

The Impact of Different Types of Diet on the Prevention of Diseases among Polish Inhabitants, Including COVID-19 Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Explanatory Variables
2.3. Measures
2.4. Statistics
3. Results
3.1. Study Group
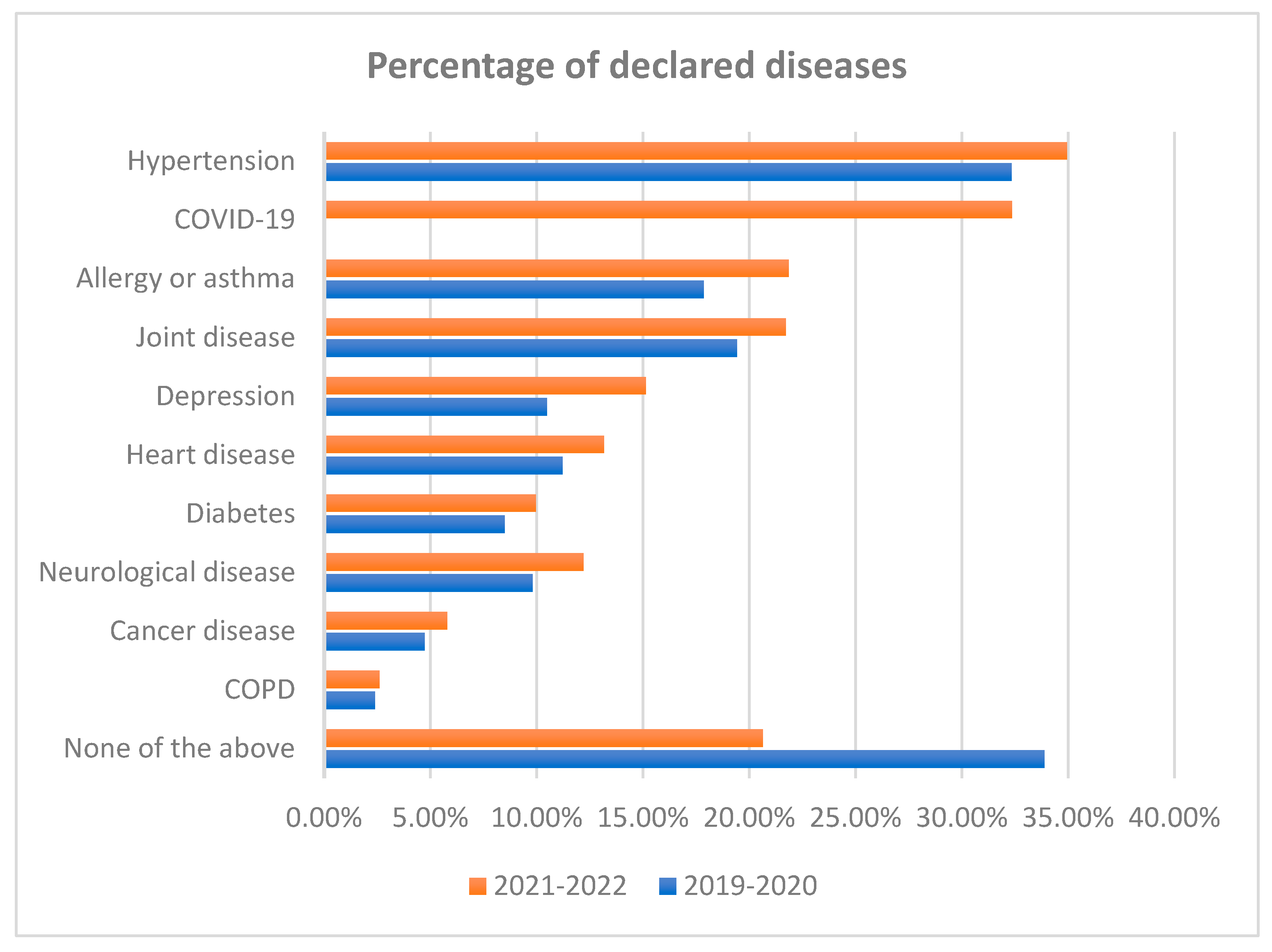
3.2. Observed Diseases
3.3. Types of Diet
3.4. Correlation between the Presence of COVID-19 Pandemic, Sociodemographic Factors, and Diet and Hypertension
3.5. Correlation between Sociodemographic Factors, Diet, and COVID-19 Disease
3.6. Correlation between the Presence of the COVID-19 Pandemic, Sociodemographic Factors, and Diet, Allergies, and Asthma
3.7. Correlation between the Presence of the COVID-19 Pandemic, Sociodemographic Factors, and Diet and Joint Diseases
3.8. Correlation between the Presence of the COVID-19 Pandemic, Sociodemographic Factors, and Diet and Depression
3.9. Correlation between the Presence of the COVID-19 Pandemic, Sociodemographic Factors, and Diet and Heart Disease
3.10. Correlations between Neurological Disease and Diet
3.11. Correlation between the Presence of the COVID-19 Pandemic, Sociodemographic Factors, and Diet and Diabetes
3.12. Correlation between the Presence of the COVID-19 Pandemic, Sociodemographic Factors, and Diet and Cancer
3.13. Correlation between the Presence of the COVID-19 Pandemic, Sociodemographic Factors, and Diet and COPD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ioannidis, J.P.A. Implausible results in human nutrition research. Br. Med. J. 2013, 347, f6698. [Google Scholar] [CrossRef] [PubMed]
- Bel-Serrat, S.; von der Schulenburg, A.; Marques-Previ, M.; Mullee, A.; Murrin, C.M. What are the determinants of vegetable intake among adolescents from socioeconomically disadvantaged urban areas? A systematic review of qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 158. [Google Scholar] [CrossRef] [PubMed]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Cardiovascular Disease Prevention: All Plant Foods Are Not Created Equal. Curr. Atheroscler. Rep. 2019, 21, 18. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Kendall, C.W.C.; Marchie, A.; Jenkins, A.L.; Augustin, L.S.A.; Ludwig, D.S.; Barnard, N.D.; Anderson, J.W. Type 2 diabetes and the vegetarian diet. Am. J. Clin. Nutr. 2003, 78, 610S–616S. [Google Scholar] [CrossRef]
- Wang, F.; Zheng, J.; Yang, B.; Jiang, J.; Fu, Y.; Li, D. Effects of vegetarian diets on blood lipids: A systematic review and meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 2015, 4, e002408. [Google Scholar] [CrossRef] [PubMed]
- Tuso, P.; Stoll, S.R.; Li, W.W. A plant-based diet, atherogenesis, and coronary artery disease prevention. Perm. J. 2015, 19, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Plant-based foods and prevention of cardiovascular disease: An overview. Am. J. Clin. Nutr. 2003, 78, 544S–551S. [Google Scholar] [CrossRef]
- Rosell, M.; Appleby, P.; Spencer, E.; Key, T. Weight gain over 5 years in 21 966 meat-eating, fish-eating, vegetarian, and vegan men and women in EPIC-Oxford. Int. J. Obes. 2006, 30, 1389–1396. [Google Scholar] [CrossRef]
- Barnard, N.D.; Scialli, A.R.; Turner-McGrievy, G.; Lanou, A.J.; Glass, J. The effects of a low-fat, plant-based dietary intervention on body weight, metabolism, and insulin sensitivity. Am. J. Med. 2005, 118, 991–997. [Google Scholar] [CrossRef]
- Berkow, S.E.; Barnard, N.D. Blood Pressure Regulation and Vegetarian Diets. Nutr. Rev. 2005, 63, 1–8. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Nishimura, K.; Barnard, N.D.; Takegami, M.; Watanabe, M.; Sekikawa, A.; Okamura, T.; Miyamoto, Y. Vegetarian diets and blood pressure ameta-analysis. JAMA Intern. Med. 2014, 174, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Phillips, F. Vegetarian nutrition. Nutr. Bull. 2005, 30, 132–167. [Google Scholar] [CrossRef]
- Ho-Pham, L.T.; Nguyen, N.D.; Nguyen, T.V. Effect of vegetarian diets on bone mineral density: A Bayesian meta-analysis. Am. J. Clin. Nutr. 2009, 90, 943–950. [Google Scholar] [CrossRef]
- Chiu, T.H.T.; Pan, W.-H.; Lin, M.-N.; Lin, C.-L. Vegetarian diet, change in dietary patterns, and diabetes risk: A prospective study. Nutr. Diabetes 2018, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Barnard, N.D.; Levin, S.M.; Watanabe, M. Vegetarian diets and glycemic control in diabetes: A systematic review and meta-analysis. Cardiovasc. Diagn. Ther. 2014, 4, 373–382. [Google Scholar] [CrossRef]
- Bonaccio, M.; Cerletti, C.; Iacoviello, L.; de Gaetano, G. Mediterranean Diet and Low-grade Subclinical Inflammation: The Moli-sani Study. Endocr. Metab. Immune Disord. Targets 2015, 15, 18–24. [Google Scholar] [CrossRef]
- Tzoulaki, I.; Brown, I.J.; Chan, Q.; Van Horn, L.; Ueshima, H.; Zhao, L.; Stamler, J.; Elliott, P. Relation of iron and red meat intake to blood pressure: Cross sectional epidemiological study. Br. Med. J. 2008, 337, 215–217. [Google Scholar] [CrossRef]
- Susic, D.; Frohlich, E.D. Salt consumption and cardiovascular, renal, and hypertensive diseases: Clinical and mechanistic aspects. Curr. Opin. Lipidol. 2012, 23, 11–16. [Google Scholar] [CrossRef]
- Cross, A.J.; Sinha, R. Meat-related mutagens/carcinogens in the etiology of colorectal cancer. Environ. Mol. Mutagen. 2004, 44, 44–55. [Google Scholar] [CrossRef]
- COVID-19 Map COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/data/mortality%0Ahttps://coronavirus.jhu.edu/map.html (accessed on 17 July 2023).
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Timothy Garvey, W.; Karen Lau, K.H.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef]
- Canada, D. Diabetes Canada Position Statement on Low-Carbohydrate Diets for Adults With Diabetes: A Rapid Review. Can. J. Diabetes 2020, 44, 295–299. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Szychowska, A.; Zimny-Zając, A.; Dziankowska-Zaborszczyk, E.; Grodzicki, T.; Drygas, W.; Zdrojewski, T. Physical Activity versus Selected Health Behaviors, Subjective Physical and Psychological Health and Multimorbidity in a Large Cohort of Polish Seniors during the COVID-19 Pandemic (Results of the National Test for Poles’ Health). Int. J. Environ. Res. Public Health 2023, 20, 556. [Google Scholar] [CrossRef] [PubMed]
- Gołębiowska, J.; Zimny-Zając, A.; Dróżdż, M.; Makuch, S.; Dudek, K.; Mazur, G.; Agrawal, S. Evaluation of the Approach towards Vaccination against COVID-19 among the Polish Population—In Relation to Sociodemographic Factors and Physical and Mental Health. Vaccines 2023, 11, 700. [Google Scholar] [CrossRef]
- Onet—Narodowy Test Zdrowia. Available online: https://narodowytestzdrowia.medonet.pl/ (accessed on 28 January 2023).
- Centers for Disease Control and Prevention about Adult BMI|Healthy Weight, Nutrition, and Physical Activity|CDC. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html%0Ahttps://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html#InterpretedAdults (accessed on 17 July 2023).
- World Health Organization; Noncommunicable Diseases. Available online: https://www.who.int/health-topics/noncommunicable-diseases#tab=tab_1 (accessed on 15 August 2023).
- Narodowy Test Zdrowia Polaków, Raport 2022. Available online: http://ocdn.eu/medonet/medonet%20market/NTZP2022_raport_display.pdf?fbclid=IwAR2OFicRpr7Lw7zxYBu5yfUJUfUCXclxgz3zNHRx3ukdRV-AVxxV8FdmrRo (accessed on 16 August 2023).
- Di Giosia, P.; Giorgini, P.; Stamerra, C.A.; Petrarca, M.; Ferri, C.; Sahebkar, A. Gender Differences in Epidemiology, Pathophysiology, and Treatment of Hypertension. Curr. Atheroscler. Rep. 2018, 20, 13. [Google Scholar] [CrossRef] [PubMed]
- Reckelhoff, J.F. Sex differences in regulation of blood pressure. Adv. Exp. Med. Biol. 2018, 1065, 139–151. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, Z.; Zhang, L.; Wang, X.; Hao, G.; Zhang, Z.; Shao, L.; Tian, Y.; Dong, Y.; Zheng, C.; et al. Status of hypertension in China: Results from the China Hypertension Survey, 2012–2015. Circulation 2018, 137, 2344–2356. [Google Scholar] [CrossRef]
- Ramirez, L.A.; Sullivan, J.C. Sex Differences in Hypertension: Where We Have Been and Where We Are Going. Am. J. Hypertens. 2018, 31, 1247–1254. [Google Scholar] [CrossRef]
- Shepard, B.D. Sex differences in diabetes and kidney disease: Mechanisms and consequences. Am. J. Physiol. Renal Physiol. 2019, 317, F456–F462. [Google Scholar] [CrossRef]
- Cutler, D.M.; Lleras-Muney, A. Education and Health: Evaluating Theories and Evidence. In Making Americans Healthier: Social and Economic Policy as Health Policy; House, J., Schoeni, R., Kaplan, G., Pollack, H., Eds.; Russell Sage Foundation: New York, NY, USA, 2008. [Google Scholar]
- David, R. Changing therapeutic paradigms in glaucoma management. Expert Opin. Investig. Drugs 1998, 7, 1063–1086. [Google Scholar] [CrossRef]
- Kumar, P.; Kumar, M.; Bedi, O.; Gupta, M.; Kumar, S.; Jaiswal, G.; Rahi, V.; Yedke, N.G.; Bijalwan, A.; Sharma, S.; et al. Role of vitamins and minerals as immunity boosters in COVID-19. Inflammopharmacology 2021, 29, 1001–1016. [Google Scholar] [CrossRef] [PubMed]
- Franco, E.; Urosa, J.; Barakat, R.; Refoyo, I. Physical activity and adherence to the mediterranean diet among spanish employees in a health-promotion program before and during the COVID-19 pandemic: The sanitas-healthy cities challenge. Int. J. Environ. Res. Public Health 2021, 18, 2735. [Google Scholar] [CrossRef] [PubMed]
- González-Monroy, C.; Gómez-Gómez, I.; Olarte-Sánchez, C.M.; Motrico, E. Eating behaviour changes during the COVID-19 pandemic: A systematic review of longitudinal studies. Int. J. Environ. Res. Public Health 2021, 18, 11130. [Google Scholar] [CrossRef] [PubMed]
- Turner-McGrievy, G.; Mandes, T.; Crimarco, A. A plant-based diet for overweight and obesity prevention and treatment. J. Geriatr. Cardiol. 2017, 14, 369–374. [Google Scholar] [CrossRef]
- Lee, K.W.; Loh, H.C.; Ching, S.M.; Devaraj, N.K.; Hoo, F.K. Effects of vegetarian diets on blood pressure lowering: A systematic review with meta-analysis and trial sequential analysis. Nutrients 2020, 12, 1604. [Google Scholar] [CrossRef]
- Hou, Y.C.; Huang, H.F.; Tsai, W.H.; Huang, S.Y.; Liu, H.W.; Liu, J.S.; Kuo, K.L. Vegetarian Diet Was Associated With a Lower Risk of Chronic Kidney Disease in Diabetic Patients. Front. Nutr. 2022, 9, 843357. [Google Scholar] [CrossRef]
- Qian, F.; Liu, G.; Hu, F.B.; Bhupathiraju, S.N.; Sun, Q. Association between Plant-Based Dietary Patterns and Risk of Type 2 Diabetes: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2019, 179, 1335–1344. [Google Scholar] [CrossRef]
- Termannsen, A.D.; Clemmensen, K.K.B.; Thomsen, J.M.; Nørgaard, O.; Díaz, L.J.; Torekov, S.S.; Quist, J.S.; Færch, K. Effects of vegan diets on cardiometabolic health: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2022, 23, e13462. [Google Scholar] [CrossRef]
- Jain, R.; Larsuphrom, P.; Degremont, A.; Latunde-Dada, G.O.; Philippou, E. Association between vegetarian and vegan diets and depression: A systematic review. Nutr. Bull. 2022, 47, 27–49. [Google Scholar] [CrossRef]
- Luo, Y.; Li, Y.; Dai, J. Low blood sodium increases risk and severity of COVID-19: A systematic review, meta-analysis and retrospective cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Lippi, G.; South, A.M.; Henry, B.M. Electrolyte imbalances in patients with severe coronavirus disease 2019 (COVID-19). Ann. Clin. Biochem. Int. J. Biochem. Lab. Med. 2020, 57, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Cure, E.; Cure, M.C. COVID-19 may affect the endocrine pancreas by activating Na+/H+ exchanger 2 and increasing lactate levels. J. Endocrinol. Investig. 2020, 43, 1167–1168. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Features (Variables) | Before the Pandemic 2019–2020 | During the Pandemic 2021–2022 | p-Value |
|---|---|---|---|
| Sex: | 0.974 | ||
| Male | 40.63% | 40.61% | |
| Female | 59.37% | 59.39% | |
| Age (years) | 0.170 | ||
| M ± SD | 50 ± 14 | 50 ± 14 | |
| Me [Q1; Q3] | 50 [40; 61] | 50 [40; 61] | |
| Min–Max | 18–99 | 18–93 | |
| Level of education: | 0.066 | ||
| Primary education | 11.54% | 12.35% | |
| Secondary education | 39.39% | 39.20% | |
| Higher education | 49.06% | 48.45% | |
| Status | 0.058 | ||
| Single | 14.84% | 15.65% | |
| In a relationship (not married) | 18.92% | 18.10% | |
| Married | 61.09% | 60.89% | |
| Widow/widower | 5.15% | 5.36% | |
| Place of residence: | 0.062 | ||
| Village | 20.95% | 20.89% | |
| Town, less than 19,000 inhabitants | 11.36% | 11.82% | |
| Town, between 20,000 and 49,000 inhabitants | 14.27% | 14.89% | |
| Town, between 50,000 and 99,000 inhabitants | 11.24% | 11.34% | |
| Town, between 100,000 and 199,000 inhabitants | 10.31% | 10.71% | |
| Town, between 200,000 and 499,000 inhabitants | 10.53% | 10.28% | |
| Town, more than 500,000 inhabitants | 21.33% | 20.08% | |
| Country region | |||
| Central region | 9.49% | 9.09% | 0.204 |
| Southern region | 24.11% | 23.47% | 0.166 |
| Eastern region | 11.84% | 11.59% | 0.474 |
| Northwestern region | 15.20% | 15.83% | 0.109 |
| Southwestern region | 10.18% | 10.55% | 0.263 |
| Northern region | 13.38% | 13.88% | 0.179 |
| Mazovian district | 15.80% | 15.59% | 0.594 |
| Body height (cm) | 0.660 | ||
| M ± SD | 170 ± 9 | 170 ± 9 | |
| Me [Q1; Q3] | 170 [164; 176] | 170 [164; 176] | |
| Min–Max | 130–206 | 140–205 | |
| Body mass (kg): | 0.468 | ||
| M ± SD | 79 ± 17 | 79 ± 18 | |
| Me [Q1; Q3] | 78 [65; 90] | 77 [65; 90] | |
| Min–Max | 30–190 | 33–205 | |
| BMI (kg/m2): | 0.065 | ||
| M ± SD | 27.1 ± 5.0 | 27.1 ± 5.2 | |
| Me [Q1; Q3] | 27 [24; 30] | 26 [24; 30] | |
| Min–Max | 13–60 | 13–59 |
| Observed Diseases | 2019–2020 * n = 17,000 | 2021–2022 n = 17,000 | p-Value |
|---|---|---|---|
| 1. Hypertension | 32.33% | 34.95% | <0.001 |
| 2. Diabetes | 8.49% | 9.95% | <0.001 |
| 3. Heart disease | 11.22% | 13.16% | <0.001 |
| 4. Chronic obstructive pulmonary disease (COPD) | 2.39% | 2.61% | 0.198 |
| 5. Allergies or asthma | 17.86% | 21.85% | <0.001 |
| 6. Depression | 10.48% | 15.14% | <0.001 |
| 7. Cancer disease | 4.74% | 5.79% | <0.001 |
| 8 Joint disease | 19.41% | 21.71% | <0.001 |
| 9. Neurological disease | 9.81% | 12.20% | <0.001 |
| 10. COVID-19 | - | 32.35% | <0.001 |
| None of the above | 33.89% | 20.64% | <0.001 |
| What Meals Do You Eat Most Often? | Before the Pandemic 2019–2020 n = 17,000 | During the Pandemic 2021–2022 n = 17,000 | p-Value |
|---|---|---|---|
| Meals balanced according to the food pyramid | 12.16% | 10.64% | <0.001 |
| Vegetarian meals | 2.44% | 2.27% | 0.144 |
| Vegan meals | 0.19% | 0.20% | 0.662 |
| Meat meals | 13.51% | 11.14% | <0.001 |
| Gluten-free meals | 0.42% | 0.46% | 0.485 |
| Dairy-free meals | 0.35% | 0.35% | 0.948 |
| Carbohydrate-restricted meals | 2.29% | 2.56% | 0.023 |
| Reduced-sodium meals | 3.75% | 3.21% | <0.001 |
| Other types of meals | 0.89% | 1.11% | 0.005 |
| I do not know | 14.00% | 18.07% | <0.001 |
| DIET | Self-Reported Disease | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Hypertension | Diabetes | Heart Disease | COPD | Allergy and Asthma | Depression | Cancer | Joint Disease | Neurological Disease | COVID-19 | |
| Meals balanced according to the food pyramid | 6.45% | 1.73% | 2.55% | 0.46% | 4.40% | 2.55% | 1.40% | 4.09% | 2.10% | 6.43% |
| Vegetarian meals | 0.92% | 0.20% | 0.44% | 0.05% | 1.26% | 1.00% | 0.24% | 0.74% | 0.41% | 1.56% |
| Vegan meals | 0.09% | 0.03% | 0.05% | 0.01% | 0.14% | 0.11% | 0.03% | 0.09% | 0.05% | 0.17% |
| Meat meals | 9.57% | 2.78% | 3.53% | 0.92% | 4.31% | 2.91% | 1.44% | 5.47% | 2.85% | 6.79% |
| Gluten-free meals | 0.28% | 0.12% | 0.17% | 0.03% | 0.36% | 0.21% | 0.08% | 0.26% | 0.16% | 0.32% |
| Dairy-free meals | 0.25% | 0.07% | 0.12% | 0.03% | 0.25% | 0.16% | 0.06% | 0.21% | 0.13% | 0.24% |
| Carbohydrate-restricted meals | 2.13% | 1.12% | 0.81% | 0.15% | 1.09% | 0.82% | 0.38% | 1.29% | 0.64% | 1.59% |
| Saodium-reduced meals | 3.84% | 1.03% | 1.65% | 0.31% | 1.46% | 0.99% | 0.70% | 2.21% | 1.12% | 1.96% |
| Another type of meals with limited carbohudrates | 0.91% | 0.32% | 0.42% | 0.09% | 0.62% | 0.48% | 0.21% | 0.70% | 0.40% | 0.74% |
| Another type of sodium-restricted meals | 13.75% | 3.98% | 5.49% | 1.35% | 7.62% | 5.91% | 2.46% | 8.99% | 5.19% | 11.41% |
| Hypertension | b | p | Beta | p | OR (95% CI) |
|---|---|---|---|---|---|
| - | - | −7.573 | <0.001 | - | |
| During the pandemic | 0.12 | <0.001 | 0.133 | <0.001 | 1.14 (1.08–1.20) |
| Male | 0.51 | <0.001 | 0.303 | <0.001 | 1.35 (1.28–1.43) |
| Age | 0.07 | <0.001 | 0.067 | <0.001 | 1.07 (1.07–1.07) |
| Education level | −0.28 | <0.001 | −0.076 | <0.001 | 0.93 (0.89–0.96) |
| Population of the place of residence | −0.03 | <0.001 | −0.015 | 0.014 | 0.99 (0.97–1.00) |
| BMI | 0.14 | <0.001 | 0.123 | <0.001 | 1.13 (1.12–1.14) |
| Meals balanced according to the food pyramid | −0.36 | <0.001 | −0.143 | <0.001 | 0.87 (0.81–0.93) |
| Vegetarian meals | −0.95 | <0.001 | −0.366 | <0.001 | 0.69 (0.60–0.81) |
| Meat meals | 0.27 | <0.001 | 0.088 | 0.009 | 1.09 (1.02–1.17) |
| Reduced-sodium meals | 0.69 | <0.001 | 0.326 | <0.001 | 1.38 (1.25–1.53) |
| COVID-19 | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −1.461 | <0.001 | - | |
| Male gender | −0.17 | <0.001 | −0.122 | <0.001 | 0.88 (0.83–0.94) |
| Age | −0.01 | <0.001 | −0.011 | <0.001 | 0.99 (0.99–0.99) |
| Married | 0.14 | <0.001 | 0.193 | <0.001 | 1.24 (1.14–1.29) |
| Meals balanced according to the food pyramid | −0.05 | 0.131 | −0.199 | <0.001 | 0.82 (0.76–0.89) |
| Reduced-sodium meals | −0.29 | <0.001 | −0.333 | <0.001 | 0.72 (0.63–0.82) |
| Allergies or Asthma | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −1.440 | <0.001 | - | |
| During the pandemic | 0.25 | <0.001 | 0.258 | <0.001 | 1.29 (1.23–1.37) |
| Male gender | −0.40 | <0.001 | −0.362 | <0.001 | 0.70 (0.66–0.74) |
| Age | −0.01 | <0.001 | −0.013 | <0.001 | 0.99 (0.98–0.99) |
| Married | −0.25 | <0.001 | −0.153 | <0.001 | 0.86 (0.81–0.91) |
| Population of the place of residence | 0.05 | <0.001 | 0.036 | <0.001 | 1.04 (1.02–1.05) |
| BMI | 0.00 | 0.099 | 0.014 | <0.001 | 1.01 (1.01–1.02) |
| Vegetarian meals | 0.36 | <0.001 | 0.198 | 0.001 | 1.22 (1.08–1.37) |
| Dairy-free meals | 0.48 | <0.001 | 0.412 | 0.005 | 1.51 (1.13–2.01) |
| Joint Disease | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −4.351 | <0.001 | - | |
| During the pandemic | 0.14 | <0.001 | 0.117 | <0.001 | 1.12 (1.06–1.19) |
| Male gender | −0.33 | <0.001 | −0.548 | <0.001 | 0.58 (0.54–0.61) |
| Age | 0.05 | <0.001 | 0.053 | <0.001 | 1.05 (1.05–1.06) |
| Education level | −0.43 | <0.001 | −0.342 | <0.001 | 0.71 (0.68–0.74) |
| Married | 0.07 | 0.006 | −0.060 | 0.045 | 0.94 (0.89–1.00) |
| Population of the place of residence | −0.04 | <0.001 | −0.017 | 0.010 | 0.98 (0.97–1.00) |
| BMI | 0.06 | <0.001 | 0.045 | <0.001 | 1.05 (1.04–1.05) |
| Meals balanced according to the food pyramid | −0.27 | <0.001 | −0.102 | 0.006 | 0.90 (0.84–0.97) |
| Dairy-free meals | 0.37 | 0.011 | 0.340 | 0.031 | 1.41 (1.03–1.91) |
| Depression | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −1.326 | <0.001 | - | |
| During the pandemic | 0.42 | <0.001 | 0.424 | <0.001 | 1.53 (1.43–1.63) |
| Male gender | −0.59 | <0.001 | −0.556 | <0.001 | 0.57 (0.53–0.62) |
| Age | −0.01 | <0.001 | −0.005 | <0.001 | 0.99 (0.99–1.00) |
| Education level | −0.05 | <0.001 | −0.141 | <0.001 | 0.87 (0.83–0.91) |
| Married | −0.50 | <0.001 | −0.396 | <0.001 | 0.67 (0.63–0.72) |
| Population of the place of residence | 0.05 | <0.001 | 0.053 | <0.001 | 1.05 (1.04–1.07) |
| Meals balanced according to the food pyramid | −0.24 | <0.001 | −0.185 | <0.001 | 0.83 (0.76–0.91) |
| Vegetarian meals | 0.46 | <0.001 | 0.250 | <0.001 | 1.28 (1.12–1.47) |
| Heart Disease | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −5.424 | <0.001 | - | |
| During the pandemic | 0.18 | <0.001 | 0.164 | <0.001 | 1.18 (1.10–1.26) |
| Age | 0.06 | <0.001 | 0.058 | <0.001 | 1.06 (1.06–1.06) |
| Education level | −0.28 | <0.001 | −0.180 | <0.001 | 0.84 (0.80–0.88) |
| BMI | 0.05 | <0.001 | 0.023 | <0.001 | 1.02 (1.02–1.03) |
| Meals balanced according to the food pyramid | −0.26 | <0.001 | −0.116 | 0.016 | 0.89 (0.81–0.98) |
| Gluten-free meals | 0.42 | 0.006 | 0.505 | 0.002 | 1.66 (1.21–2.28) |
| Dairy-free meals | 0.40 | 0.019 | 0.529 | 0.004 | 1.70 (1.19–2.43) |
| Reduced-sodium meals | 0.53 | <0.001 | 0.182 | 0.003 | 1.20 (1.06–1.35) |
| Neurological Disease | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −2.548 | <0.001 | - | |
| During pandemic | 0.25 | <0.001 | 0.220 | <0.001 | 1.25 (1.16–1.34) |
| Male gender | −0.30 | <0.001 | −0.377 | <0.001 | 0.69 (0.64–0.74) |
| Age | 0.03 | <0.001 | 0.026 | <0.001 | 1.03 (1.02–1.03) |
| Education level | −0.42 | <0.001 | −0.365 | <0.001 | 0.69 (0.66–0.73) |
| Married | −0.06 | 0.092 | −0.126 | 0.001 | 0.88 (0.82–0.95) |
| Population of the place of residence | −0.04 | <0.001 | −0.018 | 0.027 | 0.98 (0.97–1.00) |
| Meals balanced according to the food pyramid | −0.32 | <0.001 | −0.207 | <0.001 | 0.81 (0.74–0.89) |
| Vegetarian meals | −0.50 | <0.001 | −0.329 | 0.001 | 0.72 (0.59–0.88) |
| Dairy-free meals | 0.55 | 0.001 | 0.456 | 0.009 | 1.58 (1.12–2.22) |
| Diabetes | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −8.339 | <0.001 | - | |
| During the pandemic | 0.17 | <0.001 | 0.146 | <0.001 | 1.16 (1.07–1.25) |
| Male gender | 0.38 | <0.001 | 0.184 | <0.001 | 1.20 (1.11–1.30) |
| Age | 0.06 | <0.001 | 0.054 | <0.001 | 1.06 (1.05–1.06) |
| Education level | −0.31 | <0.001 | −0.190 | <0.001 | 0.83 (0.78–0.87) |
| Married | 0.25 | <0.001 | 0.093 | 0.028 | 1.10 (1.01–1.19) |
| Population of the place of residence | 0.00 | 0.826 | 0.020 | 0.031 | 1.02 (1.00–1.04) |
| BMI | 0.12 | <0.001 | 0.114 | <0.001 | 1.12 (1.11–1.13) |
| Vegetarian meals | −0.99 | <0.001 | −0.315 | 0.026 | 0.73 (0.55–0.96) |
| Dairy-free meals | −1.22 | 0.001 | −1.078 | 0.007 | 0.34 (0.16–0.74) |
| Cancer | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −6.025 | <0.001 | - | |
| During the pandemic | 0.21 | <0.001 | 0.199 | <0.001 | 1.22 (1.11–1.34) |
| Male gender | −0.31 | <0.001 | −0.456 | <0.001 | 0.63 (0.57–0.70) |
| Age | 0.05 | <0.001 | 0.053 | <0.001 | 1.05 (1.05–1.06) |
| Population of the place of residence | 0.02 | 0.042 | 0.035 | 0.002 | 1.04 (1.01–1.06) |
| Chronic Obstructive Pulmonary Disease (COPD) | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| b | p | Beta | p | OR (95% CI) | |
| - | - | −6.856 | <0.001 | - | |
| Age | 0.07 | <0.001 | 0.071 | <0.001 | 1.07 (1.07–1.08) |
| Education level | −0.57 | <0.001 | −0.495 | <0.001 | 0.61 (0.55–0.67) |
| BMI | 0.05 | <0.001 | 0.015 | 0.037 | 1.02 (1.00–1.03) |
| Meals balanced according to the food pyramid | −0.78 | <0.001 | −0.658 | <0.001 | 0.52 (0.41–0.65) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gołębiowska, J.; Zimny-Zając, A.; Makuch, S.; Dróżdż, M.; Dudek, K.; Żórawska, J.; Mazur, G.; Agrawal, S. The Impact of Different Types of Diet on the Prevention of Diseases among Polish Inhabitants, Including COVID-19 Disease. Nutrients 2023, 15, 3947. https://doi.org/10.3390/nu15183947
Gołębiowska J, Zimny-Zając A, Makuch S, Dróżdż M, Dudek K, Żórawska J, Mazur G, Agrawal S. The Impact of Different Types of Diet on the Prevention of Diseases among Polish Inhabitants, Including COVID-19 Disease. Nutrients. 2023; 15(18):3947. https://doi.org/10.3390/nu15183947
Chicago/Turabian StyleGołębiowska, Justyna, Anna Zimny-Zając, Sebastian Makuch, Mateusz Dróżdż, Krzysztof Dudek, Joanna Żórawska, Grzegorz Mazur, and Siddarth Agrawal. 2023. "The Impact of Different Types of Diet on the Prevention of Diseases among Polish Inhabitants, Including COVID-19 Disease" Nutrients 15, no. 18: 3947. https://doi.org/10.3390/nu15183947
APA StyleGołębiowska, J., Zimny-Zając, A., Makuch, S., Dróżdż, M., Dudek, K., Żórawska, J., Mazur, G., & Agrawal, S. (2023). The Impact of Different Types of Diet on the Prevention of Diseases among Polish Inhabitants, Including COVID-19 Disease. Nutrients, 15(18), 3947. https://doi.org/10.3390/nu15183947