
Iodine Deficiency, Maternal Hypothyroxinemia and Endocrine Disrupters Affecting Fetal Brain Development: A Scoping Review
 ,
,
Abstract
:1. Introduction
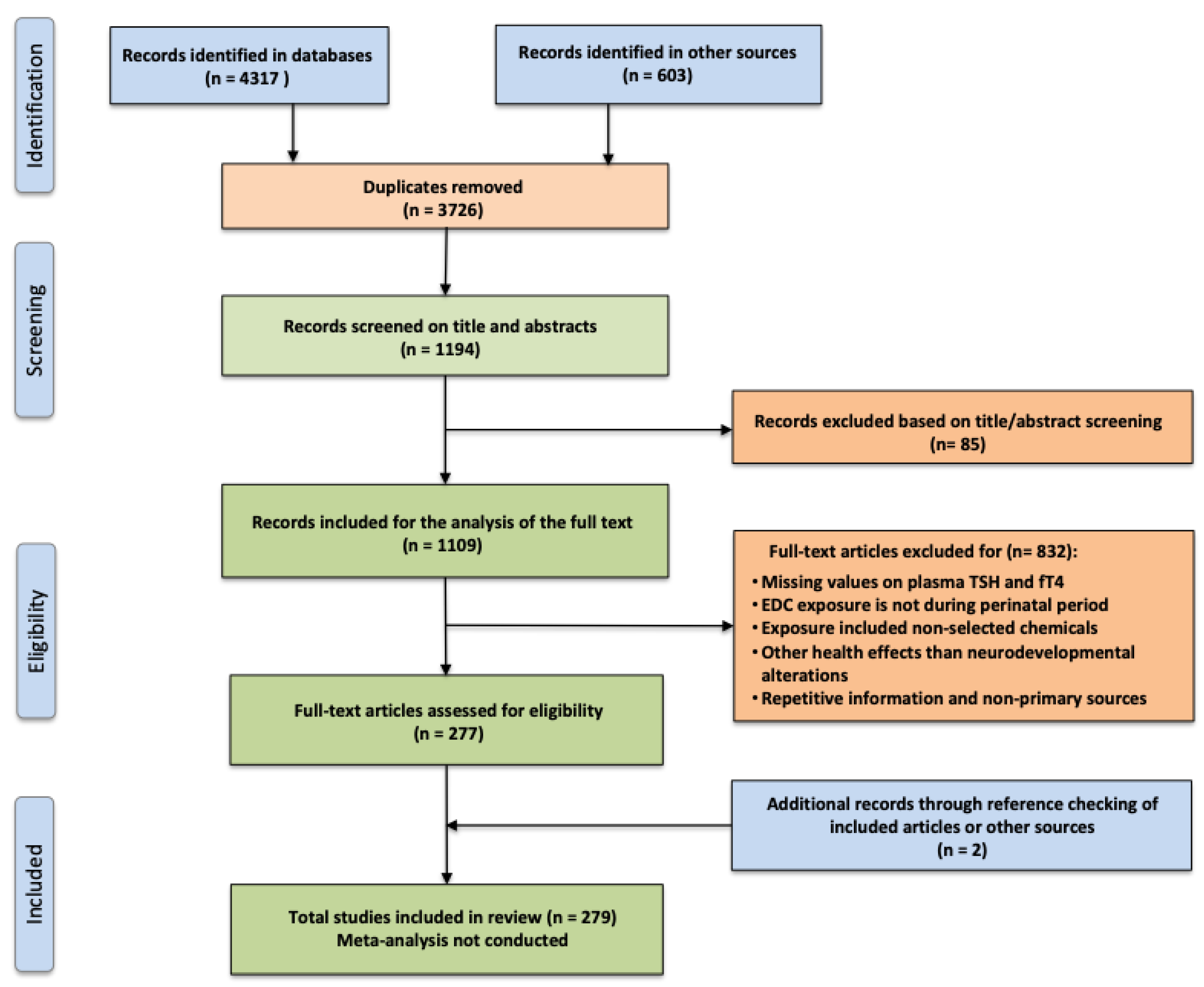
2. Materials and Methods
3. Results and Discussion
3.1. Iodine Requirements and Iodine Status of Pregnant Women in Europe
3.2. Isolated Maternal Hypothyroxinemia (IMH)
Definition, Prevalence and Causes
3.3. Prenatal Brain Development, Timing of Thyroid Hormone Action and Identification of Specific Thyroid-Related Modes-of-Actions (MoAs) in Connection with EDCs
3.4. Mild and Moderate Iodine Deficiency and Its Consequences
3.5. Influence of TDCs, Including Air Pollution on Embryonic/Fetal Neurodevelopment in Iodine-Deficient Areas
3.6. Prevention and Treatment of IMH
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eastman, C.J.; Zimmermann, M.B. The iodine deficiency disorders. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK285556/ (accessed on 1 April 2022).
- American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice. Reducing Prenatal Exposure to Toxic Environmental Agents: ACOG Committee Opinion, Number 832. Obstet. Gynecol. 2021, 138, e40–e54. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, B.; Terekeci, H.; Sandal, S.; Kelestimur, F. Endocrine disrupting chemicals: Exposure, effects on human health, mechanism of action, models for testing and strategies for prevention. Rev. Endocr. Metab. Disord. 2020, 21, 127–147. [Google Scholar] [CrossRef] [PubMed]
- Ghassabian, A.; Trasande, L. Disruption in Thyroid Signaling Pathway: A Mechanism for the Effect of Endocrine-Disrupting Chemicals on Child Neurodevelopment. Front. Endocrinol. 2018, 9, 204. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Roig, M.D.; Pascal, R.; Cahuana, M.J.; García-Algar, O.; Sebastiani, G.; Andreu-Fernández, V.; Martínez, L.; Rodríguez, G.; Iglesia, I.; Ortiz-Arrabal, O.; et al. Environmental Exposure during Pregnancy: Influence on Prenatal Development and Early Life: A Comprehensive Review. Fetal Diagn. Ther. 2021, 48, 245–257. [Google Scholar] [CrossRef]
- Köhrle, J.; Frädrich, C. Thyroid hormone system disrupting chemicals. Best Pract. Res. Clin. Endocrinol. Metab. 2021, 35, 101562. [Google Scholar] [CrossRef] [PubMed]
- Hamers, T.; Kortenkamp, A.; Scholze, M.; Molenaar, D.; Cenijn, P.H.; Weiss, J.M. Transthyretin-Binding Activity of Complex Mixtures Representing the Composition of Thyroid-Hormone Disrupting Contaminants in House Dust and Human Serum. Environ. Health Perspect. 2020, 128, 17015. [Google Scholar] [CrossRef]
- Lisco, G.; De Tullio, A.; Giagulli, V.A.; De Pergola, G.; Triggiani, V. Interference on iodine uptake and human thyroid function by perchlorate-contaminated water and food. Nutrients 2020, 12, 1669. [Google Scholar] [CrossRef]
- Demeneix, B.A. Evidence for Prenatal Exposure to Thyroid Disruptors and Adverse Effects on Brain Development. Eur. Thyroid J. 2019, 8, 283–292. [Google Scholar] [CrossRef]
- Ghassabian, A.; Pierotti, L.; Basterrechea, M.; Chatzi, L.; Estarlich, M.; Fernández-Somoano, A.; Fleisch, A.F.; Gold, D.R.; Julvez, J.; Karakosta, P.; et al. Association of Exposure to Ambient Air Pollution with Thyroid Function During Pregnancy. JAMA Netw. Open 2019, 2, e1912902. [Google Scholar] [CrossRef]
- Mughal, B.B.; Fini, J.B.; Demeneix, B.A. Thyroid-disrupting chemicals and brain development: An update. Endocr. Connect. 2018, 7, R160–R186. [Google Scholar] [CrossRef]
- Lanphear, B.P. The impact of toxins on the developing brain. Annu. Rev. Public Health 2015, 36, 211–230. [Google Scholar] [CrossRef] [PubMed]
- Hetzel, B.S. The development of a global program for the elimination of brain damage due to iodine deficiency. Asia Pac. J. Clin. Nutr. 2012, 21, 164–170. [Google Scholar] [PubMed]
- Monahan, M.; Boelaert, K.; Jolly, K.; Chan, S.; Barton, P.; Roberts, T.E. Costs and benefits of iodine supplementation for pregnant women in a mildly to moderately iodine-deficient population: A modelling analysis. Lancet Diabetes Endocrinol. 2015, 3, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Großklaus, R. Nutzen und Risiken der Jodprophylaxe. Einfluss von Jodsalz auf Schilddrüsenkrankheiten und die Gesundheit des Menschen. Prävent. Gesundh. 2007, 2, 158–166. [Google Scholar]
- Demeneix, B.; Slama, R. Endocrine Disruptors: From Scientific Evidence to Human Health Protection. In Report Commissioned by the PETI Committee of the European Parliament; Policy Department for Citizen’s Rights and Constitutional Affairs: Brussels, Belgium, 2019; Available online: http://www.europarl.europa.eu/RegData/etudes/STUD/2019/608866/IPOL_STU(2019)608866_EN.pdf (accessed on 9 October 2021).
- Trasande, L.; Zoeller, R.T.; Hass, U.; Kortenkamp, A.; Grandjean, P.; Myers, J.P.; DiGangi, J.; Hunt, P.M.; Rudel, R.; Sathyanarayana, S.; et al. Burden of disease and costs of exposure to endocrine disrupting chemicals in the European Union: An updated analysis. Andrology 2016, 4, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.G.; Cole, T.B.; Dao, K.; Chang, Y.-C.; Garrick, J.M. Developmental impact of air pollution on brain function. Neurochem. Int. 2019, 131, 104580. [Google Scholar] [CrossRef] [PubMed]
- Rivas, I.; Basagaña, X.; Cirach, M.; López-Vicente, M.; Suades-González, E.; Garcia-Esteban, R.; Álvarez-Pedrerol, M.; Dadvand, P.; Sunyer, J. Association between Early Life Exposure to Air Pollution and Working Memory and Attention. Environ. Health Perspect. 2019, 127, 57002. [Google Scholar] [CrossRef]
- D’Angiulli, A. Severe Urban Outdoor Air Pollution and Children’s Structural and Functional Brain Development, From Evidence to Precautionary Strategic Action. Front. Public Health 2018, 6, 95. [Google Scholar] [CrossRef]
- Suades-González, E.; Gascon, M.; Guxens, M.; Sunyer, J. Air Pollution and Neuropsychological Development: A Review of the Latest Evidence. Endocrinology 2015, 156, 3473–3482. [Google Scholar] [CrossRef]
- Padmanabhan, V.; Song, W.; Puttabyatappa, M. Pregnatio Perturbatio-Impact of Endocrine-Disrupting Chemicals. Endocr. Rev. 2021, 42, 295–353. [Google Scholar] [CrossRef]
- Inoue, K.; Yan, Q.; Arah, O.A.; Paul, K.; Walker, D.I.; Jones, D.P.; Ritz, B. Air Pollution and Adverse Pregnancy and Birth Outcomes: Mediation Analysis Using Metabolomic Profiles. Curr. Environ. Health Rep. 2020, 7, 231–242, Erratum in Curr. Environ. Health Rep. 2020, 7, 441. [Google Scholar] [CrossRef] [PubMed]
- Pergialiotis, V.; Kotrogianni, P.; Christopoulos-Timogiannakis, E.; Koutaki, D.; Daskalakis, G.; Papantoniou, N. Bisphenol A and adverse pregnancy outcomes: A systematic review of the literature. J. Matern. Fetal Neonatal Med. 2018, 31, 3320–3327. [Google Scholar] [CrossRef] [PubMed]
- Janssen, B.G.; Saenen, N.D.; Roels, H.A.; Madhloum, N.; Gyselaers, W.; Lefebvre, W.; Penders, J.; Vanpoucke, C.; Vrijens, K.; Nawrot, T.S. Fetal Thyroid Function, Birth Weight, and in Utero Exposure to Fine Particle Air Pollution: A Birth Cohort Study. Environ. Health Perspect. 2017, 125, 699–705. [Google Scholar] [CrossRef]
- Zhao, X.; Peng, S.; Xiang, Y.; Yang, Y.; Li, J.; Shan, Z.; Teng, W. Correlation between Prenatal Exposure to Polybrominated Diphenyl Ethers (PBDEs) and Infant Birth Outcomes: A Meta-Analysis and an Experimental Study. Int. J. Environ. Res. Public Health 2017, 14, 268. [Google Scholar] [CrossRef]
- Li, M.; Eastman, C.J. The changing epidemiology of iodine deficiency. Nat. Rev. Endocrinol. 2012, 8, 434–440. [Google Scholar] [CrossRef]
- Velasco, I.; Bath, S.C.; Rayman, M.P. Iodine as Essential Nutrient during the First 1000 Days of Life. Nutrients 2018, 10, 290. [Google Scholar] [CrossRef]
- Bath, S.C. The effect of iodine deficiency during pregnancy on child development. Proc. Nutr. Soc. 2019, 78, 150–160. [Google Scholar] [CrossRef]
- Min, H.; Dong, J.; Wang, Y.; Wang, Y.; Teng, W.; Xi, Q.; Chen, J. Maternal Hypothyroxinemia-Induced Neurodevelopmental Impairments in the Progeny. Mol. Neurobiol. 2016, 53, 1613–1624. [Google Scholar] [CrossRef]
- De Escobar, G.M.; Obregón, M.J.; del Rey, F.E. Iodine deficiency and brain development in the first half of pregnancy. Public Health Nutr. 2007, 10, 1554–1570. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xue, F. The impact of gestational hypothyroxinemia on the cognitive and motor development of offspring. J. Matern. Fetal Neonatal Med. 2020, 33, 1940–1945. [Google Scholar] [CrossRef]
- Dosiou, C.; Medici, M. Isolated maternal hypothyroxinemia during pregnancy: Knowns and unknowns. Eur. J. Endocrinol. 2017, 176, R21–R38. [Google Scholar] [CrossRef] [PubMed]
- Henrichs, J.; Ghassabian, A.; Peeters, R.P.; Tiemeier, H. Maternal hypothyroxinemia and effects on cognitive functioning in childhood: How and why? Clin. Endocrinol. 2013, 79, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Moleti, M.; Trimarchi, F.; Vermiglio, F. Doubts and Concerns about Isolated Maternal Hypothyroxinemia. J. Thyroid Res. 2011, 2011, 463029. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Glinoer, D. The regulation of thyroid function during normal pregnancy: Importance of the iodine nutrition status. Best Pract. Res. Clin. Endocrinol. Metab. 2004, 18, 133–152. [Google Scholar] [CrossRef]
- EFSA NDA Panel (EFSA Panel on Panel on Dietetic Products Nutrition and Allergies). Scientific Opinion on Dietary Reference Values for iodine. EFSA J. 2014, 12, 3660. [Google Scholar] [CrossRef]
- World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers, 3rd ed.; World Health Organization: Geneva, Switzerland, 2007; Available online: https://apps.who.int/iris/handle/10665/43781 (accessed on 1 April 2022).
- Eastman, C.J.; Ma, G.; Li, M. Optimal Assessment and Quantification of Iodine Nutrition in Pregnancy and Lactation: Laboratory and Clinical Methods, Controversies and Future Directions. Nutrients 2019, 11, 2378. [Google Scholar] [CrossRef]
- Gizak, M.; Rogers, L.; Gorstein, J.A.; Zimmermann, M.; Andersson, M. Global iodine status in school-age children, women of reproductive age, and pregnant women in 2017. In Proceedings of the Poster Presented at the Nutrition 2018, the American Society for Nutrition Annual Conference, Boston, MA, USA, 9–12 June 2018; Available online: https://www.ign.org/cm_data/251_Gizak_poster.pdf (accessed on 12 June 2018).
- The Iodine Global Network. Global Scorecard of Iodine Nutrition in 2017 in the General Population and in Pregnant Women (PW); IGN: Zurich, Switzerland, 2017; Available online: https://www.ign.org/cm_data/IGN_Global_Scorecard_AllPop_and_PW_May2017.pdf (accessed on 1 May 2017).
- Katko, M.; Gazso, A.A.; Hircsu, I.; Bhattoa, H.P.; Molnar, Z.; Kovacs, B.; Andrasi, D.; Aranyosi, J.; Makai, R.; Veress, L.; et al. Thyroglobulin level at week 16 of pregnancy is superior to urinary iodine concentration in revealing preconceptual and first trimester iodine supply. Matern. Child Nutr. 2018, 14, e12470. [Google Scholar] [CrossRef]
- Candido, A.C.; Morais, N.D.S.D.; Dutra, L.V.; Pinto, C.A.; Franceschini, S.D.C.C.; Alfenas, R.D.C.G. Insufficient iodine intake in pregnant women in different regions of the world: A systematic review. Arch. Endocrinol. Metab. 2019, 63, 306–311, Erratum in Arch. Endocrinol. Metab. 2020, 64, 96. [Google Scholar] [CrossRef]
- Baldini, E.; Virili, C.; D’Armiento, E.; Centanni, M.; Ulisse, S. Iodine Status in Schoolchildren and Pregnant Women of Lazio, a Central Region of Italy. Nutrients 2019, 11, 1647. [Google Scholar] [CrossRef]
- Medici, M.; Ghassabian, A.; Visser, W.E.; Keizer-Schrama, S.M.P.F.D.M.; Jaddoe, V.W.V.; Hooijkaas, H.; Hofman, A.; Steegers, E.A.P.; Bongers-Schokking, J.J.; Ross, H.A.; et al. Women with high early pregnancy urinary iodine levels have an increased risk of hyperthyroid newborns: The population-based Generation R Study. Clin. Endocrinol. 2014, 80, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Vandevijvere, S.; Amsalkhir, S.; Mourri, A.B.; Van Oyen, H.; Moreno-Reyes, R. Iodine deficiency among Belgian pregnant women not fully corrected by iodine-containing multivitamins: A national cross-sectional survey. Br. J. Nutr. 2013, 109, 2276–2284. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.L.; Sørensen, L.K.; Krejbjerg, A.; Møller, M.; Laurberg, P. Iodine deficiency in Danish pregnant women. Dan. Med. J. 2013, 60, A4657. [Google Scholar] [PubMed]
- Global Fortification Data Exchange. Available online: https://fortificationdata.org (accessed on 8 April 2021).
- Nyström, H.F.; Brantsæter, A.L.; Erlund, I.; Gunnarsdottir, I.; Hulthén, L.; Laurberg, P.; Mattisson, I.; Rasmussen, L.B.; Virtanen, S.; Meltzer, H.M. Iodine status in the Nordic countries—Past and present. Food Nutr. Res. 2016, 60, 31969. [Google Scholar] [CrossRef] [PubMed]
- Miles, E.A.; Vahlberg, T.; Calder, P.C.; Houttu, N.; Pajunen, L.; Koivuniemi, E.; Mokkala, K.; Laitinen, K. Iodine status in pregnant women and infants in Finland. Eur. J. Nutr. 2022, 61, 2919–2927. [Google Scholar] [CrossRef]
- Nazeri, P.; Mirmiran, P.; Shiva, N.; Mehrabi, Y.; Mojarrad, M.; Azizi, F. Iodine nutrition status in lactating mothers residing in countries with mandatory and voluntary iodine fortification programs: An updated systematic review. Thyroid 2015, 25, 611–620. [Google Scholar] [CrossRef]
- Manousou, S.; Andersson, M.; Eggertsen, R.; Hunziker, S.; Hulthén, L.; Nyström, H.F. Iodine deficiency in pregnant women in Sweden: A national cross-sectional study. Eur. J. Nutr. 2020, 59, 2535–2545. [Google Scholar] [CrossRef]
- Lindorfer, H.; Krebs, M.; Kautzky-Willer, A.A.; Bancher-Todesca, D.; Sager, M.; Gessl, A.A. Iodine deficiency in pregnant women in Austria. Eur. J. Clin. Nutr. 2015, 69, 349–354. [Google Scholar] [CrossRef]
- The Iodine Global Network. Global Scorecard of Iodine Nutrition in 2020 in the General Population Based on School-Age Children (SAC); IGN: Ottawa, ON, Canada, 2020; Available online: https://www.ign.org/cm_data/Global-Scorecard-2020-3-June-2020.pdf (accessed on 3 June 2020).
- Johner, S.A.; Thamm, M.; Schmitz, R.; Remer, T. Examination of iodine status in the German population: An example for methodological pitfalls of the current approach of iodine status assessment. Eur. J. Nutr. 2016, 55, 1275–1282. [Google Scholar] [CrossRef]
- Ittermann, T.; Albrecht, D.; Arohonka, P.; Bilek, R.; Castro, J.J.; Dahl, L.; Nystrom, H.F.; Gaberscek, S.; Garcia-Fuentes, E.; Gheorghiu, M.L.; et al. Standardized Map of Iodine Status in Europe. Thyroid 2020, 30, 1346–1354. [Google Scholar] [CrossRef]
- Hey, I.; Thamm, M. Monitoring der Jod- und Natriumversorgung bei Kindern und Jugendlichen im Rahmen der Studie des Robert Koch-Instituts zur Gesundheit von Kindern und Jugendlichen in Deutschland (KiGGS Welle 2); Abschlussbericht, Robert Koch-Institut: Berlin, Germany, 2019; Available online: https://service.ble.de/ptdb/index2.php?detail_id=47144&site_key=145&zeilenzahl_zaehler=592&NextRow=330 (accessed on 1 August 2015).
- Bissinger, K.; Herrmann, R.; Jordan, I. Salt iodisation of processed foods in Germany: Evidence, processors’ perceptions and implications for public health. Br. Food J. 2022, 124, 718–731. [Google Scholar] [CrossRef]
- Olivieri, A.; Di Cosmo, C.; De Angelis, S.; Da Cas, R.; Stacchini, P.; Pastorelli, A.; Vitti, P.; Prevention, R.O.F.G. Regional Observatories for Goiter Prevention. The way forward in Italy for iodine. Minerva Med. 2017, 108, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Szybinski, Z. Poland Remains Iodine Sufficient after 20 Years of IDD Prevention, but Pregnant Women May Be at Risk. IDD Newsletter, 1 August 2015. Available online: https://ign.org/research/ (accessed on 1 August 2015).
- Gerasimov, G. Progress of IDD Elimination through Universal Salt Iodization in the Czech Republic, Slovakia, Hungary and Poland. UNICEF Regional Office for Central and Eastern Europe, Commonwealth of Independent States and the Baltic States, March 2002. Available online: https://www.ign.org/cm_data/2002_Gerasimov_CWCP_Salt_IDDreport2002.pdf (accessed on 1 September 2002).
- Kirkegaard-Klitbo, D.M.; Perslev, K.; Andersen, S.L.; Perrild, H.; Knudsen, N.; Weber, T.; Rasmussen, L.B.; Laurberg, P. Iodine deficiency in pregnancy is prevalent in vulnerable groups in Denmark. Dan. Med. J. 2016, 63, A5286. [Google Scholar]
- Vandevijvere, S.; Mourri, A.B.; Amsalkhir, S.; Avni, F.; Van Oyen, H.; Moreno-Reyes, R. Fortification of bread with iodized salt corrected iodine deficiency in school-aged children, but not in their mothers: A national cross-sectional survey in Belgium. Thyroid 2012, 22, 1046–1053. [Google Scholar] [CrossRef]
- Trumpff, C.; De Schepper, J.; Tafforeau, J.; Van Oyen, H.; Vanderfaeillie, J.; Vandevijvere, S. Mild iodine deficiency in pregnancy in Europe and its consequences for cognitive and psychomotor development of children: A review. J. Trace Elem. Med. Biol. 2013, 27, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Delange, F. Iodine supplementation of pregnant women in Europe: A review and recommendations. Eur. J. Clin. Nutr. 2004, 58, 979–984. [Google Scholar] [CrossRef]
- Panth, P.; Guerin, G.; DiMarco, N.M. A Review of Iodine Status of Women of Reproductive Age in the USA. Biol. Trace Elem. Res. 2019, 188, 208–220. [Google Scholar] [CrossRef]
- Pop, V.J.; Kuijpens, J.L.; van Baar, A.; Verkerk, G.; Van Son, M.M.; De Vijlder, J.J.; Vulsma, T.; Wiersinga, W.M.; Drexhage, H.A.; Vader, H.L. Low maternal free thyroxine concentrations during early pregnancy are associated with impaired psychomotor development in infancy. Clin. Endocrinol. 1999, 50, 149–155. [Google Scholar] [CrossRef]
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J.; et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid 2017, 27, 315–389, Erratum in Thyroid 2017, 27, 1212. [Google Scholar] [CrossRef]
- Furnica, R.M.; Lazarus, J.H.; Gruson, D.; Daumerie, C. Update on a new controversy in endocrinology: Isolated maternal hypothyroxinemia. J. Endocrinol. Investig. 2015, 38, 117–123. [Google Scholar] [CrossRef]
- Dong, A.C.; Stagnaro-Green, A. Differences in Diagnostic Criteria Mask the True Prevalence of Thyroid Disease in Pregnancy: A Systematic Review and Meta-Analysis. Thyroid 2019, 29, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Elahi, S.; Nagra, S.A. Low maternal iodine intake and early pregnancy hypothyroxinemia: Possible repercussions for children. Indian J. Endocrinol. Metab. 2014, 18, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Moog, N.; Entringer, S.; Heim, C.; Wadhwa, P.; Kathmann, N.; Buss, C. Influence of maternal thyroid hormones during gestation on fetal brain development. Neuroscience 2017, 342, 68–100. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.E.; O’Shaughnessy, K.L.; Axelstad, M. Regulation of Thyroid-disrupting Chemicals to Protect the Developing Brain. Endocrinology 2020, 161, bqaa106. [Google Scholar] [CrossRef] [PubMed]
- López-Muñoz, E.; Mateos-Sánchez, L.; Mejía-Terrazas, G.E.; Bedwell-Cordero, S.E. Hypothyroidism and isolated hypothyroxinemia in pregnancy, from physiology to the clinic. Taiwan J. Obstet. Gynecol. 2019, 58, 757–763. [Google Scholar] [CrossRef]
- Korevaar, T.I.; Nieboer, D.; Bisschop, P.H.; Goddijn, M.; Medici, M.; Chaker, L.; de Rijke, Y.B.; Jaddoe, V.W.; Visser, T.J.; Steyerberg, E.W.; et al. Risk factors and a clinical prediction model for low maternal thyroid function during early pregnancy: Two population-based prospective cohort studies. Clin. Endocrinol. 2016, 85, 902–909. [Google Scholar] [CrossRef]
- Liu, Y.; Li, G.; Guo, N.; Liu, X.; Huang, S.; Du, Q. Association between Maternal Characteristics and the Risk of Isolated Maternal Hypothyroxinemia. Front. Endocrinol. 2022, 13, 843324. [Google Scholar] [CrossRef]
- Karbownik-Lewińska, M.; Stępniak, J.; Lewiński, A. Potential Risk Factors for Isolated Hypothyroxinemia in Women of Childbearing Age-Results from Retrospective Analysis. J. Clin. Med. 2021, 10, 5384. [Google Scholar] [CrossRef]
- Etemadi, A.; Amouzegar, A.; Mehran, L.; Tohidi, M.; Azizi, F.; Moradi, K.; Delshad, H. Isolated Hypothyroxinemia in Iranian Pregnant Women, the Role of Iodine Deficiency: A Population-Based Cross-Sectional Study. Thyroid 2020, 30, 262–269. [Google Scholar] [CrossRef]
- Knight, B.A.; Shields, B.M.; Hattersley, A.T.; Vaidya, B. Maternal hypothyroxinaemia in pregnancy is associated with obesity and adverse maternal metabolic parameters. Eur. J. Endocrinol. 2016, 174, 51–57. [Google Scholar] [CrossRef]
- Ventura, M.; Melo, M.; Carrilho, F. Selenium and Thyroid Disease: From Pathophysiology to Treatment. Int. J. Endocrinol. 2017, 2017, 1297658. [Google Scholar] [CrossRef] [PubMed]
- Teng, X.; Shan, Z.; Li, C.; Yu, X.; Mao, J.; Wang, W.; Xie, X.; Du, J.; Zhang, S.; Gao, Z.; et al. Iron Deficiency May Predict Greater Risk for Hypothyroxinemia: A Retrospective Cohort Study of Pregnant Women in China. Thyroid 2018, 28, 968–975. [Google Scholar] [CrossRef]
- Hu, X.; Wang, R.; Shan, Z.; Dong, Y.; Zheng, H.; Jesse, F.F.; Rao, E.; Takahashi, E.; Li, W.; Teng, W.; et al. Perinatal Iron Deficiency-Induced Hypothyroxinemia Impairs Early Brain Development Regardless of Normal Iron Levels in the Neonatal Brain. Thyroid 2016, 26, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Soldin, O.P.; Soldin, S.J. Thyroid hormone testing by tandem mass spectrometry. Clin. Biochem. 2011, 44, 89–94. [Google Scholar] [CrossRef]
- Lazarus, J.; Brown, R.S.; Daumerie, C.; Hubalewska-Dydejczyk, A.; Negro, R.; Vaidya, B. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur. Thyroid J. 2014, 3, 76–94. [Google Scholar] [CrossRef] [PubMed]
- Miranda, A.; Sousa, N. Maternal hormonal milieu influence on fetal brain development. Brain Behav. 2018, 8, e00920. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J. Thyroid Hormones in Brain Development and Function. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2022. [Google Scholar]
- Korevaar, T.I.M.; Medici, M.; Visser, T.J.; Peeters, R.P. Thyroid disease in pregnancy: New insights in diagnosis and clinical management. Nat. Rev. Endocrinol. 2017, 13, 610–622. [Google Scholar] [CrossRef]
- Williams, G.R. Neurodevelopmental and neurophysiological actions of thyroid hormone. J. Neuroendocrinol. 2008, 20, 784–794. [Google Scholar] [CrossRef]
- Stepien, B.K.; Huttner, W.B. Transport, Metabolism, and Function of Thyroid Hormones in the Developing Mammalian Brain. Front. Endocrinol. 2019, 10, 209. [Google Scholar] [CrossRef]
- Costeira, M.J.; Oliveira, P.; Santos, N.C.; Ares, S.; Saenz-Rico, B.; de Escobar, G.M.; Palha, J.A. Psychomotor development of children from an iodine-deficient region. J. Pediatr. 2011, 159, 447–453. [Google Scholar] [CrossRef]
- Kawahori, K.; Hashimoto, K.; Yuan, X.; Tsujimoto, K.; Hanzawa, N.; Hamaguchi, M.; Kase, S.; Fujita, K.; Tagawa, K.; Okazawa, H.; et al. Mild Maternal Hypothyroxinemia During Pregnancy Induces Persistent DNA Hypermethylation in the Hippocampal Brain-Derived Neurotrophic Factor Gene in Mouse Offspring. Thyroid 2018, 28, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Ghassabian, A.; El Marroun, H.; Peeters, R.P.; Jaddoe, V.W.; Hofman, A.; Verhulst, F.C.; Tiemeier, H.; White, T. Downstream effects of maternal hypothyroxinemia in early pregnancy: Nonverbal IQ and brain morphology in school-age children. J. Clin. Endocrinol. Metab. 2014, 99, 2383–2390. [Google Scholar] [CrossRef]
- Suárez-Rodríguez, M.; Azcona-San Julián, C.; Alzina de Aguilar, V. Hypothyroxinemia during pregnancy: The effect on neurodevelopment in the child. Int. J. Dev. Neurosci. 2012, 30, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Kasatkina, E.P.; Samsonova, L.N.; Ivakhnenko, V.N.; Ibragimova, G.V.; Ryabykh, A.V.; Naumenko, L.L.; Evdokimova, Y.A. Gestational hypothyroxinemia and cognitive function in offspring. Neurosci. Behav. Physiol. 2006, 36, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Korevaar, T.I.M.; Muetzel, R.; Medici, M.; Chaker, L.; Jaddoe, V.W.V.; de Rijke, Y.B.; Steegers, E.A.P.; Visser, T.J.; White, T.; Tiemeier, H.; et al. Association of maternal thyroid function during early pregnancy with offspring IQ and brain morphology in childhood: A population-based prospective cohort study. Lancet Diabetes Endocrinol. 2016, 4, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Lischinsky, J.E.; Skocic, J.; Clairman, H.; Rovet, J. Preliminary Findings Show Maternal Hypothyroidism May Contribute to Abnormal Cortical Morphology in Offspring. Front. Endocrinol. 2016, 7, 16. [Google Scholar] [CrossRef]
- Jansen, T.A.; Korevaar, T.I.M.; Mulder, T.A.; White, T.; Muetzel, R.L.; Peeters, R.P.; Tiemeier, H. Maternal thyroid function during pregnancy and child brain morphology: A time window-specific analysis of a prospective cohort. Lancet Diabetes Endocrinol. 2019, 7, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.L.; Carlé, A.; Karmisholt, J.; Pedersen, I.B.; Andersen, S. Mechanism in endocrinolgy: Neurodevelopmental disorders in children born to mothers with thyroid dysfunction: Evidence of fetal programming? Eur. J. Endocrinol. 2017, 177, R27–R36. [Google Scholar] [CrossRef]
- Marty, S.; Beekhuijzen, M.; Charlton, A.; Hallmark, N.; Hannas, B.R.; Jacobi, S.; Melching-Kollmuss, S.; Sauer, U.G.; Sheets, L.P.; Strauss, V.; et al. Towards a science-based testing strategy to identify maternal thyroid hormone imbalance and neurodevelopmental effects in the progeny—Part II: How can key events of relevant adverse outcome pathways be addressed in toxicological assessments? Crit. Rev. Toxicol. 2021, 51, 328–358. [Google Scholar] [CrossRef]
- Mulder, T.A.; Korevaar, T.I.; Peeters, R.P.; van Herwaarden, A.E.; de Rijke, Y.B.; White, T.; Tiemeier, H. Urinary Iodine Concentrations in Pregnant Women and Offspring Brain Morphology. Thyroid 2021, 31, 964–972. [Google Scholar] [CrossRef]
- Boas, M.; Feldt-Rasmussen, U.; Main, K.M. Thyroid effects of endocrine disrupting chemicals. Mol. Cell. Endocrinol. 2012, 355, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Jugan, M.L.; Levi, Y.; Blondeau, J.P. Endocrine disruptors and thyroid hormone physiology. Biochem. Pharmacol. 2010, 79, 939–947. [Google Scholar] [CrossRef] [PubMed]
- Hartoft-Nielsen, M.-L.; Boas, M.; Bliddal, S.; Rasmussen, K.; Main, K.; Feldt-Rasmussen, U. Do Thyroid Disrupting Chemicals Influence Foetal Development during Pregnancy? J. Thyroid Res. 2011, 2011, 342189. [Google Scholar] [CrossRef] [PubMed]
- Noyes, P.D.; Friedman, K.P.; Browne, P.; Haselman, J.T.; Gilbert, M.E.; Hornung, M.W.; Barone, S.; Crofton, K.M.; Laws, S.C.; Stoker, T.E.; et al. Evaluating Chemicals for Thyroid Disruption: Opportunities and Challenges with in Vitro Testing and Adverse Outcome Pathway Approaches. Environ. Health Perspect. 2019, 127, 95001. [Google Scholar] [CrossRef]
- Calsolaro, V.; Pasqualetti, G.; Niccolai, F.; Caraccio, N.; Monzani, F. Thyroid Disrupting Chemicals. Int. J. Mol. Sci. 2017, 18, 2583. [Google Scholar] [CrossRef]
- Duntas, L.H.; Stathatos, N. Toxic chemicals and thyroid function: Hard facts and lateral thinking. Rev. Endocr. Metab. Disord. 2015, 16, 311–318. [Google Scholar] [CrossRef]
- Gilbert, M.E.; Rovet, J.; Chen, Z.; Koibuchi, N. Developmental thyroid hormone disruption: Prevalence, environmental contaminants and neurodevelopmental consequences. Neurotoxicology 2012, 33, 842–852. [Google Scholar] [CrossRef]
- Heindel, J.J.; Balbus, J.; Birnbaum, L.; Brune-Drisse, M.N.; Grandjean, P.; Gray, K.; Landrigan, P.J.; Sly, P.D.; Suk, W.A.; Cory Slechta, D.; et al. Developmental Origins of Health and Disease: Integrating Environmental Influences. Endocrinology 2015, 156, 3416–3421. [Google Scholar] [CrossRef]
- Neven, K.Y.; Cox, B.; Cosemans, C.; Gyselaers, W.; Penders, J.; Plusquin, M.; Roels, H.A.; Vrijens, K.; Ruttens, A.; Nawrot, T.S. Lower iodine storage in the placenta is associated with gestational diabetes mellitus. BMC Med. 2021, 19, 47. [Google Scholar] [CrossRef]
- Neven, K.Y.; Wang, C.; Janssen, B.G.; Roels, H.A.; Vanpoucke, C.; Ruttens, A.; Nawrot, T.S. Ambient air pollution exposure during the late gestational period is linked with lower placental iodine load in a Belgian birth cohort. Environ. Int. 2021, 147, 106334. [Google Scholar] [CrossRef]
- Neven, K.Y.; Cox, B.; Vrijens, K.; Plusquin, M.; Roels, H.A.; Ruttens, A.; Nawrot, T.S. Determinants of placental iodine concentrations in a mild-to-moderate iodine-deficient population: An ENVIRONAGE cohort study. J. Transl. Med. 2020, 18, 426. [Google Scholar] [CrossRef] [PubMed]
- Di, N.; He, W.; Zhang, K.; Cui, J.; Chen, J.; Cheng, J.; Chu, B.; Li, S.; Xie, Y.; Xiang, H.; et al. Association of short-term air pollution with systemic inflammatory biomarkers in routine blood test: A longitudinal study. Environ. Res. Lett. 2021, 16, 035007. [Google Scholar] [CrossRef]
- Kelley, A.S.; Banker, M.; Goodrich, J.M.; Dolinoy, D.C.; Burant, C.; Domino, S.E.; Smith, Y.R.; Song, P.X.K.; Padmanabhan, V. Early pregnancy exposure to endocrine disrupting chemical mixtures are associated with inflammatory changes in maternal and neonatal circulation. Sci. Rep. 2019, 9, 5422. [Google Scholar] [CrossRef] [PubMed]
- Saenen, N.D.; Martens, D.S.; Neven, K.Y.; Alfano, R.; Bové, H.; Janssen, B.G.; Roels, H.A.; Plusquin, M.; Vrijens, K.; Nawrot, T.S. Air pollution-induced placental alterations: An interplay of oxidative stress, epigenetics, and the aging phenotype? Clin. Epigenet. 2019, 11, 124. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Liew, Z.; Uppal, K.; Cui, X.; Ling, C.; Heck, J.E.; von Ehrenstein, O.S.; Wu, J.; Walker, D.I.; Jones, D.P.; et al. Maternal serum metabolome and traffic-related air pollution exposure in pregnancy. Environ. Int. 2019, 130, 104872. [Google Scholar] [CrossRef]
- Zota, A.R.; Geller, R.J.; Romano, L.E.; Coleman-Phox, K.; Adler, N.E.; Parry, E.; Wang, M.; Park, J.-S.; Elmi, A.F.; Laraia, B.A.; et al. Association between persistent endocrine-disrupting chemicals (PBDEs, OH-PBDEs, PCBs, and PFASs) and biomarkers of inflammation and cellular aging during pregnancy and postpartum. Environ. Int. 2018, 115, 9–20. [Google Scholar] [CrossRef]
- Holland, N.; Huen, K.; Tran, V.; Street, K.; Nguyen, B.; Bradman, A.; Eskenazi, B. Urinary Phthalate Metabolites and Biomarkers of Oxidative Stress in a Mexican-American Cohort: Variability in Early and Late Pregnancy. Toxics 2016, 4, 7. [Google Scholar] [CrossRef]
- Ferguson, K.K.; Cantonwine, D.E.; McElrath, T.F.; Mukherjee, B.; Meeker, J.D. Repeated measures analysis of associations between urinary bisphenol-A concentrations and biomarkers of inflammation and oxidative stress in pregnancy. Reprod. Toxicol. 2016, 66, 93–98. [Google Scholar] [CrossRef]
- Zhou, M.; Ford, B.; Lee, D.; Tindula, G.; Huen, K.; Tran, V.; Bradman, A.; Gunier, R.; Eskenazi, B.; Nomura, D.K.; et al. Metabolomic Markers of Phthalate Exposure in Plasma and Urine of Pregnant Women. Front. Public Health 2018, 6, 298. [Google Scholar] [CrossRef]
- Chen, H.; Oliver, B.G.; Pant, A.; Olivera, A.; Poronnik, P.; Pollock, C.A.; Saad, S. Particulate Matter, an Intrauterine Toxin Affecting Foetal Development and Beyond. Antioxidants 2021, 10, 732. [Google Scholar] [CrossRef]
- Johnson, N.M.; Hoffmann, A.R.; Behlen, J.C.; Lau, C.; Pendleton, D.; Harvey, N.; Shore, R.; Li, Y.; Chen, J.; Tian, Y.; et al. Air pollution and children’s health-a review of adverse effects associated with prenatal exposure from fine to ultrafine particulate matter. Environ. Health Prev. Med. 2021, 26, 72. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.G.; Cole, T.B.; Dao, K.; Chang, Y.-C.; Coburn, J.; Garrick, J.M. Effects of air pollution on the nervous system and its possible role in neurodevelopmental and neurodegenerative disorders. Pharmacol. Ther. 2020, 210, 107523. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, K.; Kato, D.; Ikegami, A.; Hashimoto, A.; Sugio, S.; Guo, Z.; Shibushita, M.; Tatematsu, T.; Haruwaka, K.; Moorhouse, A.J.; et al. Maternal immune activation induces sustained changes in fetal microglia motility. Sci. Rep. 2020, 10, 21378. [Google Scholar] [CrossRef] [PubMed]
- Street, M.E.; Bernasconi, S. Endocrine-Disrupting Chemicals in Human Fetal Growth. Int. J. Mol. Sci. 2020, 21, 1430. [Google Scholar] [CrossRef] [PubMed]
- Genc, S.; Zadeoglulari, Z.; Fuss, S.H.; Genc, K. The adverse effects of air pollution on the nervous system. J. Toxicol. 2012, 2012, 782462. [Google Scholar] [CrossRef]
- Fini, J.-B.; Mughal, B.B.; Le Mével, S.; Leemans, M.; Lettmann, M.; Spirhanzlova, P.; Affaticati, P.; Jenett, A.; Demeneix, B.A. Human amniotic fluid contaminants alter thyroid hormone signalling and early brain development in Xenopus embryos. Sci. Rep. 2017, 7, 43786. [Google Scholar] [CrossRef]
- Mitro, S.D.; Johnson, T.; Zota, A.R. Cumulative Chemical Exposures During Pregnancy and Early Development. Curr. Environ. Health Rep. 2015, 2, 367–378. [Google Scholar] [CrossRef]
- De Renzy-Martin, K.T.; Frederiksen, H.; Christensen, J.S.; Kyhl, H.B.; Andersson, A.-M.; Husby, S.; Barington, T.; Main, K.M.; Jensen, T.K. Current exposure of 200 pregnant Danish women to phthalates, parabens and phenols. Reproduction 2014, 147, 443–453. [Google Scholar] [CrossRef]
- Bose, S.; Ross, K.R.; Rosa, M.J.; Chiu, Y.-H.M.; Just, A.; Kloog, I.; Wilson, A.; Thompson, J.; Svensson, K.; Rojo, M.M.T.; et al. Prenatal particulate air pollution exposure and sleep disruption in preschoolers: Windows of susceptibility. Environ. Int. 2019, 124, 329–335. [Google Scholar] [CrossRef]
- Vandenberg, L.N.; Colborn, T.; Hayes, T.B.; Heindel, J.J.; Jacobs, D.R., Jr.; Lee, D.-H.; Shioda, T.; Soto, A.M.; vom Saal, F.S.; Welshons, W.V.; et al. Hormones and endocrine-disrupting chemicals: Low-dose effects and nonmonotonic dose responses. Endocr. Rev. 2012, 33, 378–455. [Google Scholar] [CrossRef]
- Dutta, S.; Haggerty, D.K.; Rappolee, D.A.; Ruden, D.M. Phthalate Exposure and Long-Term Epigenomic Consequences: A Review. Front. Genet. 2020, 11, 405. [Google Scholar] [CrossRef] [PubMed]
- Préau, L.; Fini, J.-B.; Morvan-Dubois, G.; Demeneix, B. Thyroid hormone signaling during early neurogenesis and its significance as a vulnerable window for endocrine disruption. Biochim. Biophys. Acta 2015, 1849, 112–121. [Google Scholar] [CrossRef]
- Xin, F.; Susiarjo, M.; Bartolomei, M.S. Multigenerational and transgenerational effects of endocrine disrupting chemicals: A role for altered epigenetic regulation? Semin. Cell Dev. Biol. 2015, 43, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, M.F.; Chevrier, J.; Harley, K.G.; Kogut, K.; Vedar, M.; Calderon, N.; Trujillo, C.; Johnson, C.; Bradman, A.; Barr, D.B.; et al. Prenatal exposure to organophosphate pesticides and IQ in 7-year-old children. Environ. Health Perspect. 2011, 119, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Eskenazi, B.; Kogut, K.; Huen, K.; Harley, K.G.; Bouchard, M.; Bradman, A.; Boyd-Barr, D.; Johnson, C.; Holland, N. Organophosphate pesticide exposure, PON1, and neurodevelopment in school-age children from the CHAMACOS study. Environ. Res. 2014, 134, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, K.; Araki, A.; Nakajima, S.; Miyashita, C.; Ikeno, T.; Itoh, S.; Minatoya, M.; Kobayashi, S.; Mizutani, F.; Chisaki, Y.; et al. Association between prenatal exposure to organochlorine pesticides and the mental and psychomotor development of infants at ages 6 and 18 months: The Hokkaido Study on Environment and Children’s Health. Neurotoxicology 2018, 69, 201–208. [Google Scholar] [CrossRef]
- Wang, S.; Hu, C.; Lu, A.; Wang, Y.; Cao, L.; Wu, W.; Li, H.; Wu, M.; Yan, C. Association between prenatal exposure to persistent organic pollutants and neurodevelopment in early life: A mother-child cohort (Shanghai, China). Ecotoxicol. Environ. Saf. 2021, 208, 111479. [Google Scholar] [CrossRef]
- Jeddy, Z.; Kordas, K.; Allen, K.; Taylor, E.V.; Northstone, K.; Flanders, W.D.; Namulanda, G.; Sjodin, A.; Hartman, T.J. Prenatal exposure to organochlorine pesticides and early childhood communication development in British girls. Neurotoxicology 2018, 69, 121–129. [Google Scholar] [CrossRef]
- Vermeir, G.; Covaci, A.; Van Larebeke, N.; Schoeters, G.; Nelen, V.; Koppen, G.; Viaene, M. Neurobehavioural and cognitive effects of prenatal exposure to organochlorine compounds in three year old children. BMC Pediatr. 2021, 21, 99. [Google Scholar] [CrossRef]
- Jacobson, J.L.; Jacobson, S.W. Intellectual impairment in children exposed to polychlorinated biphenyls in utero. N. Engl. J. Med. 1996, 335, 783–789. [Google Scholar] [CrossRef]
- Sagiv, S.K.; Thurston, S.W.; Bellinger, D.C.; Tolbert, P.E.; Altshul, L.M.; Korrick, S.A. Prenatal organochlorine exposure and behaviors associated with attention deficit hyperactivity disorder in school-aged children. Am. J. Epidemiol. 2010, 171, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.; Okosieme, O.E.; Murphy, R.; Hales, C.; Chiusano, E.; Maina, A.; Joomun, M.; Bestwick, J.P.; Smyth, P.; Paradice, R.; et al. Maternal perchlorate levels in women with borderline thyroid function during pregnancy and the cognitive development of their offspring: Data from the Controlled Antenatal Thyroid Study. J. Clin. Endocrinol. Metab. 2014, 99, 4291–4298. [Google Scholar] [CrossRef]
- Moore, B.F.; Shapiro, A.L.; Wilkening, G.; Magzamen, S.; Starling, A.P.; Allshouse, W.B.; Adgate, J.L.; Dabelea, D. Prenatal Exposure to Tobacco and Offspring Neurocognitive Development in the Healthy Start Study. J. Pediatr. 2020, 218, 28–34.e2. [Google Scholar] [CrossRef]
- Daniel, S.; Balalian, A.A.; Insel, B.J.; Liu, X.; Whyatt, R.M.; Calafat, A.M.; Rauh, V.A.; Perera, F.P.; Hoepner, L.A.; Herbstman, J.; et al. Prenatal and early childhood exposure to phthalates and childhood behavior at age 7 years. Environ. Int. 2020, 143, 105894. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Chen, X.-Z.; Huang, X.; Wang, M.; Wu, J. The association between prenatal exposure to phthalates and cognition and neurobehavior of children-evidence from birth cohorts. Neurotoxicology 2019, 73, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Engel, S.M.; Miodovnik, A.; Canfield, R.L.; Zhu, C.; Silva, M.J.; Calafat, A.M.; Wolff, M.S.; Engel, S.M.; Miodovnik, A.; Canfield, R.L.; et al. Prenatal phthalate exposure is associated with childhood behavior and executive functioning. Environ. Health Perspect. 2010, 118, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Van den Dries, M.A.; Guxens, M.; Spaan, S.; Ferguson, K.K.; Philips, E.; Santos, S.; Jaddoe, V.W.; Ghassabian, A.; Trasande, L.; Tiemeier, H.; et al. Phthalate and Bisphenol Exposure during Pregnancy and Offspring Nonverbal IQ. Environ. Health Perspect. 2020, 128, 77009. [Google Scholar] [CrossRef]
- Olesen, T.S.; Bleses, D.; Andersen, H.R.; Grandjean, P.; Frederiksen, H.; Trecca, F.; Bilenberg, N.; Kyhl, H.B.; Dalsager, L.; Jensen, I.K.; et al. Prenatal phthalate exposure and language development in toddlers from the Odense Child Cohort. Neurotoxicol. Teratol. 2018, 65, 34–41. [Google Scholar] [CrossRef]
- Ramhøj, L.; Frädrich, C.; Svingen, T.; Scholze, M.; Wirth, E.K.; Rijntjes, E.; Köhrle, J.; Kortenkamp, A.; Axelstad, M. Testing for heterotopia formation in rats after developmental exposure to selected in vitro inhibitors of thyroperoxidase. Environ. Pollut. 2021, 283, 117135. [Google Scholar] [CrossRef]
- O’shaughnessy, K.L.; Kosian, P.A.; Ford, J.L.; Oshiro, W.M.; Degitz, S.J.; Gilbert, M.E. Developmental Thyroid Hormone Insufficiency Induces a Cortical Brain Malformation and Learning Impairments: A Cross-Fostering Study. Toxicol. Sci. 2018, 163, 101–115. [Google Scholar] [CrossRef]
- Crofton, K.M.; Gilbert, M.; Friedman, K.P.; Demeneix, B.; Marty, M.S.; Zoeller, R.T. Adverse Outcome Pathway on Inhibition of Thyroperoxidase and Subsequent Adverse Neurodevelopmental Outcomes in Mammals; OECD Series on Adverse Outcome Pathways, No. 13; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Gibson, E.A.; Siegel, E.L.; Eniola, F.; Herbstman, J.B.; Factor-Litvak, P. Effects of Polybrominated Diphenyl Ethers on Child Cognitive, Behavioral, and Motor Development. Int. J. Environ. Res. Public Health 2018, 15, 1636. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.; Lanphear, B.P.; Bellinger, D.; Axelrad, D.A.; McPartland, J.; Sutton, P.; Davidson, L.; Daniels, N.; Sen, S.; Woodruff, T.J. Developmental PBDE Exposure and IQ/ADHD in Childhood: A Systematic Review and Meta-analysis. Environ. Health Perspect. 2017, 125, 086001. [Google Scholar] [CrossRef]
- Vuong, A.M.; Yolton, K.; Xie, C.; Webster, G.M.; Sjödin, A.; Braun, J.M.; Dietrich, K.N.; Lanphear, B.P.; Chen, A. Childhood polybrominated diphenyl ether (PBDE) exposure and neurobehavior in children at 8 years. Environ. Res. 2017, 158, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Herbstman, J.B.; Mall, J.K. Developmental Exposure to Polybrominated Diphenyl Ethers and Neurodevelopment. Curr. Environ. Health Rep. 2014, 1, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Roze, E.; Meijer, L.; Bakker, A.; Van Braeckel, K.N.J.A.; Sauer, P.J.J.; Bos, A.F. Prenatal exposure to organohalogens, including brominated flame retardants, influences motor, cognitive, and behavioral performance at school age. Environ. Health Perspect. 2009, 117, 1953–1958. [Google Scholar] [CrossRef]
- Wang, Y.; Qian, H. Phthalates and Their Impacts on Human Health. Healthcare 2021, 9, 603. [Google Scholar] [CrossRef]
- Berghuis, S.A.; Soechitram, S.D.; Hitzert, M.M.; Sauer, P.J.; Bos, A.F. Prenatal exposure to polychlorinated biphenyls and their hydroxylated metabolites is associated with motor development of three-month-old infants. Neurotoxicology 2013, 38, 124–130. [Google Scholar] [CrossRef]
- Crofton, K.M.; Zoeller, R.T. Mode of action: Neurotoxicity induced by thyroid hormone disruption during development--hearing loss resulting from exposure to PHAHs. Crit. Rev. Toxicol. 2005, 35, 757–769. [Google Scholar] [CrossRef]
- Paul, K.B.; Hedge, J.M.; Bansal, R.; Zoeller, R.T.; Peter, R.; DeVito, M.; Crofton, K.M. Developmental triclosan exposure decreases maternal, fetal, and early neonatal thyroxine: A dynamic and kinetic evaluation of a putative mode-of-action. Toxicology 2012, 300, 31–45. [Google Scholar] [CrossRef]
- Wang, X.; Ouyang, F.; Fengxiu, O.; Wang, X.; Liu, Z.; Zhang, J. Maternal Urinary Triclosan Concentration in Relation to Maternal and Neonatal Thyroid Hormone Levels: A Prospective Study. Environ. Health Perspect. 2017, 125, 067017. [Google Scholar] [CrossRef]
- Johannes, J.; Jayarama-Naidu, R.; Meyer, F.; Wirth, E.K.; Schweizer, U.; Schomburg, L.; Köhrle, J.; Renko, K. Silychristin, a Flavonolignan Derived from the Milk Thistle, Is a Potent Inhibitor of the Thyroid Hormone Transporter MCT8. Endocrinology 2016, 157, 1694–1701. [Google Scholar] [CrossRef] [PubMed]
- Ruel, M.V.M.; Bos, A.F.; Soechitram, S.D.; Meijer, L.; Sauer, P.J.J.; Berghuis, S.A. Prenatal exposure to organohalogen compounds and children’s mental and motor development at 18 and 30 months of age. Neurotoxicology 2019, 72, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Chianese, R.; Troisi, J.; Richards, S.; Nori, S.L.; Fasano, S.; Guida, M.; Plunk, E.; Viggiano, A.; Pierantoni, R.; et al. Neuro-toxic and Reproductive Effects of BPA. Curr. Neuropharmacol. 2019, 17, 1109–1132. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Park, Y.J. Bisphenols and Thyroid Hormone. Endocrinol. Metab. 2019, 34, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Hansen, L.G. Ortho-substituted polychlorinated biphenyl (PCB) congeners (95 or 101) decrease pituitary response to thyrotropin releasing hormone. Toxicol. Lett. 2003, 144, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, W.; Chen, J.; Wang, N.; Chen, C.; Wang, Y.; Wan, H.; Chen, B.; Lu, Y. Association of Phthalate Exposure with Thyroid Function and Thyroid Homeostasis Parameters in Type 2 Diabetes. J. Diabetes Res. 2021, 2021, 4027380. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hu, C.; Fang, T.; Jin, Y.; Wu, R. Perspective on prenatal polychlorinated biphenyl exposure and the development of the progeny nervous system (Review). Int. J. Mol. Med. 2021, 48, 150. [Google Scholar] [CrossRef]
- Abdelouahab, N.; Langlois, M.-F.; Lavoie, L.; Corbin, F.; Pasquier, J.-C.; Takser, L. Maternal and cord-blood thyroid hormone levels and exposure to polybrominated diphenyl ethers and polychlorinated biphenyls during early pregnancy. Am. J. Epidemiol. 2013, 178, 701–713. [Google Scholar] [CrossRef]
- Derakhshan, A.; Shu, H.; Peeters, R.P.; Kortenkamp, A.; Lindh, C.H.; Demeneix, B.; Bornehag, C.-G.; Korevaar, T.I.M. Association of urinary bisphenols and triclosan with thyroid function during early pregnancy. Environ. Int. 2019, 133 Pt A, 105123. [Google Scholar] [CrossRef]
- Manikkam, M.; Tracey, R.; Guerrero-Bosagna, C.; Skinner, M.K. Plastics derived endocrine disruptors (BPA, DEHP and DBP) induce epigenetic transgenerational inheritance of obesity, reproductive disease and sperm epimutations. PLoS ONE 2013, 8, e55387. [Google Scholar] [CrossRef]
- Hernandez, A.; Stohn, J.P. The Type 3 Deiodinase: Epigenetic Control of Brain Thyroid Hormone Action and Neurological Function. Int. J. Mol. Sci. 2018, 19, 1804. [Google Scholar] [CrossRef] [PubMed]
- Kyono, Y.; Subramani, A.; Ramadoss, P.; Hollenberg, A.N.; Bonett, R.M.; Denver, R.J. Liganded Thyroid Hormone Receptors Transactivate the DNA Methyltransferase 3a Gene in Mouse Neuronal Cells. Endocrinology 2016, 157, 3647–3657. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.L. Minireview: Epigenomic Plasticity and Vulnerability to EDC Exposures. Mol. Endocrinol. 2016, 30, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Pitto, L.; Gorini, F.; Bianchi, F.; Guzzolino, E. New Insights into Mechanisms of Endocrine-Disrupting Chemicals in Thyroid Diseases: The Epigenetic Way. Int. J. Environ. Res. Public Health 2020, 17, 7787. [Google Scholar] [CrossRef]
- Alavian-Ghavanini, A.; Rüegg, J. Understanding Epigenetic Effects of Endocrine Disrupting Chemicals: From Mechanisms to Novel Test Methods. Basic Clin. Pharmacol. Toxicol. 2018, 122, 38–45. [Google Scholar] [CrossRef]
- Poston, R.G.; Saha, R.N. Epigenetic Effects of Polybrominated Diphenyl Ethers on Human Health. Int. J. Environ. Res. Public Health 2019, 16, 2703. [Google Scholar] [CrossRef]
- Hay, I.; Hynes, K.L.; Burgess, J.R. Mild-to-Moderate Gestational Iodine Deficiency Processing Disorder. Nutrients 2019, 11, 1974. [Google Scholar] [CrossRef]
- Thompson, W.; Russell, G.; Baragwanath, G.; Matthews, J.; Vaidya, B.; Thompson-Coon, J. Maternal thyroid hormone insufficiency during pregnancy and risk of neurodevelopmental disorders in offspring: A systematic review and meta-analysis. Clin. Endocrinol. 2018, 88, 575–584. [Google Scholar] [CrossRef]
- Pop, V.J.; Brouwers, E.P.; Vader, H.L.; Vulsma, T.; Van Baar, A.L.; De Vijlder, J.J. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: A 3-year follow-up study. Clin. Endocrinol. 2003, 59, 282–288. [Google Scholar] [CrossRef]
- Li, Y.; Shan, Z.; Teng, W.; Yu, X.; Li, Y.; Fan, C.; Teng, X.; Guo, R.; Wang, H.; Li, J.; et al. Abnormalities of maternal thyroid function during pregnancy affect neuropsychological development of their children at 25–30 months. Clin. Endocrinol. 2010, 72, 825–829. [Google Scholar] [CrossRef]
- Henrichs, J.; Bongers-Schokking, J.J.; Schenk, J.J.; Ghassabian, A.; Schmidt, H.G.; Visser, T.J.; Hooijkaas, H.; de Muinck Keizer-Schrama, S.M.; Hofman, A.; Jaddoe, V.V.; et al. Maternal thyroid function during early pregnancy and cognitive functioning in early childhood: The generation R study. J. Clin. Endocrinol. Metab. 2010, 95, 4227–4234. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.; Watson, J.; Ogston, S.; Hume, R.; Willatts, P.; Visser, T.; Scottish Preterm Thyroid Group. Mild maternal thyroid dysfunction at delivery of infants born ≤34 weeks and neurodevelopmental outcome at 5.5 years. J. Clin. Endocrinol. Metab. 2012, 97, 1977–1985. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.Y.; Allan, W.C.; Kloza, E.M.; Pulkkinen, A.J.; Waisbren, S.; Spratt, D.I.; Palomaki, G.E.; Neveux, L.M.; Haddow, J.E. Mid-gestational maternal free thyroxine concentration and offspring neurocognitive development at age two years. J. Clin. Endocrinol. Metab. 2012, 97, E22–E28. [Google Scholar] [CrossRef] [PubMed]
- Päkkilä, F.; Männistö, T.; Hartikainen, A.-L.; Ruokonen, A.; Surcel, H.-M.; Bloigu, A.; Vääräsmäki, M.; Järvelin, M.-R.; Moilanen, I.; Suvanto, E. Maternal and Child’s Thyroid Function and Child’s Intellect and Scholastic Performance. Thyroid 2015, 25, 1363–1374. [Google Scholar] [CrossRef]
- Grau, G.; Aguayo, A.; Vela, A.; Aniel-Quiroga, A.; Espada, M.; Miranda, G.; Martinez-Indart, L.; Martul, P.; Castaño, L.; Rica, I. Normal intellectual development in children born from women with hypothyroxinemia during their pregnancy. J. Trace Elem. Med. Biol. 2015, 31, 18–24. [Google Scholar] [CrossRef]
- Noten, A.M.; Loomans, E.M.; Vrijkotte, T.G.M.; van de Ven, P.M.; van Trotsenburg, A.S.P.; Rotteveel, J.; van Eijsden, M.; Finken, M.J.J. Maternal hypothyroxinaemia in early pregnancy and school performance in 5-year-old offspring. Eur. J. Endocrinol. 2015, 173, 563–571. [Google Scholar] [CrossRef]
- Kampouri, M.; Margetaki, K.; Koutra, K.; Kyriklaki, A.; Karakosta, P.; Anousaki, D.; Chalkiadaki, G.; Vafeiadi, M.; Kogevinas, M.; Chatzi, L. Maternal mild thyroid dysfunction and offspring cognitive and motor development from infancy to childhood: The Rhea mother-child cohort study in Crete, Greece. J. Epidemiol. Community Health 2021, 75, 29–35. [Google Scholar] [CrossRef]
- Andersen, S.L.; Andersen, S.; Liew, Z.; Vestergaard, P.; Olsen, J. Maternal Thyroid Function in Early Pregnancy and Neuropsychological Performance of the Child at 5 Years of Age. J. Clin. Endocrinol. Metab. 2018, 103, 660–670. [Google Scholar] [CrossRef]
- Chevrier, J.; Harley, K.G.; Kogut, K.; Holland, N.; Johnson, C.; Eskenazi, B. Maternal Thyroid Function during the Second Half of Pregnancy and Child Neurodevelopment at 6, 12, 24, and 60 Months of Age. J. Thyroid Res. 2011, 2011, 426427. [Google Scholar] [CrossRef]
- Fetene, D.M.; Betts, K.S.; Alati, R. Mechanisms in endocrinology: Maternal thyroid dysfunction during pregnancy and behavioural and psychiatric disorders of children: A systematic review. Eur. J. Endocrinol. 2017, 177, R261–R273. [Google Scholar] [CrossRef]
- Drover, S.S.M.; Villanger, G.D.; Aase, H.; Skogheim, T.S.; Longnecker, M.P.; Zoeller, R.T.; Reichborn-Kjennerud, T.; Knudsen, G.P.; Zeiner, P.; Engel, S.M. Maternal Thyroid Function During Pregnancy or Neonatal Thyroid Function and Attention Deficit Hyperactivity Disorder: A Systematic Review. Epidemiology 2019, 30, 130–144. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Wu, L. The impact of thyroid abnormalities during pregnancy on subsequent neuropsychological development of the offspring: A meta-analysis. J. Matern. Fetal Neonatal Med. 2016, 29, 3971–3976. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Gao, J.; Zhao, S.; Guo, Y.; Wang, Z.; Qi, F. Maternal Thyroxine Levels During Pregnancy and Outcomes of Cognitive Development in Children. Mol. Neurobiol. 2016, 53, 2241–2248. [Google Scholar] [CrossRef]
- Levie, D.; Korevaar, T.I.M.; Bath, S.C.; Murcia, M.; Dineva, M.; Llop, S.; Espada, M.; Van Herwaarden, A.E.; De Rijke, Y.B.; Ibarluzea, J.M.; et al. Association of Maternal Iodine Status with Child IQ: A Meta-Analysis of Individual Participant Data. J. Clin. Endocrinol. Metab. 2019, 104, 5957–5967. [Google Scholar] [CrossRef] [PubMed]
- Levie, D.; Korevaar, T.I.M.; Bath, S.; Dalmau-Bueno, A.; Murcia, M.; Espada, M.; Dineva, M.; Ibarluzea, J.M.; Sunyer, J.; Tiemeier, H.; et al. Thyroid Function in Early Pregnancy, Child IQ and Autistic Traits: A Meta-Analysis of Individual Participant Data. J. Clin. Endocrinol. Metab. 2018, 103, 2967–2979. [Google Scholar] [CrossRef] [PubMed]
- Leemans, M.; Couderq, S.; Demeneix, B.; Fini, J.-B. Pesticides with Potential Thyroid Hormone-Disrupting Effects: A Review of Recent Data. Front. Endocrinol. 2019, 10, 743. [Google Scholar] [CrossRef]
- Grova, N.; Schroeder, H.; Olivier, J.L.; Turner, J.D. Epigenetic and Neurological Impairments Associated with Early Life Exposure to Persistent Organic Pollutants. Int. J. Genom. 2019, 2019, 2085496. [Google Scholar] [CrossRef]
- Lenters, V.; Iszatt, N.; Forns, J.; Čechová, E.; Kočan, A.; Legler, J.; Leonards, P.; Stigum, H.; Eggesbø, M. Early-life exposure to persistent organic pollutants (OCPs, PBDEs, PCBs, PFASs) and attention-deficit/hyperactivity disorder: A multi-pollutant analysis of a Norwegian birth cohort. Environ. Int. 2019, 125, 33–42. [Google Scholar] [CrossRef]
- Rahman, M.; Shu, Y.-H.; Chow, T.; Lurmann, F.W.; Yu, X.; Martinez, M.P.; Carter, S.A.; Eckel, S.P.; Chen, J.-C.; Chen, Z.; et al. Prenatal Exposure to Air Pollution and Autism Spectrum Disorder: Sensitive Windows of Exposure and Sex Differences. Environ. Health Perspect. 2022, 130, 17008. [Google Scholar] [CrossRef]
- Vermiglio, F.; Presti, V.P.L.; Moleti, M.; Sidoti, M.; Tortorella, G.; Scaffidi, G.; Castagna, M.G.; Mattina, F.; Violi, M.A.; Crisà, A.; et al. Attention deficit and hyperactivity disorders in the offspring of mothers exposed to mild-moderate iodine deficiency: A possible novel iodine deficiency disorder in developed countries. J. Clin. Endocrinol. Metab. 2004, 89, 6054–6060. [Google Scholar] [CrossRef]
- Gaberšček, S.; Zaletel, K. Epidemiological trends of iodine-related thyroid disorders: An example from Slovenia. Arh. Hig. Rada Toksikol. 2016, 67, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Román, G.C. Autism: Transient in utero hypothyroxinemia related to maternal flavonoid ingestion during pregnancy and to other environmental antithyroid agents. J. Neurol. Sci. 2007, 262, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, T.A.; Peterson, M.K.; Charnley, G. Iodine supplementation and drinking-water perchlorate mitigation. Food Chem. Toxicol. 2015, 80, 261–270. [Google Scholar] [CrossRef]
- Leung, A.M.; Pearce, E.N.; Braverman, L.E. Environmental perchlorate exposure: Potential adverse thyroid effects. Curr Opin Endocrinol. Diabetes Obes. 2014, 21, 372–376. [Google Scholar] [CrossRef]
- Charatcharoenwitthaya, N.; Ongphiphadhanakul, B.; Pearce, E.N.; Somprasit, C.; Chanthasenanont, A.; He, X.; Chailurkit, L.; Braverman, L.E. The association between perchlorate and thiocyanate exposure and thyroid function in first-trimester pregnant Thai women. J. Clin. Endocrinol. Metab. 2014, 99, 2365–2371. [Google Scholar] [CrossRef] [PubMed]
- Ozpinar, A.; Kelestimur, F.; Songur, Y.; Can, O.; Valentin, L.; Caldwell, K.; Arikan, E.; Ünsal, I.; Serteser, M.; Inal, T.; et al. Iodine status in Turkish populations and exposure to iodide uptake inhibitors. PLoS ONE 2014, 9, e88206. [Google Scholar] [CrossRef] [PubMed]
- Suh, M.; Abraham, L.; Hixon, J.G.; Proctor, D.M. The effects of perchlorate, nitrate, and thiocyanate on free thyroxine for potentially sensitive subpopulations of the 2001–2002 and 2007–2008 National Health and Nutrition Examination Surveys. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Lumen, A.; Mattie, D.R.; Fisher, J.W. Evaluation of perturbations in serum thyroid hormones during human pregnancy due to dietary iodide and perchlorate exposure using a biologically based dose-response model. Toxicol. Sci. 2013, 133, 320–341. [Google Scholar] [CrossRef]
- Breous, E.; Wenzel, A.; Loos, U. The promoter of the human sodium/iodide symporter responds to certain phthalate plasticisers. Mol. Cell. Endocrinol. 2005, 244, 75–78. [Google Scholar] [CrossRef]
- Liu, C.; Zhao, L.; Wei, L.; Li, L. DEHP reduces thyroid hormones via interacting with hormone synthesis-related proteins, deiodinases, transthyretin, receptors, and hepatic enzymes in rats. Environ. Sci. Pollut. Res. Int. 2015, 22, 12711–12719. [Google Scholar] [CrossRef]
- Villanger, G.D.; Drover, S.S.; Nethery, R.C.; Thomsen, C.; Sakhi, A.K.; Øvergaard, K.R.; Zeiner, P.; Hoppin, J.; Reichborn-Kjennerud, T.; Aase, H.; et al. Associations between urine phthalate metabolites and thyroid function in pregnant women and the influence of iodine status. Environ. Int. 2020, 137, 105509. [Google Scholar] [CrossRef] [PubMed]
- Kamai, E.M.; Villanger, G.D.; Nethery, R.C.; Thomsen, C.; Sakhi, A.K.; Drover, S.S.M.; Hoppin, J.A.; Knudsen, G.P.; Reichborn-Kjennerud, T.; Zeiner, P.; et al. Gestational Phthalate Exposure and Preschool Attention Deficit Hyperactivity Disorder in Norway. Environ. Epidemiol. 2021, 5, e161. [Google Scholar]
- Merced-Nieves, F.M.; Dzwilewski, K.L.C.; Aguiar, A.; Musaad, S.; Korrick, S.A.; Schantz, S.L. Associations of Prenatal Exposure to Phthalates with Measures of Cognition in 4.5-Month-Old Infants. Int. J. Environ. Res. Public Health 2021, 18, 1838. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, A.; Nazareth, L.; Kaleta, D.; Polanska, K. Review of the Existing Evidence for Sex-Specific Relationships between Prenatal Phthalate Exposure and Children’s Neurodevelopment. Int. J. Environ. Res. Public Health 2021, 18, 13013. [Google Scholar] [CrossRef] [PubMed]
- Lucaccioni, L.; Trevisani, V.; Passini, E.; Righi, B.; Plessi, C.; Predieri, B.; Iughetti, L. Perinatal Exposure to Phthalates: From Endocrine to Neurodevelopment Effects. Int. J. Mol. Sci. 2021, 22, 4063. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.E.; Webster, G.M.; Vuong, A.M.; Zoeller, R.T.; Chen, A.; Hoofnagle, A.N.; Calafat, A.M.; Karagas, M.R.; Yolton, K.; Lanphear, B.P.; et al. Gestational urinary bisphenol A and maternal and newborn thyroid hormone concentrations: The HOME Study. Environ. Res. 2015, 138, 453–460. [Google Scholar] [CrossRef]
- Wang, X.; Tang, N.; Nakayama, S.F.; Fan, P.; Liu, Z.; Zhang, J.; Ouyang, F. Maternal urinary bisphenol A concentration and thyroid hormone levels of Chinese mothers and newborns by maternal body mass index. Environ. Sci. Pollut. Res. Int. 2020, 27, 10939–10949. [Google Scholar] [CrossRef]
- Li, F.; Yang, F.; Li, D.-K.; Tian, Y.; Miao, M.; Zhang, Y.; Ji, H.; Yuan, W.; Liang, H. Prenatal bisphenol A exposure, fetal thyroid hormones and neurobehavioral development in children at 2 and 4 years: A prospective cohort study. Sci. Total Environ. 2020, 722, 137887. [Google Scholar] [CrossRef]
- Braun, J.M.; Yolton, K.; Stacy, S.L.; Erar, B.; Papandonatos, G.D.; Bellinger, D.C.; Lanphear, B.P.; Chen, A. Prenatal environmental chemical exposures and longitudinal patterns of child neurobehavior. Neurotoxicology 2017, 62, 192–199. [Google Scholar] [CrossRef]
- Lim, Y.-H.; Bae, S.; Kim, B.-N.; Shin, C.H.; Lee, Y.A.; Kim, J.I.; Hong, Y.-C. Prenatal and postnatal bisphenol A exposure and social impairment in 4-year-old children. Environ. Health 2017, 16, 79. [Google Scholar] [CrossRef]
- Ejaredar, M.; Lee, Y.; Roberts, D.J.; Sauve, R.; Dewey, D. Bisphenol A exposure and children’s behavior: A systematic review. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Koutaki, D.; Paltoglou, G.; Vourdoumpa, A.; Charmandari, E. The Impact of Bisphenol A on Thyroid Function in Neonates and Children: A Systematic Review of the Literature. Nutrients 2021, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Minatoya, M.; Kishi, R. A Review of Recent Studies on Bisphenol A and Phthalate Exposures and Child Neurodevelopment. Int. J. Environ. Res. Public Health 2021, 18, 3585. [Google Scholar] [CrossRef] [PubMed]
- Brucker-Davis, F.; Ganier-Chauliac, F.; Gal, J.; Panaïa-Ferrari, P.; Pacini, P.; Fénichel, P.; Hiéronimus, S. Neurotoxicant exposure during pregnancy is a confounder for assessment of iodine supplementation on neurodevelopment outcome. Neurotoxicol. Teratol. 2015, 51, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Torres-Sánchez, L.; Gamboa, R.; Bassol-Mayagoitia, S.; Huesca-Gómez, C.; Nava, M.P.; Vázquez-Potisek, J.I.; Yáñez-Estrada, L.; Mejía-Saucedo, R.; Blanco-Muñoz, J. Para-occupational exposure to pesticides, PON1 polymorphisms and hypothyroxinemia during the first half of pregnancy in women living in a Mexican floricultural area. Environ. Health 2019, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Eskenazi, B.; An, S.; Rauch, S.A.; Coker, E.S.; Maphula, A.; Obida, M.; Crause, M.; Kogut, K.R.; Bornman, R.; Chevrier, J. Prenatal Exposure to DDT and Pyrethroids for Malaria Control and Child Neurodevelopment: The VHEMBE Cohort, South Africa. Environ. Health Perspect. 2018, 126, 047004, Erratum in Environ. Health Perspect. 2018, 126, 119001; Erratum in Environ. Health Perspect. 2020, 128, 39001. [Google Scholar] [CrossRef] [PubMed]
- Chevrier, J.; Rauch, S.; Obida, M.; Crause, M.; Bornman, R.; Eskenazi, B. Sex and poverty modify associations between maternal peripartum concentrations of DDT/E and pyrethroid metabolites and thyroid hormone levels in neonates participating in the VHEMBE study, South Africa. Environ. Int. 2019, 131, 104958. [Google Scholar] [CrossRef]
- Steinmaus, C.; Pearl, M.; Kharrazi, M.; Blount, B.C.; Miller, M.D.; Pearce, E.N.; Valentin-Blasini, L.; DeLorenze, G.; Hoofnagle, A.N.; Liaw, J. Thyroid Hormones and Moderate Exposure to Perchlorate during Pregnancy in Women in Southern California. Environ. Health Perspect. 2016, 124, 861–867. [Google Scholar] [CrossRef]
- Cowell, W.J.; Sjödin, A.; Jones, R.; Wang, Y.; Wang, S.; Whyatt, R.M.; Factor-Litvak, P.; Bradwin, G.; Hassoun, A.; Oberfield, S.; et al. Pre- and Postnatal Polybrominated Diphenyl Ether Concentrations in Relation to Thyroid Parameters Measured During Early Childhood. Thyroid 2019, 29, 631–641. [Google Scholar] [CrossRef]
- Jedynak, P.; Maitre, L.; Guxens, M.; Gützkow, K.B.; Julvez, J.; López-Vicente, M.; Sunyer, J.; Casas, M.; Chatzi, L.; Gražulevičienė, R.; et al. Prenatal exposure to a wide range of environmental chemicals and child behaviour between 3 and 7 years of age—An exposome-based approach in 5 European cohorts. Sci. Total Environ. 2021, 763, 144115. [Google Scholar] [CrossRef]
- Leko, M.B.; Gunjača, I.; Pleić, N.; Zemunik, T. Environmental Factors Affecting Thyroid-Stimulating Hormone and Thyroid Hormone Levels. Int. J. Mol. Sci. 2021, 22, 6521. [Google Scholar] [CrossRef] [PubMed]
- Ho, V.; Pelland-St-Pierre, L.; Gravel, S.; Bouchard, M.; Verner, M.-A.; Labrèche, F. Endocrine disruptors: Challenges and future directions in epidemiologic research. Environ. Res. 2022, 204 Pt A, 111969. [Google Scholar] [CrossRef]
- Salazar, P.; Villaseca, P.; Cisternas, P.; Inestrosa, N.C. Neurodevelopmental impact of the offspring by thyroid hormone system-disrupting environmental chemicals during pregnancy. Environ. Res. 2021, 200, 111345. [Google Scholar] [CrossRef] [PubMed]
- Gheidarloo, M.; Kelishadi, R.; Hovsepian, S.; Keikha, M.; Hashemipour, M. The association between prenatal exposure to organochlorine compounds and neonatal thyroid hormone levels: A systematic review. J. Pediatr. Endocrinol. Metab. 2020, 33, 21–33. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide: Executive Summary; World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/handle/10665/345334 (accessed on 1 April 2022).
- WHO. Fact Sheets 22 September 2021 Ambient (Outdoor) Air Quality and Health; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/en/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 30 September 2021).
- Burnett, R.; Chen, H.; Szyszkowicz, M.; Fann, N.; Hubbell, B.; Pope, C.A., 3rd; Apte, J.S.; Brauer, M.; Cohen, A.; Weichenthal, S.; et al. Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc. Natl. Acad. Sci. USA 2018, 115, 9592–9597. [Google Scholar] [CrossRef] [PubMed]
- Marty, M.A.; Perera, F.; Miller, M.D.; Swanson, M.; Ellickson, K.; Cory-Slechta, D.A.; Ritz, B.; Balmes, J.; Anderko, L.; Talbott, E.O.; et al. Healthy Air, Healthy Brains: Advancing Air Pollution Policy to Protect Children’s Health. Am. J. Public Health 2019, 109, 550–554. [Google Scholar] [CrossRef]
- Loftus, C.T.; Ni, Y.; Szpiro, A.A.; Hazlehurst, M.F.; Tylavsky, F.A.; Bush, N.R.; Sathyanarayana, S.; Carroll, K.N.; Young, M.; Karr, C.J.; et al. Exposure to ambient air pollution and early childhood behavior: A longitudinal cohort study. Environ. Res. 2020, 183, 109075. [Google Scholar] [CrossRef]
- Peterson, B.S.; Rauh, V.A.; Bansal, R.; Hao, X.; Toth, Z.; Nati, G.; Walsh, K.; Miller, R.L.; Arias, F.; Semanek, D.; et al. Effects of prenatal exposure to air pollutants (polycyclic aromatic hydrocarbons) on the development of brain white matter, cognition, and behavior in later childhood. JAMA Psychiatry 2015, 72, 531–540. [Google Scholar] [CrossRef]
- Zhao, Y.; Cao, Z.; Li, H.; Su, X.; Yang, Y.; Liu, C.; Hua, J. Air pollution exposure in association with maternal thyroid function during early pregnancy. J. Hazard. Mater. 2019, 367, 188–193. [Google Scholar] [CrossRef]
- Charoenratana, C.; Leelapat, P.; Traisrisilp, K.; Tongsong, T. Maternal iodine insufficiency and adverse pregnancy outcomes. Matern. Child Nutr. 2016, 12, 680–687. [Google Scholar] [CrossRef]
- Holland, E.B.; Pessah, I.N. Non-dioxin-like polychlorinated biphenyl neurotoxic equivalents found in environmental and human samples. Regul. Toxicol. Pharmacol. 2021, 120, 104842. [Google Scholar] [CrossRef] [PubMed]
- Block, M.L.; Elder, A.; Auten, R.L.; Bilbo, S.D.; Chen, H.; Chen, J.-C.; Cory-Slechta, D.A.; Costa, D.; Diaz-Sanchez, D.; Dorman, D.C.; et al. The outdoor air pollution and brain health workshop. Neurotoxicology 2012, 33, 972–984. [Google Scholar] [CrossRef] [PubMed]
- Lubczyńska, M.J.; Muetzel, R.L.; El Marroun, H.; Basagaña, X.; Strak, M.; Denault, W.; Jaddoe, V.W.; Hillegers, M.; Vernooij, M.W.; Hoek, G.; et al. Exposure to Air Pollution during Pregnancy and Childhood, and White Matter Microstructure in Preadolescents. Environ. Health Perspect. 2020, 128, 27005. [Google Scholar] [CrossRef] [PubMed]
- Guxens, M.; Lubczyńska, M.J.; Muetzel, R.L.; Dalmau-Bueno, A.; Jaddoe, V.W.; Hoek, G.; van der Lugt, A.; Verhulst, F.C.; White, T.; Brunekreef, B.; et al. Air Pollution Exposure During Fetal Life, Brain Morphology, and Cognitive Function in School-Age Children. Biol. Psychiatry 2018, 84, 295–303. [Google Scholar] [CrossRef]
- Guxens, M.; Garcia-Esteban, R.; Giorgis-Allemand, L.; Forns, J.; Badaloni, C.; Ballester, F.; Beelen, R.; Cesaroni, G.; Chatzi, L.; de Agostini, M.; et al. Air pollution during pregnancy and childhood cognitive and psychomotor development: Six European birth cohorts. Epidemiology 2014, 25, 636–647. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Park, H.; Hong, Y.-C.; Ha, M.; Kim, Y.; Kim, B.-N.; Kim, Y.; Roh, Y.-M.; Lee, B.-E.; Ryu, J.-M.; et al. Prenatal exposure to PM10 and NO2 and children’s neurodevelopment from birth to 24 months of age: Mothers and Children’s Environmental Health (MOCEH) study. Sci. Total Environ. 2014, 481, 439–445. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; Mora-Tiscareño, A.; Franco-Lira, M.; Zhu, H.; Lu, Z.; Solorio, E.; Torres-Jardón, R.; D’Angiulli, A. Decreases in Short Term Memory, IQ, and Altered Brain Metabolic Ratios in Urban Apolipoprotein ε4 Children Exposed to Air Pollution. J. Alzheimer’s Dis. 2015, 45, 757–770. [Google Scholar] [CrossRef]
- Chiu, Y.-H.M.; Hsu, H.-H.L.; Coull, B.A.; Bellinger, D.C.; Kloog, I.; Schwartz, J.; Wright, R.O.; Wright, R.J. Prenatal particulate air pollution and neurodevelopment in urban children: Examining sensitive windows and sex-specific associations. Environ. Int. 2016, 87, 56–65. [Google Scholar] [CrossRef]
- Lam, J.; Sutton, P.; Kalkbrenner, A.; Windham, G.; Halladay, A.; Koustas, E.; Lawler, C.; Davidson, L.; Daniels, N.; Newschaffer, C.; et al. A Systematic Review and Meta-Analysis of Multiple Airborne Pollutants and Autism Spectrum Disorder. PLoS ONE 2016, 11, e0161851. [Google Scholar] [CrossRef]
- Kalkbrenner, A.E.; Windham, G.C.; Serre, M.L.; Akita, Y.; Wang, X.; Hoffman, K.; Thayer, B.P.; Daniels, J.L. Particulate matter exposure, prenatal and postnatal windows of susceptibility, and autism spectrum disorders. Epidemiology 2015, 26, 30–42. [Google Scholar] [CrossRef]
- Volk, H.E.; Lurmann, F.; Penfold, B.; Hertz-Picciotto, I.; McConnell, R. Traffic-related air pollution, particulate matter, and autism. JAMA Psychiatry 2013, 70, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Clifford, A.; Lang, L.; Chen, R.; Anstey, K.J.; Seaton, A. Exposure to air pollution and cognitive functioning across the life course—A systematic literature review. Environ. Res. 2016, 147, 383–398. [Google Scholar] [CrossRef] [PubMed]
- Gong, T.; Dalman, C.; Wicks, S.; Dal, H.; Magnusson, C.; Lundholm, C.; Almqvist, C.; Pershagen, G. Perinatal Exposure to Traffic-Related Air Pollution and Autism Spectrum Disorders. Environ. Health Perspect. 2017, 125, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Luminati, O.; Brentani, A.; Flückiger, B.; Ledebur de Antas de Campos, B.; Raess, M.; Röösli, M.; de Hoogh, K.; Fink, G. Assessing the association between air pollution and child development in São Paulo, Brazil. PLoS ONE 2022, 17, e0268192. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Pearce, E.N. Testing, Monitoring, and Treatment of Thyroid Dysfunction in Pregnancy. J. Clin. Endocrinol. Metab. 2021, 106, 883–892. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.M. No Benefit of Levothyroxine Among Pregnant Hypothyroid and/or Hypothyroxinemic Women on Offspring IQ at Age 9 years. Clin. Thyroidol. 2018, 30, 100–103. [Google Scholar] [CrossRef]
- Runkle, I.; de Miguel, M.P.; Barabash, A.; Cuesta, M.; Diaz, Á.; Duran, A.; Familiar, C.; de la Torre, N.G.; Herraiz, M.Á.; Izquierdo, N.; et al. Early Levothyroxine Treatment for Subclinical Hypothyroidism or Hypothyroxinemia in Pregnancy: The St Carlos Gestational and Thyroid Protocol. Front. Endocrinol. 2021, 12, 743057. [Google Scholar] [CrossRef] [PubMed]
- Young, A.E.; Kemp, J.F.; Uhlson, C.; Westcott, J.L.; Ali, S.A.; Saleem, S.; Garcès, A.; Figueroa, L.; Somannavar, M.S.; Goudar, S.S.; et al. Women First Preconception Maternal Nutrition Trial Group. Improved first trimester maternal iodine status with preconception supplementation: The Women First Trial. Matern. Child Nutr. 2021, 17, e13204. [Google Scholar] [CrossRef]
- Berbel, P.; Mestre, J.L.; Santamaría, A.; Palazón, I.; Franco, A.; Graells, M.; González-Torga, A.; De Escobar, G.M. Delayed neurobehavioral development in children born to pregnant women with mild hypothyroxinemia during the first month of gestation: The importance of early iodine supplementation. Thyroid 2009, 19, 511–519. [Google Scholar] [CrossRef]
- Dineva, M.; Fishpool, H.; Rayman, M.P.; Mendis, J.; Bath, S.C. Systematic review and meta-analysis of the effects of iodine supplementation on thyroid function and child neurodevelopment in mildly-to-moderately iodine-deficient pregnant women. Am. J. Clin. Nutr. 2020, 112, 389–412. [Google Scholar] [CrossRef]
- Robinson, S.M.; Crozier, S.R.; Miles, E.A.; Gale, C.R.; Calder, P.C.; Cooper, C.; Inskip, H.M.; Godfrey, K.M. Preconception Maternal Iodine Status Is Positively Associated with IQ but Not with Measures of Executive Function in Childhood. J. Nutr. 2018, 148, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Moleti, M.; Presti, V.P.L.; Campolo, M.C.; Mattina, F.; Galletti, M.; Mandolfino, M.; Violi, M.A.; Giorgianni, G.; De Domenico, D.; Trimarchi, F.; et al. Iodine prophylaxis using iodized salt and risk of maternal thyroid failure in conditions of mild iodine deficiency. J. Clin. Endocrinol. Metab. 2008, 93, 2616–2621. [Google Scholar] [CrossRef] [PubMed]
- Nussey, S.; Whitehead, S. Endocrinology: An Integrated Approach; BIOS Scientific Publishers: Oxford, UK, 2001. Available online: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?call=bv.View.ShowTOC&rid=endocrin.TOC&depth=1 (accessed on 1 April 2022).
- Hynes, K.L.; Seal, J.A.; Otahal, P.; Oddy, W.H.; Burgess, J.R. Women Remain at Risk of Iodine Deficiency during Pregnancy: The Importance of Iodine Supplementation before Conception and Throughout Gestation. Nutrients 2019, 11, 172. [Google Scholar] [CrossRef]
- Machamba, A.A.L.; Azevedo, F.M.; Fracalossi, K.O.; Franceschini, S.D.C.C. Effect of iodine supplementation in pregnancy on neurocognitive development on offspring in iodine deficiency areas: A systematic review. Arch. Endocrinol. Metab. 2021, 65, 352–367. [Google Scholar] [CrossRef]
- Nazeri, P.; Shariat, M.; Azizi, F. Effects of iodine supplementation during pregnancy on pregnant women and their offspring: A systematic review and meta-analysis of trials over the past 3 decades. Eur. J. Endocrinol. 2021, 184, 91–106. [Google Scholar] [CrossRef] [PubMed]
- Harding, K.B.; Peña-Rosas, J.P.; Webster, A.C.; Yap, C.M.Y.; Payne, B.A.; Ota, E.; De-Regil, L.M. Iodine supplementation for women during the preconception, pregnancy and postpartum period. Cochrane Database Syst. Rev. 2017, 3, CD011761. [Google Scholar] [CrossRef]
- Verhagen, N.J.E.; Gowachirapant, S.; Winichagoon, P.; Andersson, M.; Melse-Boonstra, A.; Zimmermann, M.B. Iodine Supplementation in Mildly Iodine-Deficient Pregnant Women Does Not Improve Maternal Thyroid Function or Child Development: A Secondary Analysis of a Randomized Controlled Trial. Front. Endocrinol. 2020, 11, 572984. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.H.; Korevaar, T.I.; Erlund, I.; Villanger, G.D.; Caspersen, I.H.; Arohonka, P.; Alexander, J.; Meltzer, H.M.; Brantsaeter, A.L. Iodine Intake is Associated with Thyroid Function in Mild to Moderately Iodine Deficient Pregnant Women. Thyroid 2018, 28, 1359–1371. [Google Scholar] [CrossRef] [PubMed]
- Pearce, E.N.; Lazarus, J.H.; Moreno-Reyes, R.; Zimmermann, M.B. Consequences of iodine deficiency and excess in pregnant women: An overview of current knowns and unknowns. Am. J. Clin. Nutr. 2016, 104 (Suppl. S3), 918S–923S. [Google Scholar] [CrossRef]
- Manousou, S.; Eggertsen, R.; Hulthén, L.; Nyström, H.F. A randomized, double-blind study of iodine supplementation during pregnancy in Sweden: Pilot evaluation of maternal iodine status and thyroid function. Eur. J. Nutr. 2021, 60, 3411–3422. [Google Scholar] [CrossRef]
- Lopes-Pereira, M.; Roque, S.; Costa, P.; Quialheiro, A.; Santos, N.C.; Goios, A.; Vilarinho, L.; Correia-Neves, M.; Palha, J.A. Impact of iodine supplementation during preconception, pregnancy and lactation on maternal thyroid homeostasis and offspring psychomotor development: Protocol of the IodineMinho prospective study. BMC Pregnancy Childbirth 2020, 20, 693. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.A.; Ross, A.P.; Goodman, G. Assessing infant cognitive development after prenatal iodine supplementation. Am. J. Clin. Nutr. 2016, 104 (Suppl. S3), 928S–934S. [Google Scholar] [CrossRef] [PubMed]
- Troendle, J.F. Statistical design considerations applicable to clinical trials of iodine supplementation in pregnant women who may be mildly iodine deficient. Am. J. Clin. Nutr. 2016, 104 (Suppl. S3), 924S–927S. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Han, C.; Li, C.; Mao, J.; Wang, W.; Xie, X.; Li, C.; Xu, B.; Meng, T.; Du, J.; et al. Optimal and safe upper limits of iodine intake for early pregnancy in iodine-sufficient regions: A cross-sectional study of 7190 pregnant women in China. J. Clin. Endocrinol. Metab. 2015, 100, 1630–1638. [Google Scholar] [CrossRef] [PubMed]
- Schaffner, M.; Mühlberger, N.; Conrads-Frank, A.; Rushaj, V.Q.; Sroczynski, G.; Koukkou, E.; Thuesen, B.H.; Völzke, H.; Oberaigner, W.; Siebert, U.; et al. Benefits and Harms of a Prevention Program for Iodine Deficiency Disorders: Predictions of the Decision-Analytic EUthyroid Model. Thyroid 2021, 31, 494–508. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Country | General Population a | Pregnant Women b | ||||||
|---|---|---|---|---|---|---|---|---|
| Median (UIC) (μg/L) | Date of Survey (N, S) | Population | Population Iodine Intake | Median (UIC) (μg/L) | Date of Survey (N, S) | Iodine Intake | Legislation Status e (Year) | |
| Austria | 111 | 2012 (N) | SAC (7–14) | Adequate | 87 | 2009–2011 (S) | Insufficient | Mandatory (1999) |
| Belgium | 113 | 2010/11 (N) | SAC (6–12) | Adequate | 124 | 2010 (N) | Insufficient | Voluntary (2009) |
| Bulgaria | 182 | 2008 (N) | SAC (7–11) | Adequate | 165 | 2003 (N) | Adequate | Mandatory (2001) |
| Croatia | 248 | 2009 (N) | SAC (7–11) | Adequate | 140 | 2009, 2015 (S) | Insufficient | Mandatory (1996) |
| Denmark | 145 | 2015 (S) | SAC | Adequate | 101 | 2012 (S) | Insufficient | Mandatory (2000) f |
| Finland | 96 | 2017 (N) | Adults (25–74) | Insufficient | 115 | 2013–2017 (S) f | Insufficient | Voluntary f |
| France | 136 | 2006–2007 (N) | Adults (18–74) | Adequate | 65 | 2006–2009 (S) | Insufficient | Voluntary |
| Germany | 89 | 2014–2017 (N) | SAC, Adolescent (6–12) | Insufficient | 54 | 2008–2011 (N) c | Insufficient | Voluntary |
| Greece | 132 | 2018 (N) | Adults | Adequate | 127 | 2008–2015 (S) | Insufficient | Voluntary |
| Hungary | 228 | 2005 (S) | SAC (10–14) | Adequate | 128 | 2018 (S) d | Insufficient | Mandatory (2013) |
| Ireland | 111 | 2014–2015 (N) | Adolescent girls (14–15) | Adequate | 107 | 2008–2010 (S) | Insufficient | Voluntary |
| Italy | 118 | 2015–2019 (S) | SAC | Adequate | 72 | 2002–2013 (S) | Insufficient | Mandatory (2005) |
| Netherlands | 130 | 2006 (S) | Adults (50–72) | Adequate | 223 | 2002–2006 (S) | Adequate | Voluntary |
| Poland | 112 | 2009–2011 (S) | SAC (6–12) | Adequate | 113 | 2007–2008 (S) | Insufficient | Mandatory (2010) |
| Portugal | 106 | 2010 (N) | SAC | Adequate | 85 | 2005–2007 (N) | Insufficient | Voluntary |
| Romania | 255 | 2015–2016 (N) | SAC (6–11) | Adequate | 206 | 2016 (S) | Adequate | Mandatory (2009) |
| Spain | 173 | 2011–2012 (N) | SAC | Adequate | 120 | 2002–2011 (S) | Insufficient | Voluntary |
| Sweden | 125 | 2006–2007 (N) | SAC (6–12) | Adequate | 98 | 2006–2007; 2010–2012 (S) | Insufficient | Voluntary (1936) f |
| Switzerland | 137 | 2015 (N) | SAC (6–12) | Adequate | 136 | 2015 (N) | Insufficient | Voluntary |
| United Kingdom | 166 | 2015–2016 (N) | SAC, Adolescent (4–18) | Adequate | 99 | 2002–2011 (S) | Insufficient | no USI-program |
| Examples of Chemicals | Target of TDCs Action and Results | Neurodevelopmental Alterations |
|---|---|---|
| Organochlorine pesticides (OCPs) 1 Polychlorinated biphenyl compounds (PCBs) 2 | TSH receptor signaling and decreased stimulation of thyrocytes [105]. | |
| Perchlorate 3 Thiocyanate 3 Nitrate 3 Phthalates 4 | Na+/I− symporter (NIS) and inhibition of TH biosynthesis. | |
| Propylthiouracil (PTU) Methimazole (MMI) Genistein 5 4-Nonylphenol (NP) 6 Benzophenone 2 (BP2) 7 Pesticide (Amitrole) 8 | Inhibition of thyroid peroxidase (TPO) results in decreased TH synthesis and subsequent reduction in circulating concentrations of THs. | |
| OH-PCBs 2 Polybrominated diphenyl ethers (PBDEs) 9 Phthalates 4 Genistein 5 | TH-distributor proteins: displacement of T4 and T3 by thyroid serum binding protein transthyretin (TTR) and/or thyroid binding globulin (TBG) disturbs the TH homeostasis and decreases plasma TH levels. |
|
| Polychlorinated biphenyls (PCBs, OH-PCBs) 2 Triclosan 10 | Upregulation of thyroid hormone catabolism via the activation of hepatic nuclear receptors leads to a decrease in circulating TH levels [93,148]. | |
| Silymarin 11 | Interference with cellular transmembrane transporters (MCT8, MCT10 and OATP1C1) inhibits T3 uptake. |
|
| Erythrosine 12 6 propylthiouracil PCBs 2 | Modification of the deiodinase enzyme activities (DIO2, DIO3) by competitive inhibition of the enzyme or by interaction with its sulfhydryl cofactor. |
|
| Author, Year [Reference] | Total Number of Participants Tested for Outcome | Country | Maternal Thyroid Dysfunction | Gestation at TFT | Criteria for Thyroid Dysfunction | Child Age at Assessment | Neurodevelopmental Outcome Measures |
|---|---|---|---|---|---|---|---|
| Pop et al., 1999 [68] | 220 | The Netherlands | HR | 12 and 32 weeks | 10th percentile fT4 (<10.4 pmol/L) and fifth percentile fT4 (<9.8 pmol/L) | 10 months | Bayley Scales of Infant Development |
| Pop et al., 2003 [181] | 125 | The Netherlands | HR | 12, 24 and 32 weeks | fT4 <10th Percentile (12.10 pmol/L) | 1–2 years | Bayley Scale of Infant Development |
| Kasatkina et al., 2006 [95] | 35 | Russia | HR | 1st and 3rd trimesters | fT4 < 12.0 pmol/L | 6, 9 and 12 months | Gnome method, in particular, the Coefficient of Mental Development |
| Li et al., 2010 [182] | 213 | China | SH and HR | 16 to 20 weeks | SH = TSH > 97.50th percentile (4.21 mU/L), HR = tT4 < 2.50th percentile (101.79 nmol/L) | 25–30 months | Bayley Scale of Infant Development |
| Henrichs et al., 2010 [183] | 3659 | The Netherlands | HR and Co TSH | 13.3 weeks | HR = fT4 10th percentile (<11.76 pmol/L) and fifth percentile (<10.96 pmol/L), Co TSH = TSH ref range 0.03–2.50 mU/L | 18 and 30 months | MacArthur Communicative Development Inventory at 18 months, Language Development Survey at 30 months |
| Suárez-Rodríguez et al., 2012 [94] | 70 | Spain | HR | 37 weeks | fT4 < 10th percentile (9.5 pmol/L) | 38 months and 5 years | The McCarthy Scales of Children’s Abilities |
| Williams et al., 2012 [184] | 166 | UK | SH and HR | ±1 h after birth | SH = TSH > 3.0 mU/L, HR = fT4 ≤ 10th percentile (11.6 pmol/L) or tT4 ≤10th percentile (108.4 nmol/L) | 5.5 years | The McCarthy Scales of Children’s Abilities |
| Craig et al., 2012 [185] | 196 | USA | HR | 2nd trimester | fT4 < 3rd Percentile (11.84 pmol/L) | 2 years | Bayley’s Scale of Infant Development III |
| Ghassabian et al., 2014 [93]/Korevaar et al., 2016 [96] | 3737/5647 | The Netherlands | HR and SH | 13.5/13.2 weeks | HR = fT4 < 5th percentile (10.99 pmol/L), SH= TSH > 2.50 mU/L | 6 years | Snijders-Oomen Niet-verbale intelligence test, revisie (Mosaics and Categories) |
| Päkkilä et al., 2015 [186] | 5295 | Finland | HR, SH and OH | Mean 10.7 weeks | HR = fT4 < 11.4–11.09 pmol/L depending upon trimester, SH = TSH > 3.10–3.50 mU/L depending upon trimester | 8 and 16 years | Strengths and Weaknesses of ADHD Symptoms and Normal Behavior, Teacher reported child school performance, Youth Self Report and WISC-Revised |
| Grau et al., 2015 [187] | 455 | Spain | HR | 1st and 2nd trimesters | <10th Percentile (13.7–11.5 pmol/L depending on trimester) | 1 and 6–8 years | Brunet-Lezine scale and WISC-IV |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grossklaus, R.; Liesenkötter, K.-P.; Doubek, K.; Völzke, H.; Gaertner, R. Iodine Deficiency, Maternal Hypothyroxinemia and Endocrine Disrupters Affecting Fetal Brain Development: A Scoping Review. Nutrients 2023, 15, 2249. https://doi.org/10.3390/nu15102249
Grossklaus R, Liesenkötter K-P, Doubek K, Völzke H, Gaertner R. Iodine Deficiency, Maternal Hypothyroxinemia and Endocrine Disrupters Affecting Fetal Brain Development: A Scoping Review. Nutrients. 2023; 15(10):2249. https://doi.org/10.3390/nu15102249
Chicago/Turabian StyleGrossklaus, Rolf, Klaus-Peter Liesenkötter, Klaus Doubek, Henry Völzke, and Roland Gaertner. 2023. "Iodine Deficiency, Maternal Hypothyroxinemia and Endocrine Disrupters Affecting Fetal Brain Development: A Scoping Review" Nutrients 15, no. 10: 2249. https://doi.org/10.3390/nu15102249