
A Randomized Controlled Study to Test Front-of-Pack (FOP) Nutrition Labels in the Kingdom of Saudi Arabia
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Online Grocery Store
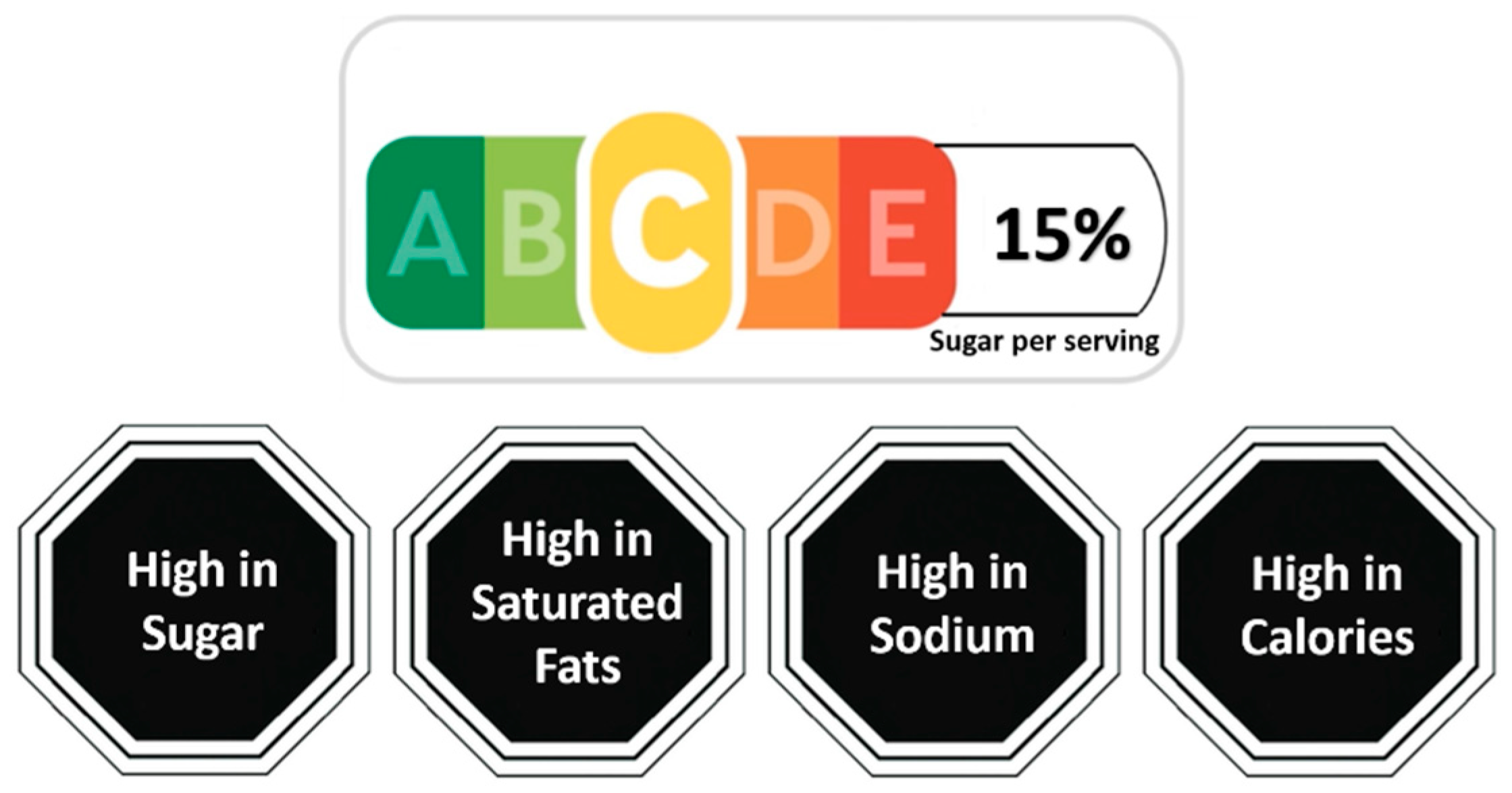
2.2. Experimental Design
2.3. Participants and Procedures
2.4. Statistical Analyses
2.4.1. Outcome Variables
2.4.2. Estimation
3. Results
3.1. Participants
3.2. The Effects of the FOP Labels on Diet Quality for All Food and Beverages
3.3. The Effects of FOP Labels on Diet Quality for Beverages Only
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Cercy, K.; Cohen, A.J.; Hay, S.I.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Fact Sheet: Noncommunicable Diseases. April 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 26 May 2023).
- Global Risks. A Global Risk Network Report: A World Economic Forum Report; in Collaboration with Citi, Marsh & McLennan Companies (MMC), Swiss Re, Wharton School Risk Center, Zurich Financial Services; World Economic Forum: Geneva, Switzerland, 2009. [Google Scholar]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Zhou, M.; Chung, S.T.; Costa, E.; Darcey, V.; et al. Ultra-processed diets cause excess calorie intake and weight gain: An inpatient randomized controlled trial of ad libitum food intake. Cell Metab. 2019, 30, 67–77.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Katan, M.B.; Ascherio, A.; Stampfer, M.J.; Willett, W.C. Trans fatty acids and cardiovascular disease. N. Engl. J Med. 2006, 354, 1601–1613. [Google Scholar] [CrossRef] [Green Version]
- Mente, A.; de Koning, L.; Shannon, H.S.; Anand, S.S. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch. Intern. Med. 2009, 169, 659–669. [Google Scholar] [CrossRef] [Green Version]
- Mendonça, R.D.; Pimenta, A.M.; Gea, A.; de la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Lopes, A.C.S.; Bes-Rastrollo, M. Ultraprocessed food consumption and risk of overweight and obesity: The University of Navarra Follow-Up (SUN) cohort study. Am. J. Clin. Nutr. 2016, 104, 1433–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nseir, W.; Nassar, F.; Assy, N. Soft drinks consumption and nonalcoholic fatty liver disease. World J. Gastroenterol. WJG 2010, 16, 2579. [Google Scholar] [CrossRef] [PubMed]
- Corvalán, C.; Reyes, M.; Garmendia, M.L.; Uauy, R. Structural responses to the obesity and non-communicable diseases epidemic: The Chilean Law of Food Labeling and Advertising. Obes Rev. 2013, 14, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Hawley, K.L.; Roberto, C.A.; Bragg, M.A.; Liu, P.J.; Schwartz, M.B.; Brownell, K.D. The science on front-of-package food labels. Public Health Nutr. 2013, 16, 430–439. [Google Scholar] [CrossRef] [Green Version]
- Department of Health UK. Guide to Creating a Front of Pack (FoP) Nutrition Label for Pre-Packed Products Sold through Retail Outlets. Department of Health, the Food Standards Agency, and Devolved Administrations in Scotland, Northern Ireland and Wales in Collaboration with the British Retail Consortium. 2016. Available online: https://www.gov.uk/government/publications/front-of-pack-nutrition-labelling-guidance (accessed on 26 May 2023).
- Jones, A.; Shahid, M.; Neal, B. Uptake of Australia’s health star rating system. Nutrients 2018, 10, 997. [Google Scholar] [CrossRef] [Green Version]
- Chantal, J.; Hercberg, S.; World Health Organization. Development of a new front-of-pack nutrition label in France: The five-colour Nutri-Score. Public Health Panor. 2017, 3, 712–725. [Google Scholar]
- Reyes, M.; Garmendia, M.L.; Olivares, S.; Aqueveque, C.; Zacarías, I.; Corvalán, C. Development of the Chilean front-of-package food warning label. BMC Public Health 2019, 19, 906. [Google Scholar] [CrossRef] [Green Version]
- Vyth, E.L.; Steenhuis, I.H.; Mallant, S.F.; Mol, Z.L.; Brug, J.; Temminghoff, M.; Feunekes, G.I.; Jansen, L.; Verhagen, H.; Seidell, J.C. A front-of-pack nutrition logo: A quantitative and qualitative process evaluation in The Netherlands. J. Health Commun. 2009, 14, 631–645. [Google Scholar] [CrossRef] [PubMed]
- Golan, E.; Kuchler, F.; Mitchell, L.; Greene, C.; Jessup, A. Economics of food labeling. J. Consum. Policy 2001, 24, 117–184. [Google Scholar] [CrossRef]
- Nikolova, H.D.; Inman, J.J. Healthy choice: The effect of simplified point-of-sale nutritional information on consumer food choice behavior. J. Mark. Res. 2015, 52, 817–835. [Google Scholar] [CrossRef]
- Block, L.G.; Peracchio, L.A. The calcium quandary: How consumers use nutrition labels. J. Public Policy Mark. 2006, 25, 188–196. [Google Scholar] [CrossRef]
- Health Promotion Board. Healthier Choice Symbol Nutrient Guidelines. Singapore: Health Promotion Board, Singapore. 2020. Available online: https://www.hpb.gov.sg/docs/default-source/newsroom/hcs-nutrient-guidelines-revised-april-2020v2.pdf (accessed on 26 May 2023).
- Santé Publique France. Conditions of Use of the Nutri-Score Logo. Contract No.: Version 21. 2020. Available online: https://www.santepubliquefrance.fr/content/download/150258/file/Nutriscore_reglement_usage_EN_310122_VDEF.pdf (accessed on 16 June 2020).
- Talati, Z.; Pettigrew, S.; Dixon, H.; Neal, B.; Ball, K.; Hughes, C. Do health claims and front-of-pack labels lead to a positivity bias in unhealthy foods? Nutrients 2016, 8, 787. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, E.A.; Doble, B.; Ang, F.J.L.; Wong, W.H.M.; van Dam, R.M. A randomized controlled trial testing the effects of a positive front-of-pack label with or without a physical activity equivalent label on food purchases. Appetite 2021, 158, 104997. [Google Scholar] [CrossRef]
- Julia, C.; Hercberg, S. Nutri-Score: Evidence of the effectiveness of the French front-of-pack nutrition label. Ernahr. Umsch. 2017, 64, 181–187. [Google Scholar]
- Finkelstein, E.A.; Ang, F.J.L.; Doble, B.; Wong, W.H.M.; van Dam, R.M. A randomized controlled trial evaluating the relative effectiveness of the multiple traffic light and nutri-score front of package nutrition labels. Nutrients 2019, 11, 2236. [Google Scholar] [CrossRef] [Green Version]
- Kerr, M.A.; McCann, M.T.; Livingstone, M.B.E. Food and the consumer: Could labelling be the answer? Proc. Nutr. Soc. 2015, 74, 158–163. [Google Scholar] [CrossRef] [Green Version]
- Variyam, J.N. Do nutrition labels improve dietary outcomes? Health Econ. 2008, 17, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Helfer, P.; Shultz, T.R. The effects of nutrition labeling on consumer food choice: A psychological experiment and computational model. Ann. N. Y. Acad. Sci. 2014, 1331, 174–185. [Google Scholar] [CrossRef]
- Crockett, R.A.; King, S.E.; Marteau, T.M.; Prevost, A.T.; Bignardi, G.; Roberts, N.W.; Stubbs, B.; Hollands, G.J.; Jebb, S.A. Nutritional labelling for healthier food or non-alcoholic drink purchasing and consumption. Cochrane Database Syst Rev. 2018, 2, CD009315. [Google Scholar]
- Egnell, M.; Talati, Z.; Hercberg, S.; Pettigrew, S.; Julia, C. Objective understanding of front-of-package nutrition labels: An international comparative experimental study across 12 countries. Nutrients 2018, 10, 1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saudi Arabia [Internet]. IHME. 2020. Available online: http://www.healthdata.org/saudi-Arabia (accessed on 26 May 2023).
- Alqunaibet, A.; Herbst, C.H.; El-Saharty, S.; Algwizani, A. Chapter 2: Prevalence and Risk Factors of NCDs in Saudi Arabia. Noncommunicable Diseases in Saudi Arabia: Toward Effective Interventions for Prevention; World Bank Publications: Washington, DC, USA, 2021. [Google Scholar]
- Alsukait, R.; Bleich, S.; Wilde, P.; Singh, G.; Folta, S. Sugary drink excise tax policy process and implementation: Case study from Saudi Arabia. Food Policy 2020, 90, 101789. [Google Scholar] [CrossRef]
- Alsukait, R.; Wilde, P.; Bleich, S.N.; Singh, G.; Folta, S.C. Evaluating Saudi Arabia’s 50% carbonated drink excise tax: Changes in prices and volume sales. Econ. Hum. Biol. 2020, 38, 100868. [Google Scholar] [CrossRef]
- The Government of Saudi Arabia. Policy—KSA National Strategy for Diet and Physical Activity for the Years 2014–2025. 2014. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/SAU_2014_KSA%20National%20Strategy%20for%20Diet%20and%20Physical%20Activity%20for%20the%20Years%20%202014-%202025%20.pdf (accessed on 26 May 2023).
- Bin Sunaid, F.F.; Al-Jawaldeh, A.; Almutairi, M.W.; Alobaid, R.A.; Alfuraih, T.M.; Bensaidan, F.N.; Alragea, A.S.; Almutairi, L.A.; Duhaim, A.F.; Alsaloom, T.A.; et al. Saudi Arabia’s healthy food strategy: Progress & hurdles in the 2030 road. Nutrients 2021, 13, 2130. [Google Scholar] [PubMed]
- Shin, S.; Finkelstein, E.A.; Puri, J. A Randomized Trial to Evaluate the Impact of Singapore’s Forthcoming Nutri-Grade Front-of-Pack Beverage Label on Food and Beverage Purchases. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 18. [Google Scholar] [CrossRef]
- Hoek Mvd, Approved by (Christopher Riker). Nutri-Score Labeling Takes Hold in the Netherlands. United States Department of Agriculture Foreign Agricultural Service; 25 February 2022. Contract No.: NL2022-0014. Available online: https://apps.fas.usda.gov/newgainapi/api/Report/DownloadReportByFileName?fileName=Nutri-Score%20Labeling%20Takes%20Hold%20in%20the%20Netherlands_The%20Hague_Netherlands_NL2022-0014.pdf (accessed on 26 May 2023).
- Ahmed, M.; Dickinson, K.; Vergeer, L.; Mulligan, C.; Franco-Arellano, B.; Julia, C.; L’Abbé, M. Evaluating the Consistency of the French Nutri-Score Front-of-Pack Scoring System with Canadian Dietary Guidelines. Curr. Dev. Nutr. 2020, 4, 4141711. [Google Scholar] [CrossRef]
- Szabo de Edelenyi, F.; Egnell, M.; Galan, P.; Druesne-Pecollo, N.; Hercberg, S.; Julia, C. Ability of the Nutri-Score front-of-pack nutrition label to discriminate the nutritional quality of foods in the German food market and consistency with nutritional recommendations. Arch. Public Health 2019, 77, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Egnell, M.; Crosetto, P.; D’almeida, T.; Kesse-Guyot, E.; Touvier, M.; Ruffieux, B.; Hercberg, S.; Muller, L.; Julia, C. Modelling the impact of different front-of-package nutrition labels on mortality from non-communicable chronic disease. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donat-Vargas, C.; Sandoval-Insausti, H.; Rey-García, J.; Ramón Banegas, J.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Five-color Nutri-Score labeling and mortality risk in a nationwide, population-based cohort in Spain: The Study on Nutrition and Cardiovascular Risk in Spain (ENRICA). Am. J. Clin. Nutr. 2021, 113, 1301–1311. [Google Scholar] [CrossRef]
- Deschasaux, M.; Huybrechts, I.; Julia, C.; Hercberg, S.; Egnell, M.; Srour, B.; Kesse-Guyot, E.; Latino-Martel, P.; Biessy, C.; Casagrande, C.; et al. Association between nutritional profiles of foods underlying Nutri-Score front-of-pack labels and mortality: EPIC cohort study in 10 European countries. BMJ 2020, 370, m3173. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Peñalvo, J.L.; Cudhea, F.; Imamura, F.; Rehm, C.D.; Mozaffarian, D. Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. JAMA 2017, 317, 912–924. [Google Scholar] [CrossRef] [Green Version]
- Micha, R.; Shulkin, M.L.; Penalvo, J.L.; Khatibzadeh, S.; Singh, G.M.; Rao, M.; Fahimi, S.; Powles, J.; Mozaffarian, D. Etiologic effects and optimal intakes of foods and nutrients for risk of cardiovascular diseases and diabetes: Systematic reviews and meta-analyses from the Nutrition and Chronic Diseases Expert Group (NutriCoDE). PLoS ONE 2017, 12, e0175149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NUSMart: An Experimental Online Grocery Store to Promote Healthier Shopping. Available online: https://nusmartbulletin.wordpress.com/ (accessed on 18 June 2023).
- Danube.sa. Available online: https://www.danube.sa/ (accessed on 18 June 2023).
- Julia, C.; Etilé, F.; Hercberg, S. Front-of-pack Nutri-Score labelling in France: An evidence-based policy. Lancet Public Health 2018, 3, e164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, S.; Vanderlee, L.; Acton, R.; Mahamad, S.; Hammond, D. The impact of front-of-package label design on consumer understanding of nutrient amounts. Nutrients 2018, 10, 1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandpur, N.; Mais, L.A.; de Morais Sato, P.; Martins, A.P.B.; Spinillo, C.G.; Rojas, C.F.U.; Garcia, M.T.; Jaime, P.C. Choosing a front-of-package warning label for Brazil: A randomized, controlled comparison of three different label designs. Food Res. Int. 2019, 121, 854–861. [Google Scholar] [CrossRef]
- Koehler, K.; Hersey, J.E.; Wohlgenant, K.C.; Kosa, K.M.; Arsenault, J.E.; Muth, M.K. Policy Research for Front of Package Nutrition Labeling: Environmental Scan and Literature Review; ASPE: Washington, DC, USA, 2011. [Google Scholar]
- Saleh, M. Assessing the consumers’ propensity for online shopping: A demographic perspective. J. Am. Acad. Bus. 2015, 21, 186–194. [Google Scholar]
- Distribution of consumers shopping for groceries online in Saudi Arabia as of 2017, by gender: Statista Research Department. 2018. Available online: https://www.statista.com/statistics/990321/saudi-arabia-share-of-consumers-shopping-for-groceries-online-by-gender/ (accessed on 26 May 2023).
- Crosetto, P.; Lacroix, A.; Muller, L.; Ruffieux, B. Nutritional and economic impact of five alternative front-of-pack nutritional labels: Experimental evidence. Eur. Rev. Agric. Econ. 2020, 47, 785–818. [Google Scholar] [CrossRef]
- Jáuregui, A.; Vargas-Meza, J.; Nieto, C.; Contreras-Manzano, A.; Alejandro, N.Z.; Tolentino-Mayo, L.; Hall, M.G.; Barquera, S. Impact of front-of-pack nutrition labels on consumer purchasing intentions: A randomized experiment in low-and middle-income Mexican adults. BMC Public Health 2020, 20, 463. [Google Scholar] [CrossRef] [PubMed]
- Kiesel, K.; Villas-Boas, S.B. Can information costs affect consumer choice? Nutritional labels in a supermarket experiment. Int. J. Ind. Organ. 2013, 31, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Ikonen, I.; Sotgiu, F.; Aydinli, A.; Verlegh, P.W. Consumer effects of front-of-package nutrition labeling: An interdisciplinary meta-analysis. J. Acad. Mark. Sci. 2020, 48, 360–383. [Google Scholar] [CrossRef] [Green Version]
- Jones, G.; Richardson, M. An objective examination of consumer perception of nutrition information based on healthiness ratings and eye movements. Public Health Nutr. 2007, 10, 238–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Variable | Control Arm | Warning Label Arm | NS Label Arm | Total |
|---|---|---|---|---|
| Age (years), mean SD | 32.4 ± 6.5 | 31.3 ± 7.0 | 31.4 ± 7.0 | 31.7 ± 6.8 |
| Female, (%) | 56 | 41 | 50 | 49 |
| Household Size, mean SD | 4.9 ± 2.0 | 4.5 ± 2.0 | 4.6 ± 2.1 | 4.7 ± 2.0 |
| High educational level (university degree and above), (%) | 86 | 80 | 79 | 82 |
| High household income (monthly income SAR 15,000 and above), (%) | 46 | 45 | 44 | 45 |
| Household with no underlying health condition, (%) | 42 | 41 | 39 | 41 |
| Most Important Drivers of Shopping Behavior (%) | ||||
| Taste | 39 | 37 | 37 | 38 |
| Price | 16 | 19 | 16 | 17 |
| Health | 23 | 22 | 29 | 24 |
| Variety | 14 | 13 | 12 | 13 |
| Convenience | 8 | 9 | 6 | 8 |
| Observations | 214 | 231 | 211 | 656 |
| Control | NS Arm | WL Arm | |
|---|---|---|---|
| Mean (SD) | |||
| Weighted NS points per serving | 32.3 | 34.8 | 32.8 |
| (4.1) | (4.9) | (4.8) | |
| Energy (kcal) per serving | 296.7 | 248.6 | 182.8 |
| (800.7) | (674.9) | (320.7) | |
| Sugar (g) per serving | 7.8 | 5.7 | 7.5 |
| (4.2) | (3.8) | (4.3) | |
| Sodium (mg) per serving | 787.3 | 673.1 | 862.2 |
| (2460.1) | (3123.6) | (5302.7) | |
| Saturated fat (g) per serving | 35.3 | 45.4 | 16.7 |
| (139.0) | (231.8) | (93.6) | |
| Total energy (in 1000 kcal) | 159.2 | 114.6 | 103.6 |
| (376.4) | (283.7) | (240.7) | |
| Total sugar (kg) | 4.5 | 2.9 | 4.0 |
| (4.7) | (2.7) | (3.7) | |
| Total sodium (g) | 726.1 | 306.4 | 573.9 |
| (2905.1) | (1053.1) | (3581.9) | |
| Total saturated fat (kg) | 24.7 | 18.5 | 9.0 |
| (107.1) | (87.8) | (42.2) | |
| Observation | 214 | 211 | 231 |
| Weighted NS Point | Energy (kcal) per Serving | Sugar (g) per Serving | Sodium (mg) per Serving | Saturated Fat (g) per Serving | |
|---|---|---|---|---|---|
| NS | 2.5 *** | −29.5 | −2.1 *** | −120.1 | 6.1 |
| (0.4) | (68.6) | (0.4) | (246.5) | (15.9) | |
| WL | 0.6 | −98.2 * | −0.5 | 28.8 | −24.6 ** |
| (0.4) | (54.7) | (0.4) | (378.2) | (11.8) | |
| NS vs. WL | 1.9 *** | 68.7 | −1.6 *** | −148.9 | 30.7 * |
| (0.5) | (52.0) | (0.4) | (389.5) | (17.4) |
| Total Energy (in 1000 kcal) | Total Sugar (kg) | Total Sodium (g) | Total Saturated Fat (kg) | |
|---|---|---|---|---|
| NS | −31.6 | −1.4 *** | −373.3 * | −7.2 |
| (30.9) | (0.3) | (197.5) | (9.2) | |
| WL | −40.8 | −0.4 | −110.7 | −17.2 ** |
| (27.4) | (0.4) | (287.2) | (8.2) | |
| NS vs. WL | 9.1 | −1.0 *** | −262.6 | 10.0 |
| (25.0) | (0.3) | (228.0) | (7.0) |
| Weighted NS Point | Energy (kcal) per Serving | Sugar (g) per Serving | Sodium (mg) per Serving | Saturated Fat (g) per Serving | |
|---|---|---|---|---|---|
| NS | 2.5 *** | −24.5 *** | −6.3 *** | −3.8 | −0.0 |
| (0.6) | (6.2) | (2.00) | (5.1) | (0.1) | |
| WL | 1.6 *** | −17.9 *** | −5.0 *** | −2.7 | −0.2 * |
| (0.6) | (6.1) | (1.7) | (5.4) | (0.1) | |
| NS vs. WL | 0.9 | −6.7 | −1.3 | −1.2 | 0.2 |
| (0.6) | (5.5) | (1.6) | (5.4) | (0.1) |
| Total Energy (in 1000 kcal) | Total Sugar (kg) | Total Sodium (g) | Total Saturated Fat (kg) | |
|---|---|---|---|---|
| NS | −1.3 | −0.3 | −0.6 | −0.01 |
| (1.0) | (0.2) | (0.7) | (0.01) | |
| WL | −1.2 | −0.3 | −0.5 | −0.01 |
| (1.1) | (0.2) | (0.8) | (0.01) | |
| NS vs. WL | −0.1 | 0.0 | −0.1 | −0.00 |
| (1.0) | (0.2) | (0.7) | (0.01) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.; Alqunaibet, A.M.; Alsukait, R.F.; Alruwaily, A.; Alfawaz, R.A.; Algwizani, A.; Herbst, C.H.; Shekar, M.; Finkelstein, E.A. A Randomized Controlled Study to Test Front-of-Pack (FOP) Nutrition Labels in the Kingdom of Saudi Arabia. Nutrients 2023, 15, 2904. https://doi.org/10.3390/nu15132904
Shin S, Alqunaibet AM, Alsukait RF, Alruwaily A, Alfawaz RA, Algwizani A, Herbst CH, Shekar M, Finkelstein EA. A Randomized Controlled Study to Test Front-of-Pack (FOP) Nutrition Labels in the Kingdom of Saudi Arabia. Nutrients. 2023; 15(13):2904. https://doi.org/10.3390/nu15132904
Chicago/Turabian StyleShin, Soye, Ada Mohammad Alqunaibet, Reem F. Alsukait, Amaal Alruwaily, Rasha Abdulrahman Alfawaz, Abdullah Algwizani, Christopher H. Herbst, Meera Shekar, and Eric A. Finkelstein. 2023. "A Randomized Controlled Study to Test Front-of-Pack (FOP) Nutrition Labels in the Kingdom of Saudi Arabia" Nutrients 15, no. 13: 2904. https://doi.org/10.3390/nu15132904
APA StyleShin, S., Alqunaibet, A. M., Alsukait, R. F., Alruwaily, A., Alfawaz, R. A., Algwizani, A., Herbst, C. H., Shekar, M., & Finkelstein, E. A. (2023). A Randomized Controlled Study to Test Front-of-Pack (FOP) Nutrition Labels in the Kingdom of Saudi Arabia. Nutrients, 15(13), 2904. https://doi.org/10.3390/nu15132904