
Parent’s Perception of the Types of Support Given to Families with an Infant with Phenylketonuria
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire
2.2. Data Analysis
2.3. Ethical Approval
3. Results
3.1. Demographic Data
3.2. Initial Feelings on Diagnosis of PKU
3.3. Support from and Trust in Healthcare Professionals
- “It is absolutely crucial to have a consistent person to deal with when learning about PKU. Someone who actually knows your family and the child with PKU.”
- “GPs don’t know what PKU is. I feel I have to inform them when I see them.”
- “The support from the health visitor did not extend to making any effort to understand PKU or what that might mean. There appeared to be no attempt to liaise with the hospital.”
- “There was no emotional support and no follow up at all regarding my own well-being.”
3.4. Where Parents Go for Support and Information
3.5. Use of Social Media for Support and Information
3.6. Preferred Method of Obtaining Dietary Information
- “I prefer to do things through my dietitian. We feel safe this way.”
- “Early on I preferred to have the dietitian there throughout the process, but with time I do feel more confident to do my own research.”
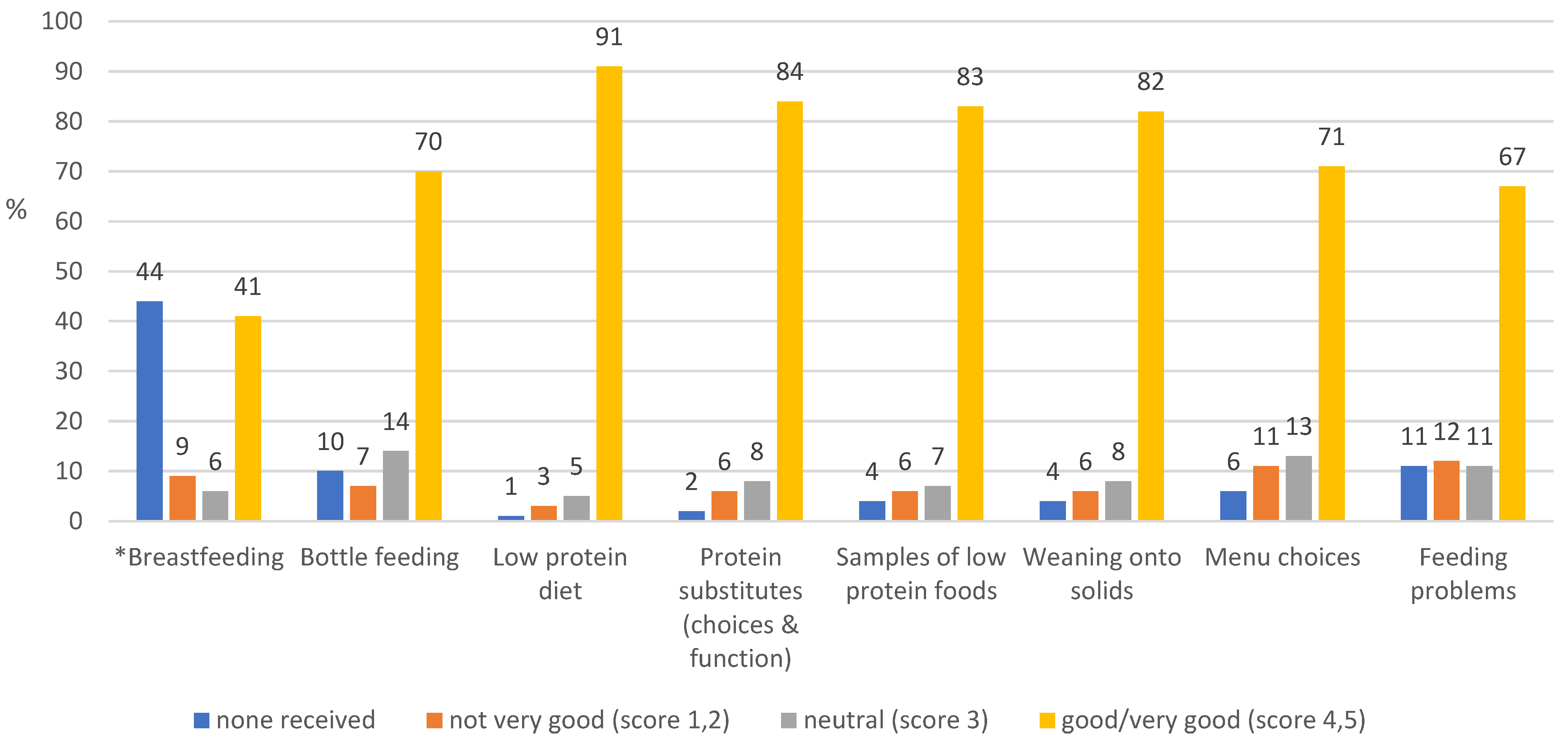
3.7. Early Education Received
- “I think it was assumed that because I was already breastfeeding, the best thing would be to continue. However we couldn’t get the hang of switching between bottle and breast.”
- “The early feeding support was handled by midwives and breastfeeding advisors but I would have preferred more input from people who knew the specific challenges of early PKU feeding.”
- “More training for dietitians on [breast] feeding would have been beneficial as I believe they are in the best place to advise and support from the beginning.”
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Wegberg, A.M.J.; Macdonald, A.; Ahring, K.; BéLanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on phenylketonuria: Diagnosis and treatment. Orphanet J. Rare Dis. 2017, 12, 162. [Google Scholar] [CrossRef] [PubMed]
- Loeber, J.G. Neonatal screening in Europe; the situation in 2004. J. Inherit. Metab. Dis. 2007, 30, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Von Der Lippe, C.; Diesen, P.S.; Feragen, K.B. Living with a rare disorder: A systematic review of the qualitative literature. Mol. Genet. Genom. Med. 2017, 5, 758–773. [Google Scholar] [CrossRef]
- Gunduz, M.; Arslan, N.; Unal, O.; Cakar, S.; Kuyum, P.; Bulbul, S.F. Depression and anxiety among parents of phenylketonuria children. Neurosciences 2015, 20, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi-Gharaei, J.; Mostafavi, S.; Alirezaei, N. Quality of Life and the Associated Psychological Factors in Caregivers of Children with Pku. Iran. J. Psychiatry 2011, 6, 66–69. [Google Scholar]
- Fidika, A.; Salewski, C.; Goldbeck, L. Quality of life among parents of children with phenylketonuria (PKU). Health Qual. Life Outcomes 2013, 11, 54. [Google Scholar] [CrossRef]
- Kazak, A.E.; Reber, M.; Snitzer, L. Childhood Chronic Disease and Family Funcitoning: A Study of Phenylketonuria. Pediatrics 1988, 81, 224–230. [Google Scholar]
- Hoedt, A.E.T.; Maurice-Stam, H.; Boelen, C.C.A.; Rubio-Gozalbo, M.E.; van Spronsen, F.J.; Wijburg, F.A.; Bosch, A.M.; Grootenhuis, M.A. Parenting a child with phenylketonuria or galactosemia: Implications for health-related quality of life. J. Inherit. Metab. Dis. 2011, 34, 391–398. [Google Scholar] [CrossRef]
- Public Health England. Newborn Blood Spot Screening Data Collection and Performance Analysis Report 1 April 2018 to 31 March 2019. Updated 16 March 2021. The NHS Newborn Bloodspot Screening Program. Available online: https://www.gov.uk/government/publications/newborn-blood-spot-screening-data-collection-and-performance-analysis-report/ (accessed on 8 May 2023).
- MacDonald, A.; Pinto, A.; Evans, S.; Ashmore, C.; MacDonald, J.; Daly, A. Home Delivery Service of Low Protein Foods in Inherited Metabolic Disorders: Does It Help? Mol. Genet. Metab. Rep. 2019, 19, 100466. [Google Scholar] [CrossRef]
- Casey, L. Caring for children with phenylketonuria. Can. Fam. Physician 2013, 59, 837–840. [Google Scholar]
- Bernstein, L.E.; Helm, J.R.; Rocha, J.C.; Almeida, M.; Feillet, F.; Link, R.M.; Giżewska, M. Nutrition education tools used in phenylketonuria: Clinician, parent and patient perspectives from three international surveys. J. Hum. Nutr. Diet. 2013, 27 (Suppl. S2), 4–11. [Google Scholar] [CrossRef] [PubMed]
- Pate, T.; Rutar, M.; Battelino, T.; Radobuljac, M.D.; Bratina, N. Support Group for Parents Coping with Children with Type 1 Diabetes. Slov. J. Public Health 2015, 54, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Facebook Statistics You Must Know in 2023. Herd Digital. Available online: https://herd.digital/blog/facebook-statistics-2022/#:~:text=Interesting%20Facebook%20Statistics%201%20Facebook%20is%20the%20most,Stories%20has%20500%20million%20daily%20viewers.%20More%20items (accessed on 11 March 2023).
- Duggan, M. “Mobile Messaging and Social Media–2015”. Pew research Center. Available online: http://www.pewinternet.org/2015/08/19/mobile-messaging-and-social-media-2015/ (accessed on 11 March 2023).
- Hickson, M.; Child, J.; Collinson, A. Future Dietitian 2025: Informing the development of a workforce strategy for dietetics. J. Hum. Nutr. Diet. 2018, 31, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Collini, A.; Parker, H.; Oliver, A. Training for difficult conversations and breaking bad news over the phone in the emergency department. Emerg. Med. J. 2021, 38, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Chudleigh, J.; Holder, P.; Moody, L.; Simpson, A.; Southern, K.; Morris, S.; Fusco, F.; Ulph, F.; Bryon, M.; Bonham, J.R.; et al. Process Evaluation of Co-Designed Interventions to Improve Communication of Positive Newborn Bloodspot Screening Results. BMJ Open 2021, 11, e050773. [Google Scholar] [CrossRef] [PubMed]
- Pelentsov, L.J.; Fielder, A.L.; Laws, T.A.; Esterman, A.J. The supportive care needs of parents with a child with a rare disease: Results of an online survey. BMC Fam. Pract. 2016, 17, 88. [Google Scholar] [CrossRef] [PubMed]
- Waisbren, S.E. Parents’ reactions after the birth of a developmentally disabled child. Am. J. Ment. Defic. 1980, 84, 345–351. [Google Scholar] [PubMed]
- Garrubba, M.; Yap, G. Trust in Health Professionals; Centre for Clinical Effectiveness, Monash Health: Melbourne, Australia, 2019. [Google Scholar]
- Young-Hyman, D.; de Groot, M.; Hill-Briggs, F.; Gonzalez, J.S.; Hood, K.; Peyrot, M. Psychosocial Care for People with Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2126–2140. [Google Scholar] [CrossRef]
- Lord, B.; Wastell, C.; Ungerer, J. Parent Reactions to Childhood Phenylketonuria. Fam. Syst. Health 2005, 23, 204–219. [Google Scholar] [CrossRef]
- Beresford, B.A.; Beresford, B.A.; Beresford, B.A. Resources and Strategies: How Parents Cope with the Care of a Disabled Child. J. Child Psychol. Psychiatry 1994, 35, 171–209. [Google Scholar] [CrossRef] [PubMed]
- Amichai-Hamburger, Y.; Etgar, S. Intimacy and Smartphone Multitasking—A New Oxymoron? Psychol. Rep. 2016, 119, 826–838. [Google Scholar] [CrossRef] [PubMed]
- Gerson, J.; Plagnol, A.C.; Corr, P.J. Passive and Active Facebook Use Measure (PAUM): Validation and relationship to the Reinforcement Sensitivity Theory. Pers. Individ. Differ. 2017, 117, 81–90. [Google Scholar] [CrossRef]
- Kirk, S.; Milnes, L. An exploration of how young people and parents use online support in the context of living with cystic fibrosis. Health Expect. 2016, 19, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Cardinali, P.; Migliorini, L.; Rania, N. The Caregiving Experiences of Fathers and Mothers of Children with Rare Diseases in Italy: Challenges and Social Support Perceptions. Front. Psychol. 2019, 10, 1780. [Google Scholar] [CrossRef]
- Plantin, L.; Daneback, K. Parenthood, information and support on the internet. A literature review of research on parents and professionals online. BMC Fam. Pract. 2009, 10, 34. [Google Scholar] [CrossRef]
- Witalis, E.; Phenylketonuria, P.S.O.; Mikoluc, B.; Motkowski, R.; Szyszko, J.; Chrobot, A.; Didycz, B.; Lange, A.; Mozrzymas, R.; Milanowski, A.; et al. Phenylketonuria patients’ and their parents’ acceptance of the disease: Multi-centre study. Qual. Life Res. 2016, 25, 2967–2975. [Google Scholar] [CrossRef]
- Broom, A. Virtually He@Lthy: The Impact of Internet Use on Disease Experience and the Doctor-Patient Relationship. Qual. Health Res. 2005, 15, 325–345. [Google Scholar] [CrossRef]
- Barak, A.; Boniel-Nissim, M.; Suler, J. Fostering empowerment in online support groups. Comput. Hum. Behav. 2008, 24, 1867–1883. [Google Scholar] [CrossRef]
- Patel, R.; Chang, T.; Greysen, S.R.; Chopra, V. Social Media Use in Chronic Disease: A Systematic Review and Novel Taxonomy. Am. J. Med. 2015, 128, 1335–1350. [Google Scholar] [CrossRef]
- Partridge, S.R.; Gallagher, P.; Freeman, B.; Gallagher, R. Facebook Groups for the Management of Chronic Diseases. J. Med. Internet Res. 2018, 20, e21. [Google Scholar] [CrossRef] [PubMed]
- Schoenebeck, S. The Secret Life of Online Moms: Anonymity and Disinhibition on Youbemom. Com. In Proceedings of the Seventh International AAAI Conference on Weblogs and Social Media, Cambridge, MA, USA, 8–11 July 2013; Volume 7, pp. 555–562. [Google Scholar]
- Leask, J.; Kinnersley, P.; Jackson, C.; Cheater, F.; Bedford, H.; Rowles, G. Communicating with parents about vaccination: A framework for health professionals. BMC Pediatr. 2012, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Taherdoost, H. What Is the Best Response Scale for Survey and Questionnaire Design; Review of Different Lengths of Rating Scale/Attitude Scale/ Likert Scale. Int. J. Acad. Res. Manag. 2019, 8, 1–10. [Google Scholar]
- Bishop, P.A.; Herron, R.L. Use and Misuse of the Likert Item Responses and Other Ordinal Measures. Int. J. Exerc. Sci. 2015, 8, 297–302. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| Parental Feelings/Emotions on PKU Diagnosis | % (n) | % (n) | |
|---|---|---|---|
| Sad | 83 (141) | Lonely | 38 (64) |
| Anxious | 81 (136) | Angry | 36 (60) |
| Overwhelmed | 81 (136) | Neutral | 3 (5) |
| Confused | 57 (97) | Calm | 2 (3) |
| Exhausted | 40 (68) | Relaxed | <1 (1) |
| Common thematic open-ended responses | |||
| Fear of the unknown/lack of knowledge | 15 (26) | ||
| “It took a lot of time to understand the condition and to fully comprehend the care needed in order to keep [her] safe.” “Scared of the unknown. What would the future be like for my child.” “I remember thinking I wish my child had another disease that she could be cured of as she was never going to be free of PKU. I thought she was going to have a very poor quality of life.” “We were told to get to the hospital immediately. We hadn’t a clue what was happening.” | |||
| Overwhelming | 8 (13) | ||
| “Never got over it—felt been hit by a train. It was heart breaking, I still cry.” “Felt like a massive life changing event and left to deal with it.” “When my child was approaching 1 year I had an emotional breakdown coming to terms with his diagnosis and all that it entailed for me.” | |||
| Shock | 5 (9) | ||
| “[He] is my 7th child and my only one with PKU -it came as a complete shock.” “It was a shock and caused us a lot of worry especially as an older cousin in the family has PKU with learning difficulties.” | |||
| How the diagnosis was conveyed | 5 (8) | ||
| “I was given the diagnosis over the phone out of hours and told to be at the hospital first thing the next morning, this led to a sleepless night as we were provided with minimal information and no support or guidance.” “We were told face to face in our house and I think this is the best way for this to be done.” “The midwife told us it could lead to brain damage and learning difficulties, those words stuck in mine and my partners mind when we didn’t know any other information about it or the fact that he will be fine on a low protein diet.” “I was called by a nurse who gave us the shocking and life-changing diagnosis and told us not to Google it but to look at the information she would email us. It’s unrealistic to tell people not to look it up on the internet.” | |||
| Diagnosis with knowledge of PKU, i.e., sibling or relative | 5 (8) | ||
| “1st baby (PKU); Absolutely broken. World had come crashing down around me. 2nd & 3rd babies (1 PKU, 1 not); Peace. Acceptance. Intense love. We all deal with what it is.” “We were already aware of PKU due to another family member and that its manageable by diet so we didn’t have the initial fears that parents that haven’t heard of PKU would have.” | |||
| Guilt | 4 (7) | ||
| “Intense guilt for having wanted my son so badly and yet giving him this burden of a life (as I saw it then).” “Thinking that it was caused by us as parents.” | |||
| Isolation | 3 (5) | ||
| “I felt hugely isolated and lonely in the 1st 5 years.” | |||
| Resignation/acceptance | 3 (5) | ||
| “Me and the husband said it is what it is, having PKU doesn’t affect quality of life, our daughter will still develop normally. We can either cry about it or just get on with it, so we’ve decided to just get on with it and support our daughter in any way we can.” | |||
| Very Helpful/Helpful (Score 4, 5) | Neutral (Score 3) | Not Very/ Not Helpful (Score 1, 2) | Not Applicable | |
|---|---|---|---|---|
| How helpful was the support from different HCPs in the early years of a PKU diagnosis (%) | ||||
| Dietitian | 92 | 4 | 4 | 1 |
| Nurse | 64 | 17 | 9 | 11 |
| Hospital doctor | 50 | 22 | 21 | 7 |
| Health visitor | 22 | 17 | 58 | 3 |
| GP | 12 | 16 | 66 | 7 |
| Psychologist | 5 | 3 | 14 | 78 |
| How much do you trust the information provided by healthcare professionals (%) | ||||
| Dietitian | 94 | 4 | 1 | 1 |
| Nurse | 73 | 12 | 3 | 12 |
| Hospital doctor | 61 | 16 | 16 | 7 |
| Health visitor | 22 | 15 | 58 | 6 |
| GP | 15 | 17 | 59 | 9 |
| Psychologist | 9 | 4 | 13 | 74 |
| Very Helpful/Helpful (Score 4, 5) | Neutral (Score 3) | Not Very/ Not Helpful (Score 1, 2) | Not Applicable | |
|---|---|---|---|---|
| Where do you go to for support, and who listens to your concerns and makes you feel better (%) | ||||
| Family | 53 | 22 | 21 | 3 |
| Other PKU parents | 53 | 12 | 13 | 21 |
| NSPKU | 52 | 10 | 21 | 17 |
| Friends | 28 | 30 | 36 | 6 |
| NSPKU conferences | 19 | 10 | 19 | 52 |
| Where do you obtain your PKU information from (%) | ||||
| Information books | 74 | 16 | 8 | 2 |
| NSPKU | 68 | 7 | 17 | 9 |
| Other PKU parents | 54 | 16 | 15 | 14 |
| Hospital PKU events | 53 | 6 | 11 | 30 |
| Company learning packages | 43 | 16 | 24 | 17 |
| NSPKU conferences | 27 | 3 | 21 | 49 |
| Family | 12 | 15 | 56 | 17 |
| Friends | 9 | 7 | 63 | 21 |
| Very Helpful/Helpful (Score 4, 5) | Neutral (Score 3) | Not Very/ Not Helpful (Score 1, 2) | Not Applicable | |
|---|---|---|---|---|
| How helpful are social media sites at providing support for PKU (%) | ||||
| 68 | 13 | 10 | 9 | |
| 52 | 8 | 9 | 30 | |
| 27 | 11 | 19 | 43 | |
| YouTube | 16 | 16 | 18 | 50 |
| Internet Forums | 7 | 2 | 24 | 67 |
| How helpful are social media sites at providing information for PKU (%) | ||||
| 69 | 11 | 12 | 7 | |
| 59 | 3 | 9 | 29 | |
| 25 | 11 | 19 | 45 | |
| YouTube | 19 | 11 | 20 | 50 |
| Internet Forums | 7 | 2 | 27 | 65 |
| Themes | % (n) |
|---|---|
| Support/understanding and sense of community/belonging | 51 (56) |
| “Offloading, emotional support.” “Solidarity and understanding from a community of people who “get it” in a way others don’t.” “Being able to empathise with other parents who are going/have gone through similar things as well as being able to help other parents feel part of a PKU family where we share ideas and ask for advice.” “It’s good to know we’re not alone and we can laugh, cry or moan about PKU related stuff.” | |
| Quick access to hints, tips, advice, solutions to problems, and potential ideas | 40 (44) |
| “Answers and ideas from people who live with PKU day in, day out.” “Quick and helpful responses of things I’m not sure about and need to know quickly.” “Don’t even have to engage with people as can just search for things people have added in the past.” “Good for ideas. But for proper information I go to my dietitian.” | |
| Food/meal/recipe ideas | 40 (44) |
| “Loads of recipe ideas and new product finds.” “I’m able to ask about certain foods which if I didn’t have this group I would be constantly bothering the dietitians!” | |
| Reassurance | 10 (11) |
| “Reassurance that things will be okay.” “To hear other parents struggling with similar issues we have so we know it’s normal to have bad days.” “Comfort in knowing I’m not the only parent going through this.” | |
| Negative experiences | 7 (8) |
| “Don’t ask for advice as often there are mixed opinions and often turns quite negative” “Interesting to see other views, but it’s often conflicting and can be quite argumentative if people disagree with your approach.” “Some people who post I don’t trust their calculations of exchanges.” “There’s a lot of misinformation out there.” “I don’t trust what is said. I only trust my dietitian. She knows what she is talking about.” |
| Themes | % (n = 104) |
|---|---|
| Pros | |
| For expertise and advice: | 32 (35) |
| “Some more professional advice online could be good as PKU is very complicated and not all nutritional information on food packages is easy to understand.” “Twitter is good because there are dietitians on there who give great support and advice.” | |
| To correct inaccurate information: | 12 (12) |
| “Sometimes what has been said may not be correct so if they see wrong information being shared, would be useful for them to set the record straight.” “This would give me more confidence in the knowledge we receive and stop a lot of conflictive responses.” | |
| To learn about PKU from a parent/patient perspective: | 9 (9) |
| “I feel like they would gain a lot more knowledge just from being in the groups and looking at the information others provide and the struggles we all face as parents with children who have PKU or as adults who have PKU.” “They would have more of an understanding of what our worries are and what sort of questions we ask.” | |
| Cons | |
| People may feel less inclined to share/it is for sharing opinions: | 10 (10) |
| “People might not open up as much to professionals as they do to other parents, therefore they get more out of it if professionals stay away.” “Sometimes parents want to write about a particular difficulty they having with a healthcare professional and look to other parents for advice in how to deal with that.” | |
| Not their role/too busy/no time: | 10 (10) |
| “I don’t think health care professionals would have time to become involved in social media groups.” | |
| Input from different hospitals/centres: | 6 (6) |
| “Too vast to control the quantity of people’s ideas and challenge behaviour especially when they are led by varying trusts and dietitians with different principles of care.” | |
| Professional vulnerability | 4 (4) |
| “I feel that health care professionals would be vulnerable to the abuse associated with a lot of social media.” | |
| Other options | |
| Do not recommend relying on Facebook for facts or would go back to dietitian | 7 (7) |
| “I would always go back for official advice from our dietitians.” “I wouldn’t trust the majority of the information on social media as some of it is coming from people who are off diet and think there doing fantastic and some is from people who have no clue. But then I see posts about some people unable to see their consultant or dietitian to ask questions so they turn to Facebook for advice.” | |
| Separate groups for HCP and parents or specific times for HCPs to join in | 3 (3) |
| “Perhaps have a drop in slot where they can answer generic questions i.e., on exchange values or suitable medication.” “It would be helpful if there was a dedicated time on social media where parents could chat about concerns in a more relaxed way, sometimes I don’t want to ring up to the hospital as it feels like I’m being a pain.” |
| Advice Given | % (n) Receiving Advice |
|---|---|
| How to take a blood test | 93 (156) * |
| When to take a blood test | 82 (137) * |
| Immunisations | 59 (99) ** |
| Child development, e.g., speech/language | 38 (63) ** |
| Vitamin supplements | 30 (50) ** |
| Dental hygiene | 25 (42) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassidy, S.; Evans, S.; Pinto, A.; Daly, A.; Ashmore, C.; Ford, S.; Buckley, S.; MacDonald, A. Parent’s Perception of the Types of Support Given to Families with an Infant with Phenylketonuria. Nutrients 2023, 15, 2328. https://doi.org/10.3390/nu15102328
Cassidy S, Evans S, Pinto A, Daly A, Ashmore C, Ford S, Buckley S, MacDonald A. Parent’s Perception of the Types of Support Given to Families with an Infant with Phenylketonuria. Nutrients. 2023; 15(10):2328. https://doi.org/10.3390/nu15102328
Chicago/Turabian StyleCassidy, Sophie, Sharon Evans, Alex Pinto, Anne Daly, Catherine Ashmore, Suzanne Ford, Sharon Buckley, and Anita MacDonald. 2023. "Parent’s Perception of the Types of Support Given to Families with an Infant with Phenylketonuria" Nutrients 15, no. 10: 2328. https://doi.org/10.3390/nu15102328
APA StyleCassidy, S., Evans, S., Pinto, A., Daly, A., Ashmore, C., Ford, S., Buckley, S., & MacDonald, A. (2023). Parent’s Perception of the Types of Support Given to Families with an Infant with Phenylketonuria. Nutrients, 15(10), 2328. https://doi.org/10.3390/nu15102328