

Therapeutic Fasting in Reducing Chemotherapy Side Effects in Cancer Patients: A Systematic Review and Meta-Analysis

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
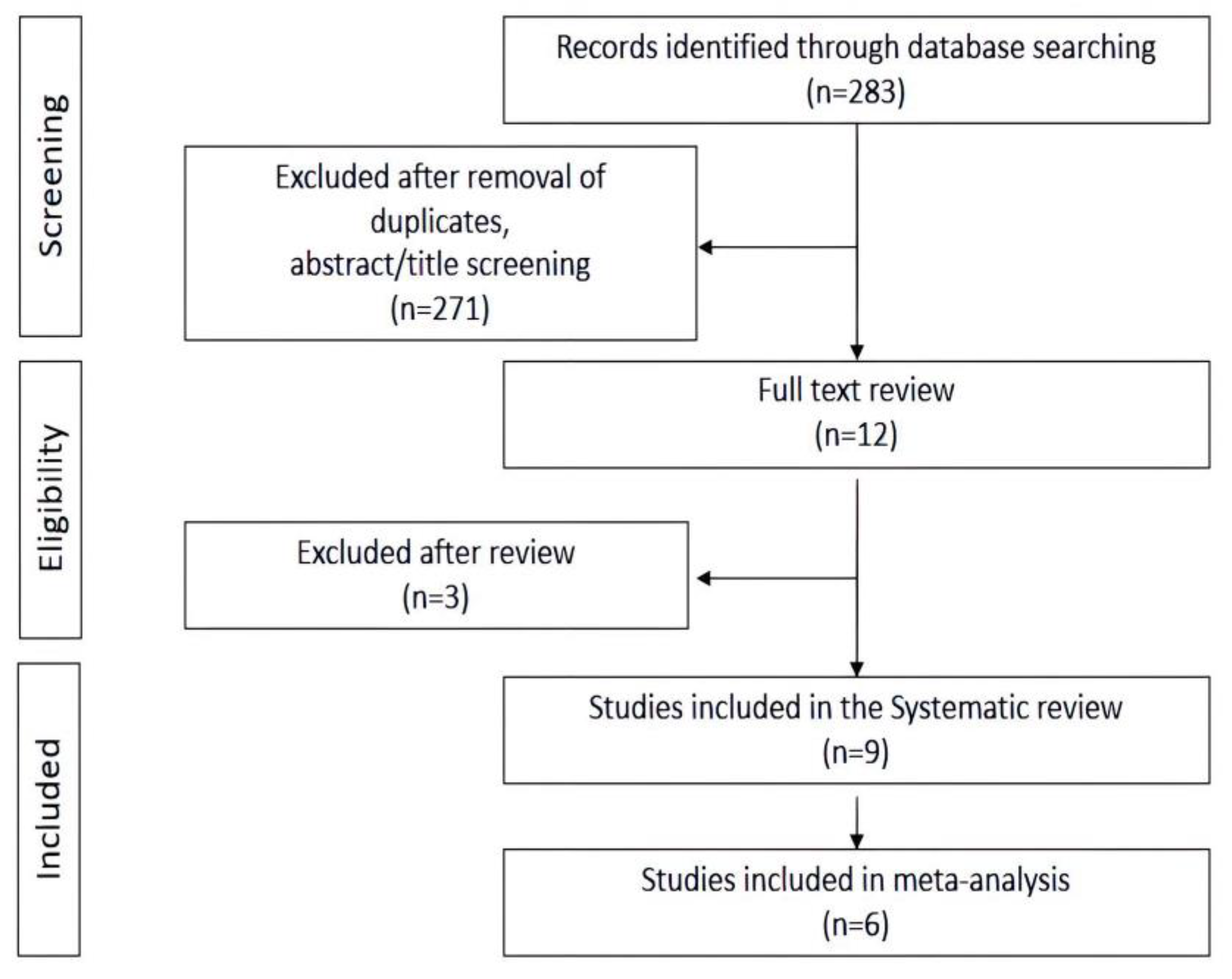
2.1. Study Selection Process
2.2. Data Extraction and Quality Assessment
2.3. Definition of Outcomes
2.4. Data Synthesis and Analysis
3. Results
3.1. Search Results
3.2. Risk of Bias
3.3. Study Characteristics
3.4. Fasting Regimes and the Risk of Chemotherapy-Side Effects
3.5. Sensitivity Analysis
4. Discussion
4.1. Limitations of the Study
4.2. Implications for Clinical Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pearce, A.; Haas, M.; Viney, R.; Pearson, S.; Haywood, P.; Brown, C.; Ward, R. Incidence and Severity of Self-Reported Chemotherapy Side Effects in Routine Care: A Prospective Cohort Study. PLoS ONE 2017, 12, e0184360. [Google Scholar] [CrossRef] [PubMed]
- Mustian, K.M.; Darling, T.V.; Janelsins, M.C.; Jean-Pierre, P.; Roscoe, J.A.; Morrow, G.R. Chemotherapy-Induced Nausea and Vomiting. US Oncol. 2008, 4, 19–23. [Google Scholar] [CrossRef]
- Tageja, N.; Groninger, H. Chemotherapy-Induced Nausea and Vomiting: An Overview and Comparison of Three Consensus Guidelines. Postgrad. Med. J. 2016, 92, 34–40. [Google Scholar] [CrossRef]
- Hwang, S.S.; Chang, V.T.; Cogswell, J.; Kasimis, B.S. Clinical Relevance of Fatigue Levels in Cancer Patients at a Veterans Administration Medical Center. Cancer 2002, 94, 2481–2489. [Google Scholar] [CrossRef] [PubMed]
- Silber, J.H.; Fridman, M.; DiPaola, R.S.; Erder, M.H.; Pauly, M.V.; Fox, K.R. First-Cycle Blood Counts and Subsequent Neutropenia, Dose Reduction, or Delay in Early-Stage Breast Cancer Therapy. J. Clin. Oncol. 1998, 16, 2392–2400. [Google Scholar] [CrossRef]
- Hesketh, P.J. Chemotherapy-Induced Nausea and Vomiting. N. Engl. J. Med. 2008, 358, 2482–2494. [Google Scholar] [CrossRef]
- Patel, P.; Robinson, P.D.; Wahib, N.; Cheung, P.; Wong, T.; Cabral, S.; Parker, A.; Cohen, M.; Devine, K.; Gibson, P.; et al. Interventions for the Prevention of Acute Phase Chemotherapy-Induced Nausea and Vomiting in Adult and Pediatric Patients: A Systematic Review and Meta-Analysis. Support. Care Cancer 2022, 30, 8855–8869. [Google Scholar] [CrossRef]
- Russo, S.; Cinausero, M.; Gerratana, L.; Bozza, C.; Iacono, D.; Driol, P.; Deroma, L.; Sottile, R.; Fasola, G.; Puglisi, F. Factors Affecting Patient’s Perception of Anticancer Treatments Side-Effects: An Observational Study. Expert Opin. Drug Saf. 2014, 13, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Caccialanza, R.; Cereda, E.; De Lorenzo, F.; Farina, G.; Pedrazzoli, P.; AIOM-SINPE-FAVO Working Group. To Fast, or Not to Fast before Chemotherapy, that is the Question. BMC Cancer 2018, 18, 337–345. [Google Scholar] [CrossRef]
- Tannenbaum, A. The Dependence of Tumor Formation on the Composition of the Calorie-Restricted Diet as Well as on the Degree of Restriction. 1945. Nutrition 1996, 12, 653–654. [Google Scholar] [CrossRef]
- Berrigan, D.; Perkins, S.N.; Haines, D.C.; Hursting, S.D. Adult-Onset Calorie Restriction and Fasting Delay Spontaneous Tumorigenesis in p53-Deficient Mice. Carcinogenesis 2002, 23, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Safdie, F.; Brandhorst, S.; Wei, M.; Wang, W.; Lee, C.; Hwang, S.; Conti, P.S.; Chen, T.C.; Longo, V.D. Fasting Enhances the Response of Glioma to Chemo- and Radiotherapy. PLoS ONE 2012, 7, e44603. [Google Scholar] [CrossRef] [PubMed]
- Di Biase, S.; Shim, H.S.; Kim, K.H.; Vinciguerra, M.; Rappa, F.; Wei, M.; Brandhorst, S.; Cappello, F.; Mirzaei, H.; Lee, C.; et al. Fasting Regulates EGR1 and Protects from Glucose- and Dexamethasone-Dependent Sensitization to Chemotherapy. PLoS Biol. 2017, 15, e2001951. [Google Scholar] [CrossRef] [PubMed]
- Brandhorst, S.; Wei, M.; Hwang, S.; Morgan, T.E.; Longo, V.D. Short-Term Calorie and Protein Restriction Provide Partial Protection from Chemotoxicity but do Not Delay Glioma Progression. Exp. Gerontol. 2013, 48, 1120–1128. [Google Scholar] [CrossRef]
- Cheng, C.; Adams, G.B.; Perin, L.; Wei, M.; Zhou, X.; Lam, B.S.; Da Sacco, S.; Mirisola, M.; Quinn, D.I.; Dorff, T.B.; et al. Prolonged Fasting Reduces IGF-1/PKA to Promote Hematopoietic-Stem-Cell-Based Regeneration and Reverse Immunosuppression. Cell Stem Cell 2014, 14, 810–823. [Google Scholar] [CrossRef] [PubMed]
- de Groot, S.; Vreeswijk, M.P.G.; Welters, M.J.P.; Gravesteijn, G.; Boei, J.J.W.A.; Jochems, A.; Houtsma, D.; Putter, H.; Van Der Hoeven, J.J.M.; Nortier, J.W.R.; et al. The Effects of Short-Term Fasting on Tolerance to (Neo) Adjuvant Chemotherapy in HER2-Negative Breast Cancer Patients: A Randomized Pilot Study. BMC Cancer 2015, 15, 652–655. [Google Scholar] [CrossRef]
- Dorff, T.B.; Groshen, S.; Garcia, A.; Shah, M.; Tsao-Wei, D.; Pham, H.; Cheng, C.; Brandhorst, S.; Cohen, P.; Wei, M.; et al. Safety and Feasibility of Fasting in Combination with Platinum-Based Chemotherapy. BMC Cancer 2016, 16, 360–366. [Google Scholar] [CrossRef]
- Bauersfeld, S.P.; Kessler, C.S.; Wischnewsky, M.; Jaensch, A.; Steckhan, N.; Stange, R.; Kunz, B.; Brückner, B.; Sehouli, J.; Michalsen, A. The Effects of Short-Term Fasting on Quality of Life and Tolerance to Chemotherapy in Patients with Breast and Ovarian Cancer: A Randomized Cross-Over Pilot Study. BMC Cancer 2018, 18, 476–482. [Google Scholar] [CrossRef]
- Safdie, F.M.; Dorff, T.; Quinn, D.; Fontana, L.; Wei, M.; Lee, C.; Cohen, P.; Longo, V.D. Fasting and Cancer Treatment in Humans: A Case Series Report. Aging 2009, 1, 988–1007. [Google Scholar] [CrossRef]
- Brandhorst, S.; Choi, I.Y.; Wei, M.; Cheng, C.W.; Sedrakyan, S.; Navarrete, G.; Dubeau, L.; Yap, L.P.; Park, R.; Vinciguerra, M.; et al. A Periodic Diet that Mimics Fasting Promotes Multi-System Regeneration, Enhanced Cognitive Performance, and Healthspan. Cell Metab. 2015, 22, 86–99. [Google Scholar] [CrossRef]
- Moyer, C.L.; Morita, R.Y. Effect of Growth Rate and Starvation-Survival on Cellular DNA, RNA, and Protein of a Psychrophilic Marine Bacterium. Appl. Environ. Microbiol. 1989, 55, 2710–2716. [Google Scholar] [CrossRef]
- Raffaghello, L.; Lee, C.; Safdie, F.M.; Wei, M.; Madia, F.; Bianchi, G.; Longo, V.D. Starvation-Dependent Differential Stress Resistance Protects Normal but Not Cancer Cells against High-Dose Chemotherapy. Proc. Natl. Acad. Sci. USA 2008, 105, 8215–8220. [Google Scholar] [CrossRef]
- Fan, Q.; Yang, L.; Zhang, X.; Ma, Y.; Li, Y.; Dong, L.; Zong, Z.; Hua, X.; Su, D.; Li, H.; et al. Autophagy Promotes Metastasis and Glycolysis by Upregulating MCT1 Expression and Wnt/Beta-Catenin Signaling Pathway Activation in Hepatocellular Carcinoma Cells. J. Exp. Clin. Cancer Res. 2018, 37, 9. [Google Scholar] [CrossRef] [PubMed]
- Poillet-Perez, L.; White, E. Role of Tumor and Host Autophagy in Cancer Metabolism. Genes Dev. 2019, 33, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Vera-Ramirez, L.; Vodnala, S.K.; Nini, R.; Hunter, K.W.; Green, J.E. Autophagy Promotes the Survival of Dormant Breast Cancer Cells and Metastatic Tumour Recurrence. Nat. Commun. 2018, 9, 1944–1946. [Google Scholar] [CrossRef]
- Bow, E.J. Infection risk and cancer chemotherapy: The impact of the chemotherapeutic regimen in patients with lymphoma and solid tissue malignancies. J. Antimicrob. Chemother. 1998, 41 (Suppl. S4), 1–5. [Google Scholar] [CrossRef]
- Murray, M.J.; Murray, A.B. Anorexia of infection as a mechanism of host defense. Am. J. Clin. Nutr. 1979, 32, 593–596. [Google Scholar] [CrossRef]
- Longo, V.D.; Mattson, M.P. Fasting: Molecular mechanisms and clinical applications. Cell Metab. 2014, 19, 181–192. [Google Scholar] [CrossRef]
- Lee, C.; Safdie, F.M.; Raffaghello, L.; Wei, M.; Madia, F.; Parrella, E.; Hwang, D.; Cohen, P.; Bianchi, G.; Longo, V.D. Reduced levels of IGF-I mediate differential protection of normal and cancer cells in response to fasting and improve chemotherapeutic index. Cancer Res. 2010, 70, 1564–1572. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, E.P. Gastrointestinal toxicity of chemotherapeutic agents. Semin Oncol. 2006, 33, 106–120. [Google Scholar] [CrossRef]
- Rangan, P.; Choi, I.; Wei, M.; Navarrete, G.; Guen, E.; Brandhorst, S.; Enyati, N.; Pasia, G.; Maesincee, D.; Ocon, V.; et al. Fasting-Mimicking Diet Modulates Microbiota and Promotes Intestinal Regeneration to Reduce Inflammatory Bowel Disease Pathology. Cell Rep. 2019, 26, 2704–2719.e6. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Long, H.A.; French, D.P.; Brooks, J.M. Optimising the Value of the Critical Appraisal Skills Programme (CASP) Tool for Quality Appraisal in Qualitative Evidence Synthesis. Res. Methods Med. Health Sci. 2020, 1, 31–42. [Google Scholar] [CrossRef]
- Amitai, I.; Gafter-Gvili, A.; Shargian-Alon, L.; Raanani, P.; Gurion, R. Obinutuzumab-Related Adverse Events: A Systematic Review and Meta-Analysis. Hematol. Oncol. 2021, 39, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Riedinger, C.J.; Kimball, K.J.; Kilgore, L.C.; Bell, C.W.; Heidel, R.E.; Boone, J.D. Water Only Fasting and its Effect on Chemotherapy Administration in Gynecologic Malignancies. Gynecol. Oncol. 2020, 159, 799–803. [Google Scholar] [CrossRef]
- de Groot, S.; Lugtenberg, R.T.; Cohen, D.; Welters, M.J.; Ehsan, I.; Vreeswijk, M.P.; Smit, V.T.; de Graaf, H.; Heijns, J.B.; Portielje, J.E.; et al. Fasting Mimicking Diet as an Adjunct To neoadjuvant Chemotherapy for Breast Cancer in the Multicentre Randomized Phase 2 DIRECT Trial. Nat. Commun. 2020, 11, 3083–3093. [Google Scholar] [CrossRef]
- Omar, E.M.; Omran, G.A.; Mustafa, M.F.; El-Khodary, N.M. Intermittent Fasting during Adjuvant Chemotherapy may Promote Differential Stress Resistance in Breast Cancer Patients. J. Egypt. Natl. Cancer Inst. 2022, 34, 38–44. [Google Scholar] [CrossRef]
- Zorn, S.; Ehret, J.; Schauble, R.; Rautenberg, B.; Ihorst, G.; Bertz, H.; Urbain, P.; Raynor, A. Impact of Modified Short-Term Fasting and its Combination with a Fasting Supportive Diet during Chemotherapy on the Incidence and Severity of Chemotherapy-Induced Toxicities in Cancer Patients—A Controlled Cross-Over Pilot Study. BMC Cancer 2020, 20, 578–587. [Google Scholar] [CrossRef]
- Lugtenberg, R.T.; de Groot, S.; Kaptein, A.A.; Fischer, M.J.; Kranenbarg, E.M.; Carpentier, M.D.; Cohen, D.; de Graaf, H.; Heijns, J.B.; Portielje, J.E.A.; et al. Quality of Life and Illness Perceptions in Patients with Breast Cancer using a Fasting Mimicking Diet as an Adjunct to Neoadjuvant Chemotherapy in the Phase 2 DIRECT (BOOG 2013-14) Trial. Breast Cancer Res. Treat. 2021, 185, 741–758. [Google Scholar] [CrossRef]
- Longo, V.D.; Di Tano, M.; Mattson, M.P.; Guidi, N. Intermittent and periodic fasting, longevity and disease. Nat. Aging 2021, 1, 47–59. [Google Scholar] [CrossRef]
- van Assen, M.A.L.M.; van Aert, R.C.M.; Wicherts, J.M. Meta-Analysis using Effect Size Distributions of Only Statistically Significant Studies. Psychol. Methods 2015, 20, 293–309. [Google Scholar] [CrossRef] [PubMed]
- Clifton, K.K.; Ma, C.X.; Fontana, L.; Peterson, L.L. Intermittent fasting in the prevention and treatment of cancer. CA Cancer J. Clin. 2021, 71, 527–546. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.M.; Power, D.G.; Daly, L.; Cushen, S.J.; Ní Bhuachalla, Ē.; Prado, C.M. Cancer-Associated Malnutrition, Cachexia and Sarcopenia: The Skeleton in the Hospital Closet 40 Years Later. Proc. Nutr. Soc. 2016, 75, 199–211. [Google Scholar] [CrossRef] [PubMed]
- Attar, A.; Malka, D.; Sabate, J.M.; Bonnetain, F.; Lecomte, T.; Aparicio, T.; Locher, C.; Laharie, D.; Ezenfis, J.; Taieb, J. Malnutrition is High and Underestimated during Chemotherapy in Gastrointestinal Cancer: An AGEO Prospective Cross-Sectional Multicenter Study. Nutr. Cancer 2012, 64, 535–542. [Google Scholar] [CrossRef]
- Gomes, F.; Baumgartner, A.; Bounoure, L.; Bally, M.; Deutz, N.E.; Greenwald, J.L.; Stanga, Z.; Mueller, B.; Schuetz, P. Association of Nutritional Support with Clinical Outcomes among Medical Inpatients Who are Malnourished or at Nutritional Risk: An Updated Systematic Review and Meta-Analysis. JAMA Netw. Open 2019, 2, e1915138. [Google Scholar] [CrossRef] [PubMed]
- Katano, S.; Yano, T.; Kouzu, H.; Ohori, K.; Shimomura, K.; Honma, S.; Nagaoka, R.; Inoue, T.; Takamura, Y.; Ishigo, T.; et al. Energy Intake during Hospital Stay Predicts all-Cause Mortality After Discharge Independently of Nutritional Status in Elderly Heart Failure Patients. Clin. Res. Cardiol. 2021, 110, 1202–1220. [Google Scholar] [CrossRef]
- McGovern, J.; Dolan, R.D.; Skipworth, R.J.; Laird, B.J.; McMillan, D.C. Cancer Cachexia: A Nutritional or a Systemic Inflammatory Syndrome? Br. J. Cancer 2022, 127, 379–382. [Google Scholar] [CrossRef]
- Ali, R.; Baracos, V.E.; Sawyer, M.B.; Bianchi, L.; Roberts, S.; Assenat, E.; Mollevi, C.; Senesse, P. Lean Body Mass as an Independent Determinant of Dose-Limiting Toxicity and Neuropathy in Patients with Colon Cancer Treated with FOLFOX Regimens. Cancer Med. 2016, 5, 607–616. [Google Scholar] [CrossRef]
- Ross, P.J.; Ashley, S.; Norton, A.; Priest, K.; Waters, J.S.; Eisen, T.; Smith, I.E.; O’Brien, M.E.R. Do Patients with Weight Loss have a Worse Outcome when Undergoing Chemotherapy for Lung Cancers? Br. J. Cancer 2004, 90, 1905–1911. [Google Scholar] [CrossRef]
- d’Avignon, D.A.; Puchalska, P.; Ercal, B.; Chang, Y.; Martin, S.E.; Graham, M.J.; Patti, G.J.; Han, X.; Crawford, P.A. Hepatic Ketogenic Insufficiency Reprograms Hepatic Glycogen Metabolism and the Lipidome. JCI Insight 2018, 3, e99762. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.R.; Losek, J.D. Rehydration: Role for Early use of Intravenous Dextrose. Pediatr. Emerg. Care 2009, 25, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Golden, S.D.; Earp, J.A.L. Social ecological approaches to individuals and their contexts: Twenty years of health education & behavior health promotion interventions. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2012, 39, 364–372. [Google Scholar]
- Drexler, U.; Dörfler, J.; von Grundherr, J.; Erickson, N.; Hübner, J. Fasting during cancer treatment: A systematic review. Qual. Life Res. 2023, 32, 1427–1446. [Google Scholar] [CrossRef]
- Lende, T.H.; Austdal, M.; Varhaugvik, A.E.; Skaland, I.; Gudlaugsson, E.; Kvaløy, J.T.; Akslen, L.A.; Søiland, H.; Janssen, E.A.M.; Baak, J.P.A. Influence of pre-operative oral carbohydrate loading vs. standard fasting on tumor proliferation and clinical outcome in breast cancer patients—A randomized trial. BMC Cancer 2019, 19, 1076. [Google Scholar] [CrossRef]
- Abdollahi, R.; Najafi, S.; Razmpoosh, E.; Shoormasti, R.S.; Haghighat, S.; Raji Lahiji, M.; Chamari, M.; Asgari, M.; Cheshmazar, E.; Zarrati, M. The Effect of Dietary Intervention Along with Nutritional Education on Reducing the Gastrointestinal Side Effects Caused by Chemotherapy among Women with Breast Cancer. Nutr. Cancer 2019, 71, 922–930. [Google Scholar] [CrossRef]
- De Souza, A.P.S.; da Silva, L.C.; Fayh, A.P.T. Nutritional Intervention Contributes to the Improvement of Symptoms Related to Quality of Life in Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy: A Randomized Clinical Trial. Nutrients 2021, 13, 589. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Study Size | Study Design | Cancer Type | Intervention Treatment | Comparison | Outcomes | Intervention Duration | Results | Conclusions |
|---|---|---|---|---|---|---|---|---|---|
| Riedinger et al. [30] 2020 | 24 | RCT | Ovarian Uterine Cervical | STF 48 h— only water for 24 h before and 24 h following each chemotherapy cycle. | No dietary modification (balanced, normo-caloric diet). | Chemotherapy-related side effects and QOL. | 6 cycles | There was no significant difference in chemotherapy-related side effects or in mean QOL scores between the groups. | No differential effect |
| de Groot et al. [16] 2015 | 13 | RCT | Breast | STF 48 h— only water, coffee, or tea without sugar for 24 h before and 24 h following each chemotherapy cycle. | Normal diet according to the guidelines for healthy nutrition, with a minimum of two pieces of fruit per day. | Feasibility and chemotherapy-related side effects. | 6 cycles | STF during chemotherapy was tolerated and reduced hematological toxicity (erythrocyte and thrombocyte counts). Non-haematological toxicity did not differ between the groups. | No differential effect |
| de Groot et al. [37] 2020 | 131 | RCT | Breast | FMD 96 h—plant-based substitution diet with low amino acids consisting of soups, broths, liquids, and tea for three days prior to and on the day of each chemotherapy cycle. | Normal diet. | Chemotherapy-related side effects, toxicity, Radiological, and pathological response to chemotherapy. | 6–8 cycles | There was no significant difference in chemotherapy-related side effects between the groups. A radiologically complete/partial response and pathological response occured more often in patients using the FMD. FMD also significantly reduced chemotherapy-induced DNA damage in T lymphocytes. | No differential effect |
| Omar et al. [38] 2022 | 48 | RCT | Breast | IF 72 h— fasting for 18 h, from 12 a.m. to 6 p.m., with eating allowed for 6 h, from 6 p.m. to 12 a.m. Water consumption is permitted during fasting Hours, and small quantities of vegetables, fruits, proteins, and carbohydrates, are allowed, with limitated sugar and fats on the day before, during, and after chemotherapy. | Normal diet. | Safety, practicality, chemotherapy-related side effects, and toxicity. | 4 cycles | IF during chemotherapy was tolerated and reduced the toxicity of chemotherapy to the gastrointestinal tract (nausea, vomiting, diarrhea, Grade I/II) compared to a normal diet. There was no significant difference in hematological parameters between the two groups after cycle 4. | No differential effect |
| Bauersfeld et al. [18] 2018 | 50 | RCT | Breast Ovarian | STF 60 h—only water, herbal tea, and small, standardized quantities of vegetable juice and light vegetable broth for 36 h before and 24 h after each chemotherapy cycle. | Normocaloric Mediterranean diet. | Safety and QOL | 4–6 cycles | STF during chemotherapy was tolerated and appeared to improve QOL and fatigue during chemotherapy (only AEs Grade I/II). | No differential effect |
| Dorff et al. [17] 2016 | 20 | non-RCT | Breast Ovarian Uterine Urothelial NSCLC | STF 72 h—only water, non-caloric beverages, and small quantities of juice or food (under 200 kcal/24 h) for 48 h before and 24 h after chemotherapy. | STF 24 h or 48 h—only water, non-caloric beverages, and small quantities of juice or food under 200 kcal/24 h for 24 h or 48 h before chemotherapy. | Safety, feasibility, and chemotherapy-related side effects toxicity. | 2 cycles | Reduction of DNA damage in leukocytes from subjects who fasted for ≥48 h (p = 0.08). There was no significant difference in neutropenia (Grade III/IV) in the 48 and 72 h cohorts compared to 24 h cohort. | No differential effect |
| Zorn et al. [39] 2020 | 51 | non-RCT | Breast Endometrial Ovarian Cervical | mSTF 96 h—Ketogenic diet that provided between 400 and 600 kcal/day for 72 h before and 24 h after chemotherapy | Normocaloric diet | Chemotherapy-related side effects, toxicity, QOL, fasting-related discomfort, compliance, nutritional status, and laboratory parameters. | 4–6 cycles | Reduced chemotherapy-induced toxicities (stomatitis, headaches, weakness; Grade I/II) and total toxicity score in mSTF group. There were significantly fewer post-mSTF chemotherapy postponements. | No differential effect |
| Lugtenberg et al. [40] 2021 | 131 | RCT | Breast | FMD 96 h—plant-based, low amino acid substitution diet consisting of soups, broths, liquids, and tea) for three days prior to and on the day of each chemotherapy cycle. | Normal diet. | QOL and illness perceptions. | 6–8 cycles | Improved QOL and illness percepition. | No differential effect |
| Sadfie et al. [19] 2009 | 10 | Case series | Breast Prostate Ovarian UterineNSCLC, Esophageal | Voluntarily fasted 48–140 h and/or following 5–56 h prior to chemotherapy | / | Chemotherapy-related side effects, toxicity | Average of 4 cycles | Six patients during chemotherapy with or without fasting reported a reduction in fatigue, weakness, and gastrointestinal side effects while fasting. | No differential effect |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferro, Y.; Maurotti, S.; Tarsitano, M.G.; Lodari, O.; Pujia, R.; Mazza, E.; Lascala, L.; Russo, R.; Pujia, A.; Montalcini, T. Therapeutic Fasting in Reducing Chemotherapy Side Effects in Cancer Patients: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2666. https://doi.org/10.3390/nu15122666
Ferro Y, Maurotti S, Tarsitano MG, Lodari O, Pujia R, Mazza E, Lascala L, Russo R, Pujia A, Montalcini T. Therapeutic Fasting in Reducing Chemotherapy Side Effects in Cancer Patients: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(12):2666. https://doi.org/10.3390/nu15122666
Chicago/Turabian StyleFerro, Yvelise, Samantha Maurotti, Maria Grazia Tarsitano, Oscar Lodari, Roberta Pujia, Elisa Mazza, Lidia Lascala, Raffaella Russo, Arturo Pujia, and Tiziana Montalcini. 2023. "Therapeutic Fasting in Reducing Chemotherapy Side Effects in Cancer Patients: A Systematic Review and Meta-Analysis" Nutrients 15, no. 12: 2666. https://doi.org/10.3390/nu15122666
APA StyleFerro, Y., Maurotti, S., Tarsitano, M. G., Lodari, O., Pujia, R., Mazza, E., Lascala, L., Russo, R., Pujia, A., & Montalcini, T. (2023). Therapeutic Fasting in Reducing Chemotherapy Side Effects in Cancer Patients: A Systematic Review and Meta-Analysis. Nutrients, 15(12), 2666. https://doi.org/10.3390/nu15122666