
The Lived Experience of Young Adult Cancer Survivors after Treatment: A Qualitative Study
 and
and
Abstract
:1. Background
2. Methods
2.1. Ethical Approval
2.2. Research Design and Participants
2.3. Data Collection
2.4. Data Analysis
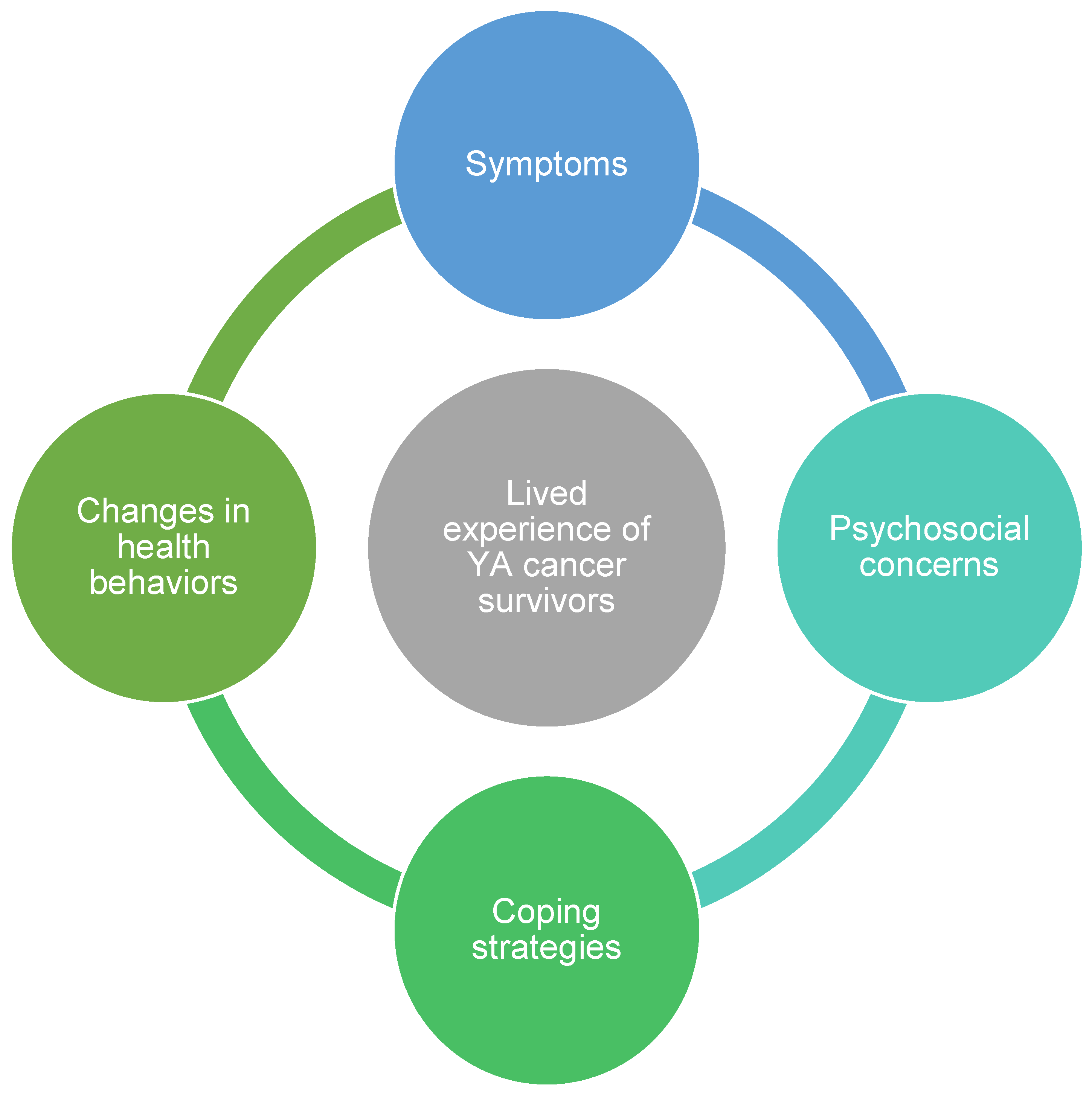
3. Results
4. Symptoms
“Yeah. I would say fatigue... I think I have too much thyroid in my body still. So, I think that’s contributing to things. For my physical appearance, yeah, I’d say my body has changed, and of course I have a scar now.”—1025, female, extended survivor.
“I felt limited physically and hopeless. And sometimes even now today at 26, even though I’m okay, now I have my days when I kinda feel like I’m falling behind because my energy is not like what it used to be, and people will never understand that.”—1015, female, long-term survivor.
4.1. Nutrition
“Yeah, during and after treatment [4 months], I just didn’t have an appetite for anything, and it was really bad when I was in the hospital and had all those medications to take. It was just a lot of stress on my body, and I just hated the idea of eating.”—1022, female, extended survivor.
“Everything just kinda tasted a little funky. It was more like a dampened flavor like, things don’t have as much flavor as I expect them to. And right now, I would say some things that are really creamy come off really waxy, so it’s a little bit of a different texture type thing, too. Just makes eating harder.”—1021, male, extended survivor.
4.2. Physical Activity
“I couldn’t do anything physical because I was at such a high level of pain. And I was exhausted all the time, just so tired it was hard to even think about being physically active.”—1012, female, extended survivor.
“More of the mobility issue than the appearance but, I mean, both kinda bothers me a little bit, just not being able to bend my leg and build that muscle back up. My leg is very atrophied, so it’s a little bit smaller than my other leg and sometimes that bothers me, but I’m just grateful to have my leg.”—1019, female, long-term survivor.
5. Psychosocial Concerns
5.1. Anxiety
“And now, I’m also thinking that maybe the surgery wasn’t as successful as we initially thought, or is it because I had a weakened dose of chemo? So, now I’m in this guessing game, and I also have so many specialists’ appointments coming up to clear up other things that are outstanding, that it’s just a little overwhelming.”—1017, male, extended survivor.
“Just a huge fear of re-occurrence. I will say I am so much more aware of anything I feel. Any symptom that I have could be related to cancer and so I always err on the side of caution, it is just a constant level of stress and anxiety. When I had a period come back, which it has been years, I thought cervical cancer… good or bad, I end up putting myself through more than the average person whenever I have any symptom.”—1002, female, long-term survivor.
5.2. Appearance
“Overall, physical appearance [is my biggest concern], I think. Because it affects everybody differently, but it’s more … mental. You lose your hair. You lose all the features that made you, you, and now you’re somebody else. My jawline. I used to have a jawline, things like that. But now, it’s just a round, pudgy face and it really just wasn’t what I wanted.”—1023, male, extended survivor.
“The biggest setback for me was obviously my hair appearance-wise. Losing my hair was a little challenging… It is much thinner than prior chemo, which I struggle with a little bit. But I have hair. So, that’s amazing.”—1016, female, long-term survivor.
5.3. Fertility
“So, one of the biggest things, and I’m sure you’re aware of this, but chemotherapy can negatively impact your fertility. I haven’t had kids yet. So, that’s a really big concern for me. The doctors tell me that some men do get their fertility back at some point. So, that’s one of my concerns.”—1004, male, long-term survivor.
“I mean, a lot of people don’t tell you. Everyone thinks, well, you’re not gonna be able to have kids, but they don’t tell you you’re gonna be in menopause which affects your fertility—I think you don’t really think about it. You just kind of say, “Oh. Other people don’t have kids.” But, no. You’re in full ovarian failure. You’re going through menopause.”—1013, female, long-term survivor.
5.4. Additional Concerns
“I didn’t want to get out of my house, did not get out of my bed, and, also, after or close to when I was recovering, it was hard for me to find a job. So, financially after, when you’re a young adult with cancer, when you had cancer that happens like you have a hard time finding work again because my current job, when I had that at the time let me go, and I had a hard time for the past four years. And I’m okay now, but it was really difficult.”—1015, female, long-term survivor.
6. Coping Strategies
Social Support
“I have a really good network of friends and family that kept me together. Whenever there was issues, I would focus on other things instead of myself or I would always think there’s somebody out there who’s worse, somebody that doesn’t have what I have. So, I was able to put that in my mind and it always helped.”—1023, male, extended survivor.
“Honestly, I went to Facebook… and I looked for support groups because I would tell my oncologist, and I just felt like they didn’t get it. They would just look at me like I’ve got four eyes, and I’m like, ‘No, this is really concerning to me.’ So, I just looked to Facebook and support groups who understood where I was coming from, and it dramatically helped because I was like, ‘I’m not crazy! You understand me! I’m not crazy!’ So, ‘til this day, I still use them. I’ve met a lot of cool friends there.”—1007, female, long-term survivor.
7. Changes in Nutrition and Physical Activity
“I was a college athlete, so I love weightlifting. I just don’t have that strength fully back yet to be able to do it. So, the most I’ll do is some lower-weight dumbbells or something like that but definitely used to have longer more high-level intensity workouts whereas now it’s more just like a maintenance getting my body moving type of thing. I work out probably like 45 min to an hour a day.”—1010, female, extended survivor.
“I wasn’t really physically active before. I used to walk around campus or things like that, but I never really did anything. I used to go to the gym every now and then. I feel like I’m more active now just because I’m putting in the effort. I do Pilates. I do rowing. I walk my dog 30 min a day, things like that. So, I feel like I’m more active now.”—1003, female, long-term survivor.
8. Discussion
Study Limitations
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scott, A.R.; Stoltzfus, K.C.; Tchelebi, L.T.; Trifiletti, D.M.; Lehrer, E.J.; Rao, P.; Bleyer, A.; Zaorsky, N.G. Trends in Cancer Incidence in US Adolescents and Young Adults, 1973–2015. JAMA Netw. Open 2020, 3, e2027738. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer statistics for adolescents and young adults, 2020. CA Cancer J. Clin. 2020, 70, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Bleyer, A. The adolescent and young adult gap in cancer care and outcome. Curr. Probl. Pediatr. Adolesc. Health Care 2005, 35, 182–217. [Google Scholar] [CrossRef]
- Zebrack, B.J.; Mills, J.; Weitzman, T.S. Health and supportive care needs of young adult cancer patients and survivors. J. Cancer Surviv. 2007, 1, 137–145. [Google Scholar] [CrossRef] [PubMed]
- LaRosa, K.N.; Stern, M.; Bleck, J.; Lynn, C.; Hudson, J.; Reed, D.R.; Quinn, G.P.; Donovan, K.A. Adolescent and Young Adult Patients with Cancer: Perceptions of Care. J. Adolesc. Young Adult Oncol. 2017, 6, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.; Davies, S.; Palmer, S.; Plaster, M. Sex, drugs, and rock ‘n’ roll: Caring for adolescents and young adults with cancer. J. Clin. Oncol. 2010, 28, 4825–4830. [Google Scholar] [CrossRef]
- Tai, E.; Buchanan, N.; Townsend, J.; Fairley, T.; Moore, A.; Richardson, L.C. Health status of adolescent and young adult cancer survivors. Cancer 2012, 118, 4884–4891. [Google Scholar] [CrossRef] [Green Version]
- Patterson, P.; McDonald, F.E.J.; Zebrack, B.; Medlow, S. Emerging Issues among Adolescent and Young Adult Cancer Survivors. Semin. Oncol. Nurs. 2015, 31, 53–59. [Google Scholar] [CrossRef]
- Parsons, H.M.; Harlan, L.C.; Lynch, C.F.; Hamilton, A.S.; Wu, X.C.; Kato, I.; Schwartz, S.; Smith, A.W.; Keel, G.; Keegan, T.H. Impact of Cancer on Work and Education Among Adolescent and Young Adult Cancer Survivors. J. Clin. Oncol. 2012, 30, 2393–2400. [Google Scholar] [CrossRef]
- Kwak, M.; Zebrack, B.J.; Meeske, K.A.; Embry, L.; Aguilar, C.; Block, R.; Hayes-Lattin, B.; Li, Y.; Butler, M.; Cole, S. Trajectories of Psychological Distress in Adolescent and Young Adult Patients With Cancer: A 1-Year Longitudinal Study. J. Clin. Oncol. 2013, 31, 2160–2166. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino, N.M.; Edelstein, K. Psychosocial Challenges and Resource Needs of Young Adult Cancer Survivors: Implications for Program Development. J. Psychosoc. Oncol. 2013, 31, 585–600. [Google Scholar] [CrossRef]
- Quinn, G.P.; Gonçalves, V.; Sehovic, I.; Bowman, M.L.; Reed, D.R. Quality of life in adolescent and young adult cancer patients: A systematic review of the literature. Patient Relat. Outcome Meas. 2015, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Sanford, S.D.; Zhao, F.; Salsman, J.M.; Chang, V.T.; Wagner, L.I.; Fisch, M.J. Symptom burden among young adults with breast or colorectal cancer. Cancer 2014, 120, 2255–2263. [Google Scholar] [CrossRef]
- Zhang, A.; Wang, K.; Zebrack, B.; Tan, C.Y.; Walling, E.; Chugh, R. Psychosocial, behavioral, and supportive interventions for pediatric, adolescent, and young adult cancer survivors: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2021, 160, 103291. [Google Scholar] [CrossRef]
- Belpame, N.; Kars, M.C.; Deslypere, E.; Rober, P.; Van Hecke, A.; Verhaeghe, S. Coping Strategies of Adolescent and Young Adult Survivors of Childhood Cancer: A Qualitative Study. Cancer Nurs. 2021, 44, E395–E403. [Google Scholar] [CrossRef]
- Phillips, F.; Jones, B.L. Understanding the lived experience of Latino adolescent and young adult survivors of childhood cancer. J. Cancer Surviv. 2014, 8, 39–48. [Google Scholar] [CrossRef]
- Newton, K.; Howard, A.F.; Thorne, S.; Kelly, M.T.; Goddard, K. Facing the unknown: Uncertain fertility in young adult survivors of childhood cancer. J. Cancer Surviv. 2021, 15, 54–65. [Google Scholar] [CrossRef]
- Langeveld, N.E.; Stam, H.; Grootenhuis, M.A.; Last, B.F. Quality of life in young adult survivors of childhood cancer. Support. Care Cancer 2002, 10, 579–600. [Google Scholar] [CrossRef]
- Woodward, E.; Jessop, M.; Glaser, A.; Stark, D. Late effects in survivors of teenage and young adult cancer: Does age matter? Ann. Oncol. 2011, 22, 2561–2568. [Google Scholar] [CrossRef]
- Fardell, J.E.; Vetsch, J.; Trahair, T.; Mateos, M.K.; Grootenhuis, M.A.; Touyz, L.M.; Marshall, G.M.; Wakefield, C.E. Health-related quality of life of children on treatment for acute lymphoblastic leukemia: A systematic review. Pediatr. Blood Cancer 2017, 64, e26489. [Google Scholar] [CrossRef]
- Dattilo, T.M.; Olshefski, R.S.; Nahata, L.; Hansen-Moore, J.A.; Gerhardt, C.A.; Lehmann, V. Growing up after childhood cancer: Maturity and life satisfaction in young adulthood. Support. Care Cancer 2021, 29, 6661–6668. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.A.; Papadakos, J.K.; Jones, J.M.; Amin, L.; Chang, E.K.; Korenblum, C.; Mina, D.S.; McCabe, L.; Mitchell, L.; Giuliani, M. Reimagining care for adolescent and young adult cancer programs: Moving with the times. Cancer 2016, 122, 1038–1046. [Google Scholar] [CrossRef] [PubMed]
- Keegan, T.H.; Lichtensztajn, D.Y.; Kato, I.; Kent, E.E.; Wu, X.C.; West, M.M.; Hamilton, A.S.; Zebrack, B.; Bellizzi, K.M.; Smith, A.W.; et al. Unmet adolescent and young adult cancer survivors information and service needs: A population-based cancer registry study. J. Cancer Surviv. 2012, 6, 239–250. [Google Scholar] [CrossRef] [PubMed]
- International Cancer Control Partnership. Survivorship 2023. Available online: https://www.iccp-portal.org/survivorship (accessed on 11 July 2023).
- Nass, S.J.; Beaupin, L.K.; Demark-Wahnefried, W.; Fasciano, K.; Ganz, P.A.; Hayes-Lattin, B.; Hudson, M.M.; Nevidjon, B.; Oeffinger, K.C.; Rechis, R.; et al. Identifying and addressing the needs of adolescents and young adults with cancer: Summary of an Institute of Medicine workshop. Oncologist 2015, 20, 186–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samet, J.M.; Bradley, C.J. Long-Term Cancer Survival: New Insights From Health Professional Cohorts. JNCI Cancer Spectr. 2022, 6, pkac022. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.; Greenwood, M.; Prior, S.; Shearer, T.; Walkem, K.; Young, S.; Bywaters, D.; Walker, K. Purposive sampling: Complex or simple? Research case examples. J. Res. Nurs. 2020, 25, 652–661. [Google Scholar] [CrossRef]
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code Saturation Versus Meaning Saturation: How Many Interviews Are Enough? Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef]
- Anthoine, E.; Moret, L.; Regnault, A.; Sébille, V.; Hardouin, J.B. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Outcomes 2014, 12, 176. [Google Scholar] [CrossRef] [Green Version]
- Thorne, S. The Great Saturation Debate: What the “S Word” Means and Doesn’t Mean in Qualitative Research Reporting; SAGE Publications Sage CA: Los Angeles, CA, USA, 2020; pp. 3–5. [Google Scholar]
- Lewis, A.; Oppenheim, A. Questionnaire Design, Interviewing and Attitude Measurement. J. Community Appl. Soc. Psychol. 1994, 4, 371–372. [Google Scholar] [CrossRef]
- Dedoose Version 9.0. Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data; Sociocultural Research Consultants, LLC: Los Angeles, CA, USA, 2021.
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Larcombe, I.; Mott, M.; Hunt, L. Lifestyle behaviours of young adult survivors of childhood cancer. Br. J. Cancer 2002, 87, 1204–1209. [Google Scholar] [CrossRef]
- Rebholz, C.E.; Rueegg, C.S.; Michel, G.; Ammann, R.A.; von der Weid, N.X.; Kuehni, C.E.; Spycher, B. Clustering of health behaviours in adult survivors of childhood cancer and the general population. Br. J. Cancer 2012, 107, 234–242. [Google Scholar] [CrossRef] [Green Version]
- Coa, K.I.; Smith, K.C.; Klassen, A.C.; Caulfield, L.E.; Helzlsouer, K.; Peairs, K.; Shockney, L. Capitalizing on the “teachable moment” to promote healthy dietary changes among cancer survivors: The perspectives of health care providers. Support. Care Cancer 2015, 23, 679–686. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Peterson, B.; McBride, C.; Lipkus, I.; Clipp, E. Current health behaviors and readiness to pursue life-style changes among men and women diagnosed with early stage prostate and breast carcinomas. Cancer 2000, 88, 674–684. [Google Scholar] [CrossRef]
- Gerhardt, C.A.; Yopp, J.M.; Leininger, L.; Valerius, K.S.; Correll, J.; Vannatta, K.; Noll, R.B. Brief report: Post-traumatic stress during emerging adulthood in survivors of pediatric cancer. J. Pediatr. Psychol. 2007, 32, 1018–1023. [Google Scholar] [CrossRef]
- Hjern, A.; Lindblad, F.; Boman, K.K. Disability in adult survivors of childhood cancer: A Swedish national cohort study. J. Clin. Oncol. 2007, 25, 5262–5266. [Google Scholar] [CrossRef]
- Boydell, K.M.; Stasiulis, E.; Greenberg, M.; Greenberg, C.; Spiegler, B. I’ll show them: The social construction of (in)competence in survivors of childhood brain tumors. J. Pediatr. Oncol. Nurs. 2008, 25, 164–174. [Google Scholar] [CrossRef]
- Bjork, M.; Nordstrom, B.; Wiebe, T.; Hallstrom, I. Returning to a changed ordinary life--families’ lived experience after completing a child’s cancer treatment. Eur. J. Cancer Care 2011, 20, 163–169. [Google Scholar] [CrossRef]

{kind=link}
| Extended Survivors (n = 12) | Long-term Survivors (n = 12) | All Participants (N = 24) | |
|---|---|---|---|
| Age: Mean ± SD (range), years | |||
| At diagnosis | 31.2 ± 6.5 (20–39) | 25.6 ± 4.9 (19–32) | 27.8 ± 6.3 (19–39) |
| At study enrollment | 31.4 ± 6.1 (21–40) | 32.1 ± 5.3 (26–40) | 31.8 ± 5.6 (21–40) |
| Body Mass Index: Mean ± SD [range], kg/m2 | |||
| At diagnosis | 28.2 ± 6.2 (22–43) | 25.7 ± 6.7 (19–41) | 27.0 ± 8.3 (19–43) |
| At study enrollment | 29.7 ± 6.5 (21–43) | 28.8 ± 8.0 (20–44) | 29.2 ± 9.1 (20–44) |
| Female Gender: n (%) | 9 (75) | 11 (92) | 20 (83) |
| Non-Hispanic Ethnicity: n (%) | 10 (83) | 11 (92) | 21 (88) |
| White Race: n (%) | 7 (58) | 6 (50) | 13 (54) |
| Education: n (%) | |||
| Some college | 0 (0) | 5 (42) | 5 (21) |
| College degree | 8 (67) | 4 (33) | 12 (50) |
| Some graduate school | 1 (8) | 1 (8) | 2 (8) |
| Graduate school degree | 3 (25) | 2 (17) | 5 (21) |
| Cancer Diagnosis: n (%) | |||
| Acute lymphoblastic leukemia | 1 (8) | 0 (0) | 1 (4) |
| Acute myeloid leukemia | 1 (8) | 2 (17) | 3 (12) |
| Bladder | 1 (8) | 0 (0) | 1 (4) |
| Breast | 2 (17) | 2 (17) | 4 (16) |
| Colorectal | 1 (8) | 0 (0) | 1 (4) |
| Hodgkin lymphoma | 2 (17) | 2 (17) | 4 (16) |
| Melanoma | 0 (0) | 1 (8) | 1 (4) |
| Non-Hodgkin lymphoma | 1 (8) | 1 (8) | 2 (8) |
| Ovarian | 1 (8) | 0 (0) | 1 (4) |
| Sarcoma | 0 (0) | 2 (17) | 2 (8) |
| Testicular | 0 (0) | 1 (8) | 1 (4) |
| Thyroid | 2 (16) | 1 (8) | 3 (12) |
| Cancer stage: n (%) | |||
| Stage 0 | 2 (17) | 1 (8) | 3 (13) |
| Stage I | 2 (17) | 1 (8) | 3 (13) |
| Stage II | 1 (8) | 2 (17) | 3 (13) |
| Stage III | 2 (17) | 1 (8) | 3 (13) |
| Stage IV | 2 (17) | 2 (17) | 4 (16) |
| No stage; deemed aggressive | 2 (17) | 2 (17) | 4 (16) |
| Prefer not to answer | 1 (8) | 3 (25) | 4 (16) |
| Therapy received: n (%) | |||
| Chemotherapy | 4 (34) | 2 (17) | 6 (25) |
| Surgery | 2 (17) | 2 (17) | 4 (16) |
| Chemotherapy + Radiation | 1 (8) | 1 (8) | 2 (8) |
| Chemotherapy + Surgery | 1 (8) | 1 (8) | 2 (8) |
| Radiation + Surgery | 1 (8) | 0 (0) | 1 (4) |
| Chemotherapy + Immunotherapy | 1 (8) | 0 (0) | 1 (4) |
| Chemotherapy + Immunotherapy + Surgery | 0 (0) | 1 (8) | 1 (4) |
| Chemotherapy + Hormonal + Surgery | 0 (0) | 1 (8) | 1 (4) |
| Chemotherapy + Radiation + Surgery | 0 (0) | 1 (8) | 1 (4) |
| Chemotherapy + Radiation + Immunotherapy + Surgery | 1 (8) | 2 (17) | 3 (13) |
| Prefer not to answer | 1 (8) | 1 (8) | 2 (8) |
| Comorbidities: n (%) | |||
| None | 9 (75) | 8 (67) | 17 (71) |
| Obesity | 2 (17) | 3 (25) | 5 (21) |
| Hypertension | 1 (8) | 0 (0) | 1 (4) |
| Obesity + High Cholesterol | 0 (0) | 1 (8) | 1 (4) |
| Themes | Extended Survivors | Both Groups | Long-Term Survivors |
|---|---|---|---|
| Symptoms | Pain, immobility, medication side effects (e.g., hair loss) | Fatigue, dietary restrictions (e.g., taste alterations, sensitivity to certain foods) | Fear of unknown, life stress (e.g., maintaining long-term relationships), hormonal changes (e.g., early onset menopause) |
| Psychosocial concerns | Acute concerns (e.g., hair loss, scarring), body image (e.g., appearance, weight fluctuations), COVID-19 isolation, medication side-effects | Treatment anxiety, fear of recurrence, feeling self-conscious, impaired quality of life | Chronic concerns (e.g., ability to find and keep a job, fertility concerns, financial burden) |
| Coping strategies | Distraction-based “negative” coping strategies (e.g., snacking, listening to music) | Mindfulness, humor, engaging in social media support groups | Action-based coping “positive” strategies (e.g., seeking social support, physical activity) |
| Changes in health behaviors | Immobility concerns limiting some physical activity and prioritizing healthy eating as a result | Value for the importance of nutrition and physical activity post-treatment | Engaging in physical activity and healthy eating behaviors |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crowder, S.L.; Sauls, R.; Gudenkauf, L.M.; James, C.; Skinner, A.; Reed, D.R.; Stern, M. The Lived Experience of Young Adult Cancer Survivors after Treatment: A Qualitative Study. Nutrients 2023, 15, 3145. https://doi.org/10.3390/nu15143145
Crowder SL, Sauls R, Gudenkauf LM, James C, Skinner A, Reed DR, Stern M. The Lived Experience of Young Adult Cancer Survivors after Treatment: A Qualitative Study. Nutrients. 2023; 15(14):3145. https://doi.org/10.3390/nu15143145
Chicago/Turabian StyleCrowder, Sylvia L., Rachel Sauls, Lisa M. Gudenkauf, Christy James, Amber Skinner, Damon R. Reed, and Marilyn Stern. 2023. "The Lived Experience of Young Adult Cancer Survivors after Treatment: A Qualitative Study" Nutrients 15, no. 14: 3145. https://doi.org/10.3390/nu15143145