
Long-Term Effects of a Ketogenic Diet for Cancer

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
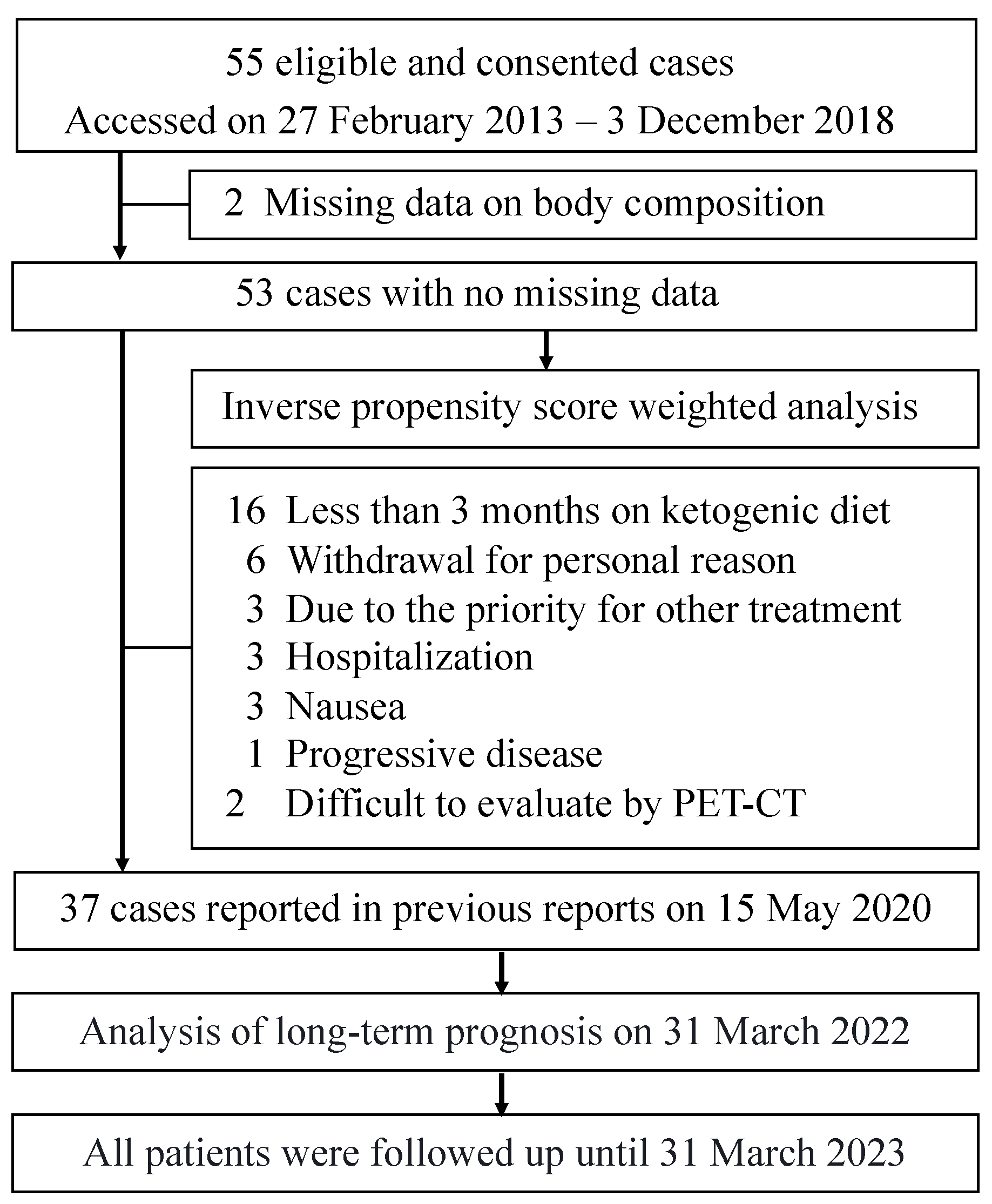
2.1. Participants and Design
2.2. Ketogenic Diet for Cancer Patients
2.3. Equipment and Evaluation Tools
2.4. Statistics
2.4.1. Long-Term Outcomes and Stratification of Survival Curves
2.4.2. Survival Analysis Using Propensity Score Weighting
2.5. Ethics
3. Results
3.1. Patient Characteristics
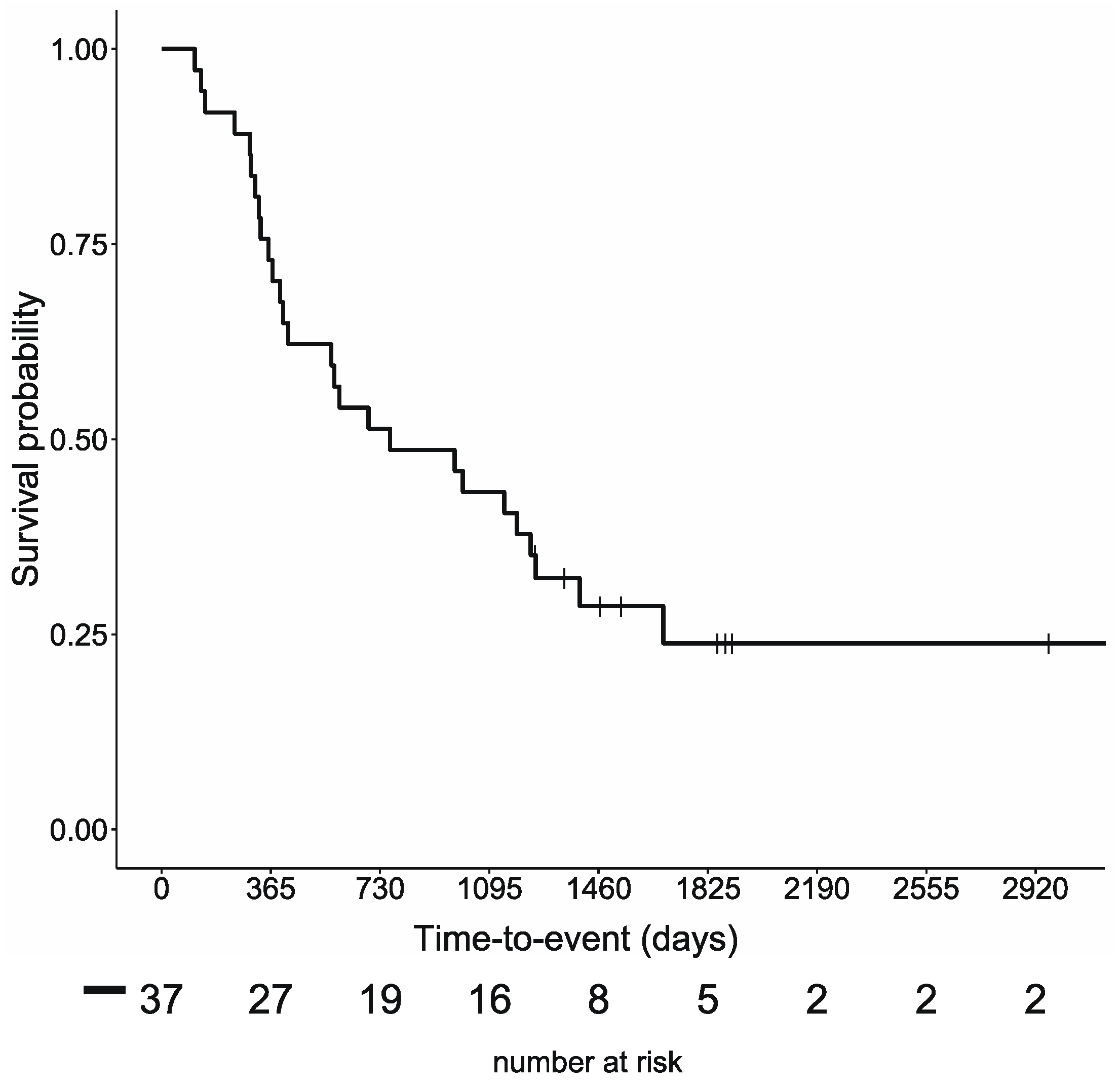
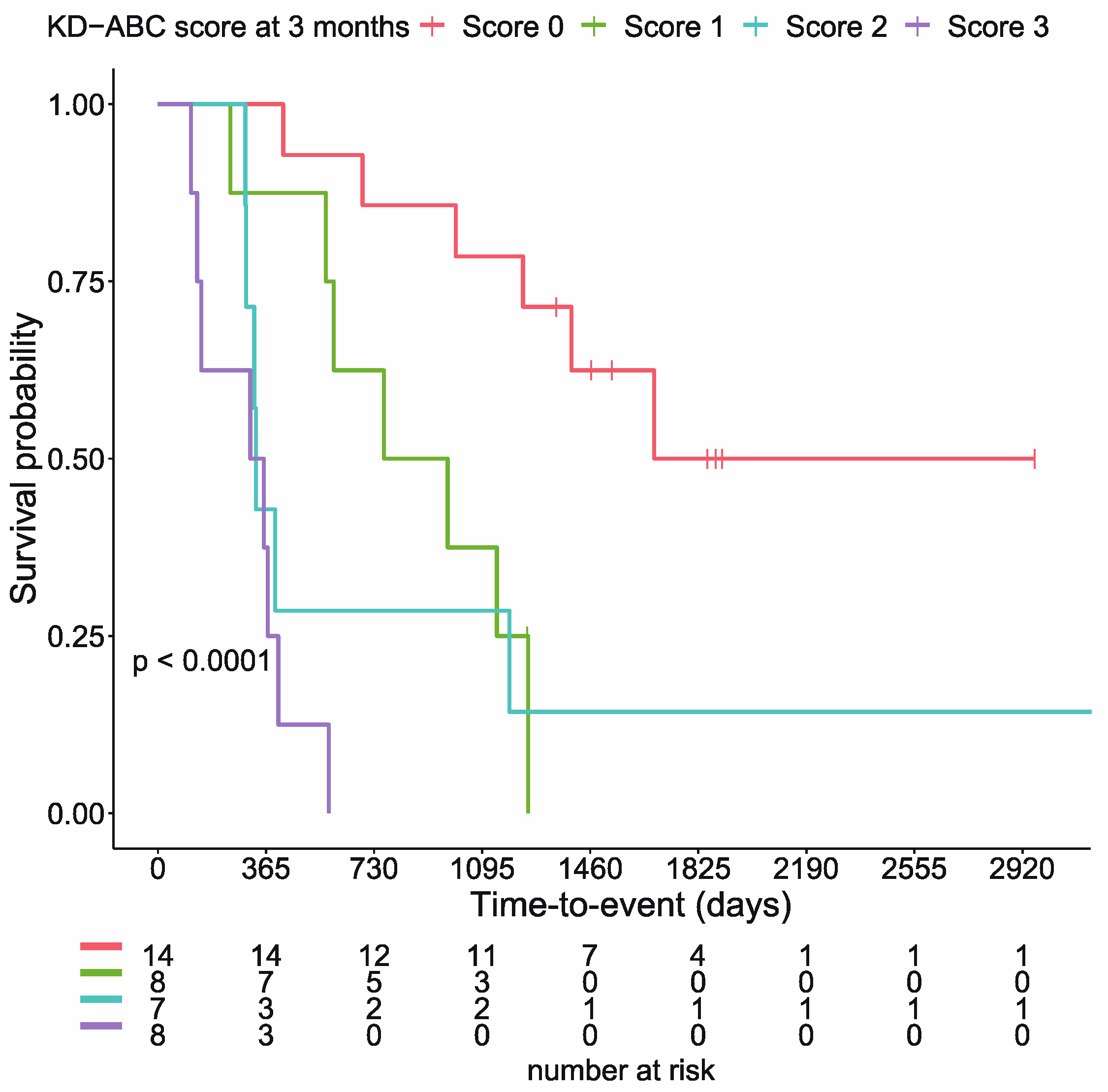
3.2. Long-Term Prognosis and Stratification of Survival Curves
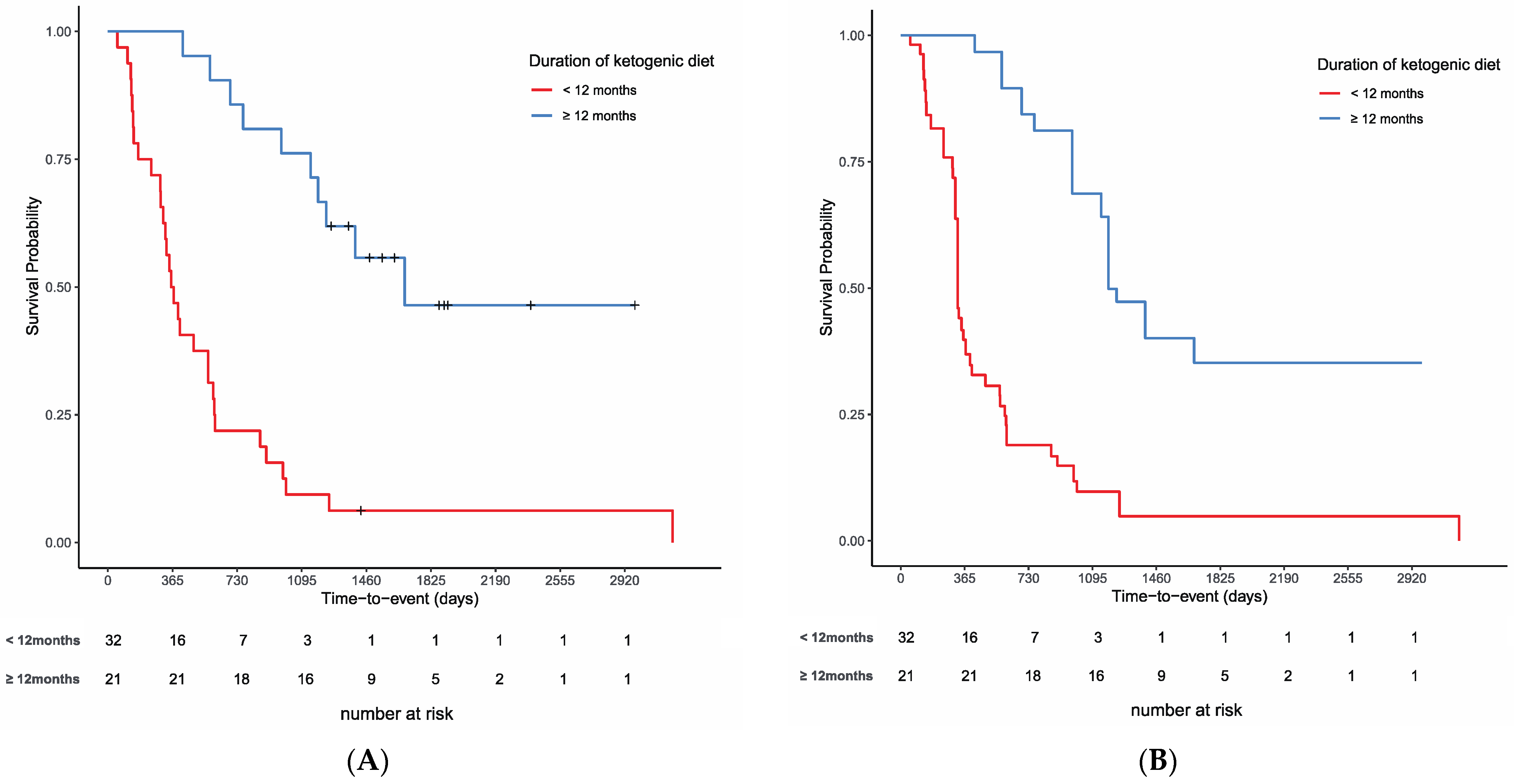
3.3. Effects of the Duration of the Ketogenic Diet on Survival
3.4. List of Long-Term Survivors on a Ketogenic Diet for Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.C.; Deutz, N.E.P.; Erickson, N.; Laviano, A.; Lisanti, M.P.; Lobo, D.N.; et al. ESPEN Expert Group Recommendations for Action against Cancer-Related Malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [PubMed]
- Kwan, P.; Schachter, S.C.; Brodie, M.J. Drug-resistant epilepsy. N. Engl. J. Med. 2011, 365, 919–926. [Google Scholar] [CrossRef]
- Klement, R.J.; Champ, C.E.; Otto, C.; Kämmerer, U. Anti-tumor effects of ketogenic diets in mice: A meta-analysis. PLoS ONE 2016, 11, e0155050. [Google Scholar] [CrossRef] [PubMed]
- Lane, J.; Brown, N.I.; Williams, S.; Plaisance, E.P.; Fontaine, K.R. Ketogenic diet for cancer: Critical assessment and research recommendations. Nutrients 2021, 13, 3562. [Google Scholar] [CrossRef] [PubMed]
- Cohen, C.W.; Fontaine, K.R.; Arend, R.C.; Soleymani, T.; Gower, B.A. Favorable effects of a ketogenic diet on physical function, perceived energy, and food cravings in women with ovarian or endometrial cancer: A randomized, controlled trial. Nutrients 2018, 10, 1187. [Google Scholar] [CrossRef]
- Cohen, C.W.; Fontaine, K.R.; Arend, R.C.; Alvarez, R.D.; Leath, C.A., III; Huh, W.K.; Bevis, K.S.; Kim, K.H.; Straughn, J.M.; Gower, B.A. A ketogenic diet reduces central obesity and serum insulin in women with ovarian or endometrial cancer. J. Nutr. 2018, 148, 1253–1260. [Google Scholar] [CrossRef]
- Khodabakhshi, A.; Akbari, M.E.; Mirzaei, H.R.; Mehrad-Majd, H.; Kalamian, M.; Davoodi, S.H. Feasibility, safety, and beneficial effects of MCT-based ketogenic diet for breast cancer treatment: A randomized controlled trial study. Nutr. Cancer 2019, 72, 627–634. [Google Scholar] [CrossRef]
- Huebner, J.; Keinki, C.; Käsmann, L. Critical remarks to the article by Khodabakhshi and colleagues reporting results from a randomized study on ketogenic diet. Clin. Nutr. 2022, 41, 1149. [Google Scholar] [CrossRef]
- Khodabakhshi, A.; Seyfried, T.N.; Kalamian, M.; Davoodi, S.H. Answer to the critical remarks to the article by Khodabakhshi and colleagues reporting results from a randomized study on ketogenic diet. Clin. Nutr. 2022, 41, 2063–2066. [Google Scholar] [CrossRef]
- Sremanakova, J.; Sowerbutts, A.M.; Burden, S. A systematic review of the use of ketogenic diets in adult patients with cancer. J. Hum. Nutr. Diet 2018, 31, 793–802. [Google Scholar] [CrossRef]
- Hagihara, K.; Kajimoto, K.; Osaga, S.; Nagai, N.; Shimosegawa, E.; Nakata, H.; Saito, H.; Nakano, M.; Takeuchi, M.; Kanki, H.; et al. Promising effect of a new ketogenic diet regimen in patients with advanced cancer. Nutrients 2020, 12, 1473. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.J.M.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Liu, C. Adjusted Kaplan–Meier estimator and log-rank test with inverse probability of treatment weighting for survival data. Statist. Med. 2005, 24, 3089–3110. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef]
- Voss, M.; Wenger, K.J.; von Mettenheim, N.; Bojunga, J.; Vetter, M.; Diehl, B.; Franz, K.; Gerlach, R.; Ronellenfitsch, M.W.; Harter, P.N.; et al. Short-term fasting in glioma patients: Analysis of diet diaries and metabolic parameters of the ERGO2 Trial. Eur. J. Nutr. 2022, 61, 477–487. [Google Scholar] [CrossRef]
- Noorlag, L.; Vos, F.Y.D.; Kok, A.; Broekman, M.L.D.; Seute, T.; Robe, P.A.; Snijders, T.J. Treatment of malignant gliomas with ketogenic or caloric restricted diets: A systematic review of preclinical and early clinical studies. Clin. Nutr. 2018, 38, 1986–1994. [Google Scholar] [CrossRef]
- Survival Statistics of Japanese Association of Clinical Cancer Centers, Cancer Survival Rates at Japanese Association of Clinical Cancer Centers. Available online: https://kapweb.chiba-cancer-registry.org/full (accessed on 31 August 2022).
- Hiyoshi, Y.; Miyamoto, Y.; Kiyozumi, Y.; Sawayama, H.; Eto, K.; Nagai, Y.; Iwatsuki, M.; Iwagami, S.; Baba, Y.; Yoshida, N.; et al. CT-guided percutaneous radiofrequency ablation for lung metastases from colorectal cancer. Int. J. Clin. Oncol. 2019, 24, 288–295. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Voss, M.; Wagner, M.; von Mettenheim, N.; Harter, P.N.; Wenger, K.J.; Franz, K.; Bojunga, J.; Vetter, M.; Gerlach, R.; Glatzel, M.; et al. ERGO2: A prospective, randomized trial of calorie-restricted ketogenic diet and fasting in addition to reirradiation for malignant glioma. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 987–995. [Google Scholar] [CrossRef]
- van der Louw, E.J.T.M.; Olieman, J.F.; van den Bemt, P.M.L.A.; Bromberg, J.E.C.; Hoop, E.O.; Neuteboom, R.F.; Catsman-Berrevoets, C.E.; Vincent, A.J.P.E. Ketogenic diet treatment as adjuvant to standard treatment of glioblastoma multiforme: A feasibility and safety study. Ther. Adv. Med. Oncol. 2019, 11, 1758835919853958. [Google Scholar] [CrossRef]
- Rieger, J.; Bähr, O.; Maurer, G.D.; Hattingen, E.; Franz, K.; Brucker, D.; Walenta, S.; Kämmerer, U.; Coy, J.F.; Weller, M.; et al. ERGO: A pilot study of ketogenic diet in recurrent glioblastoma. Int. J. Oncol. 2014, 44, 1843–1852. [Google Scholar] [CrossRef] [PubMed]
- Klein, P.; Tyrlikova, I.; Zuccoli, G.; Tyrlik, A.; Maroon, J.C. Treatment of glioblastoma multiforme with “Classic” 4:1 ketogenic diet total meal replacement. Cancer Metab. 2020, 8, 24. [Google Scholar] [CrossRef] [PubMed]
- Zahra, A.; Fath, M.A.; Opat, E.; Mapuskar, K.A.; Bhatia, S.K.; Ma, D.C.; Rodman, S.N., III; Snyders, T.P.; Chenard, C.A.; Eichenberger-Gilmore, J.M.; et al. Consuming a ketogenic diet while receiving radiation and chemotherapy for locally advanced lung cancer and pancreatic cancer: The University of Iowa experience of two phase 1 clinical trials. Radiat. Res. 2017, 187, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Dyson, G.; Snyder, M.; Kim, H.-R.; Severson, R.K. Differential effects of patient-related factors on the outcome of radiation therapy for rectal cancer. J. Radiat. Oncol. 2016, 5, 279–286. [Google Scholar] [CrossRef]
- Gwilliam, B.; Keeley, V.; Todd, C.; Gittins, M.; Roberts, C.; Kelly, L.; Barclay, S.; Stone, P.C. Development of Prognosis in Palliative Care Study (PiPS) predictor models to improve prognostication in advanced cancer: Prospective cohort study. BMJ 2011, 343, d4920. [Google Scholar] [CrossRef]
- Hamano, J.; Takeuchi, A.; Yamaguchi, T.; Baba, M.; Imai, K.; Ikenaga, M.; Matsumoto, Y.; Sekine, R.; Yamaguchi, T.; Hirohashi, T.; et al. A combination of routine laboratory findings and vital signs can predict survival of advanced cancer patients without physician evaluation: A fractional polynomial model. Eur. J. Cancer 2018, 105, 50–60. [Google Scholar] [CrossRef]
- Viganó, A.; Bruera, E.; Jhangri, G.S.; Newman, S.C.; Fields, A.L.; Suarez-Almazor, M.E. Clinical survival predictors in patients with advanced cancer. Arch. Intern. Med. 2000, 160, 861–868. [Google Scholar] [CrossRef]
- Chau, I.; Norman, A.R.; Cunningham, D.; Waters, J.S.; Oates, J.; Ross, P.J. Multivariate prognostic factor analysis in locally advanced and metastatic esophago-gastric cancer—Pooled analysis from three multicenter, randomized, controlled trials using individual patient data. J. Clin. Oncol. 2004, 22, 2395–2403. [Google Scholar] [CrossRef]
- Kaasa, S.; Mastekaasa, A.; Lund, E. Prognostic factors for patients with inoperable non-small cell lung cancer, limited disease the importance of patients’ subjective experience of disease and psychosocial well-being. Radiother. Oncol. 1989, 15, 235–242. [Google Scholar] [CrossRef]
- Efficace, F.; Bottomley, A.; Coens, C.; Steen, K.V.; Conroy, T.; Schöffski, P.; Schmoll, H.; Cutsem, E.V.; Köhne, C.-H. Does a patient’s self-reported health-related quality of life predict survival beyond key biomedical data in advanced colorectal cancer? Eur. J. Cancer 2006, 42, 42–49. [Google Scholar] [CrossRef]
- Maltoni, M.; Caraceni, A.; Brunelli, C.; Broeckaert, B.; Christakis, N.; Eychmueller, S.; Glare, P.; Nabal, M.; Viganò, A.; Larkin, P.; et al. Prognostic factors in advanced cancer patients: Evidence-based clinical recommendations—A study by the Steering Committee of the European Association for Palliative Care. J. Clin. Oncol. 2005, 23, 6240–6248. [Google Scholar] [CrossRef] [PubMed]
- Quinten, C.; Coens, C.; Mauer, M.; Comte, S.; Sprangers, M.A.; Cleeland, C.; Osoba, D.; Bjordal, K.; Bottomley, A.; on behalf of the EORTC Clinical Groups. Baseline quality of life as a prognostic indicator of survival: A meta-analysis of individual patient data from EORTC clinical trials. Lancet Oncol. 2009, 10, 865–871. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| <12 Months Group | ≥12 Months Group | Total | |
|---|---|---|---|
| Number of cases, n | 32 | 21 | 53 |
| Age, y | 57.6 ± 12.8 | 52.2 ± 10.0 | 55.5 ± 12.1 |
| Sex, male/female, n | 14/18 | 8/13 | 22/31 |
| Primary cancer, n | |||
| Non-small cell lung cancer, n | 3 | 11 | 14 |
| Colorectal cancer, n | 4 | 5 | 9 |
| Breast cancer, n | 4 | 2 | 6 |
| Pancreatic cancer, n | 1 | 3 | 4 |
| Head and neck cancer, n | 3 | 1 | 4 |
| Bone and soft tissue sarcoma, n | 3 | 1 | 4 |
| Ovarian and peritoneal cancer, n | 1 | 2 | 3 |
| Biliary tract cancer, n | 0 | 2 | 2 |
| Endometrial cancer, n | 0 | 1 | 1 |
| Bladder cancer, n | 0 | 2 | 2 |
| Brain tumor, n | 1 | 0 | 1 |
| Esophageal cancer, n | 0 | 1 | 1 |
| Gastric cancer, n | 0 | 1 | 1 |
| Prostate cancer, n | 1 | 0 | 1 |
| Follow-up time, median (range), months | 11.5 (1–104) | 44 (13–97) | 19 (1–104) |
| Duration of KD, median (range), months | 3 (0–11) | 37 (12–99) | 6 (0–99) |
| Unadjusted | Adjusted | |||||||
|---|---|---|---|---|---|---|---|---|
| <12 Months (n = 32) | ≥12 Months (n = 21) | p-Value | SMD | <12 Months (n = 54.2) | ≥12 Months (n = 41.8) | p-Value | SMD | |
| Male (%) | 14 (43.8) | 8 (38.1) | 0.902 | 0.115 | 20.0 (36.9) | 20.0 (47.9) | 0.526 | 0.223 |
| Age, y | 57.62 (13.01) | 52.24 (10.24) | 0.116 | 0.46 | 53.28 (15.86) | 54.38 (9.84) | 0.839 | 0.083 |
| Weight, kg | 54.02 (12.85) | 55.28 (11.32) | 0.716 | 0.104 | 57.02 (16.28) | 55.87 (11.36) | 0.819 | 0.082 |
| BMI | 20.38 (3.42) | 20.88 (3.26) | 0.604 | 0.147 | 21.59 (4.20) | 20.83 (2.99) | 0.553 | 0.207 |
| Lean mass of limb, kg | 16.94 (4.50) | 16.87 (4.16) | 0.955 | 0.016 | 17.06 (4.75) | 17.45 (4.47) | 0.808 | 0.084 |
| Lung cancer, n (%) | 11 (34.4) | 3 (14.3) | 0.192 | 0.482 | 13.8 (25.5) | 10.2 (24.4) | 0.945 | 0.025 |
| Laboratory tests | ||||||||
| Platelets, 104/μL | 23.65 (9.09) | 22.44 (4.83) | 0.579 | 0.166 | 21.49 (8.62) | 20.84 (5.61) | 0.793 | 0.09 |
| WBC, 103/μL | 5.75 (2.57) | 4.53 (1.87) | 0.066 | 0.545 | 5.07 (2.45) | 4.65 (1.93) | 0.58 | 0.191 |
| Creatinine, mg/dL | 0.74 (0.22) | 0.67 (0.19) | 0.269 | 0.318 | 0.71 (0.20) | 0.74 (0.23) | 0.762 | 0.111 |
| ALP, U/L | 366.50 (432.68) | 224.38 (85.62) | 0.145 | 0.456 | 307.15 (344.13) | 236.01 (83.23) | 0.207 | 0.284 |
| Potassium, mEq/L | 4.07 (0.37) | 4.10 (0.26) | 0.674 | 0.123 | 4.01 (0.35) | 4.05 (0.31) | 0.768 | 0.108 |
| BUN, mg/dL | 16.75 (5.62) | 16.29 (4.86) | 0.758 | 0.088 | 16.26 (4.75) | 17.71 (5.84) | 0.449 | 0.272 |
| Neutrophil count, 103/μL | 3.86 (1.99) | 2.67 (1.39) | 0.022 | 0.69 | 3.22 (1.95) | 2.84 (1.37) | 0.528 | 0.222 |
| CRP, mg/dL | 1.11 (1.69) | 0.20 (0.37) | 0.02 | 0.741 | 0.72 (1.41) | 0.36 (0.56) | 0.253 | 0.33 |
| Albumin, g/dL | 3.88 (0.41) | 4.21 (0.33) | 0.003 | 0.894 | 4.04 (0.41) | 4.16 (0.32) | 0.362 | 0.31 |
| EORTC-QLQ30 | ||||||||
| Global health status | 51.30 (24.04) | 62.70 (25.50) | 0.106 | 0.46 | 58.01 (24.75) | 60.25 (26.88) | 0.813 | 0.087 |
| Financial difficulties | 29.16 (33.60) | 22.21 (26.52) | 0.429 | 0.229 | 22.35 (30.63) | 25.02 (24.52) | 0.74 | 0.096 |
| Physical functioning | 82.29 (15.10) | 88.58 (13.19) | 0.126 | 0.444 | 85.66 (14.51) | 86.76 (12.24) | 0.804 | 0.082 |
| Role functioning | 75.00 (25.75) | 85.71 (26.50) | 0.149 | 0.41 | 80.79 (24.32) | 81.29 (28.78) | 0.959 | 0.019 |
| Emotional functioning | 77.08 (20.52) | 79.37 (14.10) | 0.658 | 0.13 | 79.87 (18.23) | 76.65 (18.47) | 0.64 | 0.175 |
| Cognitive functioning | 83.85 (17.70) | 81.74 (24.09) | 0.716 | 0.1 | 83.20 (16.00) | 72.76 (33.33) | 0.368 | 0.399 |
| Social functioning | 69.27 (29.97) | 82.55 (19.34) | 0.078 | 0.527 | 72.94 (26.62) | 78.37 (18.71) | 0.399 | 0.236 |
| Fatigue | 35.05 (19.38) | 36.49 (21.99) | 0.803 | 0.07 | 28.45 (19.14) | 42.56 (28.25) | 0.165 | 0.584 |
| Pain | 23.45 (21.93) | 11.91 (18.37) | 0.052 | 0.57 | 17.36 (20.09) | 11.31 (19.80) | 0.358 | 0.304 |
| Dyspnea | 15.61 (16.88) | 15.86 (17.04) | 0.959 | 0.015 | 14.44 (16.77) | 18.64 (16.94) | 0.465 | 0.249 |
| Insomnia | 30.20 (30.95) | 28.57 (36.95) | 0.863 | 0.048 | 30.55 (26.59) | 36.88 (42.64) | 0.631 | 0.178 |
| Nausea and vomiting | 7.82 (16.39) | 7.94 (12.49) | 0.977 | 0.008 | 5.20 (13.55) | 8.45 (12.12) | 0.377 | 0.253 |
| Appetite loss | 30.20 (28.54) | 20.63 (28.82) | 0.24 | 0.334 | 27.98 (25.66) | 27.38 (37.48) | 0.963 | 0.019 |
| Constipation | 16.66 (25.40) | 28.56 (30.34) | 0.129 | 0.425 | 18.40 (23.55) | 22.03 (26.87) | 0.628 | 0.144 |
| Diarrhea | 13.54 (26.59) | 11.10 (24.34) | 0.737 | 0.096 | 8.72 (22.33) | 11.49 (24.91) | 0.686 | 0.117 |
| No | Sex | Age (y) * | Cancer Type | Histology | TNM Classification | Continuation of KD | Duration of KD, Weeks | OS (Months) | Current Status † |
|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 56 | Lung cancer | Adenocarcinoma | T2aN0M1a | finished | 16 | 121 | deceased |
| 2 | F | 52 | Lung cancer | Adenocarcinoma | T2aN0M1b | Ongoing | 422 | 109 | alive |
| 3 | F | 36 | Colorectal cancer | Tubular adenocarcinoma | T4bN1aM1b | finished | 53 | 74 | alive |
| 4 | F | 41 | Breast cancer | Invasive ductal carcinoma | T3N1M1 | finished | 61 | 73 | alive |
| 5 | M | 79 | Sarcoma | Chondrosarcoma | T2N1M1 | Ongoing | 263 | 72 | alive |
| 6 | M | 46 | Oral and pharyngeal cancer | Adenoid cystic carcinoma | T4aN1M1 | finished | 121 | 81 | deceased |
| 7 | M | 55 | Lung cancer | Adenocarcinoma | T3N1M1a | Ongoing | 218 | 62 | alive |
| 8 | F | 50 | Colorectal cancer | Tubular adenocarcinoma | TXN1bM1a | Ongoing | 207 | 60 | alive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egashira, R.; Matsunaga, M.; Miyake, A.; Hotta, S.; Nagai, N.; Yamaguchi, C.; Takeuchi, M.; Moriguchi, M.; Tonari, S.; Nakano, M.; et al. Long-Term Effects of a Ketogenic Diet for Cancer. Nutrients 2023, 15, 2334. https://doi.org/10.3390/nu15102334
Egashira R, Matsunaga M, Miyake A, Hotta S, Nagai N, Yamaguchi C, Takeuchi M, Moriguchi M, Tonari S, Nakano M, et al. Long-Term Effects of a Ketogenic Diet for Cancer. Nutrients. 2023; 15(10):2334. https://doi.org/10.3390/nu15102334
Chicago/Turabian StyleEgashira, Ryuichiro, Michiko Matsunaga, Akimitsu Miyake, Sayaka Hotta, Naoko Nagai, Chise Yamaguchi, Mariko Takeuchi, Misaki Moriguchi, Satoko Tonari, Mai Nakano, and et al. 2023. "Long-Term Effects of a Ketogenic Diet for Cancer" Nutrients 15, no. 10: 2334. https://doi.org/10.3390/nu15102334
APA StyleEgashira, R., Matsunaga, M., Miyake, A., Hotta, S., Nagai, N., Yamaguchi, C., Takeuchi, M., Moriguchi, M., Tonari, S., Nakano, M., Saito, H., & Hagihara, K. (2023). Long-Term Effects of a Ketogenic Diet for Cancer. Nutrients, 15(10), 2334. https://doi.org/10.3390/nu15102334