
Understanding PPARγ and Its Agonists on Trophoblast Differentiation and Invasion: Potential Therapeutic Targets for Gestational Diabetes Mellitus and Preeclampsia

Abstract
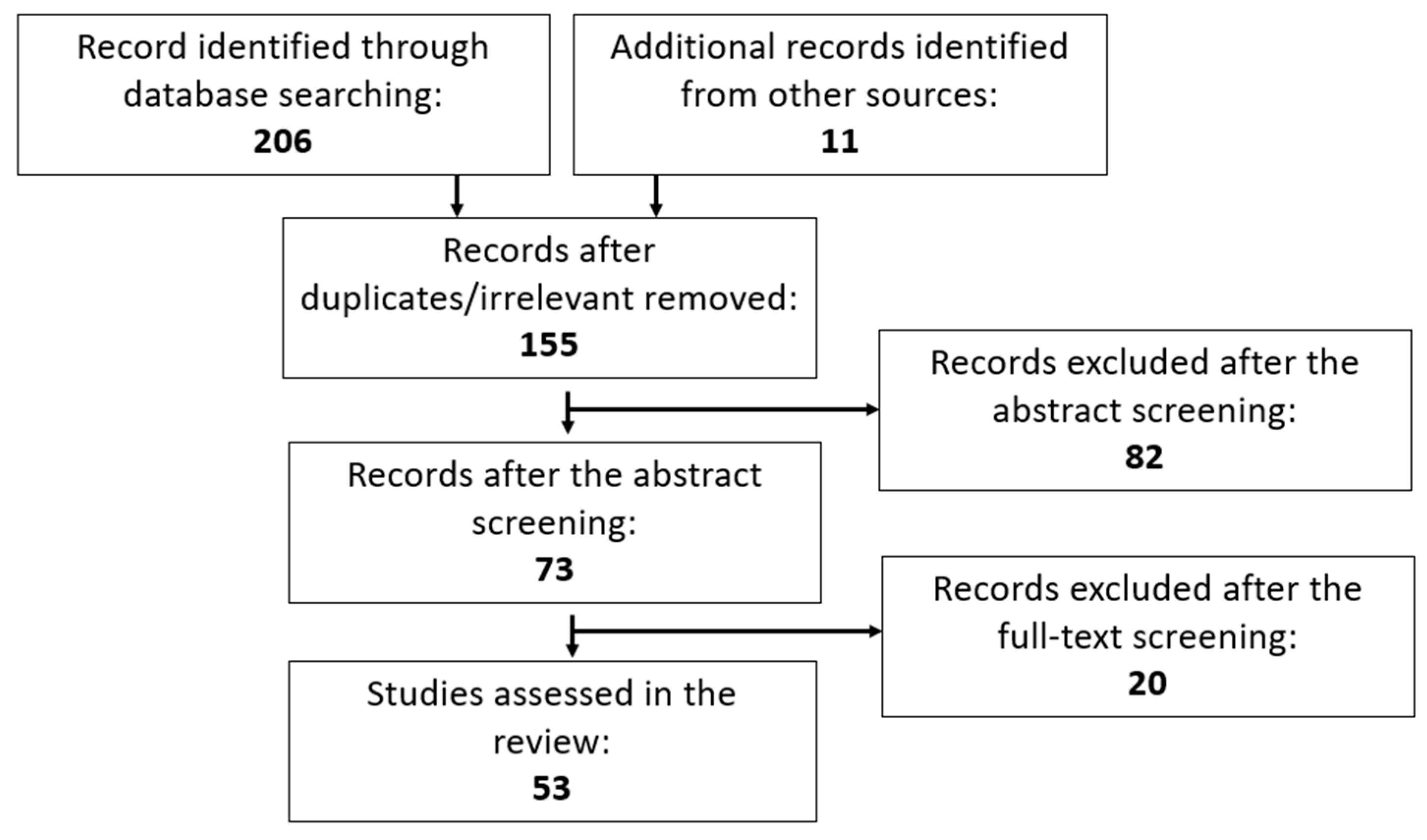
:1. Introduction
2. Peroxisome Proliferator-Activated Receptor-γ
3. PPARγ Functions in the Placenta and Trophoblasts
4. Genome-Wide Association Studies (GWAS) Suggested That PPARγ Is Associated with Preeclampsia and Gestational Diabetes Mellitus
5. The Role of PPARγ in Preeclampsia
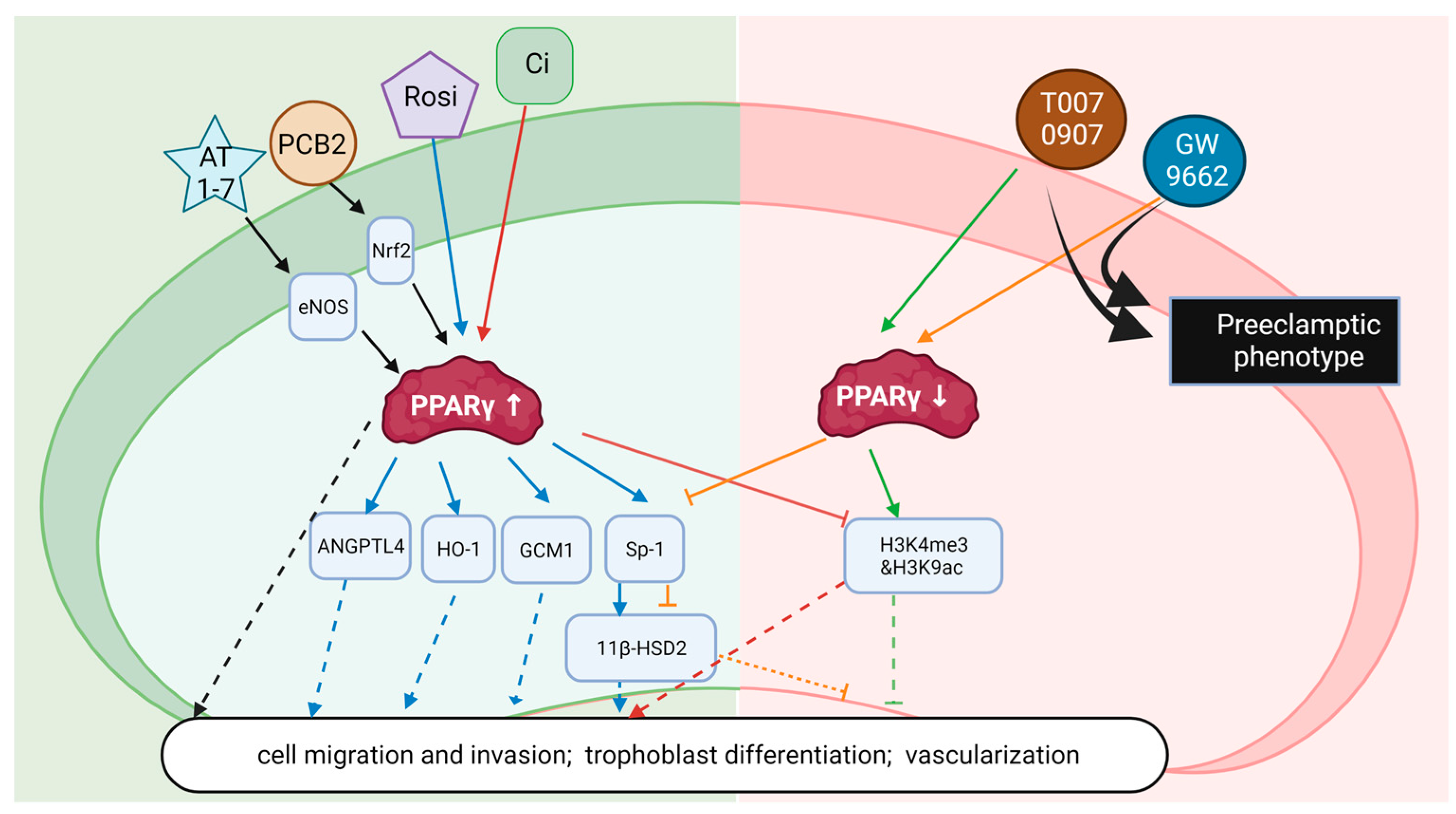
5.1. PAPRγ in the Pathogenesis of PE
5.2. Effect of PAPRγ Ligands on PE in Rodent Models
5.3. Potential Treatments of Preeclampsia Targeting PPARγ
6. PPARγ Functions in Placentas from GDM
PPARγ Function in the Placentas of GDM Patients
7. Future Directions and Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PPARγ | Peroxisome Proliferator-Activated Receptor-γ |
| GDM | Gestational Diabetes Mellitus |
| PE | Preeclampsia |
| EVTs | Extravillous trophoblasts |
| GCM1 | Glial cell missing 1 |
| T2DM | Type 2 Diabetes Mellitus |
| PBMC | Peripheral blood mononuclear cells |
| TGC | Trophoblast giant cells |
| COX | Cyclooxygenase |
| Nrf2 | Nuclear factor erythroid 2-related factor 2 |
| VEGF | Vascular endothelial growth factor |
| sFlt | soluble Fms-like tyrosine kinase |
| RUPP | Reduced uterine perfusion pressure |
| HO-1 | Heme oxygenase 1 |
| TZD | Thiazolidinedione |
| LDL | Low-density lipoproteins |
| BADGE | Bisphenol A diglycidyl ether |
| NFκB | Nuclear factor kappa-light-chain-enhancer |
| EETs | Epoxyeicosatrienoic acids |
| 15d-PGJ2 | 15-deoxy-Δ-12,14 prostaglandin J2 |
| 15-HETE | 15-Hydroxyeicosatetraenoic Acid |
| 13-HODE | 13- hydroxyoctadecadienoic acid |
References
- Trends in Pregnancy and Childbirth Complications in the U.S.; Blue cross Blue Shield: Chicago, IL, USA, 2020.
- Psilopatis, I.; Vrettou, K.; Fleckenstein, F.N.; Theocharis, S. The Role of Peroxisome Proliferator-Activated Receptors in Preeclampsia. Cells 2023, 12, 647. [Google Scholar] [CrossRef] [PubMed]
- McElwain, C.J.; McCarthy, F.P.; McCarthy, C.M. Gestational Diabetes Mellitus and Maternal Immune Dysregulation: What We Know So Far. Int. J. Mol. Sci. 2021, 22, 4261. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef]
- McElwain, C.J.; Tuboly, E.; McCarthy, F.P.; McCarthy, C.M. Mechanisms of Endothelial Dysfunction in Pre-eclampsia and Gestational Diabetes Mellitus: Windows Into Future Cardiometabolic Health? Front. Endocrinol. 2020, 11, 655. [Google Scholar] [CrossRef]
- Longhitano, E.; Siligato, R.; Torreggiani, M.; Attini, R.; Masturzo, B.; Casula, V.; Matarazzo, I.; Cabiddu, G.; Santoro, D.; Versino, E.; et al. The Hypertensive Disorders of Pregnancy: A Focus on Definitions for Clinical Nephrologists. J. Clin. Med. 2022, 11, 3420. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S.; et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef]
- Sullivan, S.D.; Umans, J.G.; Ratner, R. Hypertension complicating diabetic pregnancies: Pathophysiology, management, and controversies. J. Clin. Hypertens. 2011, 13, 275–284. [Google Scholar] [CrossRef]
- Giorgione, V.; Jansen, G.; Kitt, J.; Ghossein-Doha, C.; Leeson, P.; Thilaganathan, B. Peripartum and Long-Term Maternal Cardiovascular Health After Preeclampsia. Hypertension 2023, 80, 231–241. [Google Scholar] [CrossRef]
- Aprile, M.; Ambrosio, M.R.; D’Esposito, V.; Beguinot, F.; Formisano, P.; Costa, V.; Ciccodicola, A. PPARG in Human Adipogenesis: Differential Contribution of Canonical Transcripts and Dominant Negative Isoforms. PPAR Res. 2014, 2014, 537865. [Google Scholar] [CrossRef]
- Fajas, L.; Auboeuf, D.; Raspe, E.; Schoonjans, K.; Lefebvre, A.M.; Saladin, R.; Najib, J.; Laville, M.; Fruchart, J.C.; Deeb, S.; et al. The organization, promoter analysis, and expression of the human PPARgamma gene. J. Biol. Chem. 1997, 272, 18779–18789. [Google Scholar] [CrossRef]
- Froment, P.; Gizard, F.; Defever, D.; Staels, B.; Dupont, J.; Monget, P. Peroxisome proliferator-activated receptors in reproductive tissues: From gametogenesis to parturition. J. Endocrinol. 2006, 189, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Grygiel-Gorniak, B. Peroxisome proliferator-activated receptors and their ligands: Nutritional and clinical implications—A review. Nutr. J. 2014, 13, 17. [Google Scholar] [CrossRef] [PubMed]
- Villacorta, L.; Schopfer, F.J.; Zhang, J.; Freeman, B.A.; Chen, Y.E. PPARgamma and its ligands: Therapeutic implications in cardiovascular disease. Clin. Sci. 2009, 116, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Lehrke, M.; Lazar, M.A. The many faces of PPARgamma. Cell 2005, 123, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Makela, J.; Tselykh, T.V.; Kukkonen, J.P.; Eriksson, O.; Korhonen, L.T.; Lindholm, D. Peroxisome proliferator-activated receptor-gamma (PPARgamma) agonist is neuroprotective and stimulates PGC-1alpha expression and CREB phosphorylation in human dopaminergic neurons. Neuropharmacology 2016, 102, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Brusotti, G.; Montanari, R.; Capelli, D.; Cattaneo, G.; Laghezza, A.; Tortorella, P.; Loiodice, F.; Peiretti, F.; Bonardo, B.; Paiardini, A.; et al. Betulinic acid is a PPARgamma antagonist that improves glucose uptake, promotes osteogenesis and inhibits adipogenesis. Sci. Rep. 2017, 7, 5777. [Google Scholar] [CrossRef] [PubMed]
- Rieusset, J.; Touri, F.; Michalik, L.; Escher, P.; Desvergne, B.; Niesor, E.; Wahli, W. A new selective peroxisome proliferator-activated receptor gamma antagonist with antiobesity and antidiabetic activity. Mol. Endocrinol. 2002, 16, 2628–2644. [Google Scholar] [CrossRef]
- Giaginis, C.; Spanopoulou, E.; Theocharis, S. PPAR-gamma signaling pathway in placental development and function: A potential therapeutic target in the treatment of gestational diseases. Expert. Opin. Ther. Targets 2008, 12, 1049–1063. [Google Scholar] [CrossRef]
- van Andel, M.; Heijboer, A.C.; Drent, M.L. Adiponectin and Its Isoforms in Pathophysiology. Adv. Clin. Chem. 2018, 85, 115–147. [Google Scholar] [CrossRef]
- Wang, Y.; Pan, Z.; Chen, F. Inhibition of PPARgamma by bisphenol A diglycidyl ether ameliorates dexamethasone-induced osteoporosis in a mouse model. J. Int. Med. Res. 2019, 47, 6268–6277. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, Y.; Schmelzer, K.; Lee, T.S.; Fang, X.; Zhu, Y.; Spector, A.A.; Gill, S.; Morisseau, C.; Hammock, B.D.; et al. The antiinflammatory effect of laminar flow: The role of PPARgamma, epoxyeicosatrienoic acids, and soluble epoxide hydrolase. Proc. Natl. Acad. Sci. USA 2005, 102, 16747–16752. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, S.; Picard, F.; Vamecq, J.; Gelman, L.; Potier, N.; Zeyer, D.; Dubuquoy, L.; Bac, P.; Champy, M.F.; Plunket, K.D.; et al. A unique PPARgamma ligand with potent insulin-sensitizing yet weak adipogenic activity. Mol. Cell 2001, 8, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, R.; Hoener, P.A.; Jow, L.; Bilakovics, J.; Klausing, K.; Mais, D.E.; Faulkner, A.; Croston, G.E.; Paterniti, J.R., Jr. A selective peroxisome proliferator-activated receptor-gamma (PPARgamma) modulator blocks adipocyte differentiation but stimulates glucose uptake in 3T3-L1 adipocytes. Mol. Endocrinol. 2000, 14, 1425–1433. [Google Scholar] [CrossRef]
- Li, J.; Guo, C.; Wu, J. 15-Deoxy-∆-(12,14)-Prostaglandin J2 (15d-PGJ2), an Endogenous Ligand of PPAR-gamma: Function and Mechanism. PPAR Res. 2019, 2019, 7242030. [Google Scholar] [CrossRef] [PubMed]
- Higgins, L.S.; Mantzoros, C.S. The Development of INT131 as a Selective PPARgamma Modulator: Approach to a Safer Insulin Sensitizer. PPAR Res. 2008, 2008, 936906. [Google Scholar] [CrossRef] [PubMed]
- Camp, H.S.; Chaudhry, A.; Leff, T. A novel potent antagonist of peroxisome proliferator-activated receptor gamma blocks adipocyte differentiation but does not revert the phenotype of terminally differentiated adipocytes. Endocrinology 2001, 142, 3207–3213. [Google Scholar] [CrossRef]
- Feng, L.; Liu, W.; Yang, J.; Wang, Q.; Wen, S. Effect of Hexadecyl Azelaoyl Phosphatidylcholine on Cardiomyocyte Apoptosis in Myocardial Ischemia-Reperfusion Injury: A Hypothesis. Med. Sci. Monit. 2018, 24, 2661–2667. [Google Scholar] [CrossRef]
- O’Connor-Semmes, R.O.B.I.N.; Mydlow, P.; Walker, A.; Clark, R.V. GI262570, A PPAR [Gamma] Agonist, Maintains Metabolic Improvements throughout 24 Hour Profiles In Type 2 Diabetic Patients. Diabetes 2000, 49, A119. [Google Scholar]
- Lee, G.; Elwood, F.; McNally, J.; Weiszmann, J.; Lindstrom, M.; Amaral, K.; Nakamura, M.; Miao, S.; Cao, P.; Learned, R.M.; et al. T0070907, a selective ligand for peroxisome proliferator-activated receptor gamma, functions as an antagonist of biochemical and cellular activities. J. Biol. Chem. 2002, 277, 19649–19657. [Google Scholar] [CrossRef]
- Saether, T.; Paulsen, S.M.; Tungen, J.E.; Vik, A.; Aursnes, M.; Holen, T.; Hansen, T.V.; Nebb, H.I. Synthesis and biological evaluations of marine oxohexadecenoic acids: PPARalpha/gamma dual agonism and anti-diabetic target gene effects. Eur. J. Med. Chem. 2018, 155, 736–753. [Google Scholar] [CrossRef]
- Carmona, M.C.; Louche, K.; Lefebvre, B.; Pilon, A.; Hennuyer, N.; Audinot-Bouchez, V.; Fievet, C.; Torpier, G.; Formstecher, P.; Renard, P.; et al. S 26948: A new specific peroxisome proliferator activated receptor gamma modulator with potent antidiabetes and antiatherogenic effects. Diabetes 2007, 56, 2797–2808. [Google Scholar] [CrossRef] [PubMed]
- Seargent, J.M.; Yates, E.A.; Gill, J.H. GW9662, a potent antagonist of PPARgamma, inhibits growth of breast tumour cells and promotes the anticancer effects of the PPARgamma agonist rosiglitazone, independently of PPARgamma activation. Br. J. Pharmacol. 2004, 143, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Altmann, R.; Hausmann, M.; Spottl, T.; Gruber, M.; Bull, A.W.; Menzel, K.; Vogl, D.; Herfarth, H.; Scholmerich, J.; Falk, W.; et al. 13-Oxo-ODE is an endogenous ligand for PPARgamma in human colonic epithelial cells. Biochem. Pharmacol. 2007, 74, 612–622. [Google Scholar] [CrossRef] [PubMed]
- Ljung, B.; Bamberg, K.; Dahllof, B.; Kjellstedt, A.; Oakes, N.D.; Ostling, J.; Svensson, L.; Camejo, G. AZ 242, a novel PPARalpha/gamma agonist with beneficial effects on insulin resistance and carbohydrate and lipid metabolism in ob/ob mice and obese Zucker rats. J. Lipid Res. 2002, 43, 1855–1863. [Google Scholar] [CrossRef]
- Leghmar, K.; Cenac, N.; Rolland, M.; Martin, H.; Rauwel, B.; Bertrand-Michel, J.; Le Faouder, P.; Benard, M.; Casper, C.; Davrinche, C.; et al. Cytomegalovirus Infection Triggers the Secretion of the PPARgamma Agonists 15-Hydroxyeicosatetraenoic Acid (15-HETE) and 13-Hydroxyoctadecadienoic Acid (13-HODE) in Human Cytotrophoblasts and Placental Cultures. PLoS ONE 2015, 10, e0132627. [Google Scholar] [CrossRef]
- Cesario, R.M.; Klausing, K.; Razzaghi, H.; Crombie, D.; Rungta, D.; Heyman, R.A.; Lala, D.S. The rexinoid LG100754 is a novel RXR:PPARgamma agonist and decreases glucose levels in vivo. Mol. Endocrinol. 2001, 15, 1360–1369. [Google Scholar] [CrossRef]
- Kurtz, T.W. Treating the metabolic syndrome: Telmisartan as a peroxisome proliferator-activated receptor-gamma activator. Acta Diabetol. 2005, 42 (Suppl. 1), S9–S16. [Google Scholar] [CrossRef]
- Zhang, Z.Z.; Shang, Q.H.; Jin, H.Y.; Song, B.; Oudit, G.Y.; Lu, L.; Zhou, T.; Xu, Y.L.; Gao, P.J.; Zhu, D.L.; et al. Cardiac protective effects of irbesartan via the PPAR-gamma signaling pathway in angiotensin-converting enzyme 2-deficient mice. J. Transl. Med. 2013, 11, 229. [Google Scholar] [CrossRef]
- Tenenbaum, A.; Motro, M.; Fisman, E.Z.; Schwammenthal, E.; Adler, Y.; Goldenberg, I.; Leor, J.; Boyko, V.; Mandelzweig, L.; Behar, S. Peroxisome proliferator-activated receptor ligand bezafibrate for prevention of type 2 diabetes mellitus in patients with coronary artery disease. Circulation 2004, 109, 2197–2202. [Google Scholar] [CrossRef]
- Schug, T.T.; Berry, D.C.; Shaw, N.S.; Travis, S.N.; Noy, N. Opposing effects of retinoic acid on cell growth result from alternate activation of two different nuclear receptors. Cell 2007, 129, 723–733. [Google Scholar] [CrossRef]
- Kumagai, T.; Ikezoe, T.; Gui, D.; O’Kelly, J.; Tong, X.J.; Cohen, F.J.; Said, J.W.; Koeffler, H.P. RWJ-241947 (MCC-555), a unique peroxisome proliferator-activated receptor-gamma ligand with antitumor activity against human prostate cancer in vitro and in beige/nude/ X-linked immunodeficient mice and enhancement of apoptosis in myeloma cells induced by arsenic trioxide. Clin. Cancer Res. 2004, 10, 1508–1520. [Google Scholar] [CrossRef] [PubMed]
- Fukui, Y.; Masui, S.; Osada, S.; Umesono, K.; Motojima, K. A new thiazolidinedione, NC-2100, which is a weak PPAR-gamma activator, exhibits potent antidiabetic effects and induces uncoupling protein 1 in white adipose tissue of KKAy obese mice. Diabetes 2000, 49, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Tsunoda, M.; Ide, T.; Ohashi, M.; Mochizuki, T. Amelioration by KRP-297, a new thiazolidinedione, of impaired glucose uptake in skeletal muscle from obese insulin-resistant animals. Metabolism 1999, 48, 1450–1454. [Google Scholar] [CrossRef]
- Christofides, A.; Konstantinidou, E.; Jani, C.; Boussiotis, V.A. The role of peroxisome proliferator-activated receptors (PPAR) in immune responses. Metabolism 2021, 114, 154338. [Google Scholar] [CrossRef] [PubMed]
- Giaginis, C.; Tsantili-Kakoulidou, A.; Theocharis, S. Peroxisome Proliferator-Activated Receptor-gamma Ligands: Potential Pharmacological Agents for Targeting the Angiogenesis Signaling Cascade in Cancer. PPAR Res. 2008, 2008, 431763. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Ye, Y.; Mullikin, H.; Lin, L.; Kuhn, C.; Rahmeh, M.; Mahner, S.; Jeschke, U.; von Schonfeldt, V. Expression of trophoblast derived prostaglandin E2 receptor 2 (EP2) is reduced in patients with recurrent miscarriage and EP2 regulates cell proliferation and expression of inflammatory cytokines. J. Reprod. Immunol. 2020, 142, 103210. [Google Scholar] [CrossRef] [PubMed]
- Barak, Y.; Nelson, M.C.; Ong, E.S.; Jones, Y.Z.; Ruiz-Lozano, P.; Chien, K.R.; Koder, A.; Evans, R.M. PPAR gamma is required for placental, cardiac, and adipose tissue development. Mol. Cell 1999, 4, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Fujii, H.; Knipp, G.T. Expression of PPAR and RXR isoforms in the developing rat and human term placentas. Placenta 2002, 23, 661–671. [Google Scholar] [CrossRef]
- Peng, L.; Yang, H.; Ye, Y.; Ma, Z.; Kuhn, C.; Rahmeh, M.; Mahner, S.; Makrigiannakis, A.; Jeschke, U.; von Schonfeldt, V. Role of Peroxisome Proliferator-Activated Receptors (PPARs) in Trophoblast Functions. Int. J. Mol. Sci. 2021, 22, 433. [Google Scholar] [CrossRef]
- Diaz, M.; Bassols, J.; Lopez-Bermejo, A.; Gomez-Roig, M.D.; de Zegher, F.; Ibanez, L. Placental expression of peroxisome proliferator-activated receptor gamma (PPARgamma): Relation to placental and fetal growth. J. Clin. Endocrinol. Metab. 2012, 97, E1468–E1472. [Google Scholar] [CrossRef]
- Christians, J.K.; Beristain, A.G. ADAM12 and PAPP-A: Candidate regulators of trophoblast invasion and first trimester markers of healthy trophoblasts. Cell. Adh Migr. 2016, 10, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Fournier, T.; Handschuh, K.; Tsatsaris, V.; Evain-Brion, D. Involvement of PPARgamma in human trophoblast invasion. Placenta 2007, 28 (Suppl. A), S76–S81. [Google Scholar] [CrossRef] [PubMed]
- Tarrade, A.; Schoonjans, K.; Pavan, L.; Auwerx, J.; Rochette-Egly, C.; Evain-Brion, D.; Fournier, T. PPARgamma/RXRalpha heterodimers control human trophoblast invasion. J. Clin. Endocrinol. Metab. 2001, 86, 5017–5024. [Google Scholar] [CrossRef] [PubMed]
- Handschuh, K.; Guibourdenche, J.; Guesnon, M.; Laurendeau, I.; Evain-Brion, D.; Fournier, T. Modulation of PAPP-A expression by PPARgamma in human first trimester trophoblast. Placenta 2006, 27 (Suppl. A), S127–S134. [Google Scholar] [CrossRef]
- Mayama, R.; Izawa, T.; Sakai, K.; Suciu, N.; Iwashita, M. Improvement of insulin sensitivity promotes extravillous trophoblast cell migration stimulated by insulin-like growth factor-I. Endocr. J. 2013, 60, 359–368. [Google Scholar] [CrossRef]
- Bilban, M.; Haslinger, P.; Prast, J.; Klinglmuller, F.; Woelfel, T.; Haider, S.; Sachs, A.; Otterbein, L.E.; Desoye, G.; Hiden, U.; et al. Identification of novel trophoblast invasion-related genes: Heme oxygenase-1 controls motility via peroxisome proliferator-activated receptor gamma. Endocrinology 2009, 150, 1000–1013. [Google Scholar] [CrossRef]
- Garnier, V.; Traboulsi, W.; Salomon, A.; Brouillet, S.; Fournier, T.; Winkler, C.; Desvergne, B.; Hoffmann, P.; Zhou, Q.Y.; Congiu, C.; et al. PPARgamma controls pregnancy outcome through activation of EG-VEGF: New insights into the mechanism of placental development. Am. J. Physiol. Endocrinol. Metab. 2015, 309, E357–E369. [Google Scholar] [CrossRef]
- Kadam, L.; Kilburn, B.; Baczyk, D.; Kohan-Ghadr, H.R.; Kingdom, J.; Drewlo, S. Rosiglitazone blocks first trimester in-vitro placental injury caused by NF-kappaB-mediated inflammation. Sci. Rep. 2019, 9, 2018. [Google Scholar] [CrossRef]
- Zhang, Z.; Yang, Y.; Lv, X.; Liu, H. Interleukin-17 promotes proliferation, migration, and invasion of trophoblasts via regulating PPAR-gamma/RXR-alpha/Wnt signaling. Bioengineered 2022, 13, 1224–1234. [Google Scholar] [CrossRef]
- Shoaito, H.; Chauveau, S.; Gosseaume, C.; Bourguet, W.; Vigouroux, C.; Vatier, C.; Pienkowski, C.; Fournier, T.; Degrelle, S.A. Peroxisome proliferator-activated receptor gamma-ligand-binding domain mutations associated with familial partial lipodystrophy type 3 disrupt human trophoblast fusion and fibroblast migration. J. Cell. Mol. Med. 2020, 24, 7660–7669. [Google Scholar] [CrossRef]
- Levytska, K.; Drewlo, S.; Baczyk, D.; Kingdom, J. PPAR-gamma Regulates Trophoblast Differentiation in the BeWo Cell Model. PPAR Res. 2014, 2014, 637251. [Google Scholar] [CrossRef] [PubMed]
- Tarrade, A.; Schoonjans, K.; Guibourdenche, J.; Bidart, J.M.; Vidaud, M.; Auwerx, J.; Rochette-Egly, C.; Evain-Brion, D. PPAR gamma/RXR alpha heterodimers are involved in human CG beta synthesis and human trophoblast differentiation. Endocrinology 2001, 142, 4504–4514. [Google Scholar] [CrossRef] [PubMed]
- Milstone, D.S.; Pierre, M.A.; Mana, P.M.; O’Donnell, P.E.; Davis, V.M.; Cross, J.C.; Mortensen, R.M.; Stavrakis, G. PPAR gamma is expressed and regulates placental development and trophoblast differentiation in both humans and mice. FASEB 2006, 20, A1077. [Google Scholar] [CrossRef]
- Elchalal, U.; Humphrey, R.G.; Smith, S.D.; Hu, C.; Sadovsky, Y.; Nelson, D.M. Troglitazone attenuates hypoxia-induced injury in cultured term human trophoblasts. Am. J. Obstet. Gynecol. 2004, 191, 2154–2159. [Google Scholar] [CrossRef]
- Tache, V.; Ciric, A.; Moretto-Zita, M.; Li, Y.; Peng, J.; Maltepe, E.; Milstone, D.S.; Parast, M.M. Hypoxia and trophoblast differentiation: A key role for PPARgamma. Stem Cells Dev. 2013, 22, 2815–2824. [Google Scholar] [CrossRef] [PubMed]
- Parast, M.M.; Yu, H.; Ciric, A.; Salata, M.W.; Davis, V.; Milstone, D.S. PPARgamma regulates trophoblast proliferation and promotes labyrinthine trilineage differentiation. PLoS ONE 2009, 4, e8055. [Google Scholar] [CrossRef]
- Fox, R.; Kitt, J.; Leeson, P.; Aye, C.Y.L.; Lewandowski, A.J. Preeclampsia: Risk Factors, Diagnosis, Management, and the Cardiovascular Impact on the Offspring. J. Clin. Med. 2019, 8, 1625. [Google Scholar] [CrossRef]
- Rana, S.; Lemoine, E.; Granger, J.P.; Karumanchi, S.A. Preeclampsia: Pathophysiology, Challenges, and Perspectives. Circ. Res. 2019, 124, 1094–1112. [Google Scholar] [CrossRef]
- Backes, C.H.; Markham, K.; Moorehead, P.; Cordero, L.; Nankervis, C.A.; Giannone, P.J. Maternal preeclampsia and neonatal outcomes. J. Pregnancy 2011, 2011, 214365. [Google Scholar] [CrossRef]
- Huppertz, B. Placental origins of preeclampsia: Challenging the current hypothesis. Hypertension 2008, 51, 970–975. [Google Scholar] [CrossRef]
- Staff, A.C. The two-stage placental model of preeclampsia: An update. J. Reprod. Immunol. 2019, 134–135, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.M.; Hubel, C.A. The two stage model of preeclampsia: Variations on the theme. Placenta 2009, 30 (Suppl. A), S32–S37. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.M. Pathophysiology of ischemic placental disease. Semin. Perinatol. 2014, 38, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Wu, J.; Hu, J. Correlations of MMP-9 and PPARγ gene polymorphisms with occurrence of preeclampsia. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 771–778. [Google Scholar]
- Holdsworth-Carson, S.; Lim, R.; Mitton, A.; Whitehead, C.; Rice, G.E.; Permezel, M.; Lappas, M. Peroxisome proliferator-activated receptors are altered in pathologies of the human placenta: Gestational diabetes mellitus, intrauterine growth restriction and preeclampsia. Placenta 2010, 31, 222–229. [Google Scholar] [CrossRef]
- Mahendra, J.; Parthiban, P.S.; Mahendra, L.; Balakrishnan, A.; Shanmugam, S.; Junaid, M.; Romanos, G.E. Evidence linking the role of placental expressions of Peroxisome Proliferator-Activated Receptor-γ and Nuclear Factor-Kappa B in the pathogenesis of preeclampsia associated with periodontitis. J. Periodontol. 2016, 87, 962–970. [Google Scholar] [CrossRef]
- Armistead, B.; Kadam, L.; Siegwald, E.; McCarthy, F.P.; Kingdom, J.C.; Kohan-Ghadr, H.R.; Drewlo, S. Induction of the PPARγ (Peroxisome Proliferator-Activated Receptor γ)-GCM1 (Glial Cell Missing 1) Syncytialization Axis Reduces sFLT1 (Soluble fms-Like Tyrosine Kinase 1) in the Preeclamptic Placenta. Hypertension 2021, 78, 230–240. [Google Scholar] [CrossRef]
- He, P.; Chen, Z.; Sun, Q.; Li, Y.; Gu, H.; Ni, X. Reduced expression of 11β-hydroxysteroid dehydrogenase type 2 in preeclamptic placentas is associated with decreased PPARγ but increased PPARα expression. Endocrinology 2014, 155, 299–309. [Google Scholar] [CrossRef]
- Permadi, W.; Mantilidewi, K.I.; Khairani, A.F.; Lantika, U.A.; Ronosulistyo, A.R.; Bayuaji, H. Differences in expression of Peroxisome Proliferator-activated Receptor-gamma in early-onset preeclampsia and late-onset preeclampsia. BMC Res. Notes 2020, 13, 181. [Google Scholar] [CrossRef]
- Zeisler, H.; Llurba, E.; Chantraine, F.; Vatish, M.; Staff, A.C.; Sennstrom, M.; Olovsson, M.; Brennecke, S.P.; Stepan, H.; Allegranza, D.; et al. Predictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia. N. Engl. J. Med. 2016, 374, 13–22. [Google Scholar] [CrossRef]
- Liu, L.; Wang, R.; Xu, R.; Chu, Y.; Gu, W. Procyanidin B2 ameliorates endothelial dysfunction and impaired angiogenesis via the Nrf2/PPARgamma/sFlt-1 axis in preeclampsia. Pharmacol. Res. 2022, 177, 106127. [Google Scholar] [CrossRef]
- Liu, L.; Zhuang, X.; Jiang, M.; Guan, F.; Fu, Q.; Lin, J. ANGPTL4 mediates the protective role of PPARγ activators in the pathogenesis of preeclampsia. Cell. Death Dis. 2017, 8, e3054. [Google Scholar] [CrossRef] [PubMed]
- Kamrani, A.; Alipourfard, I.; Ahmadi-Khiavi, H.; Yousefi, M.; Rostamzadeh, D.; Izadi, M.; Ahmadi, M. The role of epigenetic changes in preeclampsia. Biofactors 2019, 45, 712–724. [Google Scholar] [CrossRef] [PubMed]
- Meister, S.; Hahn, L.; Beyer, S.; Paul, C.; Mitter, S.; Kuhn, C.; von Schönfeldt, V.; Corradini, S.; Sudan, K.; Schulz, C.; et al. Regulation of Epigenetic Modifications in the Placenta during Preeclampsia: PPARγ Influences H3K4me3 and H3K9ac in Extravillous Trophoblast Cells. Int. J. Mol. Sci. 2021, 22, 12469. [Google Scholar] [CrossRef]
- Bianco-Miotto, T.; Mayne, B.T.; Buckberry, S.; Breen, J.; Rodriguez Lopez, C.M.; Roberts, C.T. Recent progress towards understanding the role of DNA methylation in human placental development. Reproduction 2016, 152, R23–R30. [Google Scholar] [CrossRef] [PubMed]
- Nelissen, E.C.; van Montfoort, A.P.; Dumoulin, J.C.; Evers, J.L. Epigenetics and the placenta. Hum. Reprod. Update 2011, 17, 397–417. [Google Scholar] [CrossRef]
- Li, J.; LaMarca, B.; Reckelhoff, J.F. A model of preeclampsia in rats: The reduced uterine perfusion pressure (RUPP) model. Am. J. Physiol. Heart Circ. Physiol. 2012, 303, H1–H8. [Google Scholar] [CrossRef]
- McCarthy, F.P.; Drewlo, S.; Kingdom, J.; Johns, E.J.; Walsh, S.K.; Kenny, L.C. Peroxisome proliferator-activated receptor-gamma as a potential therapeutic target in the treatment of preeclampsia. Hypertension 2011, 58, 280–286. [Google Scholar] [CrossRef]
- Zhang, C.; Zhu, Y.; Shen, Y.; Zuo, C. Aspirin ameliorates preeclampsia induced by a peroxisome proliferator-activated receptor antagonist. Reprod. Sci. 2018, 25, 1655–1662. [Google Scholar] [CrossRef]
- McCarthy, F.P.; Drewlo, S.; English, F.A.; Kingdom, J.; Johns, E.J.; Kenny, L.C.; Walsh, S.K. Evidence implicating peroxisome proliferator-activated receptor-γ in the pathogenesis of preeclampsia. Hypertension 2011, 58, 882–887. [Google Scholar] [CrossRef]
- Guo, Y.; Zhu, Y.; Sun, Y.; Yang, H. The preventive effect of low-dose aspirin in a PPAR-γ antagonist treated mouse model of preeclampsia. BMC Pregnancy Childbirth 2022, 22, 606. [Google Scholar] [CrossRef] [PubMed]
- National Center for Biotechnology Information. Angiotensin (1-7). Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Angiotensin-_1-7 (accessed on 11 May 2023).
- El-Saka, M.H.; Madi, N.M.; Ibrahim, R.R.; Alghazaly, G.M.; Elshwaikh, S.; El-Bermawy, M. The ameliorative effect of angiotensin 1-7 on experimentally induced-preeclampsia in rats: Targeting the role of peroxisome proliferator-activated receptors gamma expression & asymmetric dimethylarginine. Arch. Biochem. Biophys. 2019, 671, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, T.A.; Xiang, A.H.; Page, K.A. Gestational diabetes mellitus: Risks and management during and after pregnancy. Nat. Rev. Endocrinol. 2012, 8, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Damm, P. Future risk of diabetes in mother and child after gestational diabetes mellitus. Int. J. Gynaecol. Obstet. 2009, 104 (Suppl. 1), S25–S26. [Google Scholar] [CrossRef] [PubMed]
- Weissgerber, T.L.; Mudd, L.M. Preeclampsia and diabetes. Curr. Diab Rep. 2015, 15, 9. [Google Scholar] [CrossRef]
- Yang, Y.; Wu, N. Gestational Diabetes Mellitus and Preeclampsia: Correlation and Influencing Factors. Front. Cardiovasc. Med. 2022, 9, 831297. [Google Scholar] [CrossRef]
- Karagiannis, T.; Bekiari, E.; Manolopoulos, K.; Paletas, K.; Tsapas, A. Gestational diabetes mellitus: Why screen and how to diagnose. Hippokratia 2010, 14, 151–154. [Google Scholar]
- Qin, Y.; McCauley, N.; Ding, Z.; Lawless, L.; Liu, Z.; Zhang, K.; Xie, L. Hyperglycemia results in significant pathophysiological changes of placental spiral artery remodeling and angiogenesis, further contributing to congenital defects. Front. Biosci. 2021, 26, 965–976. [Google Scholar] [CrossRef]
- Hay, W.W., Jr. Placental-fetal glucose exchange and fetal glucose metabolism. Trans. Am. Clin. Climatol. Assoc. 2006, 117, 321–339; discussion 339–340. [Google Scholar]
- Balsells, M.; Garcia-Patterson, A.; Sola, I.; Roque, M.; Gich, I.; Corcoy, R. Glibenclamide, metformin, and insulin for the treatment of gestational diabetes: A systematic review and meta-analysis. BMJ 2015, 350, h102. [Google Scholar] [CrossRef]
- Jamilian, M.; Samimi, M.; Mirhosseini, N.; Afshar Ebrahimi, F.; Aghadavod, E.; Taghizadeh, M.; Asemi, Z. A Randomized Double-Blinded, Placebo-Controlled Trial Investigating the Effect of Fish Oil Supplementation on Gene Expression Related to Insulin Action, Blood Lipids, and Inflammation in Gestational Diabetes Mellitus-Fish Oil Supplementation and Gestational Diabetes. Nutrients 2018, 10, 163. [Google Scholar] [CrossRef] [PubMed]
- Holmes, H.J.; Casey, B.M.; Bawdon, R.E. Placental transfer of rosiglitazone in the ex vivo human perfusion model. Am. J. Obstet. Gynecol. 2006, 195, 1715–1719. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.Y.; Yeung, J.H.; Lau, T.K. Placental transfer of rosiglitazone in the first trimester of human pregnancy. Fertil. Steril. 2005, 83, 955–958. [Google Scholar] [CrossRef] [PubMed]
- Nanovskaya, T.N.; Patrikeeva, S.; Hemauer, S.; Fokina, V.; Mattison, D.; Hankins, G.D.; Ahmed, M.S.; Network, O. Effect of albumin on transplacental transfer and distribution of rosiglitazone and glyburide. J. Matern.-Fetal Neonatal Med. 2008, 21, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Klinkner, D.B.; Lim, H.J.; Strawn, E.Y., Jr.; Oldham, K.T.; Sander, T.L. An in vivo murine model of rosiglitazone use in pregnancy. Fertil. Steril. 2006, 86, 1074–1079. [Google Scholar] [CrossRef] [PubMed]
- Kalyoncu, N.I.; Yaris, F.; Ulku, C.; Kadioglu, M.; Kesim, M.; Unsal, M.; Dikici, M.; Yaris, E. A case of rosiglitazone exposure in the second trimester of pregnancy. Reprod. Toxicol. 2005, 19, 563–564. [Google Scholar] [CrossRef]
- Sağır, D.; Eren, B.; Yılmaz, B.; Eren, Z.; Keleş, O.; Gökçe, A. Effects of prenatal PPAR-γ agonist rosiglitazone exposure on rat hippocampus development in a time-dependent manner: A stereological and histopathological study. Human. Exp. Toxicol. 2018, 37, 827–835. [Google Scholar] [CrossRef]
- Chan, L.Y.; Lau, T.K. Effect of rosiglitazone on embryonic growth and morphology: A study using a whole rat embryo culture model. Fertil. Steril. 2006, 86, 490–492. [Google Scholar] [CrossRef]
- Schaiff, W.T.; Knapp, F.F., Jr.; Barak, Y.; Biron-Shental, T.; Nelson, D.M.; Sadovsky, Y. Ligand-activated peroxisome proliferator activated receptor gamma alters placental morphology and placental fatty acid uptake in mice. Endocrinology 2007, 148, 3625–3634. [Google Scholar] [CrossRef]
- Nadra, K.; Quignodon, L.; Sardella, C.; Joye, E.; Mucciolo, A.; Chrast, R.; Desvergne, B. PPARgamma in placental angiogenesis. Endocrinology 2010, 151, 4969–4981. [Google Scholar] [CrossRef]
- Petrik, J.J.; Gerstein, H.C.; Cesta, C.E.; Kellenberger, L.D.; Alfaidy, N.; Holloway, A.C. Effects of rosiglitazone on ovarian function and fertility in animals with reduced fertility following fetal and neonatal exposure to nicotine. Endocrine 2009, 36, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; She, R.; Sha, W. Gestational diabetes mellitus is associated with decreased adipose and placenta peroxisome proliferator-activator receptor γ expression in a Chinese population. Oncotarget 2017, 8, 113928. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Yang, D.; Gao, L.; Zhao, M.; He, X.; Zhu, M.; Tian, C.; Liu, G.; Li, L.; Hu, C. Downregulation of peroxisome proliferator-activated receptor gamma in the placenta correlates to hyperglycemia in offspring at young adulthood after exposure to gestational diabetes mellitus. J. Diabetes Investig. 2019, 10, 499–512. [Google Scholar] [CrossRef] [PubMed]
- Knabl, J.; Huttenbrenner, R.; Hutter, S.; Gunthner-Biller, M.; Vrekoussis, T.; Karl, K.; Friese, K.; Kainer, F.; Jeschke, U. Peroxisome proliferator-activated receptor-gamma (PPARgamma) is down regulated in trophoblast cells of gestational diabetes mellitus (GDM) and in trophoblast tumour cells BeWo in vitro after stimulation with PPARgamma agonists. J. Perinat. Med. 2014, 42, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.J.; Vanderpeet, C.L.; Bartho, L.A.; McKeating, D.R.; Cuffe, J.S.M.; Holland, O.J.; Perkins, A.V. Mitochondrial dysfunction in placental trophoblast cells experiencing gestational diabetes mellitus. J. Physiol. 2021, 599, 1291–1305. [Google Scholar] [CrossRef] [PubMed]
- Suwaki, N.; Masuyama, H.; Masumoto, A.; Takamoto, N.; Hiramatsu, Y. Expression and potential role of peroxisome proliferator-activated receptor gamma in the placenta of diabetic pregnancy. Placenta 2007, 28, 315–323. [Google Scholar] [CrossRef]
- Wójcik, M.; Mac-Marcjanek, K.; Nadel, I.; Woźniak, L.; Cypryk, K. Gestational diabetes mellitus is associated with increased leukocyte peroxisome proliferator-activated receptor γ expression. Arch. Med. Sci. 2015, 11, 779–787. [Google Scholar] [CrossRef]
- Han, C.S.; Herrin, M.A.; Pitruzzello, M.C.; Mulla, M.J.; Werner, E.F.; Pettker, C.M.; Flannery, C.A.; Abrahams, V.M. Glucose and metformin modulate human first trimester trophoblast function: A model and potential therapy for diabetes-associated uteroplacental insufficiency. Am. J. Reprod. Immunol. 2015, 73, 362–371. [Google Scholar] [CrossRef]
- Jawerbaum, A.; Capobianco, E.; Pustovrh, C.; White, V.; Baier, M.; Salzberg, S.; Pesaresi, M.; Gonzalez, E. Influence of peroxisome proliferator-activated receptor gamma activation by its endogenous ligand 15-deoxy Delta12,14 prostaglandin J2 on nitric oxide production in term placental tissues from diabetic women. Mol. Hum. Reprod. 2004, 10, 671–676. [Google Scholar] [CrossRef]
- Zhang, J.; Bai, W.P. C1q/tumor necrosis factor related protein 6 (CTRP6) regulates the phenotypes of high glucose-induced gestational trophoblast cells via peroxisome proliferator-activated receptor gamma (PPARgamma) signaling. Bioengineered 2022, 13, 206–216. [Google Scholar] [CrossRef]
- Zhou, X.; Wei, L.-J.; Li, J.-Q.; Zhang, J.-Y.; Zhu, S.-L.; Zhang, H.-T.; Jia, J.; Yu, J.; Wang, S.-S.; Feng, L.; et al. The Activation of Peroxisome Proliferator-activated Receptor γ Enhances Insulin Signaling Pathways via Up-regulating Chemerin Expression in High Glucose Treated HTR-8/SVneo Cells. Matern.-Fetal Med. 2020, 2, 131–140. [Google Scholar] [CrossRef]
- Jin, D.; Sun, J.; Huang, J.; Yu, X.; Yu, A.; He, Y.; Li, Q.; Yang, Z. Peroxisome proliferator-activated receptor gamma enhances adiponectin secretion via up-regulating DsbA-L expression. Mol. Cell. Endocrinol. 2015, 411, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Li, J.Q.; Wei, L.J.; He, M.Z.; Jia, J.; Zhang, J.Y.; Wang, S.S.; Feng, L. Silencing of DsbA-L gene impairs the PPARgamma agonist function of improving insulin resistance in a high-glucose cell model. J. Zhejiang Univ. Sci. B 2020, 21, 990–998. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Agonists | Antagonists | ||
|---|---|---|---|
| Natural Ligand | Synthetic Ligand | Natural Ligand | Synthetic Ligand |
| Unsaturated fatty acid ** [15] | GW1929 [16] | Betulinic acid [17] | SR-202 [18] |
| Oxidized LDL [19] | TZD *** | NFκB [20] | BADGE [21] |
| EETs [22] | FMOC-L-Leucine [23] | Fetuin A [20] | LG100641 [24] |
| 15d-PGJ2 [25] | INT131 [26] | PD068235 [27] | |
| Azelaoyl phosphatidylcholine [28] | Farglitazar (GI262570) [29] | T0070907 [30] | |
| 9-oxoODE [31] | S26948 [32] | GW9662 [33] | |
| 13-oxoODE [34] | AZ 242 [35] | ||
| 15-HETE [36] | LG100754 [37] | ||
| 13-HODE [36] | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, Y.; Bily, D.; Aguirre, M.; Zhang, K.; Xie, L. Understanding PPARγ and Its Agonists on Trophoblast Differentiation and Invasion: Potential Therapeutic Targets for Gestational Diabetes Mellitus and Preeclampsia. Nutrients 2023, 15, 2459. https://doi.org/10.3390/nu15112459
Qin Y, Bily D, Aguirre M, Zhang K, Xie L. Understanding PPARγ and Its Agonists on Trophoblast Differentiation and Invasion: Potential Therapeutic Targets for Gestational Diabetes Mellitus and Preeclampsia. Nutrients. 2023; 15(11):2459. https://doi.org/10.3390/nu15112459
Chicago/Turabian StyleQin, Yushu, Donalyn Bily, Makayla Aguirre, Ke Zhang, and Linglin Xie. 2023. "Understanding PPARγ and Its Agonists on Trophoblast Differentiation and Invasion: Potential Therapeutic Targets for Gestational Diabetes Mellitus and Preeclampsia" Nutrients 15, no. 11: 2459. https://doi.org/10.3390/nu15112459