
Efficacy of Boswellia serrata Extract and/or an Omega-3-Based Product for Improving Pain and Function in People Older Than 40 Years with Persistent Knee Pain: A Randomized Double-Blind Controlled Clinical Trial
 ,
,  ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Intervention and Study Procedures
2.3. Study Variables
2.4. Statistical Analysis
3. Results
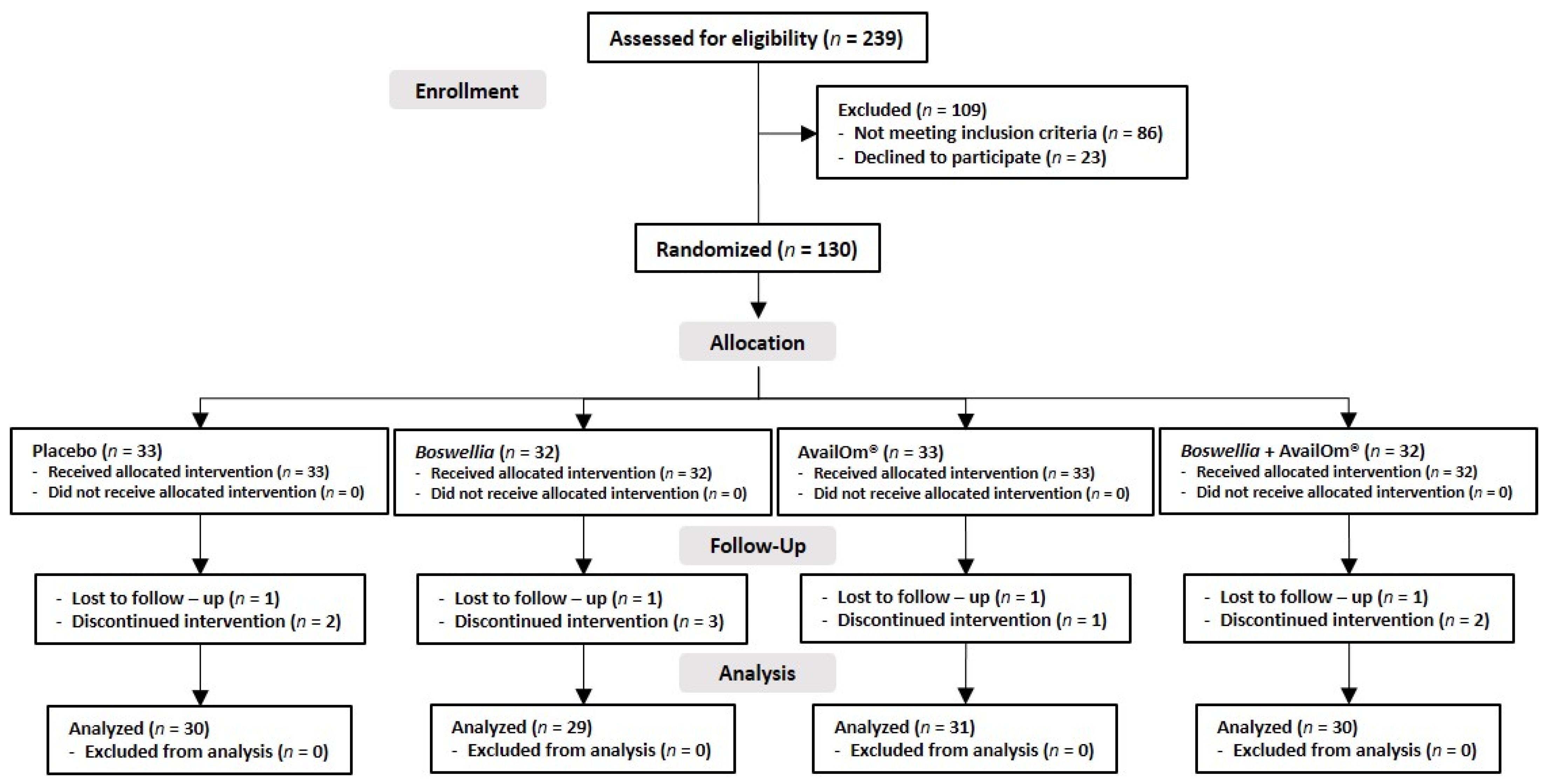
3.1. Participants
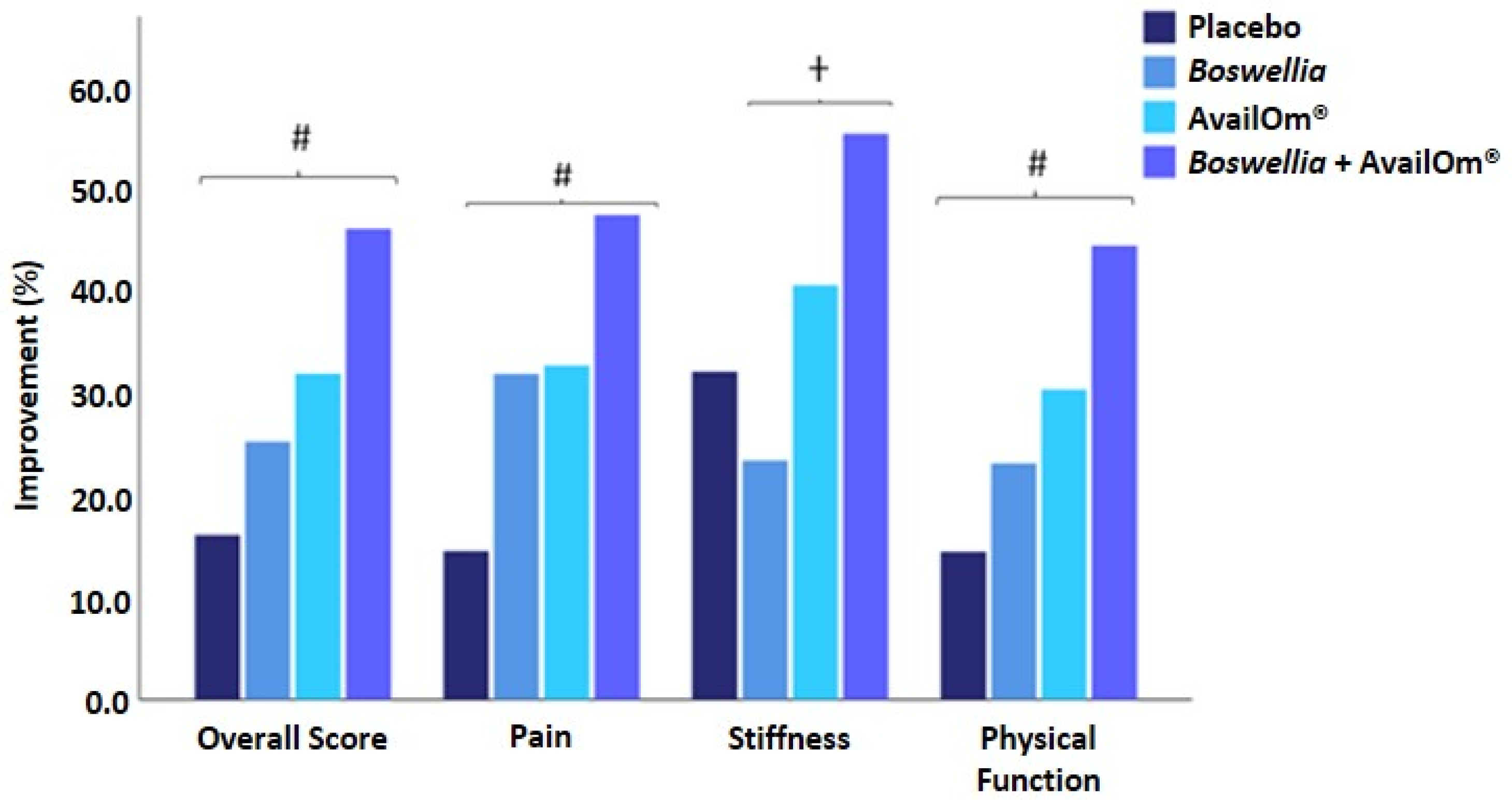
3.2. Quality of Life Assessed by the WOMAC Index
3.3. Pain Intensity
3.3.1. Initial and Final VAS Scores
3.3.2. Weekly VAS Scores
3.4. Time up and Go (TUG) Test
3.5. Muscle Strength: Isokinetic and Isometric Dynamometry
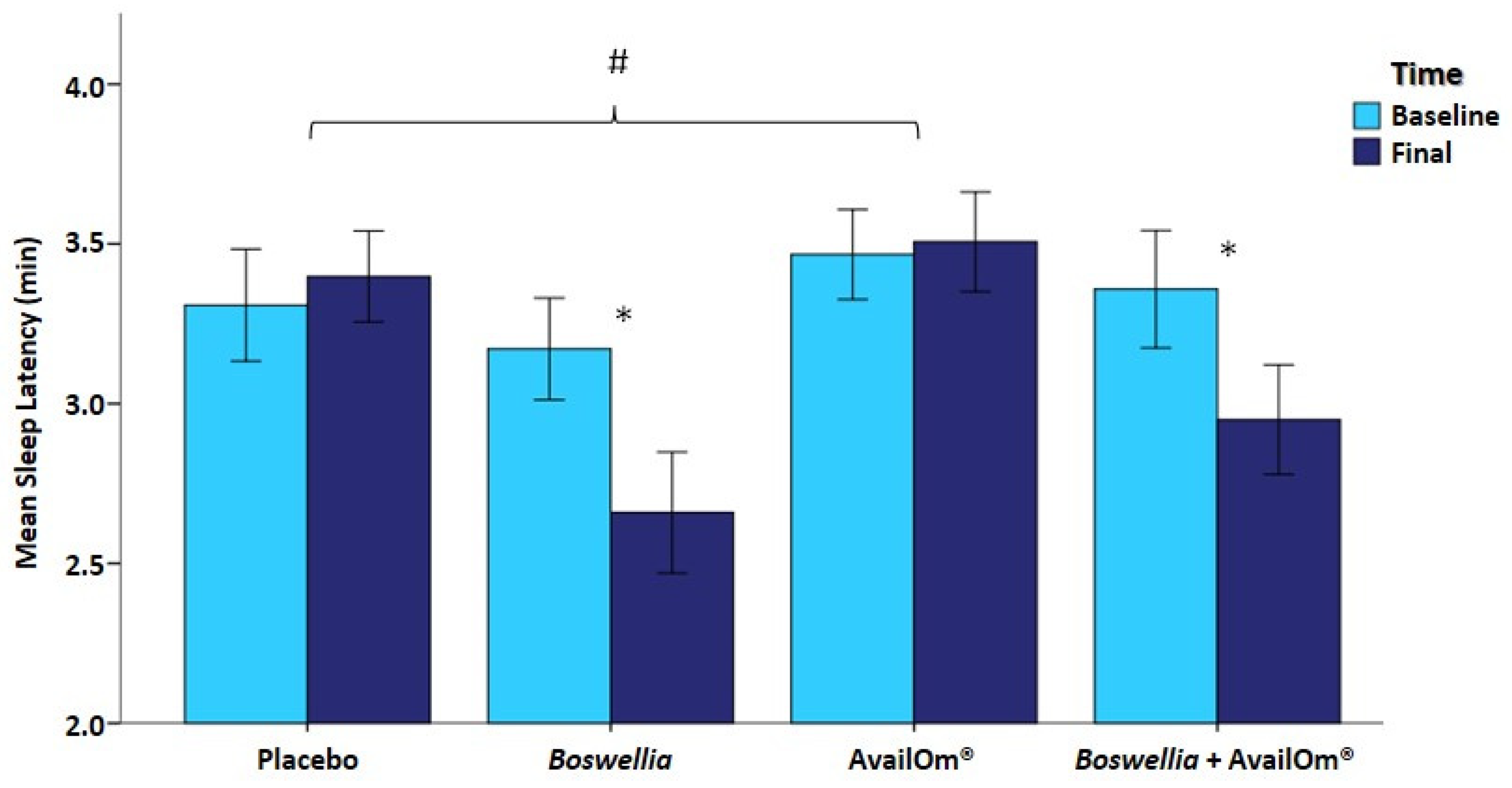
3.6. Sleep Quality
3.7. Bioavailability of Fatty Acids
3.8. Level of Physical Activity
3.9. Anthropometric Variables, Blood Pressure, and Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization—WHO. Osteoarthritis [Internet]. Available online: https://www.who.int/news-room/fact-sheets/detail/osteoarthritis (accessed on 20 July 2023).
- Long, H.; Liu, Q.; Yin, H.; Wang, K.; Diao, N.; Zhang, Y.; Lin, J.; Guo, A. Prevalence Trends of Site-Specific Osteoarthritis From 1990 to 2019: Findings From the Global Burden of Disease Study 2019. Arthritis Rheumatol. 2022, 74, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Palazzo, C.; Nguyen, C.; Lefevre-Colau, M.-M.; Rannou, F.; Poiraudeau, S. Risk factors and burden of osteoarthritis. Ann. Phys. Rehabil. Med. 2016, 59, 134–138. [Google Scholar] [CrossRef]
- Brandt, K.D.; Dieppe, P.; Radin, E.L. Etiopathogenesis of Osteoarthritis. Rheum. Dis. Clin. N. Am. 2008, 34, 531–559. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Schofield, D.; Callander, E. The individual and socioeconomic impact of osteoarthritis. Nat. Rev. Rheumatol. 2014, 10, 437–441. [Google Scholar] [CrossRef]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef]
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef]
- O’neill, T.W.; Felson, D.T. Mechanisms of Osteoarthritis (OA) Pain. Curr. Osteoporos. Rep. 2018, 16, 611–616. [Google Scholar] [CrossRef]
- Petersen, K.K.; Simonsen, O.; Olesen, A.E.; Mørch, C.D.; Arendt-Nielsen, L. Pain inhibitory mechanisms and response to weak analgesics in patients with knee osteoarthritis. Eur. J. Pain 2019, 23, 1904–1912. [Google Scholar] [CrossRef]
- Chen, T.; Zhu, J.; Zhao, Y.; Li, H.; Li, P.; Fan, J.; Wei, X. The global state of research in pain management of osteoarthritis (2000–2019): A 20-year visualized analysis. Medicine 2021, 100, e23944. [Google Scholar] [CrossRef]
- Fibel, K.H.; Hillstrom, H.J.; Halpern, B.C. State-of-the-Art management of knee osteoarthritis. World J. Clin. Cases 2015, 3, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Hermann, W.; Lambova, S.; Muller-Ladner, U. Current Treatment Options for Osteoarthritis. Curr. Rheumatol. Rev. 2018, 14, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Cordingley, D.M.; Cornish, S.M. Omega-3 Fatty Acids for the Management of Osteoarthritis: A Narrative Review. Nutrients 2022, 14, 3362. [Google Scholar] [CrossRef] [PubMed]
- Curtis, C.L.; Rees, S.G.; Little, C.B.; Flannery, C.R.; Hughes, C.E.; Wilson, C.; Dent, C.M.; Otterness, I.G.; Harwood, J.L.; Caterson, B. Pathologic indicators of degradation and inflammation in human osteoarthritic cartilage are abrogated by exposure to n-3 fatty acids. Arthritis Rheum. 2002, 46, 1544–1553. [Google Scholar] [CrossRef]
- Bahamondes, M.A.; Valdés, C.; Moncada, G. Effect of omega-3 on painful symptoms of patients with osteoarthritis of the synovial joints: Systematic review and meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, 297–306. [Google Scholar] [CrossRef]
- Cleland, L.G.; James, M.J. Omega-3 fatty acids and synovitis in osteoarthritic knees. Nat. Rev. Rheumatol. 2012, 8, 314–315. [Google Scholar] [CrossRef]
- Kuszewski, J.C.; Wong, R.H.X.; Howe, P.R.C. Fish oil supplementation reduces osteoarthritis-specific pain in older adults with overweight/obesity. Rheumatol. Adv. Pract. 2020, 4, rkaa036. [Google Scholar] [CrossRef]
- Sibbritt, D.; Lui, C.; Kroll, T.; Adams, J. Prevalence of glucosamine and omega-3 fatty acid use and characteristics of users among mid-age women: Analysis of a nationally representative sample of 10,638 women. J. Nutr. Health Aging 2016, 20, 637–644. [Google Scholar] [CrossRef]
- Safayhi, H.; Mack, T.; Sabieraj, J.; I Anazodo, M.; Subramanian, L.R.; Ammon, H.P. Boswellic acids: Novel, specific, nonredox inhibitors of 5-lipoxygenase. J. Pharmacol. Exp. Ther. 1992, 261, 1143–1146. [Google Scholar]
- Siddiqui, M.Z. Boswellia Serrata, A Potential Antiinflammatory Agent: An Overview. Indian J. Pharm. Sci. 2011, 73, 255–261. [Google Scholar]
- Kimmatkar, N.; Thawani, V.; Hingorani, L.; Khiyani, R. Efficacy and tolerability of Boswellia serrata extract in treatment of osteoarthritis of knee—A randomized double blind placebo controlled trial. Phytomedicine 2003, 10, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Majeed, M.; Majeed, S.; Narayanan, N.K.; Nagabhushanam, K. A pilot, randomized, double-blind, placebo-controlled trial to assess the safety and efficacy of a novel Boswellia serrata extract in the management of osteoarthritis of the knee. Phytother. Res. 2019, 33, 1457–1468. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; Xiang, W.; Zhang, T.; Zeng, L.; Yang, K.; Li, J. Effectiveness of Boswellia and Boswellia extract for osteoarthritis patients: A systematic review and meta-analysis. BMC Complement. Med. Ther. 2020, 20, 225. [Google Scholar] [CrossRef] [PubMed]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: A systematic review and meta-analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef]
- Victoria-Montesinos, D.; Sánchez-Macarro, M.; Gabaldón-Hernández, J.A.; Abellán-Ruiz, M.S.; Querol-Calderón, M.; Luque-Rubia, A.J.; Bernal-Morell, E.; Ávila-Gandía, V.; López-Román, F.J. Effect of Dietary Supplementation with a Natural Extract of Sclerocarya birrea on Glycemic Metabolism in Subjects with Prediabetes: A Randomized Double-Blind Placebo-Controlled Study. Nutrients 2021, 13, 1948. [Google Scholar] [CrossRef]
- Bindawas, S.M.; Vennu, V.; Al Snih, S. Differences in Health-Related Quality of Life Among Subjects With Frequent Bilateral or Unilateral Knee Pain: Data From the Osteoarthritis Initiative Study. J. Orthop. Sports Phys. Ther. 2015, 45, 128–136. [Google Scholar] [CrossRef]
- Mathieu, S.; Soubrier, M.; Peirs, C.; Monfoulet, L.-E.; Boirie, Y.; Tournadre, A. A Meta-Analysis of the Impact of Nutritional Supplementation on Osteoarthritis Symptoms. Nutrients 2022, 14, 1607. [Google Scholar] [CrossRef]
- Huang, Y.-H.; Chiu, W.-C.; Hsu, Y.-P.; Lo, Y.-L.; Wang, Y.-H. Effects of Omega-3 Fatty Acids on Muscle Mass, Muscle Strength and Muscle Performance among the Elderly: A Meta-Analysis. Nutrients 2020, 12, 3739. [Google Scholar] [CrossRef]
- Dalle, S.; Van Roie, E.; Hiroux, C.; Vanmunster, M.; Coudyzer, W.; Suhr, F.; Bogaerts, S.; Van Thienen, R.; Koppo, K. Omega-3 Supplementation Improves Isometric Strength But Not Muscle Anabolic and Catabolic Signaling in Response to Resistance Exercise in Healthy Older Adults. J. Gerontol. Ser. A 2020, 76, 406–414. [Google Scholar] [CrossRef]
- Cornish, S.M.; Cordingley, D.M.; Shaw, K.A.; Forbes, S.C.; Leonhardt, T.; Bristol, A.; Candow, D.G.; Chilibeck, P.D. Effects of Omega-3 Supplementation Alone and Combined with Resistance Exercise on Skeletal Muscle in Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2221. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, C.R.; Noll, M.; Castro, M.C.R.; Silveira, E.A. Effects of Nutritional Interventions in the Control of Musculoskeletal Pain: An Integrative Review. Nutrients 2020, 12, 3075. [Google Scholar] [CrossRef]
- Carballo-Casla, A.; García-Esquinas, E.; Banegas, J.R.; Rodríguez-Artalejo, F.; Ortolá, R. Fish consumption, omega-3 fatty acid intake, and risk of pain: The Seniors-ENRICA-1 cohort. Clin. Nutr. 2022, 41, 2587–2595. [Google Scholar] [CrossRef]
- Goldberg, R.J.; Katz, J. A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain 2007, 129, 210–223. [Google Scholar] [CrossRef] [PubMed]
- Ammon, H.P.T. Boswellic Acids in Chronic Inflammatory Diseases. Planta Medica 2006, 72, 1100–1116. [Google Scholar] [CrossRef] [PubMed]
- Börner, F.; Pace, S.; Jordan, P.M.; Gerstmeier, J.; Gomez, M.; Rossi, A.; Gilbert, N.C.; Newcomer, M.E.; Werz, O. Allosteric Activation of 15-Lipoxygenase-1 by Boswellic Acid Induces the Lipid Mediator Class Switch to Promote Resolution of Inflammation. Adv. Sci. 2022, 10, 2205604. [Google Scholar] [CrossRef]
- Lampl, C.; Haider, B.; Schweiger, C. Long-term efficacy of Boswellia serrata in four patients with chronic cluster headache. Cephalalgia 2012, 32, 719–722. [Google Scholar] [CrossRef]
- Finan, P.H.; Goodin, B.R.; Smith, M.T. The Association of Sleep and Pain: An Update and a Path Forward. J. Pain 2013, 14, 1539–1552. [Google Scholar] [CrossRef]
- Parmelee, P.A.; Tighe, C.A.; Dautovich, N.D. Sleep Disturbance in Osteoarthritis: Linkages With Pain, Disability, and Depressive Symptoms. Arthritis Care Res. 2015, 67, 358–365. [Google Scholar] [CrossRef]
- Sasaki, E.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Inoue, R.; Chiba, D.; Okubo, N.; Takahashi, I.; Nakaji, S.; Ishibashi, Y. Nocturnal Knee Pain Increases With the Severity of Knee Osteoarthritis, Disturbing Patient Sleep Quality. Arthritis Care Res. 2014, 66, 1027–1032. [Google Scholar] [CrossRef]
- de Salazar, L.; Contreras, C.; Torregrosa-García, A.; Luque-Rubia, A.J.; Ávila-Gandía, V.; Domingo, J.C.; López-Román, F.J. Oxidative Stress in Endurance Cycling Is Reduced Dose-Dependently after One Month of Re-Esterified DHA Supplementation. Antioxidants 2020, 9, 1145. [Google Scholar] [CrossRef] [PubMed]
- Karlapudi, V.; Sunkara, K.B.; Konda, P.R.; Sarma, K.V.; Rokkam, M.P. Efficacy and Safety of Aflapin®, a Novel Boswellia Serrata Extract, in the Treatment of Osteoarthritis of the Knee: A Short-Term 30-Day Randomized, Double-Blind, Placebo-Controlled Clinical Study. J. Am. Nutr. Assoc. 2022, 42, 159–168. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variables | Study Groups | |||||
|---|---|---|---|---|---|---|
| Placebo (n = 30) | Boswellia (n = 29) | AvailOm® (n = 31) | Boswellia + AvailOm® (n = 30) | Total (n = 120) | p Value | |
| Age, years | 50.2 ± 8.1 | 50.5 ± 8.2 | 51.1 ± 6.8 | 53.2 ± 10.1 | 51.3 ± 8.4 | 0.510 |
| Weight, kg | 80.1 ± 15.6 | 76.1 ± 17.9 | 76.4 ± 14.7 | 76.4 ± 14.1 | 77.2 ± 15.5 | 0.717 |
| Fat mass, % | 28.5 ± 8.4 | 28.8 ± 7.4 | 29.0 ± 8.2 | 30.8 ± 8.4 | 29.3 ± 8.1 | 0.680 |
| BMI, kg/m2 | 27.0 ± 3.5 | 25.8 ± 4.3 | 26.3 ± 3.7 | 26.9 ± 3.4 | 26.5 ± 3.7 | 0.562 |
| Systolic BP, mmHg | 124.4 ± 17.6 | 118.8 ± 20.6 | 120.9 ± 11.5 | 121.0 ± 15.1 | 121.3 ± 16.4 | 0.625 |
| Diastolic BP, mmHg | 79.6 ± 11.1 | 76.0 ± 12.7 | 78.0 ± 9.1 | 80.2 ± 11.1 | 78.5 ± 11.0 | 0.481 |
| VAS score, cm | 5.0 ± 1.7 | 5.5 ± 1.8 | 5.4 ±1.5 | 5.3 ± 1.9 | 5.3 ± 1.7 | 0.896 |
| WOMAC Score | Baseline | Final (8 Weeks) | % Improvement Due to Product | Within-Group p Value | Between-Group p Value |
|---|---|---|---|---|---|
| Overall | |||||
| Placebo | 29.3 ± 13.5 | 24.6 ± 13.3 | - | 0.047 | 0.005 |
| Boswellia | 24.4 ± 14.0 | 18.2 ± 10.0 | 9.4 | 0.011 | |
| AvailOm® | 28.0 ± 10.7 | 19.1 ± 13.2 | 15.7 | 0.001 | |
| Boswellia + AvailOm® | 34.5 ± 12.8 | 18.7 ± 11.5 | 29.7 | 0.001 | |
| Pain | |||||
| Placebo | 6.4 ± 3.1 | 5.5 ± 2.9 | - | 0.064 | 0.005 |
| Boswellia | 5.9 ± 2.2 | 4.0 ± 2.3 | 18.1 | 0.001 | |
| AvailOm® | 5.9 ± 2.5 | 4.0 ± 2.9 | 18.1 | 0.001 | |
| Boswellia + AvailOm® | 7.4 ± 2.5 | 3.9 ± 2.8 | 33.2 | 0.001 | |
| Stiffness | |||||
| Placebo | 2.5 ± 1.3 | 1.7 ± 1.5 | - | 0.011 | 0.029 |
| Boswellia | 2.1 ± 1.7 | 1.6 ± 1.6 | −8.0 | 0.129 | |
| AvailOm® | 2.9 ± 1.9 | 1.7 ± 1.5 | 9.4 | 0.001 | |
| Boswellia + AvailOm® | 3.2 ± 1.6 | 1.4 ± 1.4 | 24.3 | 0.001 | |
| Physical function | |||||
| Placebo | 20.3 ± 10.3 | 17.4 ± 10.3 | - | 0.101 | 0.013 |
| Boswellia | 16.4 ± 10.9 | 12.7 ± 7.3 | 8.4 | 0.038 | |
| AvailOm® | 19.2 ± 7.5 | 13.4 ± 9.7 | 16.0 | 0.001 | |
| Boswellia + AvailOm® | 23.9 ± 9.6 | 13.3 ± 8.5 | 30.2 | 0.001 | |
| Study Groups | VAS Score, Mean ± SD | % Improvement Due to Product | Within-Group p Value | Between-Group p Value | |
|---|---|---|---|---|---|
| Baseline | Final (8 Weeks) | ||||
| Placebo (n = 30) | 5.1 ± 1.7 | 4.0 ± 2.2 | - | 0.006 | 0.001 |
| Boswellia (n = 29) | 5.4 ± 1.8 | 2.4 ± 1.8 | 29.6 | 0.001 | |
| AvailOm® (n = 31) | 5.3 ± 1.5 | 2.3 ± 2.2 | 30.7 | 0.001 | |
| Boswellia + AvailOm® (n = 30) | 5.4 ± 1.9 | 2.4 ± 2.0 | 29.6 | 0.001 | |
| Time Point | Study Groups, VAS Score, Mean ± SD | |||
|---|---|---|---|---|
| Placebo (n = 30) | Boswellia (n = 29) | AvailOm® (n = 31) | Boswellia + AvailOm® (n = 30) | |
| Baseline | 5.0 ± 1.7 | 5.0 ± 1.8 | 5.4 ± 1.5 | 5.3 ± 1.9 |
| Week 1 | 3.8 ± 2.0 | 3.6 ± 2.2 | 3.6 ± 2.2 | 3.7 ± 2.1 |
| Week 2 | 3.6 ± 2.1 | 3.4 ± 2.1 | 3.3 ± 2.3 | 3.5 ± 1.9 |
| Week 3 | 3.5 ± 2.0 | 3.2 ± 2.2 | 3.1 ± 2.3 | 3.2 ± 2.2 |
| Week 4 | 3.4 ± 2.1 | 2.8 ± 1.9 | 2.7 ± 2.0 | 2.8 ± 2.2 |
| Week 5 | 3.3 ± 2.0 | 2.4 ± 2.0 | 2.5 ± 2.0 | 2.8 ± 2.1 |
| Week 6 | 3.3 ± 2.3 | 2.3 ± 2.0 | 2.2 ± 1.7 | 2.9 ± 2.5 |
| Week 7 | 3.2 ± 2.2 | 2.3 ± 2.0 | 1.9 ± 1.6 | 2.6 ± 2.5 |
| Week 8 | 3.2 ± 2.4 | 2.1 ± 1.9 | 1.8 ± 1.6 | 2.3 ± 2.3 |
| Within-group p value | 0.002 | 0.001 | 0.001 | 0.001 |
| Between-group p value | 0.010 | |||
| Study Group | Baseline | Final | Within-Group p Value | Between-Group p Value | ||
|---|---|---|---|---|---|---|
| Isokinetic Dynamometry | ||||||
| At 60°·s−1 knee extension | Peak torque, Nm | Placebo | 123.9 ± 59.5 | 120.0 ± 61.9 | 0.250 | 0.050 |
| Boswellia | 104.3 ± 50.9 | 108.7 ± 45.7 | 0.205 | |||
| AvailOm® | 113.5 ± 50.6 | 121.4 ± 48.9 | 0.019 | |||
| Boswellia + AvailOm® | 109.5 ± 45.2 | 115.5 ± 48.5 | 0.050 | |||
| Total work, J | Placebo | 531.4 ± 241.4 | 524.8 ± 265.6 | 0.714 | 0.577 | |
| Boswellia | 464.2 ± 219.7 | 476.3 ± 192.3 | 0.508 | |||
| AvailOm® | 496.3 ± 214.7 | 524.9 ± 212.2 | 0.107 | |||
| Boswellia + AvailOm® | 472.9 ± 190.2 | 487.8 ± 213.6 | 0.409 | |||
| Total work for 1RM, J | Placebo | 114.0 ± 50.1 | 111.8 ± 54.3 | 0.494 | 0.235 | |
| Boswellia | 100.5 ± 46.4 | 103.2 ± 40.9 | 0.388 | |||
| AvailOm® | 106.1 ± 44.2 | 111.8 ± 43.1 | 0.050 | |||
| Boswellia + AvailOm® | 103.2 ± 39.4 | 108.9 ± 42.8 | 0.048 | |||
| Average power, W | Placebo | 73.7 ± 36.6 | 74.1 ± 41.4 | 0.847 | 0.050 | |
| Boswellia | 63.7 ± 31.1 | 66.1 ± 29.0 | 0.268 | |||
| AvailOm® | 68.5 ± 30.8 | 73.4 ± 29.7 | 0.021 | |||
| Boswellia + AvailOm® | 63.9 ± 28.0 | 71.8 ± 32.3 | 0.001 | |||
| At 60°·s−1 knee flexion | Peak torque, Nm | Placebo | 62.0 ± 28.4 | 62.9 ± 30.6 | 0.690 | 0.223 |
| Boswellia | 56.3 ± 31.2 | 58.3 ± 29.6 | 0.370 | |||
| AvailOm® | 61.1 ± 32.4 | 67.5 ± 32.8 | 0.003 | |||
| Boswellia + AvailOm® | 56.0 ± 26.0 | 61.0 ± 29.5 | 0.020 | |||
| Total work, J | Placebo | 313.6 ± 159.6 | 312.9 ± 165.7 | 0.957 | 0.131 | |
| Boswellia | 282.7 ± 185.8 | 292.0 ± 170.7 | 0.460 | |||
| AvailOm® | 313.8 ± 183.7 | 343.4 ± 183.4 | 0.016 | |||
| Boswellia + AvailOm® | 277.6 ± 148.1 | 313.2 ± 164.0 | 0.005 | |||
| Total work for 1RM, J | Placebo | 69.9 ± 31.8 | 70.0 ± 35.5 | 0.950 | 0.352 | |
| Boswellia | 62.2 ± 38.0 | 65.0 ± 35.7 | 0.285 | |||
| AvailOm® | 69.1 ± 37.4 | 74.9 ± 38.1 | 0.023 | |||
| Boswellia + AvailOm® | 62.4 ± 31.1 | 68.0 ± 34.0 | 0.030 | |||
| Average power, W | Placebo | 40.4 ± 22.0 | 41.8 ± 24.2 | 0.421 | 0.050 | |
| Boswellia | 36.2 ± 24.3 | 38.1 ± 23.3 | 0.278 | |||
| AvailOm® | 40.6 ± 25.3 | 45.9 ± 25.8 | 0.003 | |||
| Boswellia + AvailOm® | 35.1 ± 21.3 | 42.5 ± 25.9 | 0.001 | |||
| At 180°·s−1 knee extension | Peak torque, Nm | Placebo | 83.3 ± 41.3 | 82.3 ± 44.2 | 0.707 | 0.208 |
| Boswellia | 68.1 ± 32.5 | 72.5 ± 33.8 | 0.127 | |||
| AvailOm® | 77.6 ± 33.1 | 84.9 ± 33.5 | 0.009 | |||
| Boswellia + AvailOm® | 70.5 ± 29.8 | 73.8 ± 32.8 | 0.251 | |||
| Total work, J | Placebo | 401.2 ± 200.7 | 389.7 ± 213.2 | 0.441 | 0.050 | |
| Boswellia | 321.6 ± 174.5 | 338.5 ± 162.5 | 0.267 | |||
| AvailOm® | 372.8 ± 164.9 | 414.5 ± 172.5 | 0.005 | |||
| Boswellia + AvailOm® | 342.6 ± 147.1 | 354.9 ± 159.4 | 0.413 | |||
| Total work for 1RM, J | Placebo | 88.3 ± 42.0 | 85.1 ± 44.3 | 0.344 | 0.050 | |
| Boswellia | 70.0 ± 38.9 | 77.2 ± 36.6 | 0.036 | |||
| AvailOm® | 81.3 ± 35.4 | 88.7 ± 34.9 | 0.024 | |||
| Boswellia + AvailOm® | 76.1 ± 32.4 | 79.4 ± 34.9 | 0.316 | |||
| Average power, W | Placebo | 133.3 ± 73.8 | 130.8 ± 80.2 | 0.641 | 0.046 | |
| Boswellia | 106.1 ± 63.4 | 112.5 ± 58.2 | 0.248 | |||
| AvailOm® | 118.4 ± 58.0 | 137.7 ± 56.9 | 0.001 | |||
| Boswellia + AvailOm® | 111.9 ± 54.1 | 119.6 ± 60.8 | 0.158 | |||
| At 180°·s−1 knee flexion | Peak torque, Nm | Placebo | 51.8 ± 24.4 | 53.0 ± 25.1 | 0.491 | 0.778 |
| Boswellia | 46.2 ± 26.6 | 46.1 ± 24.4 | 0.988 | |||
| AvailOm® | 51.9 ± 27.1 | 54.4 ± 27.1 | 0.417 | |||
| Boswellia + AvailOm® | 46.9 ± 19.0 | 48.6 ± 21.4 | 0.337 | |||
| Total work, J | Placebo | 208.2 ± 145.0 | 203.7 ± 144.9 | 0.728 | 0.194 | |
| Boswellia | 180.9 ± 165.3 | 182.1 ± 139.7 | 0.927 | |||
| AvailOm® | 210.6 ± 151.8 | 241.7 ± 148.5 | 0.016 | |||
| Boswellia + AvailOm® | 186.8 ± 124.7 | 205.5 ± 139.9 | 0.151 | |||
| Total work for 1RM, J | Placebo | 47.5 ± 30.6 | 46.3 ± 29.1 | 0.640 | 0.329 | |
| Boswellia | 40.9 ± 34.5 | 42.6 ± 29.3 | 0.513 | |||
| AvailOm® | 47.7 ± 30.9 | 52.1 ± 29.2 | 0.050 | |||
| Boswellia + AvailOm® | 42.5 ± 25.9 | 47.2 ± 30.4 | 0.050 | |||
| Average power, W | Placebo | 64.0 ± 49.4 | 62.2 ± 50.1 | 0.679 | 0.096 | |
| Boswellia | 54.0 ± 49.6 | 54.9 ± 44.5 | 0.853 | |||
| AvailOm® | 62.3 ± 53.0 | 74.4 ± 48.9 | 0.008 | |||
| Boswellia + AvailOm® | 54.7 ± 41.7 | 63.8 ± 49.5 | 0.046 | |||
| Isometric Dynamometry | 0.725 | |||||
| At 90° knee position | Peak torque, Nm | Placebo | 150.3 ± 71.5 | 153.1 ± 71.1 | 0.533 | |
| Boswellia | 140.7 ± 75.9 | 146.1 ± 67.1 | 0.246 | |||
| AvailOm® | 146.5 ± 73.5 | 153.3 ± 79.2 | 0.136 | |||
| Boswellia + AvailOm® | 138.8 ± 66.3 | 148.9 ± 65.5 | 0.029 | 0.620 | ||
| Average peak torque, Nm | Placebo | 143.2 ± 68.4 | 143.6 ± 72.6 | 0.941 | ||
| Boswellia | 132.2 ± 72.1 | 138.8 ± 66.8 | 0.146 | |||
| AvailOm® | 139.4 ± 72.3 | 145.7 ± 75.3 | 0.149 | |||
| Boswellia + AvailOm® | 131.5 ± 63.6 | 139.6 ± 62.0 | 0.050 | |||
| Variable | Baseline | Final (8 Weeks) | Within-Group p Value | Between-Group p Value |
|---|---|---|---|---|
| Sleep latency, min | ||||
| Placebo | 3.3 ± 1.0 | 3.4 ± 0.8 | 0.662 | 0.050 |
| Boswellia | 3.2 ± 0.9 | 2.7 ± 1.0 | 0.016 | |
| AvailOm® | 3.5 ± 0.8 | 3.5 ± 0.9 | 0.843 | |
| Boswellia + AvailOm® | 3.4 ± 1.0 | 3.0 ± 0.9 | 0.048 | |
| Sleep efficiency, % | ||||
| Placebo | 91.5 ± 3.6 | 91.6 ± 3.2 | 0.899 | 0.515 |
| Boswellia | 90.9 ± 2.7 | 91.9 ± 2.7 | 0.050 | |
| AvailOm® | 91.7 ± 3.6 | 91.8 ± 3.0 | 0.755 | |
| Boswellia + AvailOm® | 91.4 ± 3.2 | 92.2 ± 3.4 | 0.119 | |
| Total time in bed, min | ||||
| Placebo | 431.7 ± 60.0 | 422.1 ± 61.3 | 0.430 | 0.462 |
| Boswellia | 416.2 ± 63.0 | 427.8 ± 74.0 | 0.353 | |
| AvailOm® | 411.0 ± 56.0 | 405.6 ± 62.2 | 0.653 | |
| Boswellia + AvailOm® | 419.4 ± 65.0 | 431.7 ± 72.6 | 0.318 | |
| Total sleep time, min | ||||
| Placebo | 396.6 ± 59.6 | 390.0 ± 61.9 | 0.563 | 0.817 |
| Boswellia | 394.6 ± 68.7 | 387.2 ± 70.6 | 0.527 | |
| AvailOm® | 399.5 ± 82.7 | 391.1 ± 91.0 | 0.455 | |
| Boswellia + AvailOm® | 389.2 ± 69.2 | 394.4 ± 77.6 | 0.651 | |
| Wakefulness after sleep onset, min | ||||
| Placebo | 33.3 ± 13.1 | 33.6 ± 13.1 | 0.877 | 0.046 |
| Boswellia | 37.2 ± 13.0 | 32.5 ± 10.5 | 0.019 | |
| AvailOm® | 30.4 ± 13.3 | 30.3 ± 11.4 | 0.947 | |
| Boswellia + AvailOm® | 35.0 ± 10.7 | 28.9 ± 12.2 | 0.002 | |
| Number of awakenings | ||||
| Placebo | 13.8 ± 5.7 | 13.9 ± 5.5 | 0.912 | 0.049 |
| Boswellia | 16.2 ± 5.0 | 13.5 ± 5.0 | 0.009 | |
| AvailOm® | 15.0 ± 5.8 | 15.1 ± 5.3 | 0.954 | |
| Boswellia + AvailOm® | 17.0 ± 6.8 | 14.1 ± 6.0 | 0.005 | |
| Awakenings, mean number of min | ||||
| Placebo | 2.4 ± 0.7 | 2.4 ± 0.6 | 0.773 | 0.750 |
| Boswellia | 2.3 ± 0.4 | 2.4 ± 0.5 | 0.448 | |
| AvailOm® | 2.5 ± 0.8 | 2.5 ± 1.0 | 0.572 | |
| Boswellia + AvailOm® | 2.4 ± 0.7 | 2.3 ± 0.7 | 0.591 |
| Variable | Baseline | Final (8 Weeks) | Within-Group p Value | Between-Group p Value |
|---|---|---|---|---|
| Omega-3 index | ||||
| Placebo | 5.64 ± 0.88 | 5.45 ± 0.70 | 0.251 | 0.001 |
| Boswellia | 5.88 ± 1.01 | 5.50 ± 0.87 | 0.024 | |
| AvailOm® | 5.58 ± 1.11 | 6.10 ± 1.00 | 0.002 | |
| Boswellia + AvailOm® | 5.35 ± 0.98 | 6.02 ± 1.42 | 0.001 | |
| DHA, % | ||||
| Placebo | 3.29 ± 0.60 | 3.12 ± 0.49 | 0.098 | 0.022 |
| Boswellia | 3.38 ± 0.60 | 3.17 ± 0.55 | 0.038 | |
| AvailOm® | 3.16 ± 0.70 | 3.22 ± 0.60 | 0.507 | |
| Boswellia + AvailOm® | 3.02 ± 0.64 | 3.19 ± 0.83 | 0.050 | |
| EPA, % | ||||
| Placebo | 0.50 ± 0.23 | 0.51 ± 0.19 | 0.970 | 0.001 |
| Boswellia | 0.63 ± 0.35 | 0.50 ± 0.28 | 0.058 | |
| AvailOm® | 0.59 ± 0.37 | 0.97 ± 0.39 | 0.001 | |
| Boswellia + AvailOm® | 0.52 ± 0.27 | 0.94 ± 0.48 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Piñero, S.; Muñoz-Carrillo, J.C.; Victoria-Montesinos, D.; García-Muñoz, A.M.; Andreu-Caravaca, L.; Gómez, M.; Schölzel, M.; García-Guillén, A.I.; López-Román, F.J. Efficacy of Boswellia serrata Extract and/or an Omega-3-Based Product for Improving Pain and Function in People Older Than 40 Years with Persistent Knee Pain: A Randomized Double-Blind Controlled Clinical Trial. Nutrients 2023, 15, 3848. https://doi.org/10.3390/nu15173848
Pérez-Piñero S, Muñoz-Carrillo JC, Victoria-Montesinos D, García-Muñoz AM, Andreu-Caravaca L, Gómez M, Schölzel M, García-Guillén AI, López-Román FJ. Efficacy of Boswellia serrata Extract and/or an Omega-3-Based Product for Improving Pain and Function in People Older Than 40 Years with Persistent Knee Pain: A Randomized Double-Blind Controlled Clinical Trial. Nutrients. 2023; 15(17):3848. https://doi.org/10.3390/nu15173848
Chicago/Turabian StylePérez-Piñero, Silvia, Juan Carlos Muñoz-Carrillo, Desirée Victoria-Montesinos, Ana María García-Muñoz, Luis Andreu-Caravaca, Mario Gómez, Melanie Schölzel, Ana I. García-Guillén, and Francisco Javier López-Román. 2023. "Efficacy of Boswellia serrata Extract and/or an Omega-3-Based Product for Improving Pain and Function in People Older Than 40 Years with Persistent Knee Pain: A Randomized Double-Blind Controlled Clinical Trial" Nutrients 15, no. 17: 3848. https://doi.org/10.3390/nu15173848
APA StylePérez-Piñero, S., Muñoz-Carrillo, J. C., Victoria-Montesinos, D., García-Muñoz, A. M., Andreu-Caravaca, L., Gómez, M., Schölzel, M., García-Guillén, A. I., & López-Román, F. J. (2023). Efficacy of Boswellia serrata Extract and/or an Omega-3-Based Product for Improving Pain and Function in People Older Than 40 Years with Persistent Knee Pain: A Randomized Double-Blind Controlled Clinical Trial. Nutrients, 15(17), 3848. https://doi.org/10.3390/nu15173848