
Influence of N-Acetylcysteine Supplementation on Physical Performance and Laboratory Biomarkers in Adult Males: A Systematic Review of Controlled Trials

 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Elegibility Criteria
2.3. Information Sources
2.4. Search Methods
2.5. Methodological Quality Assessment
2.6. Risk of Bias Assessment
2.7. Study Selection
2.8. Data Extraction
2.9. Sumary Measures
3. Results
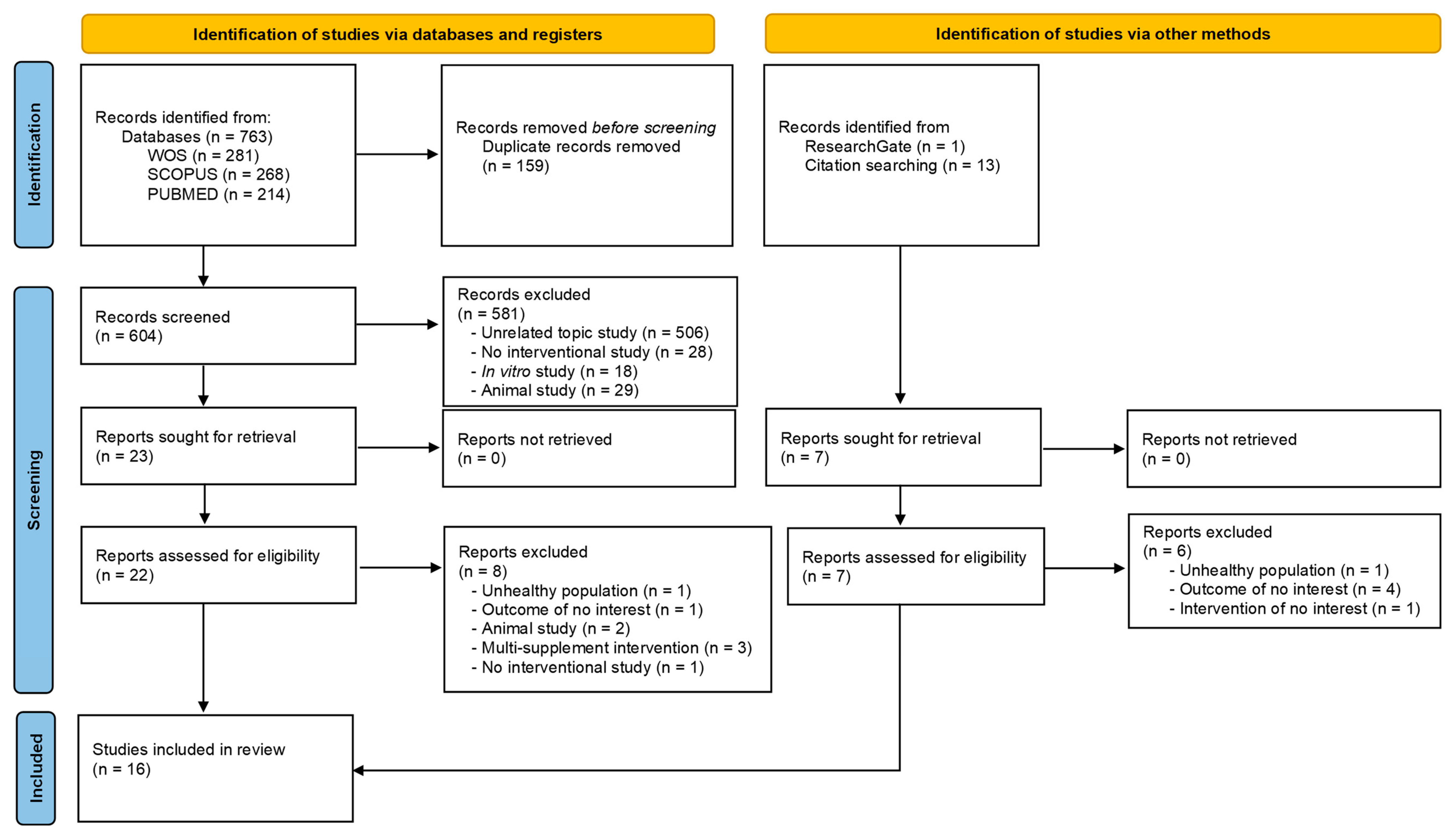
3.1. Study Selection
3.2. Quality Assessment
3.3. Risk of Bias Assessment
3.4. Characteristics of the Participants and Interventions
3.5. Outcome Evaluation
3.6. Physical Performance
3.7. Antioxidant Status
3.8. Glutathione Homeostasis
3.9. Inflammatory Response
3.10. Other Biomarkers
3.11. Adverse Effects
4. Discussion
4.1. N-Acetylcysteine Supplementation
4.2. Antioxidant Status
4.3. Glutathione Homeostasis
4.4. Inflammatory Response
4.5. Other Biomarkers
4.6. Physical Performance
4.7. Limitations
4.8. Future Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- García-Sánchez, A.; Miranda-Díaz, A.G.; Cardona-Muñoz, E.G. The Role of Oxidative Stress in Physiopathology and Pharmacological Treatment with Pro- and Antioxidant Properties in Chronic Diseases. Oxid. Med. Cell Longev. 2020, 2020, 2082145. [Google Scholar] [CrossRef]
- Jones, D.P. Redefining Oxidative Stress. Antioxid. Redox Signal. 2006, 8, 1865–1879. [Google Scholar] [CrossRef] [PubMed]
- Sies, H.; Berndt, C.; Jones, D.P. Oxidative Stress. Annu. Rev. Biochem. 2017, 86, 715–748. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.K.; Jackson, M.J. Exercise-induced oxidative stress: Cellular mechanisms and impact on muscle force production. Physiol. Rev. 2008, 88, 1243–1276. [Google Scholar] [CrossRef] [PubMed]
- Dröge, W. Free radicals in the physiological control of cell function. Physiol. Rev. 2002, 82, 47–95. [Google Scholar] [CrossRef]
- Dennis, K.K.; Go, Y.M.; Jones, D.P. Redox Systems Biology of Nutrition and Oxidative Stress. J. Nutr. 2019, 149, 553–565. [Google Scholar] [CrossRef]
- He, F.; Li, J.; Liu, Z.; Chuang, C.C.; Yang, W.; Zuo, L. Redox Mechanism of Reactive Oxygen Species in Exercise. Front. Physiol. 2016, 7, 486. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; Mielgo-Ayuso, J.; Calvo, J.S.; Martínez, A.C.; García, A.C.; Fernandez-Lazaro, C.I. Modulation of Exercise-Induced Muscle Damage, Inflammation, and Oxidative Markers by Curcumin Supplementation in a Physically Active Population: A Systematic Review. Nutrients 2020, 12, 501. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; Fernandez-Lazaro, C.I.; Mielgo-Ayuso, J.; Navascués, L.J.; Martínez, A.C.; Seco-Calvo, J. The Role of Selenium Mineral Trace Element in Exercise: Antioxidant Defense System, Muscle Performance, Hormone Response, and Athletic Performance. A Systematic Review. Nutrients 2020, 12, 1790. [Google Scholar] [CrossRef]
- Arazi, H.; Eghbali, E.; Suzuki, K. Creatine Supplementation, Physical Exercise and Oxidative Stress Markers: A Review of the Mechanisms and Effectiveness. Nutrients 2021, 13, 869. [Google Scholar] [CrossRef]
- Reid, M.B. Redox interventions to increase exercise performance. J. Physiol. 2016, 594, 5125–5133. [Google Scholar] [CrossRef] [PubMed]
- World Anti-Doping Agency, W.A.D.A. Prohibited List. Available online: https://www.wada-ama.org/sites/default/files/resources/files/2022list_final_en.pdf (accessed on 3 May 2023).
- Michailidis, Y.; Karagounis, L.G.; Terzis, G.; Jamurtas, A.Z.; Spengos, K.; Tsoukas, D.; Chatzinikolaou, A.; Mandalidis, D.; Stefanetti, R.J.; Papassotiriou, I.; et al. Thiol-based antioxidant supplementation alters human skeletal muscle signaling and attenuates its inflammatory response and recovery after intense eccentric exercise. Am. J. Clin. Nutr. 2013, 98, 233–245. [Google Scholar] [CrossRef]
- Šalamon, Š.; Kramar, B.; Marolt, T.P.; Poljšak, B.; Milisav, I. Medical and Dietary Uses of N-Acetylcysteine. Antioxidants 2019, 8, 111. [Google Scholar] [CrossRef]
- Tenório, M.C.D.S.; Graciliano, N.G.; Moura, F.A.; de Oliveira, A.C.M.; Goulart, M.O.F. N-Acetylcysteine (NAC): Impacts on Human Health. Antioxidants 2021, 10, 967. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, K.; Braakhuis, A. Performance and Side Effects of Supplementation with N-Acetylcysteine: A Systematic Review and Meta-Analysis. Sport Med. 2017, 47, 1619–1636. [Google Scholar] [CrossRef] [PubMed]
- Page Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Law, M.; Stewart, C.; Pollock, N.; Letts, L.; Bosch, J.; Westmorland, M. Guidelines for Critical Review of Qualitative Studies; McMaster University Occupational Therapy Evidence-Based Practice Research Group: Hamilton, ON, Canada, 1998; pp. 1–9. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef]
- Christensen, P.M.; Bangsbo, J. N-Acetyl cysteine does not improve repeated intense endurance cycling performance of well-trained cyclists. Eur. J. Appl. Physiol. 2019, 119, 1419–1429. [Google Scholar] [CrossRef]
- Corn, S.D.; Barstow, T.J. Effects of oral N-acetylcysteine on fatigue, critical power, and W’ in exercising humans. Respir. Physiol. Neurobiol. 2011, 178, 261–268. [Google Scholar] [CrossRef]
- Silva, L.A.; Silveira, P.C.L.; Pinho, C.A.; Tuon, T.; Pizzol, F.D.; Pinho, R.A. N-acetylcysteine supplementation and oxidative damage and inflammatory response after eccentric exercise. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Slattery, K.M.; Dascombe, B.; Wallace, L.K.; Bentley, D.J.; Coutts, A.J. Effect of N-acetylcysteine on cycling performance after intensified training. Med. Sci. Sports Exerc. 2014, 46, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.R.; Broxterman, R.M.; Ade, C.J.; Evans, K.K.; Kurti, S.P.; Hammer, S.M.; Barstow, T.J.; Harms, C.A. Acute supplementation of N-acetylcysteine does not affect muscle blood flow and oxygenation characteristics during handgrip exercise. Physiol. Rep. 2016, 4, e12748. [Google Scholar] [CrossRef] [PubMed]
- Zembron-Lacny, A.; Slowinska-Lisowska, M.; Szygula, Z.; Witkowski, Z.; Szyszka, K. Modulatory effect of N-acetylcysteine on pro-antioxidant status and haematological response in healthy men. J. Physiol. Biochem. 2010, 66, 15–21. [Google Scholar] [CrossRef]
- Zembron-Lacny, A.; Szyszka, K.; Szygula, Z. Effect of cysteine derivatives administration in healthy men exposed to intense resistance exercise by evaluation of pro-antioxidant ratio. J. Physiol. Sci. 2007, 57, 343–348. [Google Scholar] [CrossRef]
- Rhodes, K.M.; Baker, D.F.; Smith, B.T.; Braakhuis, A.J. Acute Effect of Oral N-Acetylcysteine on Muscle Soreness and Exercise Performance in Semi-Elite Rugby Players. J. Diet. Suppl. 2019, 16, 443–453. [Google Scholar] [CrossRef]
- Ferreira, L.F.; Campbell, K.S.; Reid, M.B. N-acetylcysteine in handgrip exercise: Plasma thiols and adverse reactions. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 146–154. [Google Scholar] [CrossRef]
- Leelarungrayub, D.; Khansuwan, R.; Pothongsunun, P.; Klaphajone, J. N-acetylcysteine supplementation controls total antioxidant capacity, creatine kinase, lactate, and tumor necrotic factor-alpha against oxidative stress induced by graded exercise in sedentary men. Oxid. Med. Cell Longev. 2011, 2011, 329643. [Google Scholar] [CrossRef]
- McKenna, M.J.; Medved, I.; Goodman, C.A.; Brown, M.J.; Bjorksten, A.R.; Murphy, K.T.; Petersen, A.C.; Sostaric, S.; Gong, X. N-acetylcysteine attenuates the decline in muscle Na+,K+-pump activity and delays fatigue during prolonged exercise in humans. J. Physiol. 2006, 576, 279–288. [Google Scholar] [CrossRef]
- Medved, I.; Brown, M.J.; Bjorksten, A.R.; Leppik, J.A.; Sostaric, S.; McKenna, M.J. N-acetylcysteine infusion alters blood redox status but not time to fatigue during intense exercise in humans. J. Appl. Physiol. 2003, 94, 1572–1582. [Google Scholar] [CrossRef]
- Medved, I.; Brown, M.J.; Bjorksten, A.R.; Murphy, K.T.; Petersen, A.C.; Sostaric, S.; Gong, X.; McKenna, M.J. N-acetylcysteine enhances muscle cysteine and glutathione availability and attenuates fatigue during prolonged exercise in endurance-trained individuals. J. Appl. Physiol. 2004, 97, 1477–1485. [Google Scholar] [CrossRef] [PubMed]
- Merry, T.L.; Wadley, G.D.; Stathis, C.G.; Garnham, A.P.; Rattigan, S.; Hargreaves, M.; McConell, G.K. N-Acetylcysteine infusion does not affect glucose disposal during prolonged moderate-intensity exercise in humans. J. Physiol. 2010, 588, 1623. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, H.B.; Secher, N.H.; Kappel, M.; Pedersen, B.K. N-acetylcysteine does not affect the lymphocyte proliferation and natural killer cell activity responses to exercise. Am. J. Physiol. 1998, 275, R1227–R1231. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.C.; McKenna, M.J.; Medved, I.; Murphy, K.T.; Brown, M.J.; Della Gatta, P.; Cameron-Smith, D. Infusion with the antioxidant N-acetylcysteine attenuates early adaptive responses to exercise in human skeletal muscle. Acta Physiol. 2012, 204, 382–392. [Google Scholar] [CrossRef]
- Borgström, L.; Kågedal, B.; Paulsen, O. Pharmacokinetics of N-acetylcysteine in man. Eur. J. Clin. Pharmacol. 1986, 31, 217–222. [Google Scholar] [CrossRef]
- Martínez de Victoria Muñoz, E.; Font Pérez, G.; Martínez-Larrañaga, M.R.; Picó Segura, C.; Ríos Cañavate, J.L.; Hardisson de la Torre, A. Informe del Comité Científico de la Agencia Española de Consumo, Seguridad Alimentaria y Nutrición (AECOSAN) sobre condiciones de uso de determinadas sustancias para ser empleadas en complementos alimenticios-3. Rev. Del. Com. Científico AESAN 2014, 19, 51–93. [Google Scholar]
- Salari-Moghaddam, A.; Nouri-Majd, S.; Keshteli, A.H.; Emami, F.; Esmaillzadeh, A.; Adibi, P. Association Between Dietary Total Antioxidant Capacity and Diet Quality in Adults. Front. Nutr. 2022, 9, 425. [Google Scholar] [CrossRef]
- Aldini, G.; Altomare, A.; Baron, G.; Vistoli, G.; Carini, M.; Borsani, L.; Sergio, F. N-Acetylcysteine as an antioxidant and disulphide breaking agent: The reasons why. Free Radic. Res 2018, 52, 751–762. [Google Scholar] [CrossRef]
- Margaritis, I.; Palazzetti, S.; Rousseau, A.S.; Richard, M.J.; Favier, A. Antioxidant supplementation and tapering exercise improve exercise-induced antioxidant response. J. Am. Coll. Nutr. 2003, 22, 147–156. [Google Scholar] [CrossRef]
- Aguilar Diaz De Leon, J.; Borges, C.R. Evaluation of Oxidative Stress in Biological Samples Using the Thiobarbituric Acid Reactive Substances Assay. J. Vis. Exp. 2020, 159, e61122. [Google Scholar]
- Zoppi, C.C.; Hohl, R.; Silva, F.C.; Lazarim, F.L.; Neto, J.M.; Stancanneli, M.; Macedo, D.V. Vitamin C and E Supplementation Effects in Professional Soccer Players Under Regular Training. J. Int. Soc. Sports Nutr. 2006, 3, 37. [Google Scholar] [CrossRef] [PubMed]
- Karakilcik, A.Z.; Halat, R.; Zerin, M.; Celik, H.N.Y. Effects of vitamin C and exercise on lipid profile, platelet and erythrocyte indices in young soccer players. J. Sport Med. Phys. Fit. 2014, 54, 665–671. [Google Scholar]
- Bavarsad Shahripour, R.; Harrigan, M.R.; Alexandrov, A.V. N-acetylcysteine (NAC) in neurological disorders: Mechanisms of action and therapeutic opportunities. Brain Behav. 2014, 4, 108–122. [Google Scholar] [CrossRef] [PubMed]
- McBean, G.J. Cysteine, Glutathione, and Thiol Redox Balance in Astrocytes. Antioxidants 2017, 6, 62. [Google Scholar] [CrossRef]
- Elbini Dhouib, I.; Jallouli, M.; Annabi, A.; Gharbi, N.; Elfazaa, S.; Lasram, M.M. A minireview on N-acetylcysteine: An old drug with new approaches. Life Sci. 2016, 151, 359–363. [Google Scholar] [CrossRef]
- Pirabbasi, E.; Shahar, S.; Manaf, Z.A.; Rajab, N.F.; Manap, R.A. Efficacy of Ascorbic Acid (Vitamin C) and/N-Acetylcysteine (NAC) Supplementation on Nutritional and Antioxidant Status of Male Chronic Obstructive Pulmonary Disease (COPD) Patients. J. Nutr. Sci. Vitaminol. 2016, 62, 54–61. [Google Scholar] [CrossRef]
- de la Asuncion, J.G.; Millan, A.; Pla, R.; Bruseghini, L.; Esteras, A.; Pallardo, F.V.; Sastre, J.; Viña, J. Mitochondrial glutathione oxidation correlates with age-associated oxidative damage to mitochondrial DNA. FASEB J. 1996, 10, 333–338. [Google Scholar] [CrossRef]
- Pedre, B.; Barayeu, U.; Ezeriņa, D.; Dick, T.P. The mechanism of action of N-acetylcysteine (NAC): The emerging role of H2S and sulfane sulfur species. Pharmacol. Ther. 2021, 228, 107916. [Google Scholar] [CrossRef]
- Lu, S.C. Regulation of glutathione synthesis. Mol. Aspects. Med. 2009, 30, 42–59. [Google Scholar] [CrossRef]
- Dodd, S.; Dean, O.; Copolov, D.L.; Malhi, G.S.; Berk, M. N-acetylcysteine for antioxidant therapy: Pharmacology and clinical utility. Expert. Opin. Biol. Ther. 2008, 8, 1955–1962. [Google Scholar] [CrossRef]
- de Andrade, K.Q.; Moura, F.A.; dos Santos, J.M.; de Araújo, O.R.P.; Santos, J.C.d.F.; Goulart, M.O.F. Oxidative Stress and Inflammation in Hepatic Diseases: Therapeutic Possibilities of N-Acetylcysteine. Int. J. Mol. Sci. 2015, 16, 30269–30308. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Lázaro, D.; Sánchez-Serrano, N.; Rabail, R.; Aadil, R.M.; Mielgo-Ayuso, J.; Radesca Fabiano, K.; Garrosa, E. Is Probiotics Supplementation an Appropriate Strategy to Modulate Inflammation in Physically Active Healthy Adults or Athletes? A Systematic Review. Appl. Sci. 2023, 13, 3448. [Google Scholar] [CrossRef]
- Sadowska, A.M.; Manuel-y-Keenoy, B.; Vertongen, T.; Schippers, G.; Radomska-Lesniewska, D.; Heytens, E.; De Backer, W.A. Effect of N-acetylcysteine on neutrophil activation markers in healthy volunteers: In vivo and in vitro study. Pharmacol. Res. 2006, 53, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Al-Shukaili, A.; Al-Abri, S.; Al-Ansari, A.; Monteil, M.A. Effect of N-acetyl-L-cysteine on Cytokine Production by Human Peripheral Blood Mononuclear Cells. Sultan. Qaboos Univ. Med. J. 2009, 9, 70–74. [Google Scholar]
- Hildebrandt, W.; Alexander, S.; Bärtsch, P.; Dröge, W. Effect of N-acetyl-cysteine on the hypoxic ventilatory response and erythropoietin production: Linkage between plasma thiol redox state and O(2) chemosensitivity. Blood 2002, 99, 1552–1555. [Google Scholar] [CrossRef] [PubMed]
- Vollaard, N.B.J.; Reeder, B.J.; Shearman, J.P.; Menu, P.; Wilson, M.T.; Cooper, C.E. A new sensitive assay reveals that hemoglobin is oxidatively modified in vivo. Free Radic. Biol. Med. 2005, 39, 1216–1228. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; Mielgo-Ayuso, J.; Del Valle Soto, M.; Adams, D.P.; Gutiérrez-Abejón, E.; Seco-Calvo, J. Impact of Optimal Timing of Intake of Multi-Ingredient Performance Supplements on Sports Performance, Muscular Damage, and Hormonal Behavior across a Ten-Week Training Camp in Elite Cyclists: A Randomized Clinical Trial. Nutrients 2021, 13, 3746. [Google Scholar] [CrossRef]
- Martínez-Ferrán, M.; Cuadrado-Peñafiel, V.; Sánchez-Andreo, J.M.; Villar-Lucas, M.; Castellanos-Montealegre, M.; Rubio-Martín, A.; Romero-Morales, C.; Casla-Barrio, S.; Pareja-Galeano, H. Effects of Acute Vitamin C plus Vitamin E Supplementation on Exercise-Induced Muscle Damage in Runners: A Double-Blind Randomized Controlled Trial. Nutrinets 2022, 14, 4635. [Google Scholar] [CrossRef]
- Kumar, P.; Liu, C.; Suliburk, J.; Hsu, J.W.; Muthupillai, R.; Jahoor, F.; Minard, C.G.; Taffet, G.E.; Sekhar, R.V. Supplementing Glycine and N-Acetylcysteine (GlyNAC) in Older Adults Improves Glutathione Deficiency, Oxidative Stress, Mitochondrial Dysfunction, Inflammation, Physical Function, and Aging Hallmarks: A Randomized Clinical Trial. J. Gerontol. A Biol. Sci. Med. Sci. 2023, 78, 75–89. [Google Scholar] [CrossRef]
- Kumar, P.; Liu, C.; Hsu, J.W.; Chacko, S.; Minard, C.; Jahoor, F.; Sekhar, R.V. Glycine and N-acetylcysteine (GlyNAC) supplementation in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, muscle strength, and cognition: Results of a pilot clinical trial. Clin. Transl. Med. 2021, 11, e372. [Google Scholar]
- Fernández-Lázaro, D.; Garrosa, E.; Seco-Calvo, J.; Garrosa, M. Potential Satellite Cell-Linked Biomarkers in Aging Skeletal Muscle Tissue: Proteomics and Proteogenomics to Monitor Sarcopenia. Proteomes 2022, 10, 29. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study, Year | Item | Total | % | Quality Score | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | ||||
| Christensen et al. [21], 2019 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 15 | 93.8 | E |
| Corn et al. [22], 2011 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 15 | 93.8 | E |
| Ferreira et al. [29], 2011 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 16 | 100 | E |
| Leelarungrayub et al. [30], 2011 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 13 | 81.3 | VG |
| McKenna et al. [31], 2006 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 14 | 87.5 | VG |
| Medved et al. [32], 2003 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 14 | 87.5 | VG |
| Medved et al. [33], 2004 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 15 | 93.8 | E |
| Merry et al. [34], 2010 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 14 | 87.5 | VG |
| Nielsen et al. [35], 1998 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 14 | 87.5 | VG |
| Petersen et al. [36], 2012 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 15 | 93.8 | E |
| Rhodes et al. [28], 2019 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 13 | 81.3 | VG |
| Silva et al. [23], 2008 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 15 | 93.8 | E |
| Slattery et al. [24], 2014 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 15 | 93.8 | E |
| Smith et al. [25], 2016 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 16 | 100 | E |
| Zembron-Lancy et al. [27], 2007 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 13 | 81.3 | VG |
| Zembron-Lancy et al. [26], 2010 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 13 | 81.3 | VG |
| Study, Year | Items | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total | |
| Christensen et al. [21], 2019 |  |  |  | | | | | | 6 |
| Corn et al. [22], 2011 | | | | | | | | | 6 |
| Ferreira et al. [29], 2011 | | | | | | | | | 6 |
| Leelarungrayub et al. [30], 2011 | | | | | | | | | 4 |
| McKenna et al. [31], 2006 | | | | | | | | | 6 |
| Medved et al. [32], 2003 | | | | | | | | | 6 |
| Medved et al. [33], 2004 | | | | | | | | | 5 |
| Merry et al. [34], 2010 | | | | | | | | | 5 |
| Nielsen et al. [35], 1998 | | | | | | | | | 6 |
| Petersen et al. [36], 2012 | | | | | | | | | 6 |
| Rhodes et al. [28], 2019 | | | | | | | | | 5 |
| Silva et al. [23], 2008 | | | | | | | | | 6 |
| Slattery et al. [24] | | | | | | | | | 5 |
| Smith et al. [25], 2016 | | | | | | | | | 6 |
| Zembron-Lancy et al. [27] | | | | | | | | | 5 |
| Zembron-Lancy et al. [26] | | | | | | | | | 5 |
| Characteristics | Types | Study |
|---|---|---|
| Participants | Healthy | [22,26,29,30,32] |
| Healthy physically active | [23,34] | |
| Trained | [21,24,25,27,28,31,33,35,36] | |
| Supplementation product | Registered product® | [21,22,24,27,28,29,30,34,35] |
| No reported | [23,25,26,31,32,33,36] | |
| Pharmaceutical form | Capsules | [21,22,23,24,25,28,29,35] |
| Oral solution | [29] | |
| Powder | [26,27,30] | |
| Intravenous solution | [31,32,33,34,36] | |
| Total dose | 20 mg/kg | [21] |
| 72.3 mg/kg | [22] | |
| 1000 mg/day (2 doses → 500 mg) | [28] | |
| 1200 mg/day (2 doses → 600 mg) | [24,26,30] | |
| 125 mg/kg/h during 15 min + 25 mg/kg/h during the test | [31,32,33,34,36] | |
| 6000 mg/day | [35] | |
| 10 mg/kg | [23] | |
| 70 mg/kg | [25] | |
| 1800 mg/day | [27] | |
| 9, 18, 37, 70, 140 mg/kg | [29] | |
| Duration (days) | 1 | [21,22,25,29,31,32,33,34,36] |
| 3 | [27,35] | |
| 6 | [28] | |
| 7 | [30] | |
| 8 | [26] | |
| 9 | [24] | |
| 21 | [23] | |
| Dose schedule | 60 min prior test | [21,22,25,29] |
| Morning, 1–2 h prior test | [28] | |
| Before lunch + before dinner | [24,26,27] | |
| During test | [31,32,33,34,36] | |
| Main Meal | [23,29,35] | |
| Before lunch + before dinner + prior test | [24] |
| First Author, Year of Publication, and Country | Study Design | Participants (Baseline Sample Size, Age, Sex, Withdrawals, and Final Group Sample Size) | Intervention | Outcomes | Results IG vs. CG |
|---|---|---|---|---|---|
| Christensen et al., 2019, Denmark [21] | Randomized, double-blind crossover, placebo-controlled trial | 11 ♂ Well-trained cyclists Age (mean ± SD) 28 ± 7 years Height (mean ± SD) 183 ± 7 cm Body mass (mean ± SD) 73 ± 10 kg Peak VO2max (mean ± SD) 69 ± 7 mL/min/kg Study withdrawals: 1 (to illness) n = 10 | 1500 mg (20 mg/kg) capsules NAC (Fagron BV, Rotterdam, The Netherlands) 60 min before the test 1 day Washout period: 6 days | Peak Power Blood Lactate Cycling Economy VO2max TAC Adverse reactions | ↔ Peak Power ↔ Blood Lactate ↔ Cycling Economy ↔ VO2max ↔TAC ↔ Side Effects |
| Corn et al., 2011 USA [22] | Randomized, double-blind crossover, placebo-controlled trial | 7 ♂ Healthy Age (Range) 20–24 years Body mass (mean ± SD) 89.1 ± 11 kg Height (mean ± SD) 183 ± 5 cm Study withdrawals: 0 | 72.3 ± 1.3 mg/kg Capsules NAC (Physiologics, Northglenn, CO, USA) 60 min before the test 1 day Washout period: 3 days | Peak Power Time to exhaustion (80, 90, 100, 110%) VO2max GSH | ↑* Peak Power ↑* Time to exhaustion 80% ↔ VO2max ↑* GSH |
| Ferreira et al., 2011 USA [29] | Randomized, double-blind crossover, placebo-controlled trial | 17 ♂ Healthy Age (mean ± SD) 30 ± 2 years Body Weight (mean ± SD) 86 ± 5 kg | 9 or 18 mg/kg capsules NAC (Physiologics, Northglenn, CO, USA), morning and evening before the test day 35.70 or 140 mg/kg liquid solution NAC (American Regent Laboratories Inc. Shirley, NY, USA), 60 min before the test 1 day Washout period: 7 days | GSH GSSG CySH CySS CySSG TGSH TCyS | ↑* GSH (140 mg/kg) ↓* GSSG (70, 140 mg/kg) ↑* CySH ↑* CySS ↓* CySSG (70, 140 mg/kg) ↔ TGSH ↑* TCyS ↔ CySH:TCyS ratio (capsules) ↑* CySH:TCyS ratio (líquid) |
| Leelarungrayub et al., 2011 Thailand [30] | Randomized controlled trial | 36 ♂ Healthy Age (range) 20–24 years Body mass index (range) 18.5–24.9 kg/m2 Study withdrawals: 7 16 participants IG 13 participants CG | 1200 mg/day Two doses (600 mg) NAC effervescent powder (FLUIMUCIL A 600, ZAMBON Switzerland, Ltd., Cadempino, Switzerland) 7 days | Blood Lactate VO2máx % FI TAC TNF-α. CK | ↓* Blood Lactate ↔ VO2máx ↑* % FI ↑* TAC ↔ TNF- α. ↔ CK |
| McKenna et al., 2006, Australia [31] | Randomized, double-blind crossover, placebo-controlled trial | 7 ♂ High endurance trained (running or cycling) 4–5 times per week 1–2 h per day experience ≥ 2 years Age (mean ± SD) 27.1 ± 5.6 years, Weight (mean ± SD) 76.7 ± 10.9 kg Height (mean ± SD) 180 ± 5.4 cm Study withdrawals: 0 | Intravenous infusion NAC 125 mg/kg/h for 15 min before test plus 25 mg/kg/h until the end of the test. Washout period: 7 days | Time to exhaustion VO2máx Hb Hct Na+/K+ pump activity Plasma K+ Plasma Electrolyte (Na+, Cl−, Ca2+) Acid–Base Status (HCO3−, PCO2, H+) | ↑* Time to exhaustion ↑* VO2máx ↔ Hb ↔ Hct ↓* Na+/K+ pump activity ↓* Plasma K+ ↔ Plasma Electrolyte ↔ Acid–Base Status |
| Medved et al., 2003, Australia [32] | Randomized, double-blind crossover, placebo-controlled trial counterbalanced | 8 ♂ Healthy Age (mean ± SD) 22.5 ± 2.4 years Body mass (mean ± SD) 77.81 ± 10.3 kg Height (mean ± SD) 177.6 ± 1.6 cm Study withdrawals: 0 | Intravenous infusion NAC 125 mg/kg/h for 15 min before test plus 25 mg/kg/h until the end of the test. Washout period: 5–7 days | Time to exhaustion Total work (kJ) GSH GSSG CySH, CySS TGSH GSH:TGSH ratio Hb Hct Plasma Electrolyte (Na+, Cl−, Ca2+) K+ Acid–Base Status (HCO3-, PCO2−) Adverse reactions | ↔ Time to exhaustion ↔ Total work (kJ) ↑* GSH ↓* GSSG ↑* CySH, ↑* CySS ↔ TGSH ↔ GSH:TGSH ratio ↔ Hb ↔ Hct ↔ Plasma Electrolyte (Na+, Cl−, Ca2+) ↑* K+ ↔ Acid–Base Status (HCO3−, PCO2−) ↑ Side Effects |
| Medved et al., 2004, Australia [33] | Randomized, double-blind crossover, placebo-controlled trial | 8 ♂ Endurance trained (running or cycling) 4–5 times per week 1–2 h per day experience ≥ 2 years Age (mean ± SD) 27.1 ± 5.6 years Body mass (mean ± SD) 76.7 ± 10.9 kg Height (mean ± SD) 180.3 ± 5.4 cm Study withdrawals: 0 | Intravenous infusion NAC 125 mg/kg/h for 15 min before test plus 25 mg/kg/h until the end of the test. Washout period: 5–7 days | Time to exhaustion Total work (kJ) GSH GSSG CySH, CySS TGSH GSH:TGSH ratio Adverse reactions | ↑* Time to exhaustion ↑* Total work (kJ) ↑* GSH ↔ GSSG ↑* TGSH ↑* CySH (muscle; plasma) ↑* CySS (muscle; plasma) ↔ GSSG:TGSH ratio ↔ TSGH:GSH ratio ↑ Side Effects |
| Merry et al. 2010, Australia [34] | Randomized, double-blind crossover, placebo-controlled trial counterbalanced | 9 ♂ Healthy physically active Age (mean ± SD) 23 ± 2 years Weight (mean ± SD) 79.7 ± 3.4 kg Height (mean ± SD) 179 ± 3 cm Study withdrawals: 0 | Intravenous infusion NAC (Parvolex, Faulding Pharmaceuticals) 125 mg/kg/h for 15 min before test plus 25 mg/kg/h until the end of the test. Washout period: 14 days | Blood Lactate O2 Consumption HR RER RPE GSH GSSG GSH:GSSG ratio CySH (muscle; plasma) CySS S-glutathionylation Tyrosine nitration PCr, Cr ATP, ADP, AMP AMP:ATP ratio muscle glycogen Insulin NEFA Adverse reactions | ↔ Blood Lactate ↔ O2 Uptake ↔ HR ↔ RER ↔ RPE ↔ GSH ↔ GSSG ↔ GSH:GSSG ratio ↑* CySH (muscle; plasma) ↑* CySS ↓* S-glutathionylation ↔ Tyrosine nitration ↔ PCr, Cr ↔ ATP, ADP, AMP ↔ AMP:ATP ratio ↔ muscle glycogen ↔ Insulin ↔ NEFA ↔ Side Effects |
| Nielsen et al., 1998, Denmark [35] | Randomized, double-blind crossover, placebo-controlled | 14 ♂ Healthy oarsmen trained Age (mean ± SE) 27 ± 1 years Weight (mean ± SE) 80 ± 2 kg Height (mean ± SE) 189 ± 2 cm VO2max (mean ± SE) 5.1 ± 0.2 L/min | 6000 mg/day 2 daily capsules NAC (ASTRA, Copenhagen, Denmark), 3000 mg Morning and evening meals for 3 days before the experiment, and 2 h before the exercise protocol Washout period: 21 days | Lymphocytes CD3+ CD4+ CD8+ CD14+ CD16+ CD19+ CD56+ NK activity | ↔ Lymphocytes ↔ CD3+ ↔ CD4+ ↔ CD8+ ↔ CD14+ ↔ CD16+ ↔ CD19+ ↔ CD56+ ↔ NK activity |
| Petersen et al., 2012, Australia [36] | Randomized, double-blind crossover, placebo-controlled | 8 ♂ Endurance trained (running or cycling) 4–5 times per week 1–2 h per day experience ≥ 2 years Age (mean ± SD) 27.1 ± 5.6 years Body mass (mean ± SD) 76.7 ± 10.9 kg Height (mean ± SD) 180.3 ± 5.4 cm VO2peak 65.6 ± 2.2 mL/kg Study withdrawals: 0 | Intravenous infusion NAC 125 mg/kg/h for 15 min before test plus 25 mg/kg/h until the end of the test. Washout period: 7 days | MnSOD JNK ERK1/2 p38 MAPK NF-kB/p65 IkBα IL-6 MCP-1 HSP70 PGC-1α | ↓* MnSOD ↓* JNK ↔ ERK1/2 ↔ p38 MAPK ↓*NF-kB/p65 ↔ IkBα ↔ IL-6 ↔ MCP-1 ↔ HSP70 ↔ PGC-1α |
| Rhodes et al, 2019, Australia [16] | Double-blind, pre-post, placebo-controlled | 17 ♂ Semi-professional/Semi-elite rugby players Age (mean ± SD) 20.4 ± 0.9 years Weight (mean ± SD) 103.0 ± 12.0 kg Height (mean ± SD) 182.3 ± 7.4 cm Yo-Yo Intermittent Recovery Test Level 1 (mean ± SD) 17.4 ± 1.73 Level Study withdrawals: 4 6 participants IG 7 participants CG | IG: 1 g/day (2 × 50 mg capsules) NAC (Nutrabio Labs Inc., Middlesex, NJ, USA) CG: 1 g (2 × 50 mg capsules) of placebo (sucrose and salt mixture) For 6 days. | Muscle soreness Broken bronco shuttle test Fastest shuttle time (High-intensity exercise) Side effects | ↑ Muscle Soreness ↔ Broken bronco shuttle test ↑ Fastest shuttle time ↔ Side Effects |
| Silva et al. 2008, Brazil [23] | Randomized, controlled, single-blind trial | 29 ♂ Healthy physically active Age (mean ± SD) 21.3 ± 4 years Weight (mean ± SD) 74.5 ± 7.7 kg Height (mean ± SD) 177.2 ± 6.9 cm Study withdrawals: 4 8 participants IG 9 participants CG 8 participants IG + CG | 1 capsule/day 10 mg/kg NAC 14 days before the eccentric exercise protocol and 7 days after exercise CG (21 days; placebo) IG (21 days; NAC) IG + CG (14 days NAC + 7 days placebo) | MDA Carbonylation levels TNF-α IL-10 Muscle pain | ↔ MDA ↔ Carbonylation levels ↑* TNF- α ↑*IL-10 ↓ Muscle Pain |
| Slattery et al., 2014, Australia [24] | Randomized, double-blind crossover, placebo-controlled | 10 ♂ Well-trained triathletes Age (mean ± SD) 23.6 ± 3.2 years Weight (mean ± SD) 70.5 ± 7.2 kg Height (mean ± SD) 179.8 ± 4.4 cm VO2max (mean ± SD) 663.3 ± 4.8 mL/kg/min Study withdrawals: 2 (injury and illness) | 1200 mg NAC (Batch: 254709, The Melbourne Food Ingredient Depot, Victoria, Melburne, Australia), 2 * 600 mg capsules 9 days and 2 h before the test Washout period: 21 days | Average Power 5, 10, 15 s Total work Blood lactate RPE TAC GSH GSSG GSH: GSSG ratio XO TRABS FRAP IL-6, MPC-1 NF-kB Adverse reactions | ↑* Average Power 5, 10, 15 s ↔ Total work ↔ Blood lactate ↔ RPE ↑* TAC ↔ GSH ↔ GSSG ↔ GSH: GSSG ratio ↔ XO ↓* TRABS ↔ FRAP ↓* IL-6 ↓* MPC-1 ↑* NF-kB ↔ Adverse reactions |
| Smith et al., 2016, USA [25] | Randomized, double-blind crossover, placebo-controlled | 10 ♂ Non-endurance trained Age (mean ± SD) 21.8 ± 1.2 years Weight (mean ± SD) 77.1 ± 17.5 kg Height (mean ± SD) 174.9 ± 9.3 cm Peak Power (mean ± SD) 6.0 ± 1.3 W Study withdrawals: 0 | 70 mg/kg NAC 600 mg/capsule 60 min before the test Washout period: 7 days | Time to Exhaustion GSH GSSG GSH: GSSG CySH CySS BABF DAB | ↔ Time to Exhaustion ↑* GSH ↑* GSSG ↓* GSH: GSSG ↑* CySH ↑* CySS ↔ BABF ↔ DAB |
| Zembron-Lancy et al., 2007, Poland [27] | Randomized placebo-controlled | 30 ♂ Healthy young trained (Canoeists and Rowers) Age (mean ± SD) CG 21.5 ± 1.4 years IG 21.9 ± 1.7 years Body Mass (mean ± SD) CG 87.2 ± 10.6 kg IG 87.1 ± 12.8 kg Height (mean ± SD) CG 181.7 ± 8.3 cm IG 180.7 ± 7.4 cm Body Fat (mean ± SD) CG 14.4 ± 4.6 % IG 14.5 ± 5.6 % Study withdrawals: 0 15 participants IG 15 participants CG | IG: 1800 mg/day NAC (Hexal AG, Holzkirchen, Germany) as powder dissolved in 50 mL water CG: 3 × 350 mg/day Saccharum Lactis as powder dissolved in 50 mL water | Protein Thiols SOD GPx CAT TBARS Pro-Antioxidant ratio | ↑* Protein Thiols ↔ SOD ↑* GPx ↔ GR ↔ CAT ↓* TBARS ↑* Pro-Antioxidant ratio |
| Zembron-Lancy et al., 2010, Poland [26] | 15 ♂ Healthy students Age (mean ± SD) 20.3 ± 2.3 years Body Mass (mean ± SD) 83.4 ± 14.4 kg Height (mean ± SD) 180.0 ± 1.0 cm Study withdrawals: 0 8 participants IG 7 participants CG | IG: 1200 mg/day NAC 2 daily doses (1st dose in the morning in a fasted state and the second dose 2 h before an evening meal) for 8 days prior to and 1 dose 600 mg on the day of exercise trial Each dose as powder dissolved in 50 mL of water CG: Lactose as powder dissolved in 50 mL of water | Time to exhaustion Peak Power GSH GPx GR PC TBARS EPO Hb Hct MVC MHC RCB | ↔ Time to exhaustion ↔ Peak Power ↑* GSH ↑* GPx ↑* GR ↓* PC ↓* TBARS ↑* EPO ↑* Hb ↑* Hct ↑* MVC ↑* MHC ↓* RCB |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Lázaro, D.; Domínguez-Ortega, C.; Busto, N.; Santamaría-Peláez, M.; Roche, E.; Gutiérez-Abejón, E.; Mielgo-Ayuso, J. Influence of N-Acetylcysteine Supplementation on Physical Performance and Laboratory Biomarkers in Adult Males: A Systematic Review of Controlled Trials. Nutrients 2023, 15, 2463. https://doi.org/10.3390/nu15112463
Fernández-Lázaro D, Domínguez-Ortega C, Busto N, Santamaría-Peláez M, Roche E, Gutiérez-Abejón E, Mielgo-Ayuso J. Influence of N-Acetylcysteine Supplementation on Physical Performance and Laboratory Biomarkers in Adult Males: A Systematic Review of Controlled Trials. Nutrients. 2023; 15(11):2463. https://doi.org/10.3390/nu15112463
Chicago/Turabian StyleFernández-Lázaro, Diego, Carlos Domínguez-Ortega, Natalia Busto, Mirian Santamaría-Peláez, Enrique Roche, Eduardo Gutiérez-Abejón, and Juan Mielgo-Ayuso. 2023. "Influence of N-Acetylcysteine Supplementation on Physical Performance and Laboratory Biomarkers in Adult Males: A Systematic Review of Controlled Trials" Nutrients 15, no. 11: 2463. https://doi.org/10.3390/nu15112463
APA StyleFernández-Lázaro, D., Domínguez-Ortega, C., Busto, N., Santamaría-Peláez, M., Roche, E., Gutiérez-Abejón, E., & Mielgo-Ayuso, J. (2023). Influence of N-Acetylcysteine Supplementation on Physical Performance and Laboratory Biomarkers in Adult Males: A Systematic Review of Controlled Trials. Nutrients, 15(11), 2463. https://doi.org/10.3390/nu15112463