
Effects of Prolonged Fasting during Inpatient Multimodal Treatment on Pain and Functional Parameters in Knee and Hip Osteoarthritis: A Prospective Exploratory Observational Study

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Interventions
2.4. Participants
2.5. Variables
2.6. Data Collection/Measurement
2.7. Bias
2.8. Study Size
2.9. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- RKI. 12-Monats-Prävalenz von Arthrose in Deutschland. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsJ/FactSheets/JoHM_03_2017_Praevalenz_Arthrose.pdf (accessed on 11 December 2022).
- Knapik, J.J.; Pope, R.; Orr, R.; Schram, B. Osteoarthritis: Pathophysiology, Prevalence, Risk Factors, and Exercise for Reducing Pain and Disability. J. Spec. Oper. Med. 2018, 18, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Vina, E.R.; Kwoh, C.K. Epidemiology of osteoarthritis: Literature update. Curr. Opin. Rheumatol. 2018, 30, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Wei, N.; Dai, Z. The Role of Nutrition in Osteoarthritis: A Literature Review. Clin. Geriatr. Med. 2022, 38, 303–322. [Google Scholar] [CrossRef] [PubMed]
- Di Francesco, A.; Di Germanio, C.; Bernier, M.; de Cabo, R. A time to fast. Science 2018, 362, 770–775. [Google Scholar] [CrossRef]
- Michalsen, A. Prolonged fasting as a method of mood enhancement in chronic pain syndromes: A review of clinical evidence and mechanisms. Curr. Pain. Headache Rep. 2010, 14, 80–87. [Google Scholar] [CrossRef]
- Wilhelmi de Toledo, F.; Grundler, F.; Bergouignan, A.; Drinda, S.; Michalsen, A. Safety, health improvement and well-being during a 4 to 21-day fasting period in an observational study including 1422 subjects. PLoS ONE 2019, 14, e0209353. [Google Scholar] [CrossRef]
- Drinda, S.; Grundler, F.; Neumann, T.; Lehmann, T.; Steckhan, N.; Michalsen, A.; Wilhelmi de Toledo, F. Effects of Periodic Fasting on Fatty Liver Index-A Prospective Observational Study. Nutrients 2019, 11, 2601. [Google Scholar] [CrossRef]
- Hasanpour-Dehkordi, A.; Kabiri, F.; Dris, F. Comparing the Effects of Massage Therapy and Aromatherapy on Knee Pain, Morning Stiffness, Daily Life Function, and Quality of Life in Patients with Knee Osteoarthritis. Complement. Med. Res. 2021, 28, 292–299. [Google Scholar] [CrossRef]
- Ring, R.M.; Eisenmann, C.; Kandil, F.I.; Steckhan, N.; Demmrich, S.; Klatte, C.; Kessler, C.S.; Jeitler, M.; Boschmann, M.; Michalsen, A.; et al. Mental and Behavioural Responses to Baha’i Fasting: Looking behind the Scenes of a Religiously Motivated Intermittent Fast Using a Mixed Methods Approach. Nutrients 2022, 14, 1038. [Google Scholar] [CrossRef]
- Schmidt, S.; Stange, R.; Lischka, E.; Kiehntopf, M.; Deufel, T.; Loth, D.; Uhlemann, C. Uncontrolled clinical study of the efficacy of ambulant fasting in patients with osteoarthritis. Forsch. Komplementmed. 2010, 17, 87–94. [Google Scholar] [CrossRef]
- Kjeldsen-Kragh, J.; Sumar, N.; Bodman-Smith, K.; Brostoff, J. Changes in glycosylation of IgG during fasting in patients with rheumatoid arthritis. Br. J. Rheumatol. 1996, 35, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen-Kragh, J.; Mellbye, O.J.; Haugen, M.; Mollnes, T.E.; Hammer, H.B.; Sioud, M.; Førre, O. Changes in laboratory variables in rheumatoid arthritis patients during a trial of fasting and one-year vegetarian diet. Scand. J. Rheumatol. 1995, 24, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen-Kragh, J.; Haugen, M.; Borchgrevink, C.F.; Laerum, E.; Eek, M.; Mowinkel, P.; Hovi, K.; Førre, O. Controlled trial of fasting and one-year vegetarian diet in rheumatoid arthritis. Lancet 1991, 338, 899–902. [Google Scholar] [CrossRef] [PubMed]
- Muller, H.; de Toledo, F.W.; Resch, K.L. Fasting followed by vegetarian diet in patients with rheumatoid arthritis: A systematic review. Scand. J. Rheumatol. 2001, 30, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wilhelmi de Toledo, F.; Buchinger, A.; Burggrabe, H.; Holz, G.; Kuhn, C.; Lischka, E.; Lischka, N.; Lutzner, H.; May, W.; Ritzmann-Widderich, M.; et al. Fasting therapy—An expert panel update of the 2002 consensus guidelines. Forsch. Komplementmed. 2013, 20, 434–443. [Google Scholar] [CrossRef]
- Fischer, J.M.; Kandil, F.I.; Kessler, C.S.; Nayeri, L.; Zager, L.S.; Rocabado Hennhofer, T.; Steckhan, N.; Koppold-Liebscher, D.A.; Bringmann, H.C.; Schafer, T.; et al. Stress Reduction by Yoga versus Mindfulness Training in Adults Suffering from Distress: A Three-Armed Randomized Controlled Trial including Qualitative Interviews (RELAX Study). J. Clin. Med. 2022, 11, 5680. [Google Scholar] [CrossRef]
- Kessler, C.S.; Jeitler, M.; Dhiman, K.S.; Kumar, A.; Ostermann, T.; Gupta, S.; Morandi, A.; Mittwede, M.; Stapelfeldt, E.; Spoo, M.; et al. Ayurveda in Knee Osteoarthritis-Secondary Analyses of a Randomized Controlled Trial. J. Clin. Med. 2022, 11, 3047. [Google Scholar] [CrossRef]
- Bringmann, H.C.; Michalsen, A.; Jeitler, M.; Kessler, C.S.; Brinkhaus, B.; Brunnhuber, S.; Sedlmeier, P. Meditation-based lifestyle modification in mild to moderate depression-A randomized controlled trial. Depress. Anxiety 2022, 39, 363–375. [Google Scholar] [CrossRef]
- Jeitler, M.; Michalsen, A.; Schwiertz, A.; Kessler, C.S.; Koppold-Liebscher, D.; Grasme, J.; Kandil, F.I.; Steckhan, N. Effects of a Supplement Containing a Cranberry Extract on Recurrent Urinary Tract Infections and Intestinal Microbiota: A Prospective, Uncontrolled Exploratory Study. J. Integr. Complement. Med. 2022, 28, 399–406. [Google Scholar] [CrossRef]
- Jeitler, M.; Wottke, T.; Schumann, D.; Puerto Valencia, L.M.; Michalsen, A.; Steckhan, N.; Mittwede, M.; Stapelfeldt, E.; Koppold-Liebscher, D.; Cramer, H.; et al. Ayurvedic vs. Conventional Nutritional Therapy Including Low-FODMAP Diet for Patients With Irritable Bowel Syndrome-A Randomized Controlled Trial. Front. Med. 2021, 8, 622029. [Google Scholar] [CrossRef]
- Jeitler, M.; Michalsen, A.; Frings, D.; Hubner, M.; Fischer, M.; Koppold-Liebscher, D.A.; Murthy, V.; Kessler, C.S. Significance of Medicinal Mushrooms in Integrative Oncology: A Narrative Review. Front. Pharmacol. 2020, 11, 580656. [Google Scholar] [CrossRef]
- Jeitler, M.; Roth, S.; Steckhan, N.; Meier, L.; Koppold-Liebscher, D.A.; Kandil, F.I.; Ostermann, T.; Stange, R.; Kessler, C.S.; Brinkhaus, B.; et al. Therapeutic Phlebotomy in Patients with Grade 1 Hypertension: A Randomized-Controlled Trial. J. Integr. Complement. Med. 2022, 28, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Hohmann, C.D.; Stange, R.; Steckhan, N.; Robens, S.; Ostermann, T.; Paetow, A.; Michalsen, A. The Effectiveness of Leech Therapy in Chronic Low Back Pain. Dtsch. Arztebl. Int. 2018, 115, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Ludtke, R.; Cesur, O.; Afra, D.; Musial, F.; Baecker, M.; Fink, M.; Dobos, G.J. Effectiveness of leech therapy in women with symptomatic arthrosis of the first carpometacarpal joint: A randomized controlled trial. Pain 2008, 137, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Klotz, S.; Ludtke, R.; Moebus, S.; Spahn, G.; Dobos, G.J. Effectiveness of leech therapy in osteoarthritis of the knee: A randomized, controlled trial. Ann. Intern. Med. 2003, 139, 724–730. [Google Scholar] [CrossRef]
- Michalsen, A.; Moebus, S.; Spahn, G.; Esch, T.; Langhorst, J.; Dobos, G.J. Leech therapy for symptomatic treatment of knee osteoarthritis: Results and implications of a pilot study. Altern. Ther. Health Med. 2002, 8, 84–88. [Google Scholar]
- Michalsen, A.; Ludtke, R.; Buhring, M.; Spahn, G.; Langhorst, J.; Dobos, G.J. Thermal hydrotherapy improves quality of life and hemodynamic function in patients with chronic heart failure. Am. Heart J. 2003, 146, 728–733. [Google Scholar] [CrossRef]
- Jeitler, M.; Jaspers, J.; von Scheidt, C.; Koch, B.; Michalsen, A.; Steckhan, N.; Kessler, C.S. Mind-body medicine and lifestyle modification in supportive cancer care: A cohort study on a day care clinic program for cancer patients. Psychooncology 2017, 26, 2127–2134. [Google Scholar] [CrossRef]
- Hartmann, A.M.; Dell’Oro, M.; Spoo, M.; Fischer, J.M.; Steckhan, N.; Jeitler, M.; Häupl, T.; Kandil, F.I.; Michalsen, A.; Koppold-Liebscher, D.A.; et al. To eat or not to eat—An exploratory randomized controlled trial on fasting and plant-based diet in rheumatoid arthritis (NutriFast-study). Front. Nutr. 2022, 9, 1030380. [Google Scholar] [CrossRef]
- Jeitler, M.; Lauche, R.; Hohmann, C.; Choi, K.A.; Schneider, N.; Steckhan, N.; Rathjens, F.; Anheyer, D.; Paul, A.; von Scheidt, C.; et al. A Randomized Controlled Trial of Fasting and Lifestyle Modification in Patients with Metabolic Syndrome: Effects on Patient-Reported Outcomes. Nutrients 2022, 14, 3559. [Google Scholar] [CrossRef]
- Cramer, H.; Hohmann, C.; Lauche, R.; Choi, K.A.; Schneider, N.; Steckhan, N.; Rathjens, F.; Anheyer, D.; Paul, A.; von Scheidt, C.; et al. Effects of Fasting and Lifestyle Modification in Patients with Metabolic Syndrome: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 4751. [Google Scholar] [CrossRef] [PubMed]
- Koppold-Liebscher, D.A.; Klatte, C.; Demmrich, S.; Schwarz, J.; Kandil, F.I.; Steckhan, N.; Ring, R.; Kessler, C.S.; Jeitler, M.; Koller, B.; et al. Effects of Daytime Dry Fasting on Hydration, Glucose Metabolism and Circadian Phase: A Prospective Exploratory Cohort Study in Baha’i Volunteers. Front. Nutr. 2021, 8, 662310. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.M.; Dell’Oro, M.; Kessler, C.S.; Schumann, D.; Steckhan, N.; Jeitler, M.; Fischer, J.M.; Spoo, M.; Kriegel, M.A.; Schneider, J.G.; et al. Efficacy of therapeutic fasting and plant-based diet in patients with rheumatoid arthritis (NutriFast): Study protocol for a randomised controlled clinical trial. BMJ Open 2021, 11, e047758. [Google Scholar] [CrossRef]
- Maifeld, A.; Bartolomaeus, H.; Löber, U.; Avery, E.G.; Steckhan, N.; Markó, L.; Wilck, N.; Hamad, I.; Šušnjar, U.; Mähler, A.; et al. Fasting alters the gut microbiome reducing blood pressure and body weight in metabolic syndrome patients. Nat. Commun. 2021, 12, 1970. [Google Scholar] [CrossRef]
- Koppold-Liebscher, D.; Kessler, C.S.; Steckhan, N.; Bahr, V.; Kempter, C.; Wischnewsky, M.; Hubner, M.; Kunz, B.; Paul, M.; Zorn, S.; et al. Short-term fasting accompanying chemotherapy as a supportive therapy in gynecological cancer: Protocol for a multicenter randomized controlled clinical trial. Trials 2020, 21, 854. [Google Scholar] [CrossRef] [PubMed]
- Bahr, L.S.; Bock, M.; Liebscher, D.; Bellmann-Strobl, J.; Franz, L.; Pruss, A.; Schumann, D.; Piper, S.K.; Kessler, C.S.; Steckhan, N.; et al. Ketogenic diet and fasting diet as Nutritional Approaches in Multiple Sclerosis (NAMS): Protocol of a randomized controlled study. Trials 2020, 21, 3. [Google Scholar] [CrossRef]
- Li, C.; Sadraie, B.; Steckhan, N.; Kessler, C.; Stange, R.; Jeitler, M.; Michalsen, A. Effects of A One-week Fasting Therapy in Patients with Type-2 Diabetes Mellitus and Metabolic Syndrome—A Randomized Controlled Explorative Study. Exp. Clin. Endocrinol. Diabetes 2017, 125, 618–624. [Google Scholar] [CrossRef]
- Choi, I.Y.; Piccio, L.; Childress, P.; Bollman, B.; Ghosh, A.; Brandhorst, S.; Suarez, J.; Michalsen, A.; Cross, A.H.; Morgan, T.E.; et al. A Diet Mimicking Fasting Promotes Regeneration and Reduces Autoimmunity and Multiple Sclerosis Symptoms. Cell. Rep. 2016, 15, 2136–2146. [Google Scholar] [CrossRef]
- Michalsen, A.; Li, C. Fasting therapy for treating and preventing disease—Current state of evidence. Forsch. Komplementmed. 2013, 20, 444–453. [Google Scholar] [CrossRef]
- Stange, R.; Pflugbeil, C.; Michalsen, A.; Uehleke, B. Therapeutic fasting in patients with metabolic syndrome and impaired insulin resistance. Forsch. Komplementmed. 2013, 20, 421–426. [Google Scholar] [CrossRef]
- Li, C.; Ostermann, T.; Hardt, M.; Ludtke, R.; Broecker-Preuss, M.; Dobos, G.; Michalsen, A. Metabolic and psychological response to 7-day fasting in obese patients with and without metabolic syndrome. Forsch. Komplementmed. 2013, 20, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Li, C.; Kaiser, K.; Ludtke, R.; Meier, L.; Stange, R.; Kessler, C. In-Patient Treatment of Fibromyalgia: A Controlled Nonrandomized Comparison of Conventional Medicine versus Integrative Medicine including Fasting Therapy. Evid. Based Complement. Alternat. Med. 2013, 2013, 908610. [Google Scholar] [CrossRef] [PubMed]
- Abendroth, A.; Michalsen, A.; Ludtke, R.; Ruffer, A.; Musial, F.; Dobos, G.J.; Langhorst, J. Changes of Intestinal Microflora in Patients with Rheumatoid Arthritis during Fasting or a Mediterranean Diet. Forsch. Komplementmed. 2010, 17, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Frey, U.H.; Merse, S.; Siffert, W.; Dobos, G.J. Hunger and mood during extended fasting are dependent on the GNB3 C825T polymorphism. Ann. Nutr. Metab. 2009, 54, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Kuhlmann, M.K.; Ludtke, R.; Backer, M.; Langhorst, J.; Dobos, G.J. Prolonged fasting in patients with chronic pain syndromes leads to late mood-enhancement not related to weight loss and fasting-induced leptin depletion. Nutr. Neurosci. 2006, 9, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Hoffmann, B.; Moebus, S.; Backer, M.; Langhorst, J.; Dobos, G.J. Incorporation of fasting therapy in an integrative medicine ward: Evaluation of outcome, safety, and effects on lifestyle adherence in a large prospective cohort study. J. Altern. Complement. Med. 2005, 11, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Riegert, M.; Lüdtke, R.; Bäcker, M.; Langhorst, J.; Schwickert, M.; Dobos, G.J. Mediterranean diet or extended fasting’s influence on changing the intestinal microflora, immunoglobulin A secretion and clinical outcome in patients with rheumatoid arthritis and fibromyalgia: An observational study. BMC Complement. Altern. Med. 2005, 5, 22. [Google Scholar] [CrossRef]
- Michalsen, A.; Schlegel, F.; Rodenbeck, A.; Ludtke, R.; Huether, G.; Teschler, H.; Dobos, G.J. Effects of short-term modified fasting on sleep patterns and daytime vigilance in non-obese subjects: Results of a pilot study. Ann. Nutr. Metab. 2003, 47, 194–200. [Google Scholar] [CrossRef]
- Michalsen, A.; Schneider, S.; Rodenbeck, A.; Ludtke, R.; Huether, G.; Dobos, G.J. The short-term effects of fasting on the neuroendocrine system in patients with chronic pain syndromes. Nutr. Neurosci. 2003, 6, 11–18. [Google Scholar] [CrossRef]
- Michalsen, A.; Weidenhammer, W.; Melchart, D.; Langhorst, J.; Saha, J.; Dobos, G. Short-term therapeutic fasting in the treatment of chronic pain and fatigue syndromes--well-being and side effects with and without mineral supplements. Forsch. Komplementarmed. Klass. Naturheilkd. 2002, 9, 221–227. [Google Scholar] [CrossRef]
- Clement, N.D.; Bardgett, M.; Weir, D.; Holland, J.; Gerrand, C.; Deehan, D.J. What is the Minimum Clinically Important Difference for the WOMAC Index After TKA? Clin. Orthop. Relat. Res. 2018, 476, 2005–2014. [Google Scholar] [CrossRef] [PubMed]
- Ariani, A.; Bazzichi, L.; Sarzi-Puttini, P.; Salaffi, F.; Manara, M.; Prevete, I.; Bortoluzzi, A.; Carrara, G.; Scirè, C.A.; Ughi, N.; et al. The Italian Society for Rheumatology clinical practice guidelines for the diagnosis and management of fibromyalgia Best practices based on current scientific evidence. Reumatismo 2021, 73, 89–105. [Google Scholar] [CrossRef] [PubMed]
- Oudmaijer, C.A.J.; Minnee, R.C.; Pol, R.A.; van den Boogaard, W.M.C.; Komninos, D.S.J.; van de Wetering, J.; van Heugten, M.H.; Hoorn, E.J.; Sanders, J.S.F.; Hoeijmakers, J.H.J.; et al. Fasting before living-kidney donation: Effect on donor well-being and postoperative recovery: Study protocol of a multicenter randomized controlled trial. Trials 2022, 23, 18. [Google Scholar] [CrossRef]
- Hofer, S.J.; Carmona-Gutierrez, D.; Mueller, M.I.; Madeo, F. The ups and downs of caloric restriction and fasting: From molecular effects to clinical application. EMBO Mol. Med. 2022, 14, e14418. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, E.; van Caam, A.; van der Kraan, P.M. Obesity and osteoarthritis, more than just wear and tear: Pivotal roles for inflamed adipose tissue and dyslipidaemia in obesity-induced osteoarthritis. Rheumatology 2015, 54, 588–600. [Google Scholar] [CrossRef]
- Morales-Ivorra, I.; Romera-Baures, M.; Roman-Vinas, B.; Serra-Majem, L. Osteoarthritis and the Mediterranean Diet: A Systematic Review. Nutrients 2018, 10, 1030. [Google Scholar] [CrossRef]
- Tu, C.; He, J.; Wu, B.; Wang, W.; Li, Z. An extensive review regarding the adipokines in the pathogenesis and progression of osteoarthritis. Cytokine 2019, 113, 1–12. [Google Scholar] [CrossRef]
- Gabriel, S.; Ncube, M.; Zeiler, E.; Thompson, N.; Karlsen, M.C.; Goldman, D.M.; Glavas, Z.; Beauchesne, A.; Scharf, E.; Goldhamer, A.C.; et al. A Six-Week Follow-Up Study on the Sustained Effects of Prolonged Water-Only Fasting and Refeeding on Markers of Cardiometabolic Risk. Nutrients 2022, 14, 4313. [Google Scholar] [CrossRef]
- Andersson, M.; Haglund, E.; Aili, K.; Bremander, A.; Bergman, S. Associations between metabolic factors and radiographic knee osteoarthritis in early disease—A cross-sectional study of individuals with knee pain. BMC Musculoskelet. Disord. 2022, 23, 938. [Google Scholar] [CrossRef]
- Papathanasiou, I.; Anastasopoulou, L.; Tsezou, A. Cholesterol metabolism related genes in osteoarthritis. Bone 2021, 152, 116076. [Google Scholar] [CrossRef]
- Song, Y.; Liu, J.; Zhao, K.; Gao, L.; Zhao, J. Cholesterol-induced toxicity: An integrated view of the role of cholesterol in multiple diseases. Cell. Metab. 2021, 33, 1911–1925. [Google Scholar] [CrossRef] [PubMed]
- Ertürk, C.; Altay, M.A.; Bilge, A.; Çelik, H. Is there a relationship between serum ox-LDL, oxidative stress, and PON1 in knee osteoarthritis? Clin. Rheumatol. 2017, 36, 2775–2780. [Google Scholar] [CrossRef] [PubMed]
- Fond, G.; Macgregor, A.; Leboyer, M.; Michalsen, A. Fasting in mood disorders: Neurobiology and effectiveness. A review of the literature. Psychiatry Res. 2013, 209, 253–258. [Google Scholar] [CrossRef]
- Watkins, E.; Serpell, L. The Psychological Effects of Short-Term Fasting in Healthy Women. Front. Nutr. 2016, 3, 27. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | All Patients | Knee OA | Hip OA |
|---|---|---|---|---|
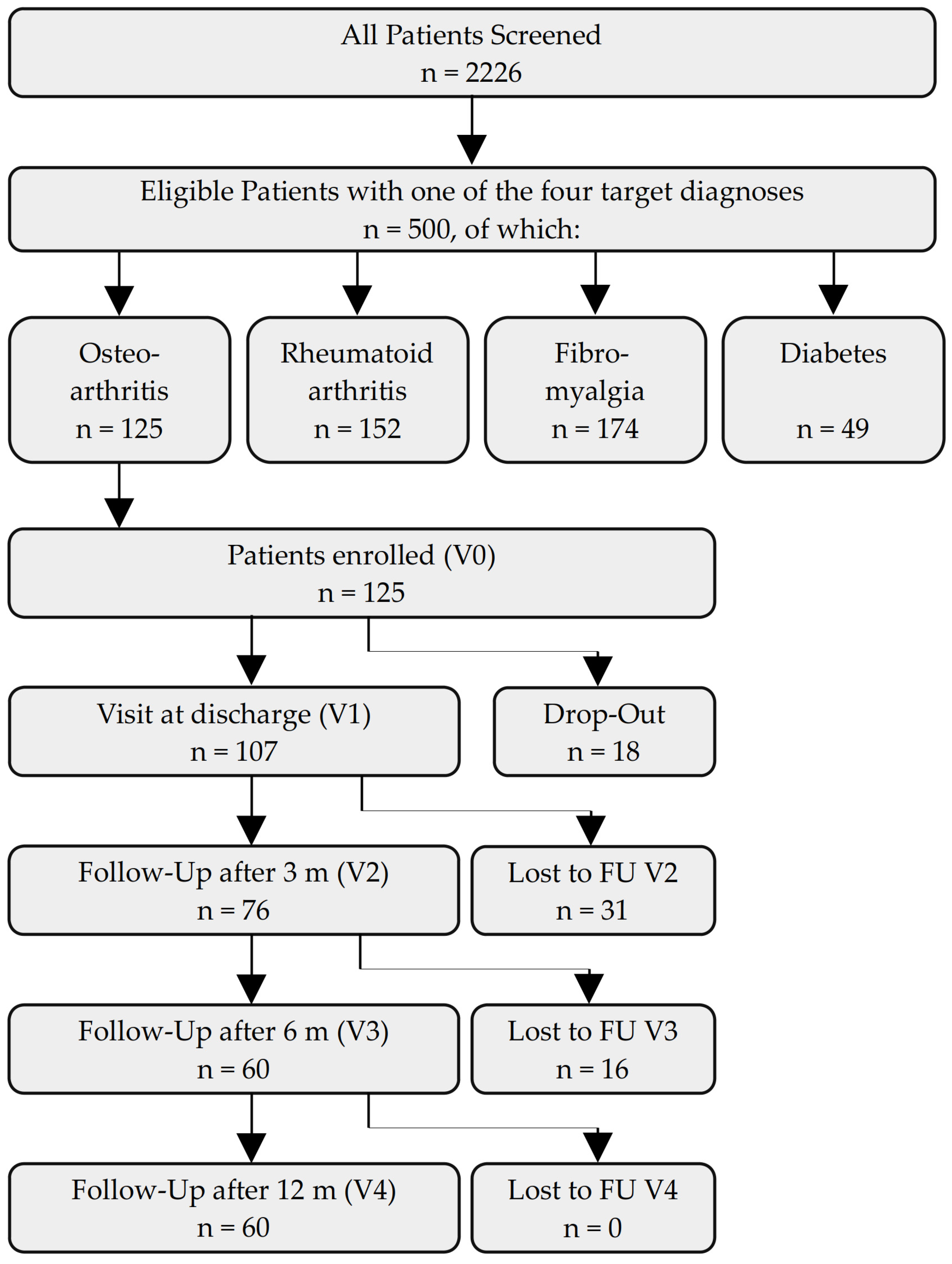
| Total | 125 (100.0%) | 97 (100.0%) | 28 (100.0%) | |
| Sex | Female | 107 (85.6%) | 81 (83.5%) | 26 (92.9%) |
| Male | 18 (14.4%) | 16 (16.5%) | 2 (7.1%) | |
| Age group (years) | 18–35 | 2 (1.6%) | 2 (2.1%) | 0 (0.0%) |
| 36–50 | 8 (6.4%) | 5 (5.2%) | 3 (10.7%) | |
| 51–65 | 77 (61.6%) | 64 (66.0%) | 13 (46.4%) | |
| 66–80 | 38 (30.4%) | 26 (26.8%) | 12 (42.9%) | |
| Marital status | single | 16 (12.8%) | 14 (14.4%) | 2 (7.1%) |
| married | 69 (55.2%) | 51 (52.6%) | 18 (64.3%) | |
| separated or divorced | 29 (23.2%) | 23 (23.7%) | 6 (21.5%) | |
| widowed | 9 (7.2%) | 7 (7.2%) | 2 (7.1%) | |
| other | 2 (1.6%) | 2 (2.1%) | 0 (0.0%) | |
| Household | single | 43 (34.4%) | 36 (37.1%) | 7 (25.0%) |
| with partner | 61 (48.8%) | 43 (44.3%) | 18 (64.3%) | |
| single with children | 4 (3.2%) | 4 (4.1%) | 0 (0.0%) | |
| with partner and children | 15 (12.0%) | 12 (12.4%) | 3 (10.7%) | |
| other | 2 (1.6%) | 2 (1.2%) | 0 (0.0%) | |
| Highest educational level | primary schooling | 8 (6.4%) | 6 (6.2%) | 2 (7.1%) |
| secondary schooling | 34 (27.2%) | 26 (26.8%) | 8 (28.6%) | |
| high school | 21 (16.8%) | 17 (17.5%) | 4 (14.3%) | |
| university degree | 56 (44.8%) | 43 (44.3%) | 13 (46.4%) | |
| other | 6 (4.8%) | 5 (5.2%) | 1 (3.6%) | |
| Occupation | self-employed | 12 (9.6%) | 10 (10.3%) | 2 (7.1%) |
| civil servant | 5 (4.0%) | 4 (4.1%) | 1 (3.6%) | |
| employed | 39 (31.2%) | 31 (32.0%) | 8 (28.6%) | |
| worker | 2 (1.6%) | 1 (1.0%) | 1 (3.6%) | |
| homemaker | 3 (2.4%) | 3 (3.1%) | 0 (0.0%) | |
| unemployed | 5 (4.0%) | 5 (5.2%) | 0 (0.0%) | |
| retired | 43 (34.4%) | 30 (30.9%) | 13 (46.4%) | |
| permanently disabled | 12 (9.6%) | 10 (10.3%) | 2 (7.1%) | |
| other | 4 (3.2%) | 3 (3.1%) | 1 (3.6%) | |
| Annual gross salary | <20.000 Euros | 49 (39.2%) | 40 (41.2%) | 9 (32.1%) |
| 20–40.000 Euro | 42 (33.6%) | 33 (34.0%) | 9 (32.1%) | |
| 40–60.000 Euro | 21 (16.8%) | 14 (14.4%) | 7 (25.0%) | |
| 60–80.000 Euro | 11 (8.8%) | 8 (8.2%) | 3 (10.7%) | |
| >80.000 Euro | 2 (1.6%) | 2 (2.1%) | 0 (0.0%) | |
| Subjective physical health status | not impaired | 1 (0.8%) | 1 (1.0%) | 0 (0.0%) |
| mildly impaired | 16 (12.8%) | 11 (11.3%) | 5 (17.9%) | |
| impaired | 76 (60.8%) | 59 (60.8%) | 17 (60.7%) | |
| strongly impaired | 32 (25.6%) | 26 (26.8%) | 6 (21.4%) | |
| Subjective psychological health status | not impaired | 21 (16.8%) | 15 (15.5%) | 6 (21.4%) |
| mildly impaired | 49 (39.2%) | 36 (37.1%) | 13 (46.4%) | |
| impaired | 38 (30.4%) | 32 (33.0%) | 6 (21.4%) | |
| strongly impaired | 17 (13.6%) | 14 (14.4%) | 3 (10.7%) | |
| Psychotherapy | none so far | 49 (39.2%) | 37 (38.1%) | 12 (42.9%) |
| ealier | 57 (45.6%) | 45 (46.4%) | 12 (42.9%) | |
| currently | 19 (15.2%) | 15 (15.5%) | 4 (14.3%) | |
| Integrative medicine | familiar with concept | 86 (68.8%) | 65 (67.0%) | 21 (75.0%) |
| Stay at this clinic | first | 83 (66.4%) | 67 (69.1%) | 16 (57.1%) |
| second | 23 (18.4%) | 16 (16.5%) | 7 (25.0%) | |
| third | 12 (9.6%) | 8 (8.2%) | 4 (14.3%) | |
| fourth | 7 (5.6%) | 6 (6.2%) | 1 (3.6%) | |
| Fasting experience | never | 56 (44.8%) | 44 (45.4%) | 12 (42.9%) |
| once | 17 (13.6%) | 12 (12.4%) | 5 (17.9%) | |
| twice | 18 (14.4%) | 14 (14.4%) | 4 (14.3%) | |
| 3 times | 9 (7.2%) | 7 (7.2%) | 2 (7.1%) | |
| 4 times | 5 (4.0%) | 5 (5.2%) | 0 (0.0%) | |
| 5 times and more | 20 (16.0%) | 15 (15.5%) | 5 (17.9%) | |
| Medication at admission | Opioids | 11 (8.8%) | 8 (8.2%) | 3 (10.7%) |
| Pain Medication | 115 (92.0%) | 88 (90.7%) | 27 (96.4%) | |
| Herbal Remedies | 52 (41.6%) | 40 (41.2%) | 12 (42.9%) | |
| Subjective impairment by OA | NRS [0–10]: M ± SD | 6.1 (±1.6) | 6.2 (±1.6) | 5.9 (±1.5) |
| Anticipation of efficacy | NRS [0–10]: M ± SD | 6.4 (±2.0) | 6.4 (±1.9) | 6.4 (±2.5) |
| Difference between V1 and V0 * | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter | Visit | M | SD | n | M | SD | T | p | d |
| Cholesterol (mg/dL) | V0 | 239.2 | 44.86 | 84 | |||||
| V1 | 201.1 | 48.85 | 70 | −38.4 | 31.20 | 10.23 | <0.001 | 0.80 | |
| LDL (mg/dL) | V0 | 155.9 | 38.27 | 81 | |||||
| V1 | 129.8 | 46.91 | 63 | −24.5 | 30.72 | 6.29 | <0.001 | 0.56 | |
| HDL (mg/dL) | V0 | 58.2 | 13.80 | 81 | |||||
| V1 | 49.2 | 12.61 | 62 | −8.0 | 7.74 | 8.12 | <0.001 | 0.59 | |
| Triglycerides (mg/dL) | V0 | 133.7 | 66.42 | 84 | |||||
| V1 | 113.1 | 47.25 | 66 | −24.5 | 67.43 | 2.92 | 0.005 | 0.42 | |
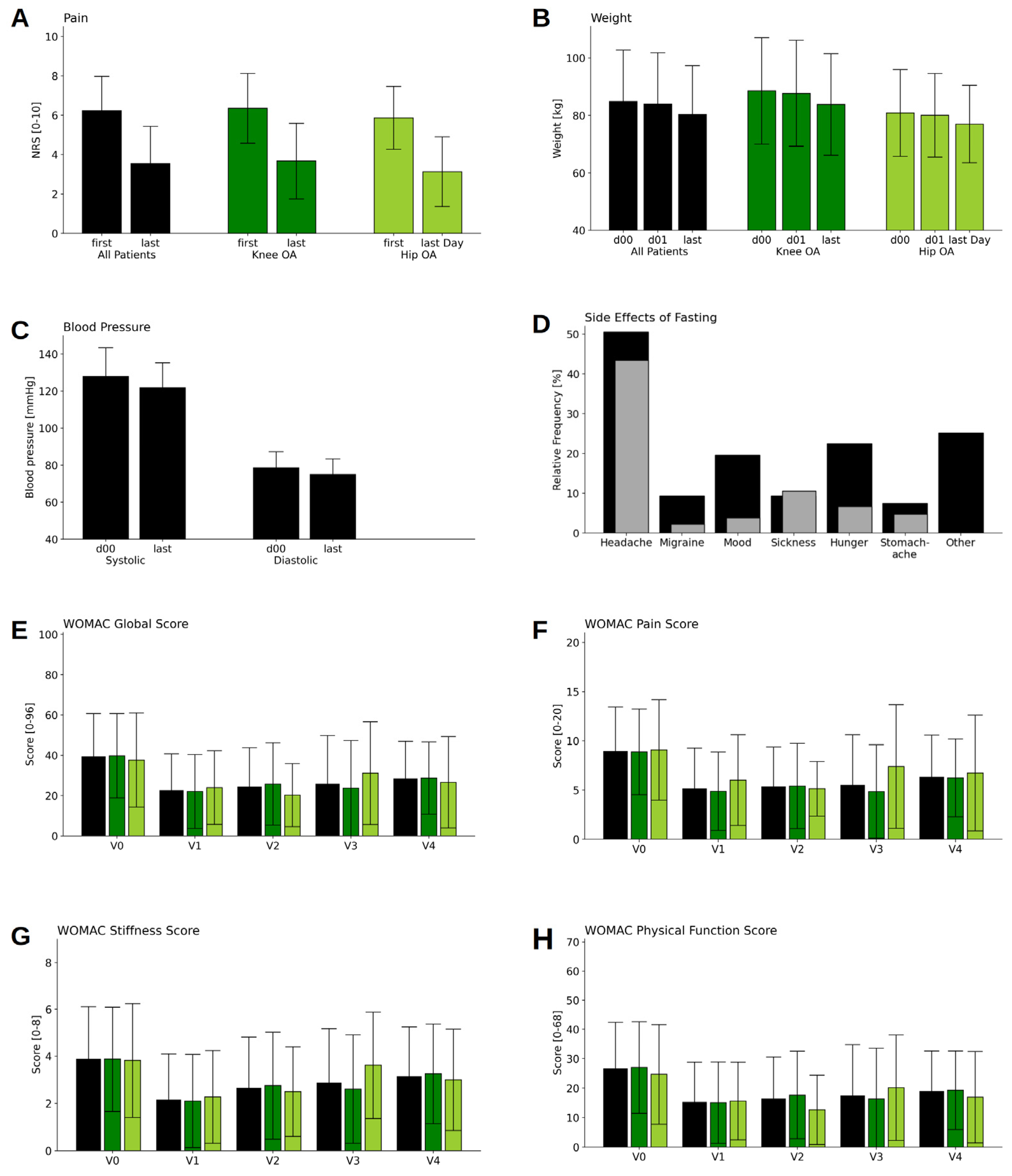
| NRSPain (scale 0–10) | V0 | 6.2 | 1.72 | 90 | |||||
| V1 | 3.5 | 1.87 | 64 | −2.7 | 1.98 | 10.8 | <0.001 | 1.48 | |
| Weight (kg) | V0 | 84.8 | 17.9 | 115 | |||||
| D 01 | 83.9 | 17.74 | 115 | ||||||
| V1 | 80.3 | 16.88 | 115 | −3.6 | 1.65 | 23.29 | <0.001 | 0.21 | |
| Systolic BP (mmHg) | V0 | 128.0 | 15.34 | 115 | |||||
| V1 | 121.8 | 13.42 | 115 | −6.2 | 15.93 | 4.15 | <0.001 | 0.43 | |
| Diastolic BP (mmHg) | V0 | 78.6 | 8.61 | 115 | |||||
| V1 | 74.9 | 8.4 | 115 | −3.7 | 10.55 | 3.70 | <0.001 | 0.43 | |
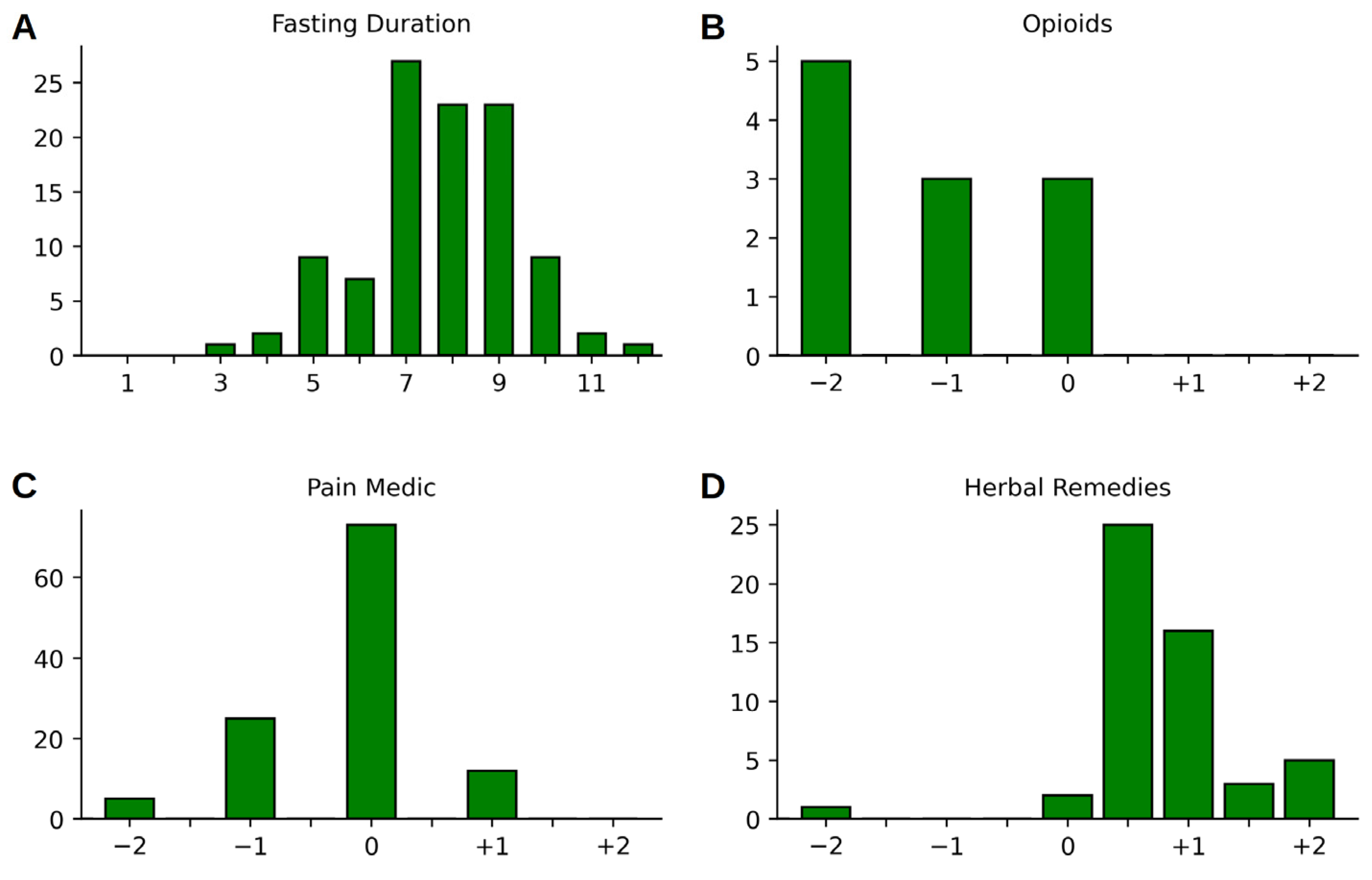
| Change | −2 | −1 | −0.5 | 0 | +0.5 | +1 | +1.5 | +2 |
|---|---|---|---|---|---|---|---|---|
| Opioids | 5 | 3 | 0 | 3 | 0 | 0 | 0 | 0 |
| Pain Medication | 5 | 25 | 0 | 73 | 0 | 12 | 0 | 0 |
| Herbal Remedies | 1 | 0 | 0 | 2 | 25 | 16 | 3 | 5 |
| Difference to V0 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter | Visit | M | SD | n | M | SD | T | p | d |
| WHO 5 | V0 | 11 | 4.74 | 107 | |||||
| V1 | 15.4 | 4.75 | 107 | 4.5 | 4.94 | 9.29 | <0.001 | 0.94 | |
| V2 | 15.3 | 4.96 | 68 | 3.6 | 4.27 | 7 | <0.001 | 0.74 | |
| V3 | 14.9 | 5.04 | 56 | 3.4 | 4.54 | 5.57 | <0.001 | 0.67 | |
| V4 | 14.3 | 4.61 | 53 | 2.7 | 5.05 | 3.8 | <0.001 | 0.56 | |
| MAAS | V0 | 3.9 | 0.87 | 107 | |||||
| V1 | 4.1 | 0.77 | 107 | 0.2 | 0.61 | 4.07 | 0.001 | 0.29 | |
| V2 | 4.2 | 0.79 | 68 | 0.2 | 0.6 | 3.28 | 0.002 | 0.28 | |
| V3 | 4 | 0.81 | 56 | 0.1 | 0.57 | 1.87 | 0.067 | 0.18 | |
| V4 | 4 | 0.91 | 53 | 0.2 | 0.71 | 1.98 | 0.053 | 0.21 | |
| HADS Depression | V0 | 10.9 | 3.74 | 107 | |||||
| V1 | 8.5 | 3.32 | 107 | −2.3 | 3.01 | 7.94 | <0.001 | 0.65 | |
| V2 | 8.5 | 3.17 | 68 | −2 | 3.13 | 5.35 | <0.001 | 0.59 | |
| V3 | 9.1 | 3.64 | 56 | −1.5 | 3.3 | 3.29 | 0.002 | 0.37 | |
| V4 | 9.5 | 3.37 | 53 | −0.9 | 2.76 | 2.32 | 0.024 | 0.24 | |
| HADS Anxiety | V0 | 10.3 | 3.73 | 107 | |||||
| V1 | 8.2 | 3.69 | 107 | −2.1 | 2.91 | 7.28 | <0.001 | 0.55 | |
| V2 | 8.3 | 3.18 | 68 | −1.7 | 2.4 | 5.91 | <0.001 | 0.52 | |
| V3 | 8.6 | 3.6 | 56 | −1.7 | 2.84 | 4.38 | <0.001 | 0.45 | |
| V4 | 9 | 3.36 | 53 | −1.1 | 2.96 | 2.76 | 0.008 | 0.32 | |
| WOMAC Global Score (0–96) | V0 | 37.7 | 19.33 | 107 | |||||
| V1 | 22.5 | 18.16 | 101 | −14.9 | 13.37 | 11.18 | <0.001 | 0.79 | |
| V2 | 23.3 | 17.25 | 68 | −12.9 | 13.84 | 7.65 | <0.001 | 0.71 | |
| V3 | 24.6 | 22.98 | 56 | −11.4 | 20.17 | 4.19 | <0.001 | 0.53 | |
| V4 | 28 | 17.98 | 53 | −10 | 18.5 | 3.89 | <0.001 | 0.55 | |
| WOMAC Pain Score (0–20) | V0 | 8.5 | 3.98 | 107 | |||||
| V1 | 5.1 | 4.12 | 101 | −3.4 | 3.61 | 9.29 | <0.001 | 0.82 | |
| V2 | 5.1 | 3.64 | 68 | −3.1 | 3.67 | 6.98 | <0.001 | 0.81 | |
| V3 | 5.2 | 5.02 | 56 | −2.7 | 4.42 | 4.58 | <0.001 | 0.59 | |
| V4 | 6.3 | 4.24 | 53 | −2 | 4.57 | 3.1 | 0.003 | 0.47 | |
| WOMAC Subscale Stiffness Score (0–8) | V0 | 3.8 | 2.18 | 107 | |||||
| V1 | 2.1 | 1.94 | 101 | −1.6 | 1.81 | 8.79 | <0.001 | 0.76 | |
| V2 | 2.6 | 2.03 | 68 | −1.2 | 1.83 | 5.26 | <0.001 | 0.56 | |
| V3 | 2.7 | 2.14 | 56 | −1 | 1.92 | 3.73 | <0.001 | 0.46 | |
| V4 | 3.2 | 2.11 | 53 | −0.6 | 2.42 | 1.91 | 0.062 | 0.31 | |
| WOMAC Physical Function Score (0–68) | V0 | 25.4 | 14.5 | 107 | |||||
| V1 | 15.2 | 13.5 | 101 | −10 | 9.8 | 10.22 | <0.001 | 0.71 | |
| V2 | 15.6 | 12.73 | 68 | −8.6 | 9.93 | 7.09 | <0.001 | 0.64 | |
| V3 | 16.6 | 16.54 | 56 | −7.7 | 14.96 | 3.81 | <0.001 | 0.49 | |
| V4 | 18.5 | 13.08 | 53 | −7.3 | 13.08 | 4.05 | <0.002 | 0.55 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koppold, D.A.; Kandil, F.I.; Güttler, O.; Müller, A.; Steckhan, N.; Meiß, S.; Breinlinger, C.; Nelle, E.; Hartmann, A.M.; Jeitler, M.; et al. Effects of Prolonged Fasting during Inpatient Multimodal Treatment on Pain and Functional Parameters in Knee and Hip Osteoarthritis: A Prospective Exploratory Observational Study. Nutrients 2023, 15, 2695. https://doi.org/10.3390/nu15122695
Koppold DA, Kandil FI, Güttler O, Müller A, Steckhan N, Meiß S, Breinlinger C, Nelle E, Hartmann AM, Jeitler M, et al. Effects of Prolonged Fasting during Inpatient Multimodal Treatment on Pain and Functional Parameters in Knee and Hip Osteoarthritis: A Prospective Exploratory Observational Study. Nutrients. 2023; 15(12):2695. https://doi.org/10.3390/nu15122695
Chicago/Turabian StyleKoppold, Daniela A., Farid I. Kandil, Oliver Güttler, Anna Müller, Nico Steckhan, Sara Meiß, Carolin Breinlinger, Esther Nelle, Anika M. Hartmann, Michael Jeitler, and et al. 2023. "Effects of Prolonged Fasting during Inpatient Multimodal Treatment on Pain and Functional Parameters in Knee and Hip Osteoarthritis: A Prospective Exploratory Observational Study" Nutrients 15, no. 12: 2695. https://doi.org/10.3390/nu15122695
APA StyleKoppold, D. A., Kandil, F. I., Güttler, O., Müller, A., Steckhan, N., Meiß, S., Breinlinger, C., Nelle, E., Hartmann, A. M., Jeitler, M., Hanslian, E., Fischer, J. M., Michalsen, A., & Kessler, C. S. (2023). Effects of Prolonged Fasting during Inpatient Multimodal Treatment on Pain and Functional Parameters in Knee and Hip Osteoarthritis: A Prospective Exploratory Observational Study. Nutrients, 15(12), 2695. https://doi.org/10.3390/nu15122695