

Impact of Homocysteine as a Preconceptional Screening Factor for In Vitro Fertilization and Prevention of Miscarriage with Folic Acid Supplementation Following Frozen-Thawed Embryo Transfer: A Hospital-Based Retrospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects Characteristics and Data Handling
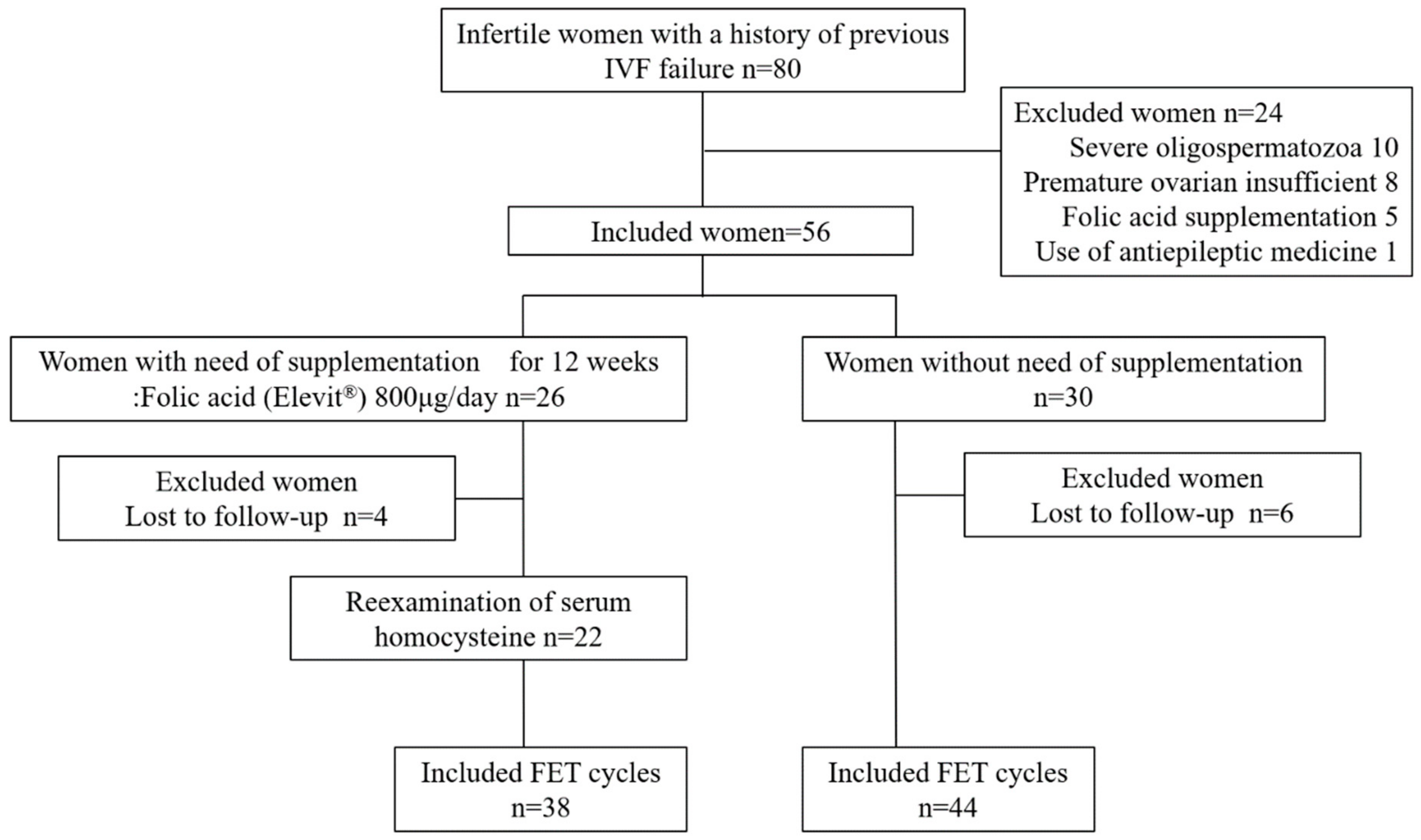
2.2. Prospective Interventional Study of Folic Acid Intake
2.3. Ethical Statement
2.4. Statistical Analyses
3. Results
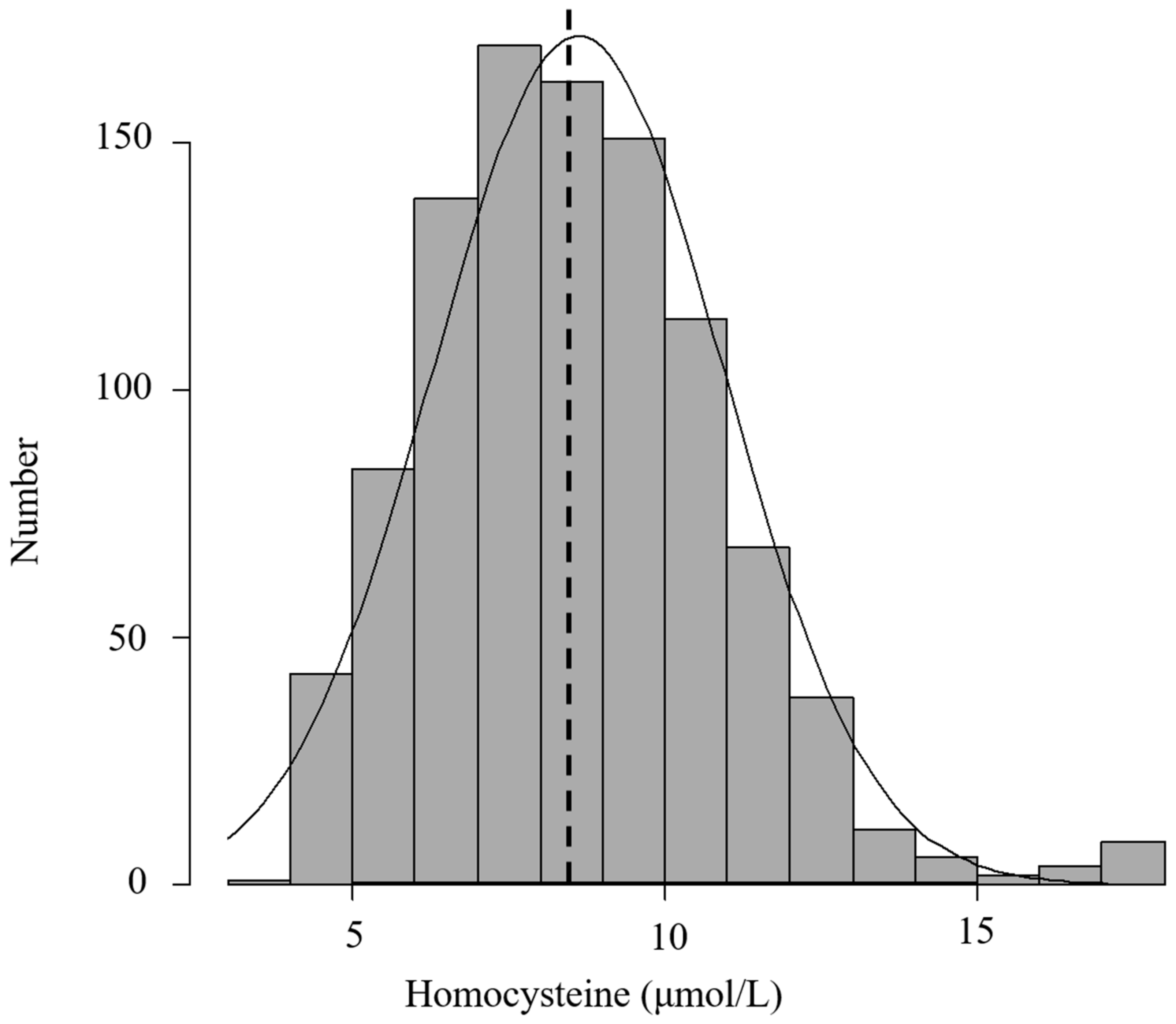
3.1. Baseline Characteristics of the Study Participants
3.2. Association of Homocysteine Status with Reproductive Makers
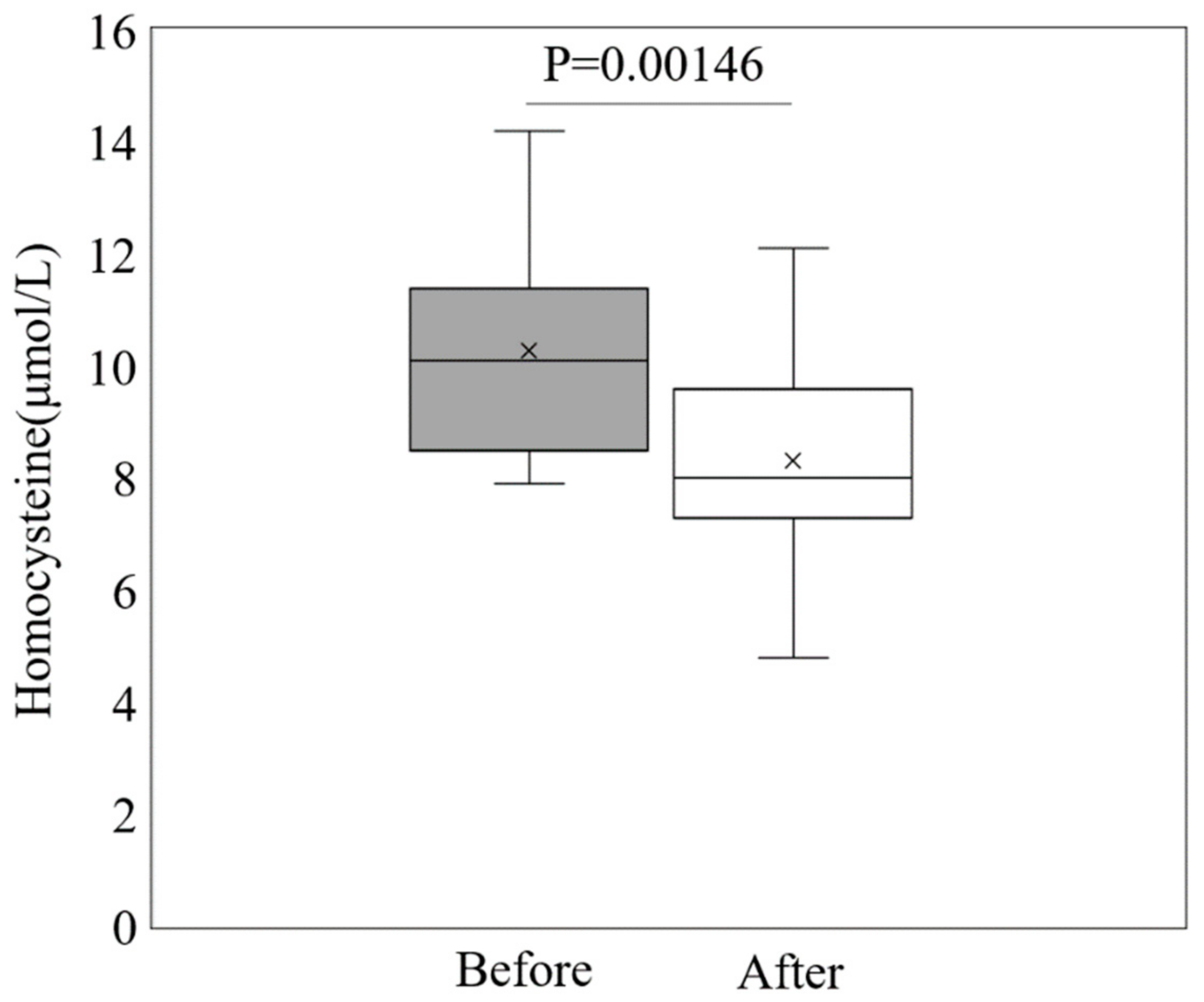
3.3. Impact of Folic Acid Supplementation on Homocysteine Levels and Pregnancy Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Calhaz-Jorge, C.; de Geyter, C.; Kupka, M.S.; de Mouzon, J.; Erb, K.; Mocanu, E.; Motrenko, T.; Scaravelli, G.; Wyns, C.; Goossens, V. Assisted reproductive technology in Europe, 2012: Results generated from European registers by ESHRE. Hum. Reprod. 2016, 31, 1638–1652. [Google Scholar] [CrossRef] [PubMed]
- Mantikou, E.; Youssef, M.A.; van Wely, M.; van der Veen, F.; Al-Inany, H.G.; Repping, S.; Mastenbroek, S. Embryo culture media and IVF/ICSI success rates: A systematic review. Hum. Reprod. Update 2013, 19, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Van den Boogaard, N.M.; Bensdorp, A.J.; Oude Rengerink, K.; Barnhart, K.; Bhattacharya, S.; Custers, I.M.; Coutifaris, C.; Goverde, A.J.; Guzick, D.S.; Hughes, E.C.; et al. Prognostic profiles and the effectiveness of assisted conception: Secondary analyses of individual patient data. Hum. Reprod. Update 2014, 20, 141–151. [Google Scholar] [CrossRef]
- Klonoff-Cohen, H. Female and male lifestyle habits and IVF: What is known and unknown. Hum. Reprod. Update 2005, 11, 180–204. [Google Scholar] [CrossRef]
- Hornstein, M.D. Lifestyle and IVF outcomes. Reprod. Sci. 2016, 23, 1626–1629. [Google Scholar] [CrossRef] [PubMed]
- Cueto, H.T.; Riis, A.H.; Hatch, E.E.; Wise, L.A.; Rothman, K.J.; Sørensen, H.T.; Mikkelsen, E.M. Folic acid supplementation and fecundability: A Danish prospective cohort study. Eur. J. Clin. Nutr. 2016, 70, 66–71. [Google Scholar] [CrossRef]
- Braga, D.P.A.F.; Halpern, G.; Setti, A.S.; Figueira, R.C.S.; Iaconelli, A., Jr.; Borges, E., Jr. The impact of food intake and social habits on embryo quality and the likelihood of blastocyst formation. Reprod. Biomed. Online 2015, 31, 30–38. [Google Scholar] [CrossRef]
- Firns, S.; Cruzat, V.F.; Keane, K.N.; Joesbury, K.A.; Lee, A.H.; Newsholme, P.; Yovich, J.L. The effect of cigarette smoking, alcohol consumption and fruit and vegetable consumption on IVF outcomes: A review and presentation of original data. Reprod. Biol. Endocrinol. 2015, 13, 134. [Google Scholar] [CrossRef]
- Ebisch, I.M.W.; Thomas, C.M.G.; Peters, W.H.M.; Braat, D.D.M.; Steegers-Theunissen, R.P.M. The importance of folate, zinc and antioxidants in the pathogenesis and prevention of subfertility. Hum. Reprod. Update 2007, 13, 163–174. [Google Scholar] [CrossRef]
- Wald, N.J.; Morris, J.K.; Blakemore, C. Public health failure in the prevention of neural tube defects: Time to abandon the tolerable upper intake level of folate. Public Health Rev. 2018, 39, 2. [Google Scholar] [CrossRef]
- Van Gool, J.D.; Hirche, H.; Lax, H.; De Schaepdrijver, L. Folic acid and primary prevention of neural tube defects: A review. Reprod. Toxicol. 2018, 80, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wang, Y.; Xin, X.; Zhang, Y.; Liu, D.; Peng, Z.; He, Y.; Xu, J.; Ma, X. Effect of folic acid supplementation on preterm delivery and small for gestational age births: A systematic review and meta-analysis. Reprod. Toxicol. 2017, 67, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.; Lopes, C.; Pinto, E. Folate and folic acid in the periconceptional period: Recommendations from official health organizations in thirty-six countries worldwide and WHO. Public Health Nutr. 2016, 19, 176–189. [Google Scholar] [CrossRef] [PubMed]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W.; García, F.A.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; Landefeld, C.S. Folic acid supplementation for the prevention of neural tube defects: US Preventive Services Task Force recommendation statement. JAMA 2017, 317, 183–189. [Google Scholar] [PubMed]
- Kancherla, V.; Botto, L.D.; Rowe, L.A.; Shlobin, N.A.; Caceres, A.; Arynchyna-Smith, A.; Zimmerman, K.; Blount, J.; Kibruyisfaw, Z.; Ghotme, K.A.; et al. Preventing birth defects, saving lives, and promoting health equity: An urgent call to action for universal mandatory food fortification with folic acid. Lancet Glob. Health 2022, 10, e1053–e1057. [Google Scholar] [CrossRef]
- Ishikawa, T.; Obara, T.; Nishigori, H.; Nishigori, T.; Metoki, H.; Ishikuro, M.; Tatsuta, N.; Mizuno, S.; Sakurai, K.; Nishijima, I.; et al. Update on the prevalence and determinants of folic acid use in Japan evaluated with 91,538 pregnant women: The Japan Environment and Children’s Study. J. Matern.-Fetal Neonatal Med. 2020, 33, 427–436. [Google Scholar] [CrossRef]
- Fowler, B. Homocysteine: Overview of biochemistry, molecular biology, and role in disease processes. In Seminars in Vascular Medicine; Thieme Medical Publishers, Inc.: New York, NY, USA, 2005; pp. 77–86. [Google Scholar]
- Steegers-Theunissen, R.P.M.; Boers, G.J.; Blom, H.; Trijbels, F.M.; Eskes, T.A.B. Hyperhomocysteinaemia and recurrent spontaneous abortion or abruptio placentae. Lancet 1992, 339, 1122–1123. [Google Scholar] [CrossRef]
- Botto, L.D.; Olney, R.S.; Erickson, J.D. Vitamin supplements and the risk for congenital anomalies other than neural tube defects. Am. J. Med. Genet. Part C Semin. Med. Genet. 2004, 125C, 12–21. [Google Scholar] [CrossRef]
- Cordero, A.M.; Crider, K.S.; Rogers, L.M.; Cannon, M.J.; Berry, R.J. Optimal serum and red blood cell folate concentrations in women of reproductive age for prevention of neural tube defects: World Health Organization guidelines. Morb. Mortal. Wkly. Rep. 2015, 64, 421. [Google Scholar]
- Boxmeer, J.C.; Steegers-Theunissen, R.P.M.; Lindemans, J.; Wildhagen, M.F.; Martini, E.; Steegers, E.A.P.; Macklon, N.S. Homocysteine metabolism in the pre-ovulatory follicle during ovarian stimulation. Hum. Reprod. 2008, 23, 2570–2576. [Google Scholar] [CrossRef]
- Stanger, O.; Weger, M. Interactions of homocysteine, nitric oxide, folate and radicals in the progressively damaged endothelium. Clin. Chem. Lab. Med. 2003, 41, 1444–1454. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.-L.; Kuo, T.-L.; Lee, Y.-T. Effects of methionine-induced hyperhomocysteinemia on endothelium-dependent vasodilation and oxidative status in healthy adults. Circulation 2000, 101, 485–490. [Google Scholar] [CrossRef]
- Vanaerts, L.A.G.J.M.; Blom, H.J.; Deabreu, R.A.; Trijbels, F.J.M.; Eskes, T.K.A.B.; Peereboom-Stegeman, J.H.J.C.; Noordhoek, J. Prevention of neural tube defects by and toxicity of L-homocysteine in cultured postimplantation rat embryos. Teratology 1994, 50, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Haggarty, P.; McCallum, H.; McBain, H.; Andrews, K.; Duthie, S.; McNeill, G.; Templeton, A.; Haites, N.; Campbell, D.; Bhattacharya, S. Effect of B vitamins and genetics on success of in-vitro fertilisation: Prospective cohort study. Lancet 2006, 367, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S.; Kahn, S.R.; Rozen, R.; Evans, R.; Platt, R.W.; Chen, M.F.; Goulet, L.; Séguin, L.; Dassa, C.; Lydon, J.; et al. Vasculopathic and thrombophilic risk factors for spontaneous preterm birth. Int. J. Epidemiol. 2009, 38, 715–723. [Google Scholar] [CrossRef]
- Boyama, B.A.; Cepni, I.; Imamoglu, M.; Oncul, M.; Tuten, A.; Yuksel, M.A.; Kervancioglu, M.E.; Kaleli, S.; Ocal, P. Homocysteine in embryo culture media as a predictor of pregnancy outcome in assisted reproductive technology. Gynecol. Endocrinol. 2016, 32, 193–195. [Google Scholar] [CrossRef]
- Ocal, P.; Ersoylu, B.; Cepni, I.; Guralp, O.; Atakul, N.; Irez, T.; Idil, M. The association between homocysteine in the follicular fluid with embryo quality and pregnancy rate in assisted reproductive techniques. J. Assist. Reprod. Genet. 2012, 29, 299–304. [Google Scholar] [CrossRef]
- Murto, T.; Kallak, T.K.; Hoas, A.; Altmäe, S.; Salumets, A.; Nilsson, T.K.; Skoog Svanberg, A.; Wånggren, K.; Yngve, A.; Stavreus-Evers, A. Folic acid supplementation and methylenetetrahydrofolate reductase (MTHFR) gene variations in relation to in vitro fertilization pregnancy outcome. Acta Obstet. Gynecol. Scand. 2015, 94, 65–71. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Chiu, Y.H.; Williams, P.L.; Ford, J.B.; Toth, T.L.; Hauser, R.; Chavarro, J.E. Association between serum folate and vitamin B-12 and outcomes of assisted reproductive technologies. Am. J. Clin. Nutr. 2015, 102, 943–950. [Google Scholar] [CrossRef]
- Baggott, J.E.; Morgan, S.L.; Ha, T.; Vaughn, W.H.; Hine, R.J. Inhibition of folate-dependent enzymes by non-steroidal anti-inflammatory drugs. Biochem. J. 1992, 282, 197–202. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Yücel, B.; Kelekci, S.; Demirel, E. Decline in ovarian reserve may be an undiagnosed reason for unexplained infertility: A cohort study. Arch. Med. Sci. 2018, 14, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Demir, B.; Guven, S.; Guven, E.S.; Atamer, Y.; Gul, T. Serum IL-6 level may have role in the pathophysiology of unexplained infertility. Am. J. Reprod. Immunol. 2009, 62, 261–267. [Google Scholar] [CrossRef]
- Liu, L.; Lin, Z.; Lin, P.; Jiang, Z. Association between serum homocysteine level and unexplained infertility in in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI): A retrospective, hospital-based, case-control study. J. Clin. Lab. Anal. 2020, 34, e23167. [Google Scholar] [CrossRef]
- Altmäe, S.; Stavreus-Evers, A.; Ruiz, J.R.; Laanpere, M.; Syvänen, T.; Yngve, A.; Salumets, A.; Nilsson, T.K. Variations in folate pathway genes are associated with unexplained female infertility. Fertil. Steril. 2010, 94, 130–137. [Google Scholar] [CrossRef]
- Berker, B.; Kaya, C.; Aytac, R.; Satiroglu, H. Homocysteine concentrations in follicular fluid are associated with poor oocyte and embryo qualities in polycystic ovary syndrome patients undergoing assisted reproduction. Hum. Reprod. 2009, 24, 2293–2302. [Google Scholar] [CrossRef]
- Oyawoye, O.; Abdel Gadir, A.; Garner, A.; Constantinovici, N.; Perrett, C.; Hardiman, P. Antioxidants and reactive oxygen species in follicular fluid of women undergoing IVF: Relationship to outcome. Hum. Reprod. 2003, 18, 2270–2274. [Google Scholar] [CrossRef]
- Wang, H.; Han, A.; Jiang, S.; Cao, D.; Jiang, Y.; Sun, L.; Zou, N.; Tao, S.; Xue, X.; Shao, X.; et al. Homocysteine Level Related to Age Is Associated With Embryo Quality in Women Who Had IVF With Diminished Ovarian Reserve. Front. Reprod. Health 2022, 4, 886277. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.K.; Ye, C.; Swaminathan, B.; Hanley, A.J.; Connelly, P.W.; Sermer, M.; Zinman, B.; Retnakaran, R. The persistence of maternal vitamin D deficiency and insufficiency during pregnancy and lactation irrespective of season and supplementation. Clin. Endocrinol. 2016, 84, 680–686. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Van Schoor, N.; Lips, P. Worldwide vitamin D status. Vitam. D 2018, 2, 15–40. [Google Scholar] [CrossRef]
- Heyden, E.; Wimalawansa, S. Vitamin D: Effects on human reproduction, pregnancy, and fetal well-being. J. Steroid Biochem. Mol. Biol. 2018, 180, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Kiely, M.E.; Wagner, C.; Roth, D. Vitamin D in pregnancy: Where we are and where we should go. J. Steroid Biochem. Mol. Biol. 2020, 201, 105669. [Google Scholar] [CrossRef]
- Dabrowski, F.A.; Grzechocinska, B.; Wielgos, M. The Role of Vitamin D in Reproductive Health—A Trojan Horse or the Golden Fleece? Nutrients 2015, 7, 4139–4153. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, D. Recurrent pregnancy loss in patients with thyroid dysfunction. Indian J. Endocrinol. Metab. 2012, 16, S350. [Google Scholar] [CrossRef]
- Li, N.; Wu, H.M.; Hang, F.; Zhang, Y.S.; Li, M.J. Women with recurrent spontaneous abortion have decreased 25(OH) vitamin D and VDR at the fetal-maternal interface. Braz. J. Med. Biol. Res. 2017, 50, e6527. [Google Scholar] [CrossRef]
- Ota, K.; Dambaeva, S.; Han, A.-R.; Beaman, K.; Gilman-Sachs, A.; Kwak-Kim, J. Vitamin D deficiency may be a risk factor for recurrent pregnancy losses by increasing cellular immunity and autoimmunity. Hum. Reprod. 2013, 29, 208–219. [Google Scholar] [CrossRef]
- Ota, K.; Dambaeva, S.; Kim, M.W.I.; Han, A.R.; Fukui, A.; Gilman-Sachs, A.; Beaman, K.; Kwak-Kim, J. 1,25-Dihydroxy-vitamin D3 regulates NK-cell cytotoxicity, cytokine secretion, and degranulation in women with recurrent pregnancy losses. Eur. J. Immunol. 2015, 45, 3188–3199. [Google Scholar] [CrossRef]
- Kwak-Kim, J.; Skariah, A.; Wu, L.; Salazar, D.; Sung, N.; Ota, K. Humoral and cellular autoimmunity in women with recurrent pregnancy losses and repeated implantation failures: A possible role of vitamin D. Autoimmun. Rev. 2016, 15, 943–947. [Google Scholar] [CrossRef]
- Abedi, P.; Mohaghegh, Z.; Afshary, P.; Latifi, M. The relationship of serum vitamin D with pre-eclampsia in the Iranian women. Matern. Child Nutr. 2014, 10, 206–212. [Google Scholar] [CrossRef]
- Kriebitzsch, C.; Verlinden, L.; Eelen, G.; van Schoor, N.M.; Swart, K.; Lips, P.; Meyer, M.B.; Pike, J.W.; Boonen, S.; Carlberg, C. 1,25-dihydroxyvitamin D3 influences cellular homocysteine levels in murine preosteoblastic MC3T3-E1 cells by direct regulation of cystathionine β-synthase. J. Bone Miner. Res. 2011, 26, 2991–3000. [Google Scholar] [CrossRef]
- Amer, M.; Qayyum, R. The relationship between 25-hydroxyvitamin D and homocysteine in asymptomatic adults. J. Clin. Endocrinol. Metab. 2014, 99, 633–638. [Google Scholar] [CrossRef]
- Ota, K.; Takahashi, T.; Han, A.; Damvaeba, S.; Mizunuma, H.; Kwak-Kim, J. Effects of MTHFR C677T polymorphism on vitamin D, homocysteine and natural killer cell cytotoxicity in women with recurrent pregnancy losses. Hum. Reprod. 2020, 35, 1276–1287. [Google Scholar] [CrossRef] [PubMed]
- Al-Bayyari, N.; Al-Zeidaneen, S.; Hamadneh, J. Vitamin D3 prevents cardiovascular diseases by lowering serum total homocysteine concentrations in overweight reproductive women: A randomized, placebo-controlled clinical trial. Nutr. Res. 2018, 59, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Kaye, A.D.; Jeha, G.M.; Pham, A.D.; Fuller, M.C.; Lerner, Z.I.; Sibley, G.T.; Cornett, E.M.; Urits, I.; Viswanath, O.; Kevil, C.G. Folic acid supplementation in patients with elevated homocysteine levels. Adv. Ther. 2020, 37, 4149–4164. [Google Scholar] [CrossRef]
- Kalhan, S.C. One carbon metabolism in pregnancy: Impact on maternal, fetal and neonatal health. Mol. Cell. Endocrinol. 2016, 435, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, M.; Habeebullah, S.; Sridhar, M.G. Revisiting the role of first trimester homocysteine as an index of maternal and fetal outcome. J. Pregnancy 2014, 2014, 123024. [Google Scholar] [CrossRef]
- Dodds, L.; Fell, D.B.; Dooley, K.C.; Armson, B.A.; Allen, A.C.; Nassar, B.A.; Perkins, S.; Joseph, K.S. Effect of homocysteine concentration in early pregnancy on gestational hypertensive disorders and other pregnancy outcomes. Clin. Chem. 2008, 54, 326–334. [Google Scholar] [CrossRef]
- Chakraborty, P.; Goswami, S.K.; Rajani, S.; Sharma, S.; Kabir, S.N.; Chakravarty, B.; Jana, K. Recurrent Pregnancy Loss in Polycystic Ovary Syndrome: Role of Hyperhomocysteinemia and Insulin Resistance. PLoS ONE 2013, 8, e64446. [Google Scholar] [CrossRef]
- Liakishev, A. Homocysteine lowering with folic acid and B vitamins in vascular disease. Kardiologiia 2006, 46, 70. [Google Scholar]
- Gaskins, A.J.; Rich-Edwards, J.W.; Hauser, R.; Williams, P.L.; Gillman, M.W.; Ginsburg, E.S.; Missmer, S.A.; Chavarro, J.E. Maternal prepregnancy folate intake and risk of spontaneous abortion and stillbirth. Obs. Gynecol. 2014, 124, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Pacchiarotti, A.; Mohamed, M.A.; Micara, G.; Linari, A.; Tranquilli, D.; Espinola, S.B.; Aragona, C. The possible role of hyperhomocysteinemia on IVF outcome. J. Assist. Reprod. Genet. 2007, 24, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Tian, X.; Liu, H.; Wang, J.; Wang, F. Homocysteine increases uterine artery blood flow resistance in women with pregnancy loss. J. Gynecol. Obstet. Hum. Reprod. 2023, 52, 102533. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.; Fei, Y.; Li, J.; Shi, Y.; Yang, X. A Novel Review of Homocysteine and Pregnancy Complications. BioMed Res. Int. 2021, 2021, 6652231. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | 1060 |
| Age(y) | 36.3 ± 4.4 |
| Gravity | 0.48 ± 0.8 |
| Parity | 0.16 ± 0.4 |
| Miscarriage | 0.32 ± 0.6 |
| BMI (kg/m2) | 21.6 ± 5.4 |
| Type of infertility | |
| Uterine factor | 14.9% (158) |
| Fallopian tube factor | 24.0% (255) |
| Ovulation factor | 15.8% (164) |
| PCOS | 6.1% (65) |
| Cervical factor | 9.5% (101) |
| Endometriosis | 14.8% (157) |
| Male factor | 32.0% (339) |
| unexplained | 29.8% (316) |
| Life style | |
| Smoking | 2.3% (24) |
| Alcohol | 3.1% (33) |
| Exercise | 6.4% (68) |
| Basal FSH (IU/mL) | 8.0 ± 3.1 |
| Basal LH(IU/mL) | 5.7 ± 2.6 |
| Basal E2 (pg/mL) | 43.5 ± 44.5 |
| AMH (ng/L) | 3.12 ± 3.0 |
| 25(OH) vitamin D (ng/mL) | 14.5 ± 5.8 |
| Serum Homocysteine level (μmol/L) | 8.6 ± 2.3 |
| Previous No. of IVF/ICSI failure | 1.9 ± 1.5 |
| Previous No. of ET failure | 0.6 ± 1.1 |
| Total gonadotropin dose used (IU/L) | 1647.2 ± 619.8 |
| Endometrial thickness on hCG day (mm) | 10.1 ± 2.8 |
| E2 level on hCG day(pmol/L) | 2042.6 ± 1386.2 |
| Fertilization | |
| IVF | 43.9% (465) |
| ICSI | 42.7% (453) |
| Split | 10.1% (107) |
| Ovulation regimens | |
| GnRH-agonist long protocol | 1.0% (11) |
| GnRH-agonist short protocol | 0.6% (7) |
| GnRH-antagonist | 72.2% (765) |
| Moderate stimulation | 8.5% (90) |
| PPOS | 17.6% (187) |
| Total number of oocytes retrieved | 7.82 ± 5.9 |
| No. of M-II oocytes | 6.1 ± 4.8 |
| MII rate | 81.2% |
| Fertilization rate | 74.0% |
| No. of high-quality blastocyst | 1.8 ± 2.3 |
| High quality blastocyst rate | 35.8% |
| Quartile of Homocysteine Level, μmol/L | |||||
|---|---|---|---|---|---|
| Q1 (<7.0) | Q2 (≤7.0–8.5<) | Q3 (≤8.5–10.1<) | Q4 (≥10.1) | p | |
| AMH | 3.27 ± 3.1 | 3.52 ± 3.3 | 2.82 ± 2.5 * | 3.13 ± 2.9 | 0.05 |
| Basal FSH | 7.76 ± 3.0 | 8.05 ± 3.1 | 7.90 ± 3.3 | 8.41 ± 3.2 | 0.11 |
| Basal LH | 5.62 ± 2.8 | 5.52 ± 2.5 | 5.52 ± 2.5 | 5.93 ± 2.8 | 0.34 |
| Basal E2 | 39.8 ± 28.5 | 37.9 ± 21.1 | 47.1 ± 77.2 | 44.0 ± 23.0 | 0.09 |
| 25(OH)VD | 16.3 ± 5.7 ** | 14.1 ± 6.0 | 14.0 ± 6.1 | 13.2 ± 5.2 | <0.001 |
| Previous No. of IVF failure | 1.7 ± 1.2 | 1.9 ± 1.5 | 1.9 ± 1.2 | 2.3 ± 2.0 | <0.001 |
| Previous No. of ET failure | 0.6 ± 1.1 | 0.5 ± 1.1 | 0.7 ± 1.2 | 0.48 ± 1.1 | 0.21 |
| E2 on hCG trigger | 2232.3 ± 1505.8 | 2008.4 ± 1396.1 | 1925.0 ± 1386.0 | 2004.5 ± 1233.0 | 0.07 |
| Total FSH/HMG amount | 1685.2 ± 588.4 | 1604.7 ± 587.7 | 1675.5 ± 712.4 | 1623.9 ± 580.7 | 0.37 |
| No. of oocytes retrieved | 8.1 ± 6.3 | 7.6 ± 5.6 | 7.6 ± 5.9 | 8.0 ± 6.0 | 0.68 |
| No. of MII | 6.4 ± 5.3 | 5.9 ± 4.4 | 6.0 ± 5.0 | 6.2 ± 4.6 | 0.68 |
| MII rate (%) | 80.9 ± 21.3 | 81.8 ± 20.4 | 82.2 ± 22.0 | 79.9 ± 23.5 | 0.62 |
| Fertilization rate (%) | 75.6 ± 26.4 | 72.7 ± 27.4 | 76.8 ± 24.0 | 70.7 ± 26.1 *** | 0.03 |
| No. of Blastocyst | 1.8 ± 2.5 | 1.8 ± 2.3 | 1.7 ± 2.1 | 1.9 ± 2.2 | 0.86 |
| High-quality blastocyst rate (%) | 34.9 ± 32.2 | 35.5 ± 32.9 | 36.5 ± 33.4 | 36.2 ± 31.0 | 0.95 |
| Folic Acid (n = 22) | No Intervention (n = 24) | p Value | |
|---|---|---|---|
| Age(y) | 34.2 ± 3.0 | 35.0 ± 4.3 | 0.56 |
| BMI | 21.8 (18.9–23.2) | 21.6 (19.6–24.0) | 0.67 |
| Gravity | 0 (0–0) | 0 (0–1) | 0.18 |
| Parity | 0 (0–0) | 0 (0–0) | 0.64 |
| Miscarriage | 0 (0–0) | 0 (0–1) | 0.24 |
| Basal FSH (IU/mL) | 6.4 ± 1.9 | 7.2 ± 2.3 | 0.26 |
| Basal LH (IU/mL) | 5.0 ± 2.1 | 5.7 ± 2.6 | 0.34 |
| Basal E2 (pg/ml) | 38.0 (25.0–51.0) | 39.0 (25.0–50.3) | 0.85 |
| 25(OH)vitamin (ng/mL) | 10.8 ± 5.0 | 14.5 ± 4.6 | 0.01 |
| AMH (ng/mL) | 2.45 (1.34–4.95) | 2.80 (1.47–4.67) | 0.10 |
| Homocysteine (μmol/L) | 10.1 (8.6–11.4) | 8.6 (7.8–9.6) | 0.01 |
| Folic Acid (n = 22, 38 FET cycles) | No Supplementation (n = 24, 44 FET Cycles) | 95% Confident Interval | p Value | ||
|---|---|---|---|---|---|
| Low | High | ||||
| Clinical pregnancy | 16 (42.1) | 10 (22.7) | 0.15 | 1.25 | 0.97 |
| Miscarriage | 5 (31.3) | 7 (70.0) | 0.02 | 1.20 | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogawa, S.; Ota, K.; Takahashi, T.; Yoshida, H. Impact of Homocysteine as a Preconceptional Screening Factor for In Vitro Fertilization and Prevention of Miscarriage with Folic Acid Supplementation Following Frozen-Thawed Embryo Transfer: A Hospital-Based Retrospective Cohort Study. Nutrients 2023, 15, 3730. https://doi.org/10.3390/nu15173730
Ogawa S, Ota K, Takahashi T, Yoshida H. Impact of Homocysteine as a Preconceptional Screening Factor for In Vitro Fertilization and Prevention of Miscarriage with Folic Acid Supplementation Following Frozen-Thawed Embryo Transfer: A Hospital-Based Retrospective Cohort Study. Nutrients. 2023; 15(17):3730. https://doi.org/10.3390/nu15173730
Chicago/Turabian StyleOgawa, Seiji, Kuniaki Ota, Toshifumi Takahashi, and Hiroaki Yoshida. 2023. "Impact of Homocysteine as a Preconceptional Screening Factor for In Vitro Fertilization and Prevention of Miscarriage with Folic Acid Supplementation Following Frozen-Thawed Embryo Transfer: A Hospital-Based Retrospective Cohort Study" Nutrients 15, no. 17: 3730. https://doi.org/10.3390/nu15173730