Bagshaw, S.M.; Bell, M.; Bihorac, A.; Birkhahn, R.; Cely, C.M.; Chawla, L.S.; et al. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit. Care 2013, 17, R25. [Google Scholar] [CrossRef] [Green Version]
- Dusse, F.; Edayadiyil-Dudásova, M.; Thielmann, M.; Wendt, D.; Kahlert, P.; Demircioglu, E.; Jakob, H.; Schaefer, S.T.; Pilarczyk, K. Early prediction of acute kidney injury after transapical and transaortic aortic valve implantation with urinary G1 cell cycle arrest biomarkers. BMC Anesthesiol. 2016, 16, 76. [Google Scholar] [CrossRef] [Green Version]
- Doi, K.; Noiri, E.; Sugaya, T. Urinary L-type fatty acid-binding protein as a new renal biomarker in critical care. Curr. Opin. Crit. Care 2010, 16, 545–549. [Google Scholar] [CrossRef]
- Liu, K.L.; Lee, K.T.; Chang, C.H.; Chen, Y.C.; Lin, S.M.; Chu, P.H. Elevated plasma thrombomodulin and angiopoietin-2 predict the development of acute kidney injury in patients with acute myocardial infarction. Crit. Care 2014, 18, R100. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Yuan, J.; Zhao, Y.; Zha, Y. Urine interleukin-18 in prediction of acute kidney injury: A systemic review and meta-analysis. J. Nephrol. 2015, 28, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.; Qiu, H.; Zhu, Y.; Lu, Y.; Li, W. Preprocedural SII Combined with High-Sensitivity C-Reactive Protein Predicts the Risk of Contrast-Induced Acute Kidney Injury in STEMI Patients Undergoing Percutaneous Coronary Intervention. J. Inflamm. Res. 2022, 15, 3677–3687. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Li, D.; Xu, T.; Chen, Z.; Shan, Y.; Zhao, L.; Fu, G.; Luan, Y.; Xia, S.; Zhang, W. Systemic Immune-Inflammation Index Predicts Contrast-Induced Acute Kidney Injury in Patients Undergoing Coronary Angiography: A Cross-Sectional Study. Front. Med. 2022, 9, 841601. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Song, Y.; Geru, A.; Li, Y. Role of Hydration in Contrast-Induced Nephropathy in Patients Who Underwent Primary Percutaneous Coronary Intervention. Int. Heart J. 2019, 60, 1077–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, C.; Buerkle, G.; Buettner, H.J.; Petersen, J.; Perruchoud, A.P.; Eriksson, U.; Marsch, S.; Roskamm, H. Prevention of contrast media-associated nephropathy: Randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty. Arch. Intern. Med. 2002, 162, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R.; Gordon, P.; Manoukian, S.V.; Abbott, J.D.; Kereiakes, D.J.; Jeremias, A.; Kim, M.; Dauerman, H.L.; BOSS Trial Investigators. Randomized Trial of Bicarbonate or Saline Study for the Prevention of Contrast-Induced Nephropathy in Patients with CKD. Clin. J. Am. Soc. Nephrol. 2015, 10, 1519–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zapata-Chica, C.A.; Bello Marquez, D.; Serna-Higuita, L.M.; Nieto-Ríos, J.F.; Casas-Arroyave, F.D.; Donado-Gómez, J.H. Sodium bicarbonate versus isotonic saline solution to prevent contrast-induced nephropathy: A systematic review and meta-analysis. Colomb. Med. 2015, 46, 90–103. [Google Scholar] [CrossRef]
- Liu, Y.; Li, H.; Chen, S.; Chen, J.; Tan, N.; Zhou, Y.; Liu, Y.; Ye, P.; Ran, P.; Duan, C.; et al. Excessively High Hydration Volume May Not Be Associated With Decreased Risk of Contrast-Induced Acute Kidney Injury After Percutaneous Coronary Intervention in Patients With Renal Insufficiency. J. Am. Heart Assoc. 2016, 5, e003171. [Google Scholar] [CrossRef] [Green Version]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [Green Version]
- Marenzi, G.; Ferrari, C.; Marana, I.; Assanelli, E.; De Metrio, M.; Teruzzi, G.; Veglia, F.; Fabbiocchi, F.; Montorsi, P.; Bartorelli, A.L. Prevention of contrast nephropathy by furosemide with matched hydration: The MYTHOS (Induced Diuresis With Matched Hydration Compared to Standard Hydration for Contrast Induced Nephropathy Prevention) trial. JACC Cardiovasc. Interv. 2012, 5, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maioli, M.; Toso, A.; Leoncini, M.; Musilli, N.; Grippo, G.; Ronco, C.; McCullough, P.A.; Bellandi, F. Bioimpedance-Guided Hydration for the Prevention of Contrast-Induced Kidney Injury: The HYDRA Study. J. Am. Coll. Cardiol. 2018, 71, 2880–2889. [Google Scholar] [CrossRef] [PubMed]
- Qian, G.; Fu, Z.; Guo, J.; Cao, F.; Chen, Y. Prevention of Contrast-Induced Nephropathy by Central Venous Pressure-Guided Fluid Administration in Chronic Kidney Disease and Congestive Heart Failure Patients. JACC Cardiovasc. Interv. 2016, 9, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Brar, S.S.; Aharonian, V.; Mansukhani, P.; Moore, N.; Shen, A.Y.; Jorgensen, M.; Dua, A.; Short, L.; Kane, K. Haemodynamic-guided fluid administration for the prevention of contrast-induced acute kidney injury: The POSEIDON randomised controlled trial. Lancet 2014, 383, 1814–1823. [Google Scholar] [CrossRef] [PubMed]
- Liang, M.; Yang, S.; Fu, N. Efficacy of short-term moderate or high-dose rosuvastatin in preventing contrast-induced nephropathy: A meta-analysis of 15 randomized controlled trials. Medicine 2017, 96, e7384. [Google Scholar] [CrossRef]
- Zhou, X.; Dai, J.; Xu, X.; Wang, Z.; Xu, H.; Chen, J.; Qiu, Y.; Mao, W. Comparative Efficacy of Statins for Prevention of Contrast-Induced Acute Kidney Injury in Patients With Chronic Kidney Disease: A Network Meta-Analysis. Angiology 2019, 70, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Leoncini, M.; Toso, A.; Maioli, M.; Tropeano, F.; Villani, S.; Bellandi, F. Early high-dose rosuvastatin for contrast-induced nephropathy prevention in acute coronary syndrome: Results from the PRATO-ACS Study (Protective Effect of Rosuvastatin and Antiplatelet Therapy On contrast-induced acute kidney injury and myocardial damage in patients with Acute Coronary Syndrome). J. Am. Coll. Cardiol. 2014, 63, 71–79. [Google Scholar] [CrossRef]
- Weisbord, S.D.; Gallagher, M.; Jneid, H.; Garcia, S.; Cass, A.; Thwin, S.S.; Conner, T.A.; Chertow, G.M.; Bhatt, D.L.; Shunk, K.; et al. Outcomes after Angiography with Sodium Bicarbonate and Acetylcysteine. N. Engl. J. Med. 2018, 378, 603–614. [Google Scholar] [CrossRef]
- ACT Investigators. Acetylcysteine for prevention of renal outcomes in patients undergoing coronary and peripheral vascular angiography: Main results from the randomized Acetylcysteine for Contrast-induced nephropathy Trial (ACT). Circulation 2011, 124, 1250–1259. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Y.; Qiu, H.; Hu, X.Y.; Luo, T.; Gao, X.J.; Zhao, X.Y.; Zhang, J.; Wu, Y.; Yan, H.B.; Qiao, S.B.; et al. Risk Factors of Contrast-induced Acute Kidney Injury in Patients Undergoing Emergency Percutaneous Coronary Intervention. Chin. Med. J. 2017, 130, 45–50. [Google Scholar] [CrossRef]
- Bainey, K.R.; Rahim, S.; Etherington, K.; Rokoss, M.L.; Natarajan, M.K.; Velianou, J.L.; Brons, S.; Mehta, S.R.; CAPTAIN Investigators. Effects of withdrawing vs continuing renin-angiotensin blockers on incidence of acute kidney injury in patients with renal insufficiency undergoing cardiac catheterization: Results from the Angiotensin Converting Enzyme Inhibitor/Angiotensin Receptor Blocker and Contrast Induced Nephropathy in Patients Receiving Cardiac Catheterization (CAPTAIN) trial. Am. Heart J. 2015, 170, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Vogt, B.; Ferrari, P.; Schönholzer, C.; Marti, H.P.; Mohaupt, M.; Wiederkehr, M.; Cereghetti, C.; Serra, A.; Huynh-Do, U.; Uehlinger, D.; et al. Prophylactic hemodialysis after radiocontrast media in patients with renal insufficiency is potentially harmful. Am. J. Med. 2001, 111, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Lauri, G.; Campodonico, J.; Marana, I.; Assanelli, E.; De Metrio, M.; Grazi, M.; Veglia, F.; Fabbiocchi, F.; Montorsi, P.; et al. Comparison of two hemofiltration protocols for prevention of contrast-induced nephropathy in high-risk patients. Am. J. Med. 2006, 119, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Marana, I.; Lauri, G.; Assanelli, E.; Grazi, M.; Campodonico, J.; Trabattoni, D.; Fabbiocchi, F.; Montorsi, P.; Bartorelli, A.L. The prevention of radiocontrast-agent-induced nephropathy by hemofiltration. N. Engl. J. Med. 2003, 349, 1333–1340. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Class/Stage | Criterion SCr/GFR | Urine Output | ||
| RIFLE | AKIN | KDIGO | RIFLE/AKIN/KDIGO | |
| Risk (RIFLE)/ Stage 1 (AKIN and KDIGO) | SCr increase ×1.5 within 7 days or GFR decrease >25% | SCr increase ≥26.5 μmol/L (≥0.3 mg/dL) within 48 h or 1.5–2× within 7 days | SCr increase ≥26.5 μmol/L (≥0.3 mg/dL) within 48 h or 1.5–1.9× within 7 days | <0.5 mL/kg/h (>6 h) |
| Injury (RIFLE)/ Stage 2 (AKIN and KDIGO) | SCr increase ×2 or GFR decrease >50% | SCr increase 2–3× | SCr increase 2–2.9× | <0.5 mL/kg/h (>12 h) |
| Failure (RIFLE)/ Stage 3 (AKIN and KDIGO) | SCr increase ×3 or SCr ≥ 354 μmol/L (≥4 mg/dL) with acute rise 44 μmol/L (>0.5 mg/dL) or GFR decrease >75% | SCr increase ×3 or SCr ≥ 354 μmol/L (≥4 mg/dL) with acute rise 44 μmol/L (>0.5 mg/dL) or need for RRT | SCr increase ×3 or SCr ≥ 354 μmol/L (≥4 mg/dL) or need for RRT | <0.3 mL/kg/h (>24 h) or anuria >12 h |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maksimczuk, J.; Galas, A.; Krzesiński, P. What Promotes Acute Kidney Injury in Patients with Myocardial Infarction and Multivessel Coronary Artery Disease—Contrast Media, Hydration Status or Something Else? Nutrients 2023, 15, 21. https://doi.org/10.3390/nu15010021
Maksimczuk J, Galas A, Krzesiński P. What Promotes Acute Kidney Injury in Patients with Myocardial Infarction and Multivessel Coronary Artery Disease—Contrast Media, Hydration Status or Something Else? Nutrients. 2023; 15(1):21. https://doi.org/10.3390/nu15010021
Chicago/Turabian StyleMaksimczuk, Joanna, Agata Galas, and Paweł Krzesiński. 2023. "What Promotes Acute Kidney Injury in Patients with Myocardial Infarction and Multivessel Coronary Artery Disease—Contrast Media, Hydration Status or Something Else?" Nutrients 15, no. 1: 21. https://doi.org/10.3390/nu15010021