

Use of Dietary Fibers in Reducing the Risk of Several Cancer Types: An Umbrella Review

Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Methodology Quality
2.5. Evidence Quality Assessment
2.6. Data Analysis
3. Results
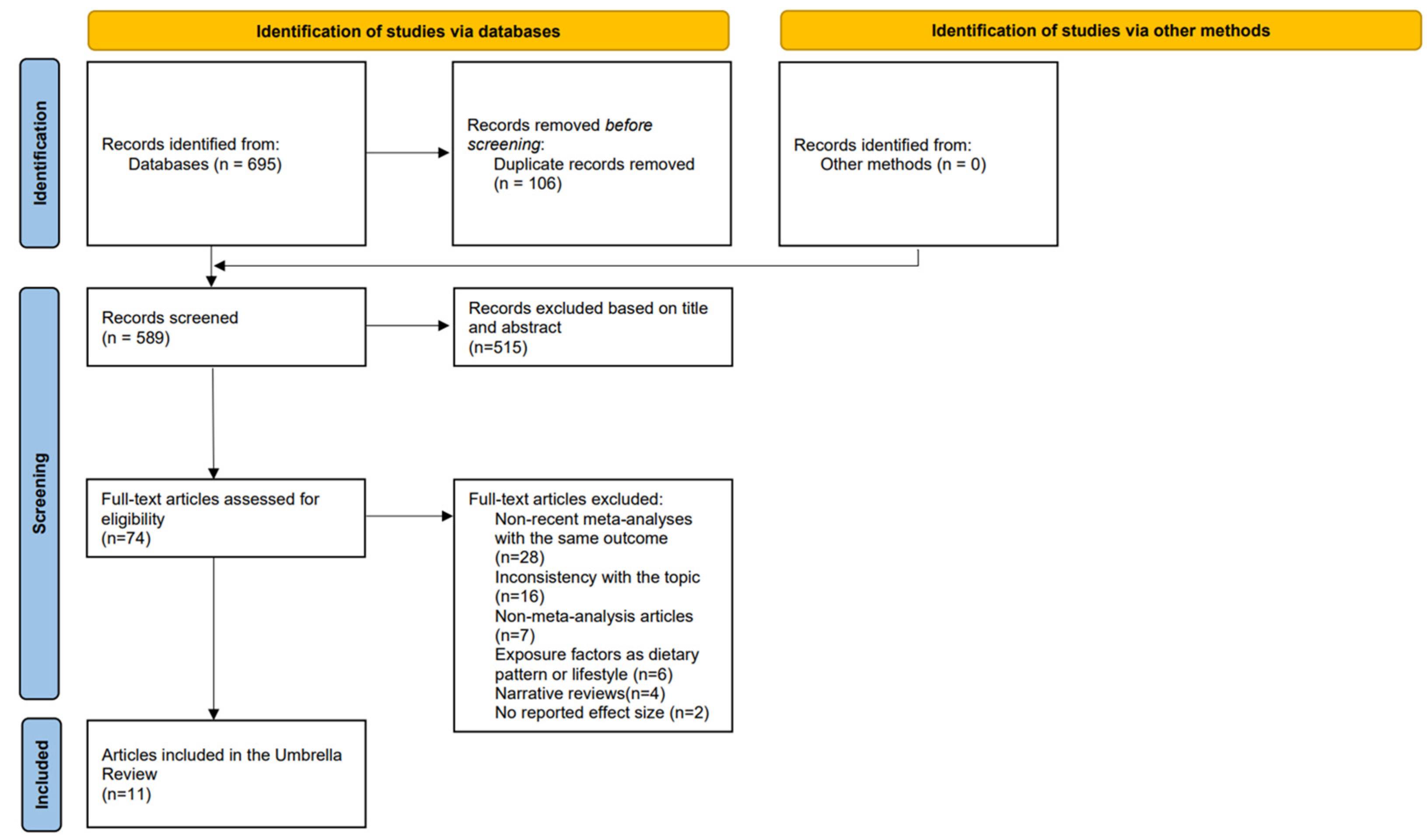
3.1. Research Screening
3.2. The Characteristics of the Included Study
3.3. Methodology Quality Assessment
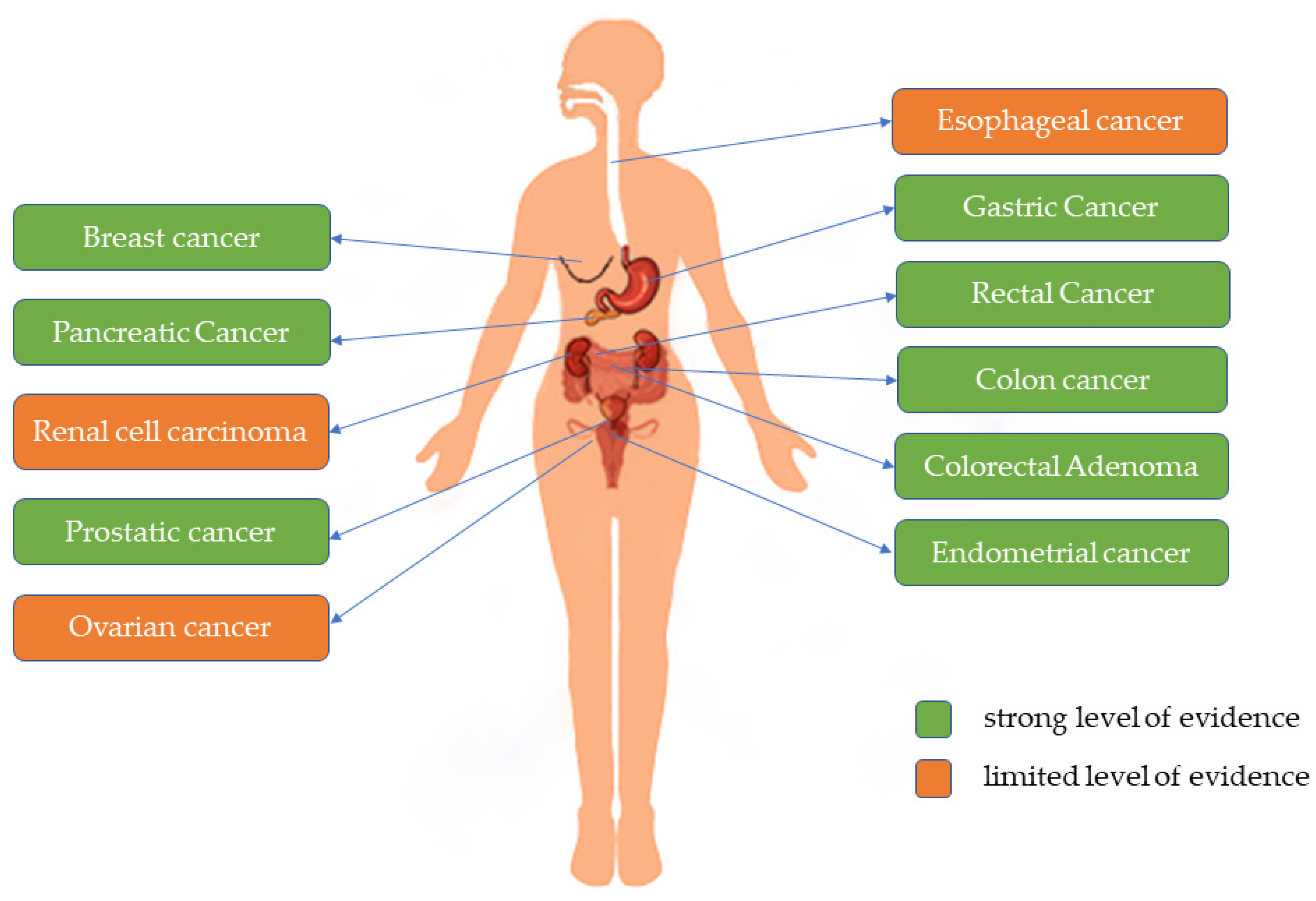
3.4. Evidence Quality Evaluation
3.5. Association Analysis of Dietary Fiber and Cancer
3.5.1. Esophageal and Gastric Cancer
3.5.2. Colon and Rectal Cancers and Colorectal Adenomas
3.5.3. Breast, Ovarian, and Endometrial Cancer
3.5.4. Other Cancers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Health Estimates: Leading Causes of Death. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed on 30 March 2023).
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. World Cancer Report: Cancer Research for Cancer Prevention; IARC: Lyon, France; ISBN 978-92-832-0447-3.
- Kerr, J.; Anderson, C.; Lippman, S.M. Physical Activity, Sedentary Behaviour, Diet, and Cancer: An Update and Emerging New Evidence. Lancet Oncol. 2017, 18, e457–e471. [Google Scholar] [CrossRef] [PubMed]
- Hijová, E.; Bertková, I.; Štofilová, J. Dietary Fibre as Prebiotics in Nutrition. Cent. Eur. J. Public Health 2019, 27, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Dongmei, Y.; Liyun, Z.; Wenhua, Z. Status and trends in consumption of grains and dietary fiber among Chinese adults (1982–2015). Nutr. Rev. 2020, 78, 43–53. (In Chinese) [Google Scholar] [CrossRef]
- Stephen, A.M.; Champ, M.M.-J.; Cloran, S.J.; Fleith, M.; van Lieshout, L.; Mejborn, H.; Burley, V.J. Dietary Fibre in Europe: Current State of Knowledge on Definitions, Sources, Recommendations, Intakes and Relationships to Health. Nutr. Res. Rev. 2017, 30, 149–190. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Holford, T.R.; Zhang, Y.; Boyle, P.; Mayne, S.T.; Dai, M.; Zheng, T. Dietary Fiber Intake and Risk of Breast Cancer by Menopausal and Estrogen Receptor Status. Eur. J. Nutr. 2013, 52, 217–223. [Google Scholar] [CrossRef]
- Tantamango, Y.M.; Knutsen, S.F.; Beeson, L.; Fraser, G.; Sabate, J. Association between Dietary Fiber and Incident Cases of Colon Polyps: The Adventist Health Study. Gastrointest. Cancer Res. 2011, 4, 161–167. [Google Scholar]
- Zaineddin, A.K.; Buck, K.; Vrieling, A.; Heinz, J.; Flesch-Janys, D.; Linseisen, J.; Chang-Claude, J. The Association Between Dietary Lignans, Phytoestrogen-Rich Foods, and Fiber Intake and Postmenopausal Breast Cancer Risk: A German Case-Control Study. Nutr. Cancer 2012, 64, 652–665. [Google Scholar] [CrossRef]
- Deschasaux, M.; Zelek, L.; Pouchieu, C.; His, M.; Hercberg, S.; Galan, P.; Latino-Martel, P.; Touvier, M. Prospective Association between Dietary Fiber Intake and Breast Cancer Risk. PLoS ONE 2013, 8, e79718. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Giovannucci, E.L.; Colditz, G.A.; Hunter, D.J.; Stampfer, M.J.; Rosner, B.; Speizer, F.E.; Willett, W.C. Dietary Fiber and the Risk of Colorectal Cancer and Adenoma in Women. N. Engl. J. Med. 1999, 340, 169–176. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective. Choice Rev. Online 2008, 45, 45-5024. [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing Systematic Reviews: Methodological Development, Conduct and Reporting of an Umbrella Review Approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef]
- Liu, W.; Zeng, Y.; Shao, Y.; Wang, K. Dietary fiber intake and risk of prostate cancer: A Meta-analysis. J. Int. Oncol. 2016, 43, 758. (In Chinese) [Google Scholar] [CrossRef]
- Farvid, M.S.; Spence, N.D.; Holmes, M.D.; Barnett, J.B. Fiber Consumption and Breast Cancer Incidence: A Systematic Review and Meta-Analysis of Prospective Studies. Cancer 2020, 126, 3061–3075. [Google Scholar] [CrossRef]
- Gianfredi, V.; Nucci, D.; Salvatori, T.; Dallagiacoma, G.; Fatigoni, C.; Moretti, M.; Realdon, S. Rectal Cancer: 20% Risk Reduction Thanks to Dietary Fibre Intake. Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1579. [Google Scholar] [CrossRef]
- Gianfredi, V.; Salvatori, T.; Villarini, M.; Moretti, M.; Nucci, D.; Realdon, S. Is Dietary Fibre Truly Protective against Colon Cancer? A Systematic Review and Meta-Analysis. Int. J. Food Sci. Nutr. 2018, 69, 904–915. [Google Scholar] [CrossRef]
- Huang, T.; Ding, P.; Chen, J.; Yan, Y.; Zhang, L.; Liu, H.; Liu, P.; Che, J.; Zheng, J.; Yao, X. Dietary Fiber Intake and Risk of Renal Cell Carcinoma: Evidence from a Meta-Analysis. Med. Oncol. 2014, 31, 125. [Google Scholar] [CrossRef]
- Li, H.; Mao, H.; Yu, Y.; Nan, Y. Association between Dietary Fiber and Endometrial Cancer: A Meta-Analysis. Nutr. Cancer 2020, 72, 959–967. [Google Scholar] [CrossRef]
- Nucci, D.; Santangelo, O.E.; Provenzano, S.; Fatigoni, C.; Nardi, M.; Ferrara, P.; Gianfredi, V. Dietary Fiber Intake and Risk of Pancreatic Cancer: Systematic Review and Meta-Analysis of Observational Studies. Int. J. Environ. Res. Public Health 2021, 18, 11556. [Google Scholar] [CrossRef]
- Nucci, D.; Fatigoni, C.; Salvatori, T.; Nardi, M.; Realdon, S.; Gianfredi, V. Association between Dietary Fibre Intake and Colorectal Adenoma: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4168. [Google Scholar] [CrossRef]
- Sun, L.; Zhang, Z.; Xu, J.; Xu, G.; Liu, X. Dietary Fiber Intake Reduces Risk for Barrett’s Esophagus and Esophageal Cancer. Crit. Rev. Food Sci. Nutr. 2017, 57, 2749–2757. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Ding, Y.; Xin, X.; Wang, W.; Zhang, D. Dietary Fiber Intake Is Associated with a Reduced Risk of Ovarian Cancer: A Dose-Response Meta-Analysis. Nutr. Res. 2018, 57, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xu, G.; Ma, M.; Yang, J.; Liu, X. Dietary Fiber Intake Reduces Risk for Gastric Cancer: A Meta-Analysis. Gastroenterology 2013, 145, 113–120.e3. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate Quality and Human Health: A Series of Systematic Reviews and Meta-Analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Dahl, W.J.; Stewart, M.L. Position of the Academy of Nutrition and Dietetics: Health Implications of Dietary Fiber. J. Acad. Nutr. Diet 2015, 115, 1861–1870. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- World Cancer Research Fund International. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective: A Summary of the Third Expert Report; World Cancer Research Fund International: London, UK, 2018; pp. 15–30. [Google Scholar]
- Wang, C.; Li, P.; Xuan, J.; Zhu, C.; Liu, J.; Shan, L.; Du, Q.; Ren, Y.; Ye, J. Cholesterol Enhances Colorectal Cancer Progression via ROS Elevation and MAPK Signaling Pathway Activation. Cell. Physiol. Biochem. 2017, 42, 729–742. [Google Scholar] [CrossRef]
- Farhana, L.; Nangia-Makker, P.; Arbit, E.; Shango, K.; Sarkar, S.; Mahmud, H.; Hadden, T.; Yu, Y.; Majumdar, A.P.N. Bile Acid: A Potential Inducer of Colon Cancer Stem Cells. Stem Cell Res. Ther. 2016, 7, 181. [Google Scholar] [CrossRef]
- Stadler, J.; Stern, H.S.; Yeung, K.S.; McGuire, V.; Furrer, R.; Marcon, N.; Bruce, W.R. Effect of High Fat Consumption on Cell Proliferation Activity of Colorectal Mucosa and on Soluble Faecal Bile Acids. Gut 1988, 29, 1326–1331. [Google Scholar] [CrossRef]
- Akin, H.; Tözün, N. Diet, Microbiota, and Colorectal Cancer. J. Clin. Gastroenterol. 2014, 48 (Suppl. S1), S67–S69. [Google Scholar] [CrossRef]
- Fung, K.Y.C.; Cosgrove, L.; Lockett, T.; Head, R.; Topping, D.L. A Review of the Potential Mechanisms for the Lowering of Colorectal Oncogenesis by Butyrate. Br. J. Nutr. 2012, 108, 820–831. [Google Scholar] [CrossRef] [PubMed]
- Bordonaro, M.; Lazarova, D.L.; Sartorelli, A.C. Butyrate and Wnt Signaling: A Possible Solution to the Puzzle of Dietary Fiber and Colon Cancer Risk? Cell Cycle 2008, 7, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Grosse, Y.; Baan, R.; Straif, K.; Secretan, B.; Ghissassi, F.E.; Cogliano, V. Carcinogenicity of Nitrate, Nitrite, and Cyanobacterial Peptide Toxins. Lancet Oncol. 2006, 7, 628–629. [Google Scholar] [CrossRef] [PubMed]
- Møller, M.E.; Dahl, R.; Bøckman, O.C. A Possible Role of the Dietary Fibre Product, Wheat Bran, as a Nitrite Scavenger. Food Chem. Toxicol. 1988, 26, 841–845. [Google Scholar] [CrossRef]
- Mayne, S.T.; Navarro, S.A. Diet, Obesity and Reflux in the Etiology of Adenocarcinomas of the Esophagus and Gastric Cardia in Humans. J. Nutr. 2002, 132, 3467S–3470S. [Google Scholar] [CrossRef]
- Mulholland, H.G.; Cantwell, M.M.; Anderson, L.A.; Johnston, B.T.; Watson, R.G.P.; Murphy, S.J.; Ferguson, H.R.; McGuigan, J.; Reynolds, J.V.; Comber, H.; et al. Glycemic Index, Carbohydrate and Fiber Intakes and Risk of Reflux Esophagitis, Barrett’s Esophagus, and Esophageal Adenocarcinoma. Cancer Causes Control 2009, 20, 279–288. [Google Scholar] [CrossRef]
- McFadden, D.; Riggs, D.; Jackson, B.; Cunningham, C. Corn-Derived Carbohydrate Inositol Hexaphosphate Inhibits Barrett’s Adenocarcinoma Growth by pro-Apoptotic Mechanisms. Oncol. Rep. 2008, 19, 563–566. [Google Scholar] [CrossRef]
- Clemons, M.; Goss, P. Estrogen and the Risk of Breast Cancer. N. Engl. J. Med. 2001, 344, 276–285. [Google Scholar] [CrossRef]
- Persson, I. Estrogens in the Causation of Breast, Endometrial and Ovarian Cancers—Evidence and Hypotheses from Epidemiological Findings. J. Steroid Biochem. Mol. Biol. 2000, 74, 357–364. [Google Scholar] [CrossRef]
- Key, T.; Appleby, P.; Barnes, I.; Reeves, G. Endogenous Hormones and Breast Cancer Collaborative Group Endogenous Sex Hormones and Breast Cancer in Postmenopausal Women: Reanalysis of Nine Prospective Studies. J. Natl. Cancer Inst. 2002, 94, 606–616. [Google Scholar] [CrossRef]
- Cohen, L.A.; Zhao, Z.; Zang, E.A.; Wynn, T.T.; Simi, B.; Rivenson, A. Wheat Bran and Psyllium Diets: Effects on N-Methylnitrosourea-Induced Mammary Tumorigenesis in F344 Rats. J. Natl. Cancer Inst. 1996, 88, 899–907. [Google Scholar] [CrossRef]
- Maskarinec, G.; Morimoto, Y.; Takata, Y.; Murphy, S.P.; Stanczyk, F.Z. Alcohol and Dietary Fibre Intakes Affect Circulating Sex Hormones among Premenopausal Women. Public Health Nutr. 2006, 9, 875–881. [Google Scholar] [CrossRef]
- Slavin, J.L. Mechanisms for the Impact of Whole Grain Foods on Cancer Risk. J. Am. Coll. Nutr. 2000, 19, 300S–307S. [Google Scholar] [CrossRef]
- Streppel, M.T.; Arends, L.R.; van ’t Veer, P.; Grobbee, D.E.; Geleijnse, J.M. Dietary Fiber and Blood Pressure: A Meta-Analysis of Randomized Placebo-Controlled Trials. Arch. Intern. Med. 2005, 165, 150–156. [Google Scholar] [CrossRef]
- Salmerón, J.; Manson, J.E.; Stampfer, M.J.; Colditz, G.A.; Wing, A.L.; Willett, W.C. Dietary Fiber, Glycemic Load, and Risk of Non-Insulin-Dependent Diabetes Mellitus in Women. JAMA 1997, 277, 472–477. [Google Scholar] [CrossRef]
- Meyer, K.A.; Kushi, L.H.; Jacobs, D.R.; Slavin, J.; Sellers, T.A.; Folsom, A.R. Carbohydrates, Dietary Fiber, and Incident Type 2 Diabetes in Older Women. Am. J. Clin. Nutr. 2000, 71, 921–930. [Google Scholar] [CrossRef]
- Aune, D.; Chan, D.S.M.; Greenwood, D.C.; Vieira, A.R.; Rosenblatt, D.A.N.; Vieira, R.; Norat, T. Dietary Fiber and Breast Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies. Ann. Oncol. 2012, 23, 1394–1402. [Google Scholar] [CrossRef]
- Pillow, P.C.; Duphorne, C.M.; Chang, S.; Contois, J.H.; Strom, S.S.; Spitz, M.R.; Hursting, S.D. Development of a Database for Assessing Dietary Phytoestrogen Intake. Nutr. Cancer 1999, 33, 3–19. [Google Scholar] [CrossRef]
- Cunat, S.; Hoffmann, P.; Pujol, P. Estrogens and Epithelial Ovarian Cancer. Gynecol. Oncol. 2004, 94, 25–32. [Google Scholar] [CrossRef]
- Franceschi, S.; Maso, L.D.; Augustin, L.; Negri, E.; Parpinel, M.; Boyle, P.; Jenkins, D.J.A.; LaVecchia, C. Dietary Glycemic Load and Colorectal Cancer Risk. Ann. Oncol. 2001, 12, 173–178. [Google Scholar] [CrossRef]
- Yu, H.; Rohan, T. Role of the Insulin-like Growth Factor Family in Cancer Development and Progression. J. Natl. Cancer Inst. 2000, 92, 1472–1489. [Google Scholar] [CrossRef] [PubMed]
- Hsing, A.W.; Gao, Y.-T.; Chua, S.; Deng, J.; Stanczyk, F.Z. Insulin Resistance and Prostate Cancer Risk. J. Natl. Cancer Inst. 2003, 95, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.A. Whole Grains, Legumes, and the Subsequent Meal Effect: Implications for Blood Glucose Control and the Role of Fermentation. J. Nutr. Metab. 2012, 2012, 829238. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.D.; Bickerton, A.S.; Dennis, A.L.; Vidal, H.; Frayn, K.N. Insulin-Sensitizing Effects of Dietary Resistant Starch and Effects on Skeletal Muscle and Adipose Tissue Metabolism. Am. J. Clin. Nutr. 2005, 82, 559–567. [Google Scholar] [CrossRef]
- Johnston, K.L.; Thomas, E.L.; Bell, J.D.; Frost, G.S.; Robertson, M.D. Resistant Starch Improves Insulin Sensitivity in Metabolic Syndrome. Diabet. Med. 2010, 27, 391–397. [Google Scholar] [CrossRef]
- Wolpin, B.M.; Bao, Y.; Qian, Z.R.; Wu, C.; Kraft, P.; Ogino, S.; Stampfer, M.J.; Sato, K.; Ma, J.; Buring, J.E.; et al. Hyperglycemia, Insulin Resistance, Impaired Pancreatic β-Cell Function, and Risk of Pancreatic Cancer. J. Natl. Cancer Inst. 2013, 105, 1027–1035. [Google Scholar] [CrossRef]
- Ma, Y.; Griffith, J.A.; Chasan-Taber, L.; Olendzki, B.C.; Jackson, E.; Stanek, E.J.; Li, W.; Pagoto, S.L.; Hafner, A.R.; Ockene, I.S. Association between Dietary Fiber and Serum C-Reactive Protein. Am. J. Clin. Nutr. 2006, 83, 760–766. [Google Scholar] [CrossRef]
- Dítě, P.; Hermanová, M.; Trna, J.; Novotný, I.; Růžička, M.; Liberda, M.; Bártková, A. The Role of Chronic Inflammation: Chronic Pancreatitis as a Risk Factor of Pancreatic Cancer. Dig. Dis. 2012, 30, 277–283. [Google Scholar] [CrossRef]
- Bansal, P.; Sonnenberg, A. Pancreatitis Is a Risk Factor for Pancreatic Cancer. Gastroenterology 1995, 109, 247–251. [Google Scholar] [CrossRef]
- King, D.E.; Egan, B.M.; Woolson, R.F.; Mainous, A.G.; Al-Solaiman, Y.; Jesri, A. Effect of a High-Fiber Diet vs a Fiber-Supplemented Diet on C-Reactive Protein Level. Arch. Intern. Med. 2007, 167, 502–506. [Google Scholar] [CrossRef]
- Vinolo, M.A.R.; Rodrigues, H.G.; Nachbar, R.T.; Curi, R. Regulation of Inflammation by Short Chain Fatty Acids. Nutrients 2011, 3, 858–876. [Google Scholar] [CrossRef]
- Wang, F.; Xu, Y. Body Mass Index and Risk of Renal Cell Cancer: A Dose-Response Meta-Analysis of Published Cohort Studies. Int. J. Cancer 2014, 135, 1673–1686. [Google Scholar] [CrossRef]
- Slavin, J. Fiber and Prebiotics: Mechanisms and Health Benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef]
- Daniel, C.R.; Park, Y.; Chow, W.-H.; Graubard, B.I.; Hollenbeck, A.R.; Sinha, R. Intake of Fiber and Fiber-Rich Plant Foods Is Associated with a Lower Risk of Renal Cell Carcinoma in a Large US Cohort. Am. J. Clin. Nutr. 2013, 97, 1036–1043. [Google Scholar] [CrossRef]
- Bao, C.; Yang, X.; Xu, W.; Luo, H.; Xu, Z.; Su, C.; Qi, X. Diabetes Mellitus and Incidence and Mortality of Kidney Cancer: A Meta-Analysis. J. Diabetes Complicat. 2013, 27, 357–364. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Step | Search Strategy |
|---|---|
| #1 | (“Dietary Fiber” [Mesh] OR Dietary Fibers [Title/Abstract] OR Wheat Bran [Title/Abstract] OR Wheat Brans [Title/Abstract] OR Roughage [Title/Abstract] OR Roughages [Title/Abstract] OR Soluble dietary fiber [Title/Abstract] OR Insoluble dietary fiber [Title/Abstract] OR Fiber [Title/Abstract] OR Hemicellulose [Title/Abstract] OR Lignin [Title/Abstract] OR Pectin [Title/Abstract]) AND (“Neoplasms” [Mesh] OR Tumor [Title/Abstract] OR Neoplasm [Title/Abstract] OR Tumors [Title/Abstract] OR Neoplasia [Title/Abstract] OR Neoplasias [Title/Abstract] OR Cancer [Title/Abstract] OR Cancers [Title/Abstract] OR Malignant Neoplasm [Title/Abstract] OR Malignancy [Title/Abstract] OR Malignancies [Title/Abstract] OR Malignant Neoplasms [Title/Abstract]) |
| #2 | “Meta-Analysis as Topic” [Mesh] OR “Meta-Analysis” [Publication Type] OR “Systematic Review” [Publication Type] OR meta-analysis [Title/Abstract] OR data pooling [Title/Abstract] OR data poolings [Title/Abstract] OR clinical trial overview [Title/Abstract] OR clinical trial overviews [Title/Abstract] |
| #3 | #1 AND #2 |
| Cancer | Number of Studies | Number and Type of Study Included | Number of Cases/Sample Size | Assessed with | Main Result | Heterogeneity | Dose–Response | Publication Bias | Methodology Assessment Tools |
|---|---|---|---|---|---|---|---|---|---|
| Prostatic cancer | 10 | 5C, 5CC | 12,058/254,213 | TDF, IDF, SDF, FDF, VDF, CDF | RR (TDF): 0.87 (0.77–0.99); RR (IDF): 0.65 (0.45–0.88); RR (SDF): 0.78 (0.64–0.95); RR (FDF): 0.98 (0.85–1.12); RR (VDF): 0.91 (0.70–1.18); RR (CDF): 1.03 (0.95–1.12) | TDF: I2 = 56.6%; IDF: I2 = 56.0%; SDF: I2 = 0.0%; FDF: I2 = 31.4%; VDF: I2 = 75.0%; GDF: I2 = 0.0% | Per 1 g/day increment in total dietary fiber RR: 0.996 (0.989–1.002) | p = 0.064 | NOS |
| Breast cancer | 20 | 2CC, 17C, 1CT | 69,735/2,092,037 | TDF, IDF, SDF, FDF, VDF, CDF, LDF | RR (TDF): 0.92 (0.88–0.95); RR (IDF): 0.93 (0.86–1.00); RR (SDF): 0.90 (0.84–0.96); RR (FDF): 0.93 (0.89–0.96); RR (VDF): 0.95 (0.90–1.00); RR (CDF): 0.97 (0.93–1.01); RR (LDF): 0.97 (0.92–1.03) | TDF: I2 = 12.6%; IDF: I2 = 33.4%; SDF: I2 = 12.6%; FDF: I2 = 9.0%; VDF: I2 = 39.6%; CDF: I2 = 29.6%; LDF: I2 = 0.0% | p > 0.05 | NR | |
| Rectal cancer | 22 | 9CC, 13C | >1000/2,876,136 | TDF | RR: 0.77 (0.66–0.89) | I2 = 9.1% | p = 0.816 | ROB | |
| Colon cancer | 21 | 8CC, 13C | >1000/2,627,391 | TDF | RR: 0.74 (0.67–0.82) | I2 = 43.8% | p = 0.177 | ROB | |
| Renal cell carcinoma | 7 | 4CC, 3C | 6115/941,202 | TDF, IDF, SDF, FDF, VDF, CDF, LDF | RR (TDF): 0.84 (0.74–0.96); RR (FDF): 0.92 (0.80–1.05); RR (VDF): 0.70 (0.49–1.00); RR (CDF): 1.04 (0.91–1.18); RR (LDF): 0.80 (0.69–0.93) | TDF: I2 = 23.8%; FDF: I2 = 0.0%; VDF: I2 = 76.9%; GDF: I2 = 0.0%; LDF: NA | Per 10 g/day increment in total dietary fiber RR: 0.94 (0.80–1.11) | Egger’s test and Begg’s test (p= 0.728, p= 0.707, respectively) | NOS |
| Endometrial cancer | 16 | 13CC, 3C | 6563/198,174 | TDF | RR: 0.86 (0.78–0.93) | I2 = 69.1% | p > 0.05 | NOS | |
| Pancreatic cancer | 18 | 15CC, 3C | >1000/343,120 | TDF | RR: 0.63 (0.53–0.76) | I2 = 68.2% | p = 0.006 | NR | |
| Colorectal adenoma | 21 | 12CC, 8C, 1CT | >1000/157,725 | TDF | RR: 0.71 (0.68–0.75) | I2 = 62.7% | p = 0.838 | NR | |
| Esophageal cancer | 15 | 15CC | 3625/16,885 | TDF | RR: 0.52 (0.43–0.64) | I2 = 71.6% | Per 10 g/day increment in total dietary fiber RR: 0.69 (0.61–0.79) | p > 0.05 | NOS |
| Ovarian cancer | 19 | 14CC, 5C | 8200/567,742 | TDF | RR: 0.70 (0.57–0.87) | I2 = 83.5% | p = 0.276 | NR | |
| Gastric cancer | 21 | 19CC, 2C | 6950/580,064 | TDF | RR: 0.58 (0.49–0.67) | I2 = 62.2% | Per 10 g/day increment in total dietary fiber RR: 0.56 (0.45–0.71) | p = 0.931 | NOS |
| Level of Evidence a | Criteria b | Cancer |
|---|---|---|
| Convincing | Meta-analyses of prospective cohort studies with evidence of dose–response relation, no heterogeneity, no potential confounding factors identified, and eventual disagreement of results over time reasonably explained. | Gastric cancer |
| Probable | Meta-analyses should include at least six case–control or three prospective cohort studies, with a sample size greater than 1000 cases, no high or unexplained heterogeneity (I2 < 75%), no identified potential confounders, and the final difference in results over time was reasonably explained. | Endometrial cancer Rectal cancer Colon cancer Breast cancer Prostatic cancer Pancreatic cancer Colorectal adenoma |
| Suggestive | Meta-analyses of prospective cohort studies with a lack of information on significant heterogeneity (I2 < 75%) and identification of potential confounding factors (such as different findings in subgroups). | Ovarian cancer Renal cell carcinoma |
| Inconclusive | Meta-analyses of case–control studies, limited prospective cohort studies included in meta-analyses (n < 3), or evident contrasting results from meta-analyses with the same level of evidence. | Esophageal cancer |
| Improbable evidence | Meta-analyses of prospective cohort studies with no significant statistical association, non-significant dose–response association, a large number of studies or cases, no high and unexplained heterogeneity (I2 < 75%), the robustness of results in sensitivity analyses, and no plausible mechanisms. | None |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, J.; Wang, J.; Li, Y.; Xue, K.; Kan, J. Use of Dietary Fibers in Reducing the Risk of Several Cancer Types: An Umbrella Review. Nutrients 2023, 15, 2545. https://doi.org/10.3390/nu15112545
Hu J, Wang J, Li Y, Xue K, Kan J. Use of Dietary Fibers in Reducing the Risk of Several Cancer Types: An Umbrella Review. Nutrients. 2023; 15(11):2545. https://doi.org/10.3390/nu15112545
Chicago/Turabian StyleHu, Jun, Junjing Wang, Yuxing Li, Kun Xue, and Juntao Kan. 2023. "Use of Dietary Fibers in Reducing the Risk of Several Cancer Types: An Umbrella Review" Nutrients 15, no. 11: 2545. https://doi.org/10.3390/nu15112545
APA StyleHu, J., Wang, J., Li, Y., Xue, K., & Kan, J. (2023). Use of Dietary Fibers in Reducing the Risk of Several Cancer Types: An Umbrella Review. Nutrients, 15(11), 2545. https://doi.org/10.3390/nu15112545